Embed Size (px)
Citation preview

Diseases of thyroid & parathyroid glands
(2 of 2)

Thyroid neoplasms
Benign
Malignant
Adenomas
Carcinomas
Majority are nonfunctional…coldnodule on thyroid scan (taking lessradioactive material than the surrounding normal tissue)
Minority are oversecreting (toxic adenomas)…hot nodule on thyroid scan & associated
with hyperthyroidism
Mutations
Gain of function
TSH receptor
GNAS
Toxic adenomaRAS
Also seen in toxic multinodular goiterNonfunctioning adenomas…also seen in follicular carcinoma
Papillary(85% of the cases)
Follicular
Anaplastic(undifferentiated)
Medullary
from follicular epithelial cells
from parafollicular C cells
Most of the time hot nodules are benign, while 10% of cold nodules are malignant

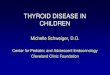
Thyroid adenoma Solitary, well-circumscribed and encapsulated
*Resembling normal follicles
Hurthle cell adenoma (the cells show abundant finely granular eosinophilic cytoplasm)
Follicular adenoma
*The most important to differentiate from follicular carcinoma is the integrity of the capsule and absence of vascular invasion…so FNA (fine needle aspiration cytology)cannot tell us if it is a follicular adenoma or follicular carcinoma…we need in this case to remove the nodule and assess the capsule(histopathologcal examination)
Endocrine atypia (focal nuclear pleomorphism, atypia,and prominent nucleoli) is accepted
Usually as a painless nodulein neck examination and on ultrasound…if large may compress adjacent structuresand cause dysphagia for example
Elsevier. Kumar et al. Robbins and Cotran pathologic basis of diseases 9th…modified Elsevier. Kumar et al. Robbins and Cotran pathologic
basis of diseases 9th…(Courtesy Dr. Mary Sunday, Duke University, Durham,N.C.)

Thyroid carcinoma, epidemiology & risk factors
• Females more in early and middle adult years, but equal in childhood and late adult life
• The most important risk factor: Ionizing radiation…especially papillary carcinoma
• Iodine deficiency goiter multinodular goiter minor risk for
follicular carcinoma

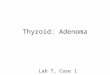
Papillary carcinoma
also nuclear grooves (coffee bean nuclei)
= ground-glass
*Single or multiple painless nodules, nonfunctioning
Psammoma body
*Lymphatic invasion is usually present & metastases to adjacent cervical lymph nodes occur in up to one-half of cases…may be detected first*Hematogenous spread is much less common
*Papillae are not mandatory and nuclear features are enough…e.g., the most common variant is encapsulated follicular variant (follicles not papillae)
*FNA is good for diagnosis
*Indolent, 10-year survival 95%
*Poor prognosis factors: age >40, extrathyroid extension and distant metastases*Lymph node involvement is less important in prognosis
*The treatment is total thyroidectomy(because of the risk for multicentricity)
MAP kinase pathway activationis the most common(especially BRAF oncogene)
https://library.med.utah.edu/WebPath/ENDOHTML/ENDO027.html...modified
Elsevier. Kumar et al. Robbins basic pathology 10th…modified

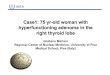
Follicular carcinoma *The 2nd most common thyroid carcinoma*at older age than papillary (40-60)*a much higher percentage in areas with dietary iodine deficiency
*mostly presents as a solitary cold nodule…in rare cases, may be hyperfunctional
*Tendency for hematogenous spread…especially to the lungs & bone*Regional lymph node metastasis is uncommon
Capsule invasion…the most important for diagnosis
We need histopathological examinationto assess for this. FNA is not beneficial in differentiating follicular adenoma from carcinoma
*Removed by surgery…metastases can be ablated by radioactive iodine
Elsevier. Kumar et al. Robbins basic pathology 10th

Anaplastic carcinoma
*Undifferentiated*mostly conversion from well-differentiated (papillary or follicular) but may be de novo*TP53 mutations*Aggressive, large, with extrathyroid extension into the adjacent structures in the neck*Metastasis common*Mortality rate 100%...usually in less than 1year (due to the extension into vital neck structures)*Usually older ages (>60)*Undifferentiated cells (anaplastic)…large or spindle*Adjacent foci of well differentiated tumor may be found
Check http://www.pathologyoutlines.com/topic/thyroidundiff.html for references
Check http://www.pathologyoutlines.com/topic/thyroidundiff.html for references

Medullary carcinoma
*a neuroendocrine tumor*from parafollicular C cells*secretes calcitonin…its measurement is important for diagnosis and postoperative followup*in some cases, secretion of other hormones like somatostatin, serotonin & vasoactive intestinal peptide*70% are sporadic and 30% familial:-MEN 2A-MEN 2B-Familial medullary thyroid carcinoma without associated MEN syndrome*RET receptor tyrosine kinase gain of function mutations…in sporadic and familial cases*5th & 6th decades…sporadic and familial not associated with MEN*MEN 2A and MEN 2B can occur even in children*Multicentricity is especially common in familial cases*polygonal to spindle-shaped cells, which may form nests, trabeculae, and even follicles. Amyloid deposits, derived from altered calcitonin molecules, are present in the adjacent stroma in many cases
*Multicentric C cell hyperplasia in the surroundingthyroid parenchyma…seen only in familial cases…may be a precursor lesion
*Immunohistochemical staining shows positivity for calcitonin…in both the cytoplasm of tumor cells and the amyloid material
We can offer prophylactic thyroidectomy
Elsevier. Kumar et al. Robbins basic pathology 10th

Parathyroid hormone actions, introductionThe activity of the parathyroid glands is controlled by the level of free (ionized) calcium in the blood

Parathyroid (hormone) diseases
Hyperparathyroidism Hypoparathyroidism*far less common than hyper*causes:-surgical ablation (with thyroidectomy for example)-congenital absence (Di George)-autoimmune hypoparathyroidism(AIRE mutation)*symptoms: neuromuscular irritability (carpopedal spasm, tetany, facial grimacing)…cataracts if chronic…arrhythmia, increased intracranial
pressure and seizures may occur
1ry
2ry*with chronic renal failure*less excretion of phosphate…so it increases in blood and binds free Ca*less α1-hydroxylase activityproduction by the kidney soless active vitamin D so less calciumabsorption from gut*hyperplasia of the parathyroids will occur*Bone changes similar to 1ry may also occur… = renal osteodystrophyand metastatic calcification (driven by hyperphosphatemia) may also occur*serum calcium is near normal
3ry
*adults*women more*Causes:-adenoma (most common)-hyperplasia (diffuse or nodular)-carcinoma*Genetic abnormalities in parathyroid tumors:-Cyclin D1 (oncogene)-MEN1 (tumor suppressor)…not only in familial cases*adenoma is usually solitary & encapsulated*Most parathyroid adenomas weigh between 0.5 and 5 g*hyperplasia usually more than 1 gland, but may be one*Carcinoma usually irregular and may exceed 10g*Invasion of surrounding tissues and metastasis arethe only definitive criteria to say: carcinoma*painful bones, renal stones, abdominal groans, andpsychic moans
also
If activity increases until hypercalcemia…parathyroidectomy is needed
*What is osteitis fibrosa cystica?*What is brown tumor?

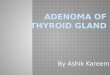
Parathyroid adenoma
The other glands are normal in size or somewhat shrunken
Compressed rim of the remaining normal tissuecapsule
Adenoma
Less fat
-Mainly chief cells-Endocrine atypia is accepted
= sestamibi scan
The most common cause of hypercalcemia in outpatients is: 1ry hyperparathyroidismThe most common cause of hypercalcemia in inpatients is: malignancy
Elsevier. Kumar et al. Robbins basic pathology 10th…(Courtesy of Dr. Nicole Cipriani, Departmentof Pathology, University of Chicago, Chicago, Illinois.)…modified
Elsevier. Kumar et al. Robbins basic pathology 10th…modified