Embed Size (px)
Citation preview

405
ECTOPIC PREGNANCYBy G. BANCROFT-LIVINGSTON, M.D. (Lond.), F.R.C.S. (Eng.), M.R.C.O.G.
Senior Registrar and Research Assistant, The Middlesex Hospital, London
The term' ectopic pregnancy ' includes all preg-nancies which occur outside the uterine cavity andis, therefore, a more inclusive one than ' extra-uterine pregnancy,' which by definition excludesangular (interstitial) pregnancy and pregnancy ina rudimentary horn of a bicornuate uterus.
Ectopic pregnancy received only scant attentionin the medical literature of the mediaeval and re-naissance periods, and it fell to Parry (I876) tograsp the full significancee of the condition and torealize that it was amenable to surgical treatment.This realization coincided with the great stridesbeing made in abdominal surgery, and Tait per-formed his first laparotomy for the condition inI883. This patient died, but during the next fiveyears he performed 42 laparotomies for ectopicpregnancy with but two deaths (Tait, i888).
Since the days of Tait the condition has con-tinued to cause both diagnostic and therapeuticdifficulty, and, therefore, a review of 98 casestreated at the Middlesex Hospital between theyears I930 and I950 was considered worthwhile.The fact that only 98 cases of ectopic pregnancy
could be found over a 20 year period in a largegeneral hospital suggests that the condition .is notcommon. Our 98 cases represent an incidence ofectopic pregnancy to term intra-uterine pregnancyof about one in zoo. This figure agrees very closelywith that quoted by Eastman (1950), but is verymuch lower than the incidence of one in 50 preg-nancies described by Ingraham (I949).Aetiology
It remains a firm belief that fertilization of theovum takes place in the ampullary portion of theFallopian tube. Why, then, is ectopic pregnancysuch a relatively uncommon condition? It must beadmitted that the answer to this question is notcompletely known, but remembering the mode offertilization of the ovum, it is reasonable to assumethat ectopic pregnancy may occur under any con-dition in which retardation or arrest of the onwardmovement of the fertilized ovum is possible orlikely. These conditions may be listed as follows:
I. Obstruction of the Fallopian tube fromwithout.
2. Obstruction of the lumen of the tube.3. Destruction of the tubal ciliated epithelium.4. Fibrosis of the muscle of the Fallopian tube.5. Congenital tubal abnormalities.6. Tubal endometriosis.Inflammatory tubal changes causing tubal
fibrosis, obstruction or epithelial damage may fol-low salpingitis or pelvic peritonitis from any cause.Tubal abnormalities such as accessory ostia orcongenital diverticula predispose to ectopic preg-nancy, as does tubal endometriosis, where deciduamay form in the affected tube, thereby encouragingtubal implantation of the ovum. Inflammatorytubal changes and the associated risk of ectopicpregnancy can often be suspected from the history,whereas congenital tubal abnormalities, and mostcases of tubal endometriosis, are pathologicaldiagnoses and can only interest the clinician inretrospect. When all is said and done, there areno apparent aetiological factors in a large pro-portion of cases of ectopic pregnancy. In the serieshere presented, only 20 gave a positive history ofprevious pelvic inflammation.
TABLE IHISTORY IN 98 CASES OF ECTOPIc GESTATION
Previous Abortion 9.. .. .. 9Previous Ectopic Pregnancy .. .. 5Previous Salpingitis I.. .. .. .. IPrevious Appendicitis.. .. .. .. 2 20Recent Salpingostomy .. .. .. IRecent Tubal Insufflation .. .. ..Graffenburg Ring Present .. .Negative History .. .. .. .. 78
Siegler (I945) found residua of pelvic inflam-matory disease in 78 per cent. of 127 cases.Beacham (I948) in New Orleans and Buss (1950)and his colleagues in Cape Town found a very highincidence of ectopic pregnancy which they relatedto the frequency of salpingitis and pelvic inflam-mation in a large coloured population.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

406 POSTGRADUATE MEDICAL JOURNAL August 1953
TABLE 2
AGE DISTRIBUTION OF 98 CASES OF ECTOPIc GESTATION
Under 20 years .. .. .. .. .. 0
21-30 years .. .. .. .. .. 4231-40 years .. .. .. .. .. .. 51Over 41 years .. .. .. .. 5
This age distribution does not in itself call forcomment, but it must.also be noted that 51 of thesecases were nulliparous, a much higher incidencethan that reported by Siegler (I945) (24.5 per cent.)or Gioanni and Wirtz (I949) (26.6 per cent.).
MotatyThe mortality from ectopic pregnancy has
diminished with the advent of antibiotics, im-proved methods of anaesthesia and wider use ofblood transfusion. There were no deaths amongstthe 98 cases here reported, and other workers suchas Echols (I934) and Leff and Winson (i947) havealso reported large series without a death. Thereis no room for complacency, however, as Siegler(1945) submits a mortality of 3.9 per cent. in127 cases.
Symptoms and DiagnosisFig. i shows the various courses that an un-
ruptured ectopic pregnamey may tae. They areseparated into the 'rare,' the 'uncommon' andthe' coMiprqn.' A fill understanding of these pos-sibilities is essential to the clinician. Without thisunderstanlding symptQs and signs which are con-fusing at the best of times become quite un-intelligible. If the condition of ectopic pregnancyin its various pathological varieties is borne inmind in every eas of obscre tbdominal or pelvicdisorder in women, the erroneous diagnoses willbe reduced to a minimum.The Fallopias tube is a totly unsuitable site
for the development of a pregnancy beyond a verylimited time, ad for this rean tubal pregnancyreaching term is indeed a rare occurrence; no caseoccurred in the aeries reported.
Secondary abdominal pregnancy is not quite sorare. This series contains one such case, and theusual reported incidence is about i per cent. of allectopics. At some time relatively early in preg-nancy the Fallopian tube'ruptures, freeing the em-bryo and its membranes, which then gain attach-
UNRUPMTRO EcrOPcPA(GNANCY
tubal pregnancy Q.Qpt'Q.¶
Tubal TubalTubaf(4tANQj lekege mole
I I b/liIe bleeding
I .I
4, wr T
I I hO ^-
I. Iqev
I WWMN' 1, Ct74A0I l
FIG. i.-The natural history of ectopic pregnancy.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

August I953 BANCROFT-LIVINGSTON: Ectopic Pregnancy 407
ment at some other intraperitoneal site, and de-velopment continues. This incident may passunnoticed, a.d attention is not called to the con-dition until spurious labour develops. Painfuluterine contractioas occur near term, and after avariable period of time the foetus dies. Laparo-tomy at this stage will lead to extraction of a deadfoetus. The problem then arises: What is to bedone with the placenta? It is probably attached tothe bowel or its mesen-tery and attemapted removalwould lead to catastrophic bleeding. in thesecircumstances it is best to divide the umbilicalcord as near to the placenta as possible and toleave the placenta alone.
Mrs. L.O., aged 33, was admitted to the MiddlesexHospital on October I5, I'935. She was at term andfoetal death had apparently occurred between three andfour weeks previously. The foetus was presenting bythe breech, and five unsuccessful attempts hWd beenmade to induce labour. Examination and intra-uterineexploration under anaesthesia revealed the true diag-nosis, and a dead foetus was removed from the peritonealcavity. The placenta was seen to be attached to themesentery of the small bowel and was left undisturbed.The patient made an uninterrupted recovery.
This treatment is approved by most authorities,but Nicodemus and Carrigg (I940) point out thatif the placenta can be removed without risk ofbleeding, then recovery is most likely to be smoothand uncomplicated. They also affirm that thelargest number of maternal deaths occur in thosecases in which marsupialization or drainage hasbeen carried out.Laparotomy performed subsequently in some of
these cases has proved that placental absorptioncan occur. Cases are on record in which the con-dition has passed unrecognized at the time, to bediagnosed perhaps many years later when laparo-tomy reveals a partially absorbed and calcifiedfoetus lying in the peritoneal cavity.
It is possible to diagnose secondary abdominalpregnancy before spurious labour or foetal deathhave occurred. There are many reports of thishaving been done, and the important diagnosticpoints appear to be abnormal and unstable foetalpositions associated with undue ease of palpatiqnof the foetus lying free in the peritoneal cavity.The diagnosis can be confirmed by exploration ofthe uterine cavity with a sound or by hystero-salpingography. In these circumstances, laparo-tomy at term, extraction of the foetus and themanagement of the placenta as suggested above,would be the best line of treatment to adopt(Roques and Winterton, 1937).
Suter and Wichser (I948) state that about 25 percent. of all ectopic pregnancies diagnosed after thefifth month of pregnancy will result in livingbabies. They sound the warning, however, that
one-third of these infants wilt have major or minordeformities and only one-half of them will surviveeight days or more.A diagnosis of ectopic pregnancy in the early
stages before tubal rupture or leakage has occurredis possible, but has rarely been made in our ex-perience. A short period of amenorrhoea accom-panied by vague abdominal pain situated in one orother iliac fossa might prompt a pelvic examinationat which a small tender mass in one or other lateralfornix might be detected. In these circumstancesit is unlikely that more than a suspicion of the con-dition will be aroused.Sudden tubal rupture with little or no warning
constitutes the type of ectopic pregnancy des-cribed in many of the standard textbooks. It iscertainly very dramatic when seen but fortunatelyconstitutes only a small proportion of any series.The history is short, and may be one of amenor-rhoea accompanied by slight vaginal bleeding.There is sudden collapse with well-marked signsof shock, severe abdominal pain and obvious evi-dence of severe intraperitoneal bleeding. Thediagnosis is obvious, the only doubt about thecase being the eventual outcome for the patient.
TABLE 3LENGTH OF HISTORY OF 98 CASES OF ECTOPIC PREGNANCY
Under 24 hours .. 2424 hours-7 days .. I5 (I becoming suddenly acute)Over 7 days.. .* 5I (3 ,,Uncertain .. .. 7
One full-time secondary pregnancy is excluded.
A glance at the above table shows that onlyabout 25 per cent. of all cases have a history ofless than 24 hours, and it is from this group thatthe dramatic cases of sudden tubal rupture aredrawn. It is as well to remember that in a smallproportion of the cases with a short history thediagnosis is made before tubal rupture has oc-curred. Those cases in which tubal leakage, sug-gested by a long history, becomes a sudden severerupture should also be remembered. It is thislatter occurrence that constitutes one of thesoundest arguments for early surgery in all cases inwhich an ectopic pregnancy has been diagnosed.Four such cases occurred in the series here'pre-sented, two of them in circumstances which it iswell to notice. Determined palpation of a leakingor partially ruptured tube may convert it into afreely bleeding completely ruptured one, withserious and perhaps disastrous results.
Mrs. R.G. was known to be three months' pregnantand on January 9, I950, at I a.m., she summoned hergeneral practitioner. She had been bleeding slightlyfor five days and was suffering from severe abdominal
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

408 POSTGRADUATE MEDICAL JOURNAL August I953
pain. Her doctor suspected a ruptured ectopic preg-nancy and arranged for an ambulance to take her tohospital. She was seen in the casualty department at4.30 a.m., where the casualty officer examined her andconsidered that there was very little wrong. She wassent home by ambulance but when she arrived homethe ambulance attendants realized that she was gravelyill and brought her straight back to hospital. By thistime it was 7 a.m., and her condition on admission wasgrave. She was severely shocked and pulseless, but therapid transfusion of two pints of blood supported hersufficiently for laparotomy and removal of the rupturedright Fallopian tube to be carried out. The peritonealcavity was full of fresh blood and blood clot. A post-operative blood transfusion hastened an uneventfulconvalescence.
The other case in which acute were superim-posed upon chronic symptoms occurred after ex-amination of a patient in hospital by house officer,registrar and consultant. Baird (I950) drawsattention to the fact that such sudden bursting ofthe Fallopian tube with severe bleeding may alsooccur whilst an obscure case is being examinedunder anaesthesia.About io per cent. of cases of ectopic pregnancy
present with sudden tubal rupture and severe intra-
peritoneal bleeding and it is in this group thatdeaths are most likely to occur.The most usual course for an ectopic pregnancy
is that of tubal leakage proceeding to peritubalhaematocele, pelvic haematocele, tubal mole ortubal abortion (Fig. i). By tubal abortion ismeant extrusion of the ovum from the fimbriatedend of the tube after bleeding around it hasseparated it from the wall of the tube. This is adiagnosis which will probably only be made atlaparotomy and occurred eight times in our series.How often this condition occurs and escapesdiagnosis is pure guesswork, but it has beensuggested that it is more common than is realizedand is perhaps responsible for many of the in-cidents of amenorrhoea followed by some irregularbleeding and abdominal pain seen in practice.The incidence of tubal abortion and the other sitesof implantation of ectopic pregnancy in our seriesis seen depicted in Fig. 2.A tubal mole results when the ovum has been
detached from the wall of the tube by bleeding anddies. The tube does not rupture, nor does ex-
R ANATOMICAL SITUATION OF 89 CASES OF L
B ECTOPIC GESTATION. G
D H
A. LEFT AMPULLA. 31.B. RIGHT AMPULLA. 42.
* ~C- TUBALD.J ABORTION. .
9 CASES EXCLUDED, INCLUDING ONE E. INTERSTITIAL. I.OF SECONDARY ABDOMINAL f ISTHMUS. 2.PREGNANCY. G. TUBAL MOLE. 3.
H. PRIMARY 2OVARIAN. A
FIG. 2.-Situation of 89 cases of ectopic pregnancy.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

August I953 BANCROFT-LIVINGSTON: Ectopic Pregnancy 409
trusion of the ovum from the fimbriated end of thetube occur; symptoms subside and the diagnosisis only made at laparotomy. Only three suchcases were encountered in our series (Fig. 2).
In the majority of cases of ectopic pregnancy amoderate degree of intraperitoneal bleeding occurs;if it is limited in amount the blood clots in thevicinity of the rent in the tube, forming a peritubalhaematocele. Somewhat heavier bleeding willcause spill into the pouch of Douglas where clottingoccurs-pelvic haematocele. In rare cases thetube leaks from the area enclosed between the twolayers of the broad ligament and a haematoma isformed.
In most of these patients the history extendsover a period exceeding 24 hours and diagnosismay not be easy. In the series here presented acorrect pre-operative diagnosis was made in only7I patients (Fig. 3); in 27 cases a variety ofdiagnoses were made for a variety of reasons.
Study of Table 4 shows that a large number ofthese incorrectly diagnosed cases suffered no delayin treatment. Nine cases were recognized as acuteabdominal emergencies of obscure aetiology and
TABLE 4INCORRECT DIAGNOSES IN 27 CASES OF ECTOPIC
PREGNANCY
Acute Abdominal Emergency.. ..Abortion .. .. .. .. .Pelvic Tumour .. ..5Fibroids .. ..3Pleurisy .. .. .. .. .. .. 27Salpingitis . tAppendicitis .. .. ..Twisted Pedicle of an Ovarian Cyst .ICarcinoma of Body of Uterus..
in two more cases a diagnosis of torsion of thepedicle of an ovarian cyst and acute appendicitisdemanded urgent surgery. In the remainder ofthese cases there was very real doubt. The historywas long and the symptoms were vague and vari-able. Slow leakage from the tube occurred and aperitubal or pelvic haematocele formed. As thesecases may at any stage become acute, accuratediagnosis is an urgent necessity.The acute cases are usually diagnosed correctly,
and Atlee (I947) found only iz incorrect diagnoses
EC fWSW- 9BC-
]-. . . ..,.,..-, -S \.--T *- \
..
.s ..
r
\' /".\, 's...1
..
|S A
, ' g---= R f ...................................... . . ... - , ---= . - , ........ .-, f.' Vf .' .; \,
--2- --J \
f N \
,., j .... ,.\
t'.- 4, 6 \
w t 9rr}.
FIG. 3.-Diagnosi8 and symptoms of 98 cases of ectopic pregnancy.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
in a series of ioo cases; -he stresses the fact thatonly two of these incorrect diagnoses were in acutecases. Beacham (i948), in a very large series ofcases, reported that a correct diagnosis was mnade in44 per cent. up to 1920, 62 per cent. from 192i to1936 and 82 per cent. from I937 to 1946. Heattributed the rising accuracy of diagnosis to in-creased alertness to the possibility of the condition.When a correct diagnosis is made without delay,
it has almost invariably been made on the presenceof abdominal pain, slight vaginal bleeding and thedetection of an adnexal mass. Eighty-five of ourcases presented with abdominal pain and bleedingand in 25 of these a mass was detected (Fig. 3).Leff and Winson (I947) found this triad present in63 per cent. of their patients, 83 per cent. havingpain and bleeding only. In only a proportion ofcases will there be a suggestion of early pregnancy;31 of our patients gave a history of arnenorrhoeaor ' a period overdue' (Fig. 3). irn many casessymptoms arise before a period could be missed,and then the diagnosis may be further obscured bythe appearance of irregulr and persistent vaginalbleeding.The presence of unclotted blood in the peri-
toneal cavity may give rise to two very suggestivediagnostic points, firstly referred pain over the tipof the shoulder due to irritation of the under sur-face of the diaphragm and secondly bluish dis-colouration around the umbilicus known asCullen's sign (Cullen, I9I8). This sign has notbeen seen by us and only occurred once in theseries reported by Way (1949). Shoulder tip painoccurred in I2 of our cases but many authors finda much higher incidence, Way (I949) quoting afigure of 6o per cent. for his series. It is in-teresting to note that occasionally this pain may beaggravated or even produced in the first instanceby raising the foot of the bed and allowing theblood to run towards the diaphragm.A pelvic haematocele may cause rectal dis-
comfort and in six of our patients severe tenesmuswas present. In two of our patients a pelvichaematocele caused acute retention of urine, apossibility referred to by few other authors.Some degree of abdominal pain iS present in
almost ioo per cent. of cases, and it is well to re-member that it mqy be due to one of severalcauses:
i. Acute pain due to sudden tubal rupture.2. Dull pain due to slow tearing of the tube.3. Colicky pain of tubal peristalsis (tubal abor-
tion).4. Peritoneal irritation including shoulder tip
pain.5. Pain elicited by palpation.Slight vaginal bleeding from the uterine decidual
membrane is also present in. a large number of
cases. Occasionally the decidua may be shed intact,as happened in two of our patients. Histologicalexaminaation of the membrane may soiw a verymarked decidual reaction and no chorionic viili,a finding very suggestive of ectopic pregnancy.Arguing from this, some workers have advocatedhistological examination of endometrium obtainedby curettage as a means of making a diagnosis inobscure cases. Romney (i95o) examined iI5endometrial linings from cases of ectopic preg-nancy and found that only 9.1 per cent. showed adecidual reaction. These figures indicate that theexamination has only limited value, but in difficultand unusual cases which have been submitted touterine curettage with a diagnosis of abortion, thecurettings obtained should be examined micro-scopically.
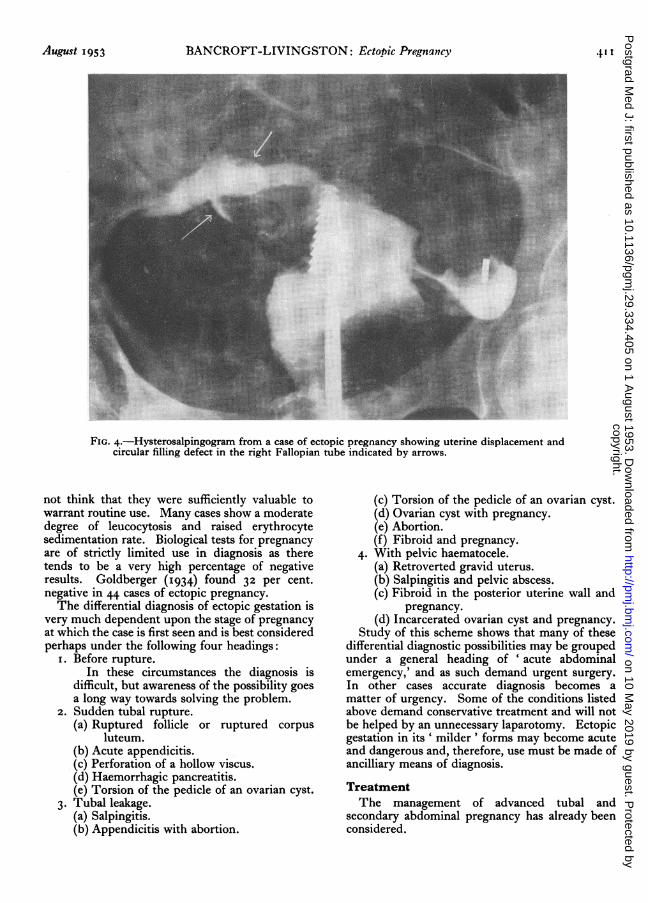
In doubtful cases, direct inspection of theFallopian tubes by peritoneoscopy or culdoscopyhas been advocated, although we have no personalexperience of either. Falls (i950) has written infavour of culdoscopy, but Schauffler (1945) hasstated that he has not been impressed by the pro-cedure and recommends aspiration of the pouchof Douglas by means of a needle and syringe. Thisprocedure may be of value as long as it is realizedthat a negative result does nothing to rule out thepossibility of ectopic gestation (Decker, I947). Asfar as peritoneoscopy is, concerned, it seems to holdvery few advantages over laparotomy and is nearlyas dangerous. Hysterosalpingography would ap-pear at first examination to be a foolhardy pro-cedure in cases of ectopic gestation, but Nielsen(I947) has had considerable experience with theprocedure and finds it free from danger. He usesa water soluble contrast medium and describes acharacteristic uterine atony and several pQssibletubal appearances:
i. Tube fills, showing filling defect.2. Tube fills, but no defect.3. Tube partly fills.4. Tube not filled.He points out that 50 per cent. of cases fall into
group (i), and in such circumstances a correctdiagnosis should be made. He recognizes sepsis,severe bleeding and intra-uterine abortion ascontra-indications to the procedure. We have hadexperience of the procedure in only two cases andin both a positive and correct diagnosis was madeon the presence of a tubal, filing defect (Fig. 4).The dangers of the procedure appear to have beenover-exaggerated.
Other ancilliaty methods of diagnosis are of verylimited wlue. The deteetion of acid haematin inthe circulation my lbe of value in obscure cases,and Pommerenke (i936) makes a claim for the de-tection of circulating bilirubin. We have had nopersonal experience of these methods but would
AuRgust 1953410
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from
August 1953 1IANCROFT-LIVINGSTON: Ectopic Pregnancy 41 t
FIG. 4.-Hysterosalpingogram from a case of ectopic pregnancy showing uterine displacement andcircular filling defect in the right Fallopian tube indicated by arrows.
not think that they were sufficiently valuable towarrant routine use. Many cases show a moderatedegree of leucocytosis and raised erythrocytesedimentation rate. Biological tests for pregnancyare of strictly limited use in diagnosis as theretends to be a very high percentage of negativeresults. Goldberger (I934) found 32 per cent.negative in 44 cases of ectopic pregnancy.The differential diagnosis of ectopic gestation is
very much dependent upon the stage of pregnancyat which the case is first seen and is best consideredperhaps under the following four headings:
i. Before rupture.In these circumstances the diagnosis is
difficult, but awareness of the possibility goesa long way towards solving the problem.
2. Sudden tubal rupture.(a) Ruptured follicle or ruptured corpus
luteum.(b) Acute appendicitis.(c) Perforation of a hollow viscus.(d) Haemorrhagic pancreatitis.(e) Torsion of the pedicle of an ovarian cyst.
3. Tubal leakage.(a) Salpingitis.(b) Appendicitis with abortion.
(c) Torsion of the pedicle of an ovarian cyst.(d) Ovarian cyst with pregnancy.(e) Abortion.(f) Fibroid and pregnancy.
4. With pelvic haematocele.(a) Retroverted gravid uterus.(b) Salpingitis and pelvic abscess.(c) Fibroid in the posterior uterine wall and
pregnancy.(d) Incarcerated ovarian cyst and pregnancy.
Study of this scheme shows that many of thesedifferential diagnostic possibilities may be groupedunder a general heading of ' acute abdominalemergency,' and as such demand urgent surgery.In other cases accurate diagnosis becomes amatter of urgency. Some of the conditions listedabove demand conservative treatment and will notbe helped by an unnecessary laparotomy. Ectopicgestation in its' milder' forms may become acuteand dangerous and, therefore, use must be made ofancilliary means of diagnosis.
TreatmentThe management of advanced tubal and
secondary abdominal pregnancy has already beenconsidered.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from
4I2 POSTGRADUATE MEDICAL JOURNAL Atugust 1953
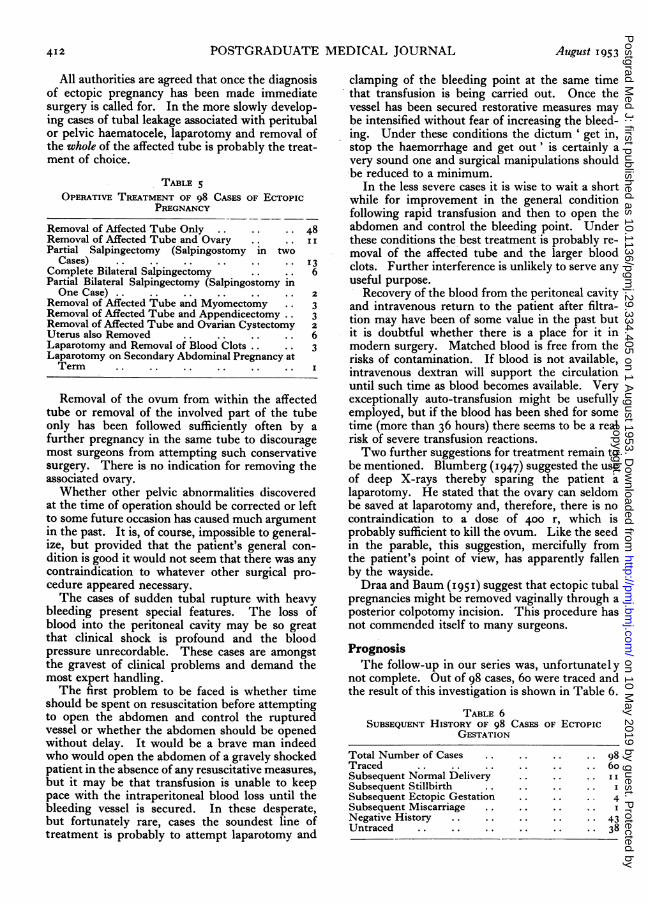
All authorities are agreed that once the diagnosisof ectopic pregnancy has been made immediatesurgery is called for. In the more slowly develop-ing cases of tubal leakage associated with peritubalor pelvic haematocele, laparotomy and removal ofthe whole of the affected tube is probably the treat-ment of choice.
TABLE 5OPERATIVE TREATMENT OF 98 CASES OF ECTOPIC
PREGNANCY
Removal of Affected Tube Only .. .. .. 48Removal of Affected Tube and Ovary .. .. IPartial Salpingectomy (Salpingostomy in two
Cases) .. .. .. .. .. .. 3Complete Bilateral Salpingectomy .. .. 6Partial Bilateral Salpingectomy (Salpingostomy inOne Case) .. .. .. .. .. .. 2
Removal of Affected Tube and Myomectomy .. 3Removal of Affected Tube and Appendicectomy .. 3Removal of Affected Tube and Ovarian Cystectomy 2Uterus also Removed .. .. .. . 6Laparotomy and Removal of Blood Clots .. .. 3Laparotomy on Secondary Abdominal Pregnancy atTenn .. .. .. .. .. ..
Removal of the ovum from within the affectedtube or removal of the involved part of the tubeonly has been followed sufficiently often by afurther pregnancy in the same tube to discouragemost surgeons from attempting such conservativesurgery. There is no indication for removing theassociated ovary.Whether other pelvic abnormalities discovered
at the time of operation should be corrected or leftto some future occasion has caused much argumentin the past. It is, of course, impossible to general-ize, but provided that the patient's general con-dition is good it would not seem that there was anycontraindication to whatever other surgical pro-cedure appeared necessary.The cases of sudden tubal rupture with heavy
bleeding present special features. The loss ofblood into the peritoneal cavity may be so greatthat clinical shock is profound and the bloodpressure unrecordable. These cases are amongstthe gravest of clinical problems and demand themost expert handling.The first problem to be faced is whether time
should be spent on resuscitation before attemptingto open the abdomen and control the rupturedvessel or whether the abdomen should be openedwithout delay. It would be a brave man indeedwho would open the abdomen of a gravely shockedpatient in the absence of any resuscitative measures,but it may be that transfusion is unable to keeppace with the intraperitoneal blood loss until thebleeding vessel is secured. In these desperate,but fortunately rare, cases the soundest line oftreatment is probably to attempt laparotomy and
clamping of the bleeding point at the same timethat transfusion is being carried out. Once thevessel has been secured restorative measures maybe intensified without fear of increasing the bleed-ing. Under these conditions the dictum ' get in,stop the haemorrhage and get out' is certainly avery sound one and surgical manipulations shouldbe reduced to a minimum.
In the less severe cases it is wise to wait a shortwhile for improvement in the general conditionfollowing rapid transfusion and then to open theabdomen and control the bleeding point. Underthese conditions the best treatment is probably re-moval of the affected tube and the larger bloodclots. Further interference is unlikely to serve anyuseful purpose.
Recovery of the blood from the peritoneal cavityand intravenous return to the patient after filtra-tion may have been of some value in the past butit is doubtful whether there is a place for it inmodern surgery. Matched blood is free from therisks of contamination. If blood is not available,intravenous dextran will support the circulationuntil such time as blood becomes available. Veryexceptionally auto-transfusion might be usefullyemployed, but if the blood has been shed for sometime (more than 36 hours) there seems to be a realrisk of severe transfusion reactions.Two further suggestions for treatment remain to
be mentioned. Blumberg (I947) suggested the useof deep X-rays thereby sparing the patient alaparotomy. He stated that the ovary can seldombe saved at laparotomy and, therefore, there is nocontraindication to a dose of 400 r, which isprobably sufficient to kill the ovum. Like the seedin the parable, this suggestion, mercifully fromthe patient's point of view, has apparently fallenby the wayside.Draa and Baum (I951) suggest that ectopic tubal
pregnancies might be removed vaginally through aposterior colpotomy incision. This procedure hasnot commended itself to many surgeons.
PrognosisThe follow-up in our series was, unfortunately
not complete. Out of 98 cases, 6o were traced andthe result of this investigation is shown in Table 6.
TABLE 6SUBSEQUENT HISTORY OF 98 CASES OF ECTOPIC
GESTATION
Total Number of Cases .. .. .. .. 98Traced .. .. .. .. .. .. 6oSubsequent Normal Delivery .. .. .. ISubsequent Stillbirth .. .. .. ..Subsequent Ectopic Gestation .. .. .. 4Subsequent Miscarriage .. .. .. .. INegative History .. .. .. .. .. 43Untraced .. .. .. .. .. .. 38
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from

Augutst 195,3 BANCROFT-LIVINGSTON: Ectopic Pregnancy 413
It is impossible to draw any conclusion fromthese figures except to say that normal pregnancymay well occur after an ectopic gestation andanother ectopic gestation is far from rare.A study of the literature throws very little more
light on the problem. Way (1949) was only ableto trace 58 cases out of 85 suitable for review andof these three had had another ectopic pregnancyand i I patients shared 13 intra-uterine preg-nancies. Masani (1949) states that from varioussurveys that have appeared in the literature, 30to 40 per cent. are likcly to conceive at a later date,and the recurrence rate of ectopic pregnancy isabout 4 per cent. These figures are in accord withour findings, but Schumann (I92I) quotes a one ineight chance of recurrent ectopic pregnancy.
In view of the limitations of most follow-upinvestigations we can probably do no better thanagree with Eastman (1950) when he states thatthere is one chance in three of subsequent preg-nancy occurring in a patient who has had anectopic pregnancy and of these subsequent preg-nancies approximately one in ten terminates inanother ectopic. He points out that this is 30times the usual incidence of this complication.
Summaryi. Ninety-eight cases of ectopic gestation oc-
curring during a 20-year period are presented.2. The aetiology is discussed, with special re-
ference to previous pelvic inflammation.3. The various pathological types are listed and
special attention is paid to the way in which theypresent clinically.
4. It is noted that although the diagnosis maynot always be obvious, in about one-third of theobscure cases an acute abdominal emergency ispresent which demands urgent surgery.
5. A correct diagnosis was made in 77 per cent.of our cases. Acute sudden tubal rupture withprofuse bleeding is very seldom misdiagnosed.
6. Although various ancilliary diagnosticmethods are presented, it is stressed that accuratediagnosis depends primarily upon an accuratehistory and full clinical examination.
7. Once a diagnosis has been made laparotomyis essential and complete removal of the involvedFallopian tube is the treatment of choice. Whetheror not other intra-abdominal disease is corrected atthe same time depends upon the patient's generalcondition at the time of laparotomy.
8. There were no deaths in this series and withmodern anaesthesia, transfusion and antibioticsthe death rate should be very low in any series butdepends very largely upon accurate diagnosis andprompt treatment.
9. Follow-up in this series is incomplete, but itis suggested that following ectopic gestation apatient stands one chance in three of becomingpregnant again, and in one in ten of these sub-sequent pregnancy will be ectopic.
I wish to thank the consultant staff of theMiddlesex Hospital for permission to report thisseries of cases and especially Mr. F. W. Roquesand Mr. W. R. Winterton for allowing me to quotetheir case previously reported and for their in-terest in this paper.The illustrations are the work of Miss E. D.
Hewland and Mr. T. E. Cowan and were preparedfor publication by Mr. M. Turney. To these alsoI wish to express my thanks.
BIBLIOGRAPHYATLEE, H. B. (I947), Canad. med. Ass. J., 56, 268.BAIRD, D. (1950), 'Combined Textbook of Obstetrics and
Gynaecology,' Livingstone, Edinburgh.BEACHAM, W. D., et al. (1948), J. Amer. med. Ass., 136, 365.BLUMBERG, E. F. (I947), Med. Pr., 2I8, 399.BUSS, T. ST. V., et al. (I950), S. Afr. med. 7., 24, 664.CULLEN, T. S. (I 9 I 8), Amer. 7. Obstet. Dis. Wom., 78, 457.DECKER, A. (I947), Amer. 7. Surg., 73, 313.DRAA, C. C., and BAUM, H. C. (I9si), Amer. Y. Obstet. Gynec.,
6I, 300.
EASTMAN, N. J. (I950), 'William's Obstetrics,' ioth edition,Appleton-Century-Crofts Inc., New York.
ECHOLS, C. M. (I934), 7. Amer. med. Ass., I03, I686.FALLS, F. H. (i950), Surg. Clin. N. Amer., 30, 207.GIOANNI, L., and WIRTZ, L. (I949), Rev. franc. Gynec., 44, 288.GOLDBERGER, M. A., et al. (I934),J7. Amer. med. Ass., 103, 12I0.INGRAHAM, H. C., et al. (I949), N.Y. St. 7. Med., 49, i562.LEFF, B., and WINSON, S. G. (I947), Amer. 7. Obstet. Gynec.,
53, 296.MASANI, K. M. (I949), 'Ectopic Pregnancy,' Popular Book
Depot, Bombay.NICODEMUS, R. E., and CARRIGG, L. G. (1940), Amer. J7.Obstet. Gynec., 39, 153.NIELSEN, B. (1947), Acta radiol. Stockh., 28, I85.PARRY, J. S. (I876), 'Extra-uterine Pregnancy,' London.POMMERENKE, W. T. (I936), Amer.Y. Obstet. Gynec., 3I, 65o.ROMNEY, S. L., et al. (i950), Surg. Gynec. Obstet., gi, 605.ROQUES, F., and WINTERTON, W. R. (I937),J7. Obstet. Gynec.
Brit. Emp., 44, 687.SCHAUFFLER, G. C. (1945), West. Y. Surg., 53, 301.SCHUMANN, E. A. (1921), 'Extra-uterine Pregnancy,' D.
Appleton & Co., New York.SIEGLER, S. L. (I945), N. Y. St. _. Med., 45, 1974.SUTER, M., and WICHSER, C. (1948), Amer. J. Obstet. Gynec.,
55, 489.TAIT, R. L. (I888), 'Lectures on ectopic pregnancy and pelvic
haematocele,' Birmingham.WAY, S. (1949), Y. int. Coil. Surg., 12, 550.WHITACRE, F. E., and BRYAN, T. (1949), 7. med. Ass. Ala.,
z8, I
NOTE: In the article by R. S. Smith published in June, 1953, entitled 'Searching the MedicalLiterature' it was stated that the latest volume indexes to appear for the Abstracts of World Medicinewere those for 1950. In fact, the indexes for 195I had already appeared. We regret this error and theEditor of Abstracts of World Medicine states that it is his aim to reduce the delay in publishing theindexes still further.
copyright. on 10 M
ay 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.334.405 on 1 A
ugust 1953. Dow
nloaded from