Embed Size (px)
Citation preview

Echocardiographic Evaluation of Congenital Mitral Valve Anomalies in Children
Anirban Banerjee, MD, Thomas Kohl, MD, and Norman H. Silverman, MD
Con enital mitral valve anomalies were diagnosed in 3, 65 c ildren, whose ages ranged from newborn to 18
years, using 2-dimensional, color, pulsed-, and contin- uous-wave Doppler ultrasound. Data were collected over 7.5 years from 13,400 new studies. Data in these patients were compared with those obtained by car- diac catheterization, cardiac surgery, and autopsy. We detected 4 different lesions: (1) congenital mitral steno- sis with 2 papillary muscles (n = 24); (2) parachute mitral valve, with a single papillary muscle (n = 24); (3) isolated cleft in the mitral valve (n = 10); and (4) double-orifice mitral valve (n = 7). A supravalvar mitral ring was detected in 21 patients with mitral stenosis; however, it never occurred as an isolated lesion and was invariably associated with some other left ventric- ular inflow or outflow obstruction. The supravalvar rin was associated with a pamchute deformity of the mitra 9 valve in 17 patients; in only 4 was this abnormality associated with mitral stenosis with 2 papillary mus- cles. In patients with congenital mitral stenosis, the peak
and mean transmitral Doppler velocities were increased si
9 nificantly compared with those in controls (peak
ve ocity 1.53 + 0.74 vs 0.86 f 0.25 m/s, respectively, p 4.01; mean velocity 1.13 f 0.61 vs 0.58 ?: 0.11 m/s, respectively, p ~0.01). The correlation between mean transmitral pressure gradient obtained by Dop- pler and cardiac catheterization was fair (r = 0.75). However, the correlation between the mitral valve areas calculated by the Doppler pressure half-time method and by the Gorlin formula was poor (r = 0.57). Eleven of the 24 patients with pamchute mitral valve defor- mities had Doppler evidence of an increased transmi- tral gradient. In children, echocardiogmphy proved su- perior to cineangiography as a diagnostic modality, and can be relied upon in making management deci- sions, but Doppler velocities, including pressure half- time, applicable in adults for calculation of mitral valve area are unreliable.
(Am J Cardiol 1995;76:1284-1291)
C ongenital mitral valve abnormalities constitute a wide spectrum of cardiac malformations that are rare in
children. Congenital mitral stenosis, an important com- ponent of this group, was detected in 1.2% of autopsied patients with congenital heart disease’ and in 0.42% of all cardiac patients.* Earlier descriptions were based on clinical reports and pathologic specimens’.‘,“; however, high-resolution echocardiography has facilitated the diagnosis.5--x The Doppler techniques used in adults9**0 to calculate diastolic pressure decrease across the mitral valve and mitral valve area have not been validated in children. We therefore undertook the present study to define the spectrum of such malformations in children, correlating our echocardiographic findings with data from cardiac catheterizations, direct surgical observa- tions, and autopsy specimens.
METHODS Between January 1985 and June 1992, a total of
13,400 new patients underwent echocardiographic eval- uation at the University of California, San Francisco. Six- ty-five (35 boys and 30 girls, age range newborn to I8 years) were diagnosed with at least I form of congenital mitral valve abnormality. We reviewed medical records,
From the Cordiovascu!ar Research lnstrtute and the Department of Pedratrics IJniversity or California, San Francisco, San Francisco, Cnlrfarnio. This study was supported in part by Research and Train- ing Grant H107.544 from the National Institutes of Health, Bethes- da, h’wyiand, and a research fund from the Devtsche Forschungs gemeinschaft. Bonn, Germany. Manuscript received May 30, 1995; revised manuscript received and accepted August 3 1, 1995.
Address far reprints: Norman H. Silverman, IvID, Box 02 14, M- 342A. Uni~versity of California, San Francisco, San Francisco, Cali- farnin 94 143-02 14.
echocardiograms, cardiac catheterization studies, surgi- cal reports, and autopsy specimens. Fifteen normal chil- dren matched for age and size served as controls for the congenital mitral stenosis group, allowing comparison of Doppler velocities across the mitral valve.
The mitral valve abnormalities found and evaluated in this study were: (1) congenital mitral stenosis. (2) para- chute mitral valve, (3) isolated cleft in the mitral valve, and (4) double-orifice mitral valve. Patients were exclud- ed from this study who had mitral valve prolapse, car triatriatum, hypoplastic left heart syndrome, or abnor- malities of the left-sided component of the atrioventric- ular valve in atrioventricular septal defects. Isolated mitral regurgitation without an obvious abnormality of the mitral valve was excluded. Also excluded were pa- tients with univentricular atrioventricular connections and those with congenitally corrected transposition of the great arteries demonstrating abnormalities of the left atrioventricular valve.
Over a 75year period, all children in our series un- derwent a complete echocardiographic examination, in- cluding 2-dimensional echocardiography, M-mode, pulsed-, and continuous-wave Doppler studies using a variety of commercially available scanners with trans- ducers appropriate for patient size. The Doppler color flow modality was added in 1986. Two-dimensional imaging was performed using standard echocardio- graphic planes from the parasternal, apical, subcostal, and suprasternal windows. All studies were recorded on videotape. The peak and mean Doppler velocities were measured for calculating peak and mean transmitral pressure gradients. We also calculated the mitral valve area from the Doppler signal using the pressure half-time
1284 THE AMERICAN JOURNAL OF CARDIOLOGY’ VOl 76 DECEMBER 15, 1995

methodlo: mitral valve area (cm*) = 220/PHT, where 220 is a constant that corresponds to a mitral valve area of 1 cm*, and PHT is the pressure half-time (ms).
Cardiac catheterization and cineangiography were performed in 56 of the 65 patients with congenital mitral valve abnormalities. Doppler data recorded either on the day before or within 1 month after catheterization were used for comparison. Based on an earlier study,6 the severity of mitral stenosis was classified as mild, mod- erate, or severe. A peak transmitral gradient of 8 to 10 mm Hg was considered mild, 11 to 15 mm Hg moder- ate, and >15 mm Hg severe mitral stenosis. We adopt- ed this classification with reservations, because in chil- dren, a high transmitral pressure gradient may not be generated, even in the presence of severe mitral stenoses, because of a frequent association of atria1 communica- tion or multiple levels of left-sided obstructions.1~11-14
The mitral valve area could be calculated from the revised Gorlin formula in 12 patients undergoing cardiac catheterization.rs*r6
Of the 65 patients, 58 underwent a form of cardiac surgery. Some of these were palliative or unrelated to the mitral valve (e.g., coarctation of aorta). The valvar structure and support apparatus were confirmed by direct visualization by the surgeon in 29 patients with mitral valve abnormalities. Mitral valve morphology was con- firmed from pathologic specimens from 7 patients.
Statistical analysis: Doppler velocity data are pre- sented as mean f SD. The effective mitral valve orifice and Doppler velocity data obtained from the group of patients with congenital mitral stenosis were compared with the control group by unpaired Student’s t test. A p value <0.05 was considered statistically significant. A least-squares linear regression analysis was performed between (1) the transmitral gradient obtained by Doppler
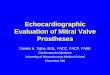
FIGURE 1. This magnified apical d-chamber view (A 4 Ch.) was obtained from an adolescent female with congenital mitral stenosis associated with 2 papillary muscles. In this end-dias- tolic frame, the mitral vahfe can be identified between the left atrium (LA) and left ventricle (LV)..The mitral valve and support apparatus appear thickened. In addition, there is a false ten- don (arrow] attached from the papilla I = inferior; 1 = left; R = right; RA = rrg 3
muscle to the septum.
ventricle; S = superior. t atrium; RV = right
TABLE I Classification of 65 Patients With Congenital Mitral Valve Anomalies
Mitral Valve Anomaly
isolated congenital mitral stenosis
(excluding parachute mitral valves) Parachute mitral valve
Complete Shone’s complex Incomplete Shone’s complex
lsoloted cleft in mitral valve
Double-orifice mitral valve
Patients (%)
24 (37)
24 (37) 10 (15) 14 (22) 10 115)
7 1111
measurements and that obtained by cardiac catheteriza- tion, (2) the mitral valve area obtained from the Doppler pressure half-time method and from the Gorlin formu- la, and (3) the peak transmitral gradient obtained by car- diac catheterization and mitral valve areas calculated by the Gorlin and pressure half-time methods.
RESULTS Of 13,400 new echocardiograms, 65 patients had at
least 1 form of congenital mitral valve abnormality, an incidence of 0.49% (Table I).
Congenital mitral stenosis (with 2 papillary muscles): Congenital mitral stenosis was diagnosed in 24 patients (37%); our incidence was 0.18% in all new patients undergoing echocardiography in our laboratory. Hemo- dynamic evaluation by cardiac catheterization was per-
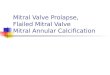
FIGURE 2. This continuous-wave Doppkx signal was obtained from a neonate with severe congenital mitral stenosis requiring valve replacement. The early E wave is lower than the subse- quent A wave. The heart rate is 126 beats/min, and there is little time for decoy of the venous filling before atrial controc- tion occurs.

formed in 14 of these 24 patients (58%), and the modi- fied Gorlin formula could be applied in 12 of them. Car- diac catheterization showed that 8 patients had mild, 3 moderate, and 3 severe mitral stenosis, which was sub- sequently confirmed during surgery in 11 patients and during autopsy in 3.
The mitral valve leatlets appeared thickened and dys- plastic in 14 of the 24 patients (58%) with congenital mitral stenosis. The leaflets appeared echo-dense, moved poorly, and domed during diastolic filling of the left ven- tricle (Figure 1). The subvalvar mitral apparatus had a similar echo-dense, crowded appearance in all patients with congenital mitral stenosis. The morphology and
FIGURE 3. Top, Dop increased velocity 2
er color flow mapping evidence of blood flow across a sknosed mihal valve.
Mtom, 4-chamber reference ima color flow map was generated. Ar
from which the Doppler breviations OS in Figure 1.
movement of the mitral valve were best visualized in the parastemal long-axis view, whereas the subvalvar appa- ratus was best visualized from the apical and subcostal 4-chamber views.
The peak Doppler velocity obtained in these patients had a mean value of 1.53 + 0.74 m/s (range 0.82 to 3.65), which was higher than that obtained in the control group (0.86 + 0.25 m/s, p ~0.01) (Figure 2). The mean Doppler velocity was also significantly higher in patients with congenital mitral stenosis (1.13 f 0.61 vs 0.58 + 0.11 m/s, p ~0.01). In some patients, the increased Doppler veloc- ity was well defined by Doppler color flow mapping (Fig- ure 3). The peak transmittal gradient obtained by Doppler showed a poor correlation with the peak gradi- ent between left atrial A wave and left ventricular end- diastolic pressures at catheterization (r = 0.56, SEE + 7.67). The correlation between the mean Doppler gra- dient and the mean transmitral gradient at catheteriza-
Mean Doppler Gradient (mm Hi9
7 1
30 1 0 /
25.
20
15
10 : / 0
5
0
n=13 r = 0.75 y=l.l8x-8.03
0 5 10 15 20 25 30 35
Mean Catheterization Gradient (mm Hg)
FIGURE 4. Correlation between mean fransmilral pressure ra- dients derived from Cardiac catheterization and from Do & r echocardiogmphy. y = 1.18x -8.03.
N am-Doppler (;I9
I 4
0
3.5.
3.
2.5.
2.
1.5.
1. n= 12 Q 0.5 . 0 r 0.57 =
, y = 0.61x + 1.17 04 .
0 0.5 1 1.5 2 2.5 3 3.5 4
Mv area-Gorlii
(cm2)
FIGURE 5. Correlation between mitral valve (Mv) areas calcu- lated from Ihe Gorlin formula and by Doppler pressure half- time method.
1286 THE AMERICAN JOURNAL OF CARDIOLOGYz VOL. 76 DECEMBER 15, 1995

tion was better (r = 0.75, SEE + 5.4) (Figure 4).
TABLE II left Heart Obstructive lesions Associated With Congenital Mitral Volve Anomalies*
The mitral valve area derived bv the Doppler pressure half-time metho& 2.9 PMV ICMV DOMV
+ 1.4 cm*, correlated poorly with that left Heart Obstructive Lesions (n ??4] (n = 24) (n = 10) (n = 7)
derived from the Gorlin formula, 1.54 Supravalvar mitral ring 4 (16.7) 17 (70.8) -
f 0.8 cm* (r = 0.57, SEE +: 0.85) (Fig- Subvolvar aortic stenosis 8 (33.3) 9 (37.5) -
ure 5). Mitral valve areas calculated Bicuspid oortic valve 4 (16.7) 6 (25) - -
from both the Doppler pressure half- Volvar oortic stenosis 5 (20.8) 5 (20.8) Aortic arch hypoplosia 2 (8.3) 8 (33.3) 2 (20.0) 2 (28.6)
time method and the Gorlin method Coarctotion of oorto 6 125.0) 11 (45.81 1 (10.01 2 (28.6)
also showed poor correlations with the Aortic interruption - 3 i12.5j ‘- ‘-
peak transmitral pressure gradient de- *More than I such lesion can be associated with a congenital mitral valve anomaly.
rived by catheterization (r = 0.30 and Values ore expressed as number (96).
0.48, respectively, SEE f 1.1 and + 0.9, DOMV = double-orifice mitral valve; ICMV = isolated cleft in mitral valve; MS = congenital mitral
stenosis; PMV = parachute mitral valve.
respectively) (F&re 6A and 6B). I
_ . Parachute mitral vahre: A parachute mitral valve was
detected in 24 patients (37%). A single papillary mus- cle in the left ventricle, a hallmark of this lesion, was identified in the parastemal short-axis, apical 4-chamber, or subcostal sagittal plane, usually in the position of the posteromedial papillary muscle (Figure 7). The mitral valve leaflets appeared dense and demonstrated restrict- ed motion in most patients. Two patients had 2 very closely positioned papillary muscles, constituting a par- tial type of parachute deformity of the mitral valve.3v7.1s
A parachute mitral valve was frequently associated with other left heart obstructive lesions, such as supraval- var mitral ring, abnormal and stenosed mitral valve, subaortic stenosis, and coarctation of the aorta, thus con- stituting either a complete form of Shone’s complex (when all 4 components of the complex were present) or an incomplete form (when fewer components were present) (Tables I and II). A concomitant supravalvar mitral ring was recognized in 71% of patients with a parachute mitral valve deformity in our series, making it the most frequently detected left heart obstructive lesion in the presence of a parachute mitral valve.
The peak and mean Doppler velocities across the mitral valve were increased in 11 patients with parachute mitral valve compared with those in the control group (peak velocity 1.35 f 0.24 vs 0.86 + 0.25 m/s, respec- tively, p cO.05; mean velocity 0.98 f 0.21 vs 0.58 + 0.11 m/s, respectively, p ~0.05). Doppler color flow mapping was not helpful in defining this lesion, but showed evi- dence of flow disturbance.
Seventeen of the 24 patients underwent cardiac catheterization; a significant transmitral gradient was detected in only 14 (58%). In 3 of these patients, despite the fact that a transmitral grsdient was detected at catheterization, no gradient was detected by Doppler echocardiography. The single papillary muscle was detected by cineangiography in only 7 of the 24 patients (29%). The mitral valve apparatus was commented on in 10 surgeries and 2 autopsies (1 of the autopsies was performed in a patient who previously had undergone an operation) in which the presence of a parachute mitral valve was confirmed in all patients during surgery and
7) and apical 4-chamber views. The attachment of the membrane was within 1 to 3 mm of the mitral valve annulus on the atria1 surface of the mitral valve, with the membrane of the supravalvar mitral ring prolapsing into the mitral valve orifice during diastole. The left atria1 appendage was visualized in 9 of 21 patients (43%). The supravalvar ring was always proximal to the appendage, in contradistinction to car triatriatum. An isolated supra- valvar mitral ring was not detected in any patient: it was
4.5 A 1 0 n= 13
4, 0 r = 0.30 = -0.07x + 3.08 3.5 y
3,
2.5
2.
1.5
1. 0
0 0.5, 0
01 . . . . . . . . 4 0 2 4 6 6 10 12 14 16 18 20
Peak Catheterization Gradient (mm Hg)
B 4 3.5
0 n= 12 r = 0.48 y=a.lx+2.74
Ol 0 2 4 6 8 10 12 14 16 16 20
Peak Catheterization Gradient (mm Hg)
autopsy. Supravahrar mitral ring: A membranous supravalvar FIGURE 6. Correlation between transmitral pressure gmdient
mitral ring was recognized in 21 of 65 patients (31%) derived from cardiac catheterization and [Aj mitral v&e.(MV)
with mitral valve abnormalities in our series. This mem- area calcukted by the Doppler pressure half-time method ( -0.07x + X08), and (8j mitral valve area calculated from x
= e
brane was best seen in the parastemal long-axis (Figure Goblin formula (n = 12, r = 0.48, y = -0.1x + 2.74).
CONGENiTAl HEART DlSEASF./CONGENITAL LITRAI VALVF ANOUAIIES 1287

invariably associated with 21 component of Shone’s complex, thereby constituting a complete or incomplete form of this comp1ex.n A parachute mitral valve was often associated with a supravalvar mitral ring, and was detected in 17 of 21 patients (81%). A stenotic mitral valve with 2 papillary muscles was associated with a supravalvar mitral ring in 4 patients (19%).
In only 2 of 21 patients (10%) with a supravalvar mitral ring, the ring itself caused a significant obstruc- tion that was detected by Doppler echocardiography and subsequently confirmed by catheterization. In the remaining patients, the ring itself appeared to cause no additional obstruction. Doppler color flow mapping showed evidence of color flow convergence toward the center of the supravalvar mitral ring and valve.
isolated CM of m’hral valve: Isolated clefts in mitral valve, unassociated with atrioventricular septal defects, were detected in 10 patients (15%) in our series. The clefts were detected exclusively in the anterior leatlets of the mitral valves. The parastemal short-axis or equiv- alent subcostal view at the level of the mitral valve leaflets, which also shows the left ventricular outflow tract, effectively identified the cleft in the anterior leallet (Figure 8). In all 10 patients, the cleft in the anterior leaflet pointed to the left ventricular outflow tract in con-
stenotic mitral valve leadin stenotic orifice of the mitra
be the posteromedial
1288 THE AMERICAN JOURNAL OF CARDIOLOGYm VOL. 76 DECEMBER 15, 1995

tradistinction to the so-called “mitral valve clefts” found in atrioventricular septal defects, which point toward the ventricular inlet septum.
No patient had evidence of an atrioventricular septal defect. However, in 2 patients, attachment of chordae tendineae arising from the margins of the cleft to the ventricular septum created left ventricular outflow tract obstruction. Doppler color flow mapping showed evi- dence of mitral regurgitation through the cleft in 9 patients (Figure 8, bottom right), which was severe in 4. The isolated cleft in the anterior mitral leaflet was sur- gically repaired in these 4.
Of the 10 patients with isolated cleft of the mitral valve, 6 underwent cardiac catheterization. Although mitral regurgitation was detected in all patients, the actu- al cleft in the anterior leaflet was visualized in only 1 patient by cineangiography.
Doubk-orifke mahi v&e: Double-orifice mitral valve was an uncommon lesion, detected in 7 of 65 patients (11%) with congenital anomalies of the mitral valve. The short-axis plane at the level of the annulus was best for detecting this lesion (Figure 9). This feature was also evident in subcostal coronal and sagittal views, and in apical 4-chamber views. In 3 patients, both orifices were of equal size, whereas in the others they were of unequal size; the smaller orifice was often located in the antero- lateral part of the left ventricle. In the 7 patients with double-orifice mitral valve, the mitral valve annulus was small in 3. Mitral regurgitation was noted in 2 patients. A type 1 truncus arteriosus lesion was noted in 1 patient, 2 patients had Down syndrome, and another had the
FlGURE 8. This figure demonstrates the features of cleft mitral volve. Tap w, o subcostol sagittal view from o patient with trons- position of the
lei reat arteries and ventricular septal defect with a cleft in the mitral volve. lhe puknana ventricle (LV). The cl& in the anterior mitrol vohre lea&t &mo/I 4-1 is seen, as is
ottery (PA) is seen oris- mg from the xe chordal attachment ta the ventricular septum (large arrow]. Thus, the mitral volve leaflet assumes 0 hileaflet co&gurotion. Top * hf, 0 modii
mstemol short-axis view (P S Ax.) demonstrotin lztwee i#l
the cleft in the anterior leofletofthe mitral valve lsmo QITOWSJ, lying “w n the left atrium (IA) and the left ventricle. e left atria1 o pfydoqe (*) IS indicated by on amow. Bottom hvrmes from 0
d&rent patient with a cleft mitral volve token in the pamstemol s ott-axa wew. Arrows indicate the position of the cleft ot end- stole.
7 6ot/rxn right fiome, the same early systolic frame with superimposed color mop defines mitral regurgitation thraugh the
c eft. Other abbreviations as in previous figures.
CONGENITAl HEART DISEASE/CONGENITAL MITRAI VAIVE ANOMALIES 1289

r k6l.E III Cardiac Malformations Associated With Mitral Valve Abnormalities*
PMV ICMV DOMV
Associated Cardiac Malformations (n ??4] (n = 24) (n = 10) b = 7)
Ventricular septal defect 10 (41.7) 12 (50.0) 4 (40.0) 4 (57)
Double outlet right ventricle 4 (16.7) 2 (8.3) 1 (10.0) -
D-transposition 2 (8.3) 3 (12.5) 1 (10.0) -
Tetralogy of Fallot 1 (4.2) 1 (4.2)
Pulmonary stenosis 3 (12.5) 4 (16.7) 1 (10.0) 1 (14.3)
Truncus arteriosus left SVC/cardinal vein 4 (16.7) 5 (20.8) 1
1 (14.3) 2 (28.6)
*More than 1 such lesion can be associated with o congenital mitral valve anomaly. Values are expressed as number (%). SVC - superior vena cove; other abbreviations as in Table II.
CHARGE association. The left heart obstructive lesions associated with double-orifice mitral valve were seen in 2 patients with tubular hypoplasia of the aortic arch and in 2 with coarctation of the aorta (Table II).
Associated cardiac lesions: One or more left-sided obstructive lesions were often associated with congeni- tal mitral valve anomalies (Table II). Various cardiac malformations also coexisted either singly or in combi- nations in patients with congenital mitral valve ailom- alies (Table III).
DISCUSSION In this study, we have described the spectrum of con-
genital mitral abnormalities in the pediatric population by echocardiography, and compared these observations with cineangiographic, surgical, and postmortem de- scription of these lesions. The advantages of echocardi- ography over cineangiography are the clearer demon- stration of thickening of the valve cusps and chordal attachments, better visualization of papillary muscles and interpapillary spaces, and better appreciation of the mobility of the valve leaflets.
Congenital mitral stenosis: The incidence was 0.18% in patients undergoing echocardiography in our labora-
FIGURE 9. A pasternal short-axis view (P S Ax.) of a patient with a double-orifice mitral valve. In this patient, both of the orifices (MVOl and MVO2) were of approximately equal size. A = anterior; P = posterior; other abbreviations as in Figure 1.
tory compared with a 0.42% incidence in patients with congenital heart dis- ease quoted in an earlier clinical series.2 This may well relate to many patients admitted to our laboratory who do not have structural heart disease. The continuous-wave Doppler veloci- ty was often not significantly elevated in patients with congenital mitral steno- sis because of an atrial communication or the masking effect of an associated coarctation.nJ3
Whereas in adults the mean trans- mitral Doppler gradient showed a good
correlation with mean transmitral pressure gradient,Y only a fair correlation (r = 0.75) was found in our series of children. Because the 2 gradients represent 2 differ- ent phases of diastole, they should not be compared. Studies performed in adults in normal sinus rhythm have shown that the mitral valve area calculated by the Dop- pler pressure half-time method had a good (r = 0.95) to fair (r = 0.73) correlation with the mitral valve area cal- culated from the Gorlin formula.‘x18 The correlation between the 2 methods was poorer in our study (r = 0.57). Because the mitral valve area calculated by the Gorlin method and by the Doppler pressure half-time method were compared with each other, no attempts were made to correct the mitral valve areas for body sur- face area. The poor correlation may be due to several reasons. First, this was a retrospective study, with mea- surements not performed simultaneously. Such nonsi- multaneous correlation has been good in earlier stud- ies.1s-20 Second, the pressure half-time of 220 ms was chosen arbitrarily in adults because it correlated well with a critical mitral valve area of 1.0 cm2.10 It appears that in children, where mitral valve areas are small and heart rates rapid, the same relation as that used in adults is not applicable. Based on a simple mathematic model, it has been shown that the pressure half-time depends not only on mitral valve area, but also on left atrial and ventricular compliance and peak transmitral pressure gradient. 21 In young infants the E- and A-wave ratios in the mitral valve Doppler waveform are different from those noted in older children and adults, and may reflect altered atrial or ventricular compliance (Figure 2), and alter the assessment of transmitral pressure gradient in children, or valve area by Doppler techniques. Third, the mitral valve area calculated from the Gorlin formula has been noted to be less reliable at faster heart rates,22 as it would be in infants who normally have rapid heart rates, and in those who may have additional communications or obstructions.
Echocardiography was superior to cineangiography in diagnosing a parachute mitral valve (the latter suc- ceeding in only 29% of patients), whereas Doppler evi- dence of mitral stenosis was detected in only 11 patients. Only 1 patient in our series had tetralogy of Fallot with right ventricular obstruction.1*23
Supmvahrar mitral ring: The 31% incidence of supra- valvar mitral ring in this echocardiographic series was slightly higher than a 17% to 19% incidence noted in earlier studies of congenital anomalies of the mitral
1290 THE AMERICAN JOURNAL OF CARDIOLOGYe VOL. 76 DECEMBER 15. 1995

valve.‘.3 On echocardiography, a supravalvar mitral ring is characterized by a membrane-like structure that is fre- quently adherent to the atrial surface of the mitral valve leaflets and is often detected in diastole during slow, frame-by-frame advance of the videotape.‘4 A supraval- var mitral ring may be missed on 2-dimensional echo- cardiography if it is not actively sought.
In this study. surgical resection of the supravaivar mitral ring was performed in only 2 patients, indicating that the ring, per se, did not cause significant obstruc- tion in most patients. This lack of obstruction can be explained by the frequent presence of an atria1 commu- nication, but also implies that the opening in the supra- valvar mitral ring is often large and unobstructive.“.2s
l&ted deft in the mitral valve: As noted in previous studies,26q’7 cineangiography often failed to diagnose a cleft in the mitral valve, which was clearly shown by echocardiography and later substantiated during surgery. In keeping with previous reports,z8q29 we noted that in true isolated cleft in the mitral valve, the cleft points toward the left ventricular outflow tract.
The left ventricular outflow tract obstruction noted in 2 patients in our series may be caused by insertion of the accessory chordae to the ventricular septum. and was noted to be most severe if the chordae inserted into the ventricular septum just beneath the right aortic CUSP.~~ The left ventricular outflow tract obstruction appears to be the result of tethering of the anterior mitral leaflet caused by the accessory chordae attached to the ven- tricular septum.z6,30
Double-orifice mitral vahre: Double-orifice mitral valve is an uncommon mitral valve lesion found in 1% of autopsied cases of congenital heart diseasea3’ This anom- aly has been described by morphologists to be of 2 types: 1 type is associated with atrioventricular septal defects and is caused by a fibrous tissue “bridge” across the mitral valve orifice: the other type is caused by redupli- cation of the orifice, with each suborifice supported by its own tension apparatus.3’q32 We believe that these 2 types cannot be distinguished echocardiographically. Mild mitral stenosis and mitral incompetence noted in some patients with double-orifice mitral valve were not significant enough to warrant surgical repair. A rare com- bination of a double-orifice mitral valve with a truncus arteriosus type 1 was found in 1 patient.‘”
Study limitation: An anomalous mitral arcade. a rare lesion of the mitral valve, first described pathologically and subsequently by echocardiography.6.34 was not de- tected in our echocardiographic series.
1. Collins-Nakai RL. Rosenthal A. Castaneda AR. Bernhard WF. Nadas AS. Con- genital mitral stenosis. A rwicw of 20 years’ experience. Cirwluriot~ 197756: 1039-1047.
2. Nadas 4s. Fyler DC. Pediatric Cardiology. 3rd cd. Philadelphia: WB Saunders. lY7?:683~,87. 3. Davachi F. Moller JH. Edwards JE. Diacascs of the mitral >alw in ~nlhncy. ,An anatomic analysi% of 5.5 cases. Circularion 197 1:43:565-579. 4. Ruckman RK. Van Praagh R. Anatomic types ofcongenital mitral srenosis: rcpwt of 49 autopsy casts with consideration of diagnosis and surgic;tl implications. Ant J Cordial lY78;42:S92-601. 5. Snider AR. Rage CL. Schiller NB. Silwrman NH. Congenital left ventricular inflw obstruction evaluated hy two-dimensional cchwardiography. Cirwlarit~~r
lYXO:hl :X-%X55. 6. Grenadier E. Sahn DJ. Valdes-Crw I.M. Allen HD, Oliveira Lima C. Goldberg SJ. Two-dimensional echo Doppler study of congenital disorders of the mitral valw Am Hew? .I 19X4:107:3 19-32.5. 7. C&no V. Pieroni DR. hlorera IA. Roland JM. Gingell RL. Two-dimensional
echocardiogrephic examination of mitral valve ahnonnalitius associated with COLIC- tatton of the aotta. Cirw/crfiorr 19X4:69:924-932. 8. Smallhorn J. ‘Tommasini G. Deanfield J. Douglas J. Gibson D. Macannry F. Congenital lmiwal sIcnosis. r\natomical and functional asesmcnt hy cchocardiog- lraph). Br //~wr-r J I% I :1S:S??-S33. 9. Harle L. Brubakk A. Trom\dal A. Anpelsrn B. Noninvasive assessment of pres- sure drop m Intilml wnosis h> Doppler ultrasound. tlr Heurt J 1978:40:131-140. 10. Hatle 1.. Angelsen B. Tromsdal A. Noninvasive assessment of atrioventncular pressure half-tune hy Doppler ultrasound. C‘i,ruhrion 1979:ti IO96 I 104.
11. Shone JD. Sellers RD. .Andrruon RC. Adams P Jr. Lillehei CW, Edwards JE. The dewlopmrntal complex of “parachute mitral val\e” wprawlvular ring of left atrium. ruhnortic blenubis and coarctation of aona. Am J Curdiol lY63:l I :7 11725. 12. Ri_rg? TW. Lapin GD. Paul \lH. Muster Al. Ben) TE. ~~easurement of mitral \alve orifice arca in Infants and children h> two-dimensional rchtrardiopraphy. J Am Co11 (‘urdiol 19X.3: I :X7.:-X7X. 13. Rownquist GC. Congcnilal mitral valve disease assxiated with coarctation of the aorta. A spectrum that includes parachute deformity of the mitral v&e. Circu- kUiO,l I Y74:JY:9X5-9Y3. 14. .Iloore P. Adatta I, Spevak PJ. Kcanc JF. Per? SB. Casraneda AR. Lock JE. Severe wngunitnl mitrill ‘itenohis m infants. C‘inxdafron 1994:R9:209’-?I06 15. Gorlin R. Gorlin G. Hydraulic fommula for calculation of the area of the stcnot- ic mimtl \alve. other cardiac valves. and central circulatory shunts. Am Hewn J lY51:4I:I-21). 16. Cohen \lV. Gorlin R. Modified oritice equation for the calculation ot mitral valve are;,. Am Hewf J 1972:X4:839-840. 17. Gowale~ MA. Child IS. Kri\okapich J. Compariwn of two-dimensional and Doppler cchocanliography and Intracardiac hemod~namica for quantitication of mitral ,tcnosis. A~I .I C’wdiol lYX7:60:327-3.Q 18. Smith MD. Wsrnhauph T . Gra!hurn PA. Curlry JC. Spain MG. DrMaria AN. Value and limiutions of Doppler prebaure half-time in quantifying mitral atmosis: a compariwn with mtcrtm~anomcter catheter recordings. Atrr Ifearf J 1991: I2 I : 48k-MX. 19. Smith MD. Handshoe R. Hand\hw S. Kwan OL. DeMaria AN. Comparative accuracy of two-dltnensional cchwardiography and Doppler pressure half-time metho& in asseb.rinp reverity ot mitral stenosis in patients with and without prior cotlllliiyIun)l~lnl). Cirutkotio~r 19X6:73: I I)0 107. 20. Fredman CS. Pcarum AC. Labovitr AJ. Kern MJ. Compariwn of hemody- namic pressure hall-time method and Gclrlin formula x ith Doppler and echocar- diographic determinationa ot mitral val\e arca in patients with comhined mitral stcnosi\ and regurgiution. .4m Heur/ J IOYO:I lY:l21-129. 21. Thomas JD. Weymnn AF.. Doppler mitral pressure half-time: a clinical tool in search of theoretical jub~ificarion. J Am Co11 (bnliol 1987:10:0?3-Y2Y. 22. Kern \IJ. ‘zguim I:. Intetpretntmn ot cardiac palhophysiolopy from pressure u avcfimn analysis: mitral val\e gradients: pan I. (‘&rr Curdirwrw Dicry~ 1992: 26:30X-21 6. 23. Benp .I. Leachman RD. Cooley DA. Klima T . Lufsshanowski R. Supravalvu- lar mitral stenosis ass&ted with tetralo;! of Fallot. A~I J Cordial lY76;37: Ill-II-I. 24. Sullivan ID. Robinson PJ. de LeaI M. Graham TP Jr. Membranous supravalvu- lar mitral #sto\i\: a trcatahle form of congenltnl hean disease. J Am Co/l Cordial 19Xh;X:l5Y-164.
25. Jnuohstein MD. Hirachfeld SS. Concealed leti atria1 membrane: pitfalls in the tl~agnost\ (II‘ <‘or tristriatum :md ~upra\alvr mitral ring. :ltn J C~rrdiol 1982;49: 78(&7X6. 26. Di %gni F.. Edward\ JE. Clctt antenor Irallet of the mitral valve with intact repu. A wld~ of 70 ca.,lz?. Am J (‘urdrol lYX3;5 l:YlY-Y26. 27. 51:unney FJ. Bain HH. loneacu Ml. Deverall PB. Scott 0. Angiocardio- praphiclpathologic correlations m congenital mitral salve anomalies. Eur J Ccrrdi- 01 l’J76:4:lY-211. 28. Smallhorn JF. .Tomma\ini G. Anderson RH. \laaartney FJ. Assessment ofatri- wcntricular septal tlcfcct\ h) two dimensional echwardiography. Hr Hem J 1982; -17: IOY-I 2 I. 29. Smallhorn JF. dc la\al \I. Stark J. Somerville J. Taylor JF. Anderson RH. Ilacartney FJ. lwlawd anterw mitral cleft. Tao dimensional echwardiographic assesment and differentiation Itom “clefts” aaswia~ed with atrioventricular septal defect. Hr Hrm-f .I 19X2:4X: 10% I 16. 30. Seller\ RD. Lillehei 0%. Edwards JE. Suhaortic stenosis caused hy anomalies of the atriowntricular val\e\. J T/~oru~~ (‘crrdiovo.w Swg 11)644:4X:2X9-302. 31. Ratio-Kodrigo A. Van Pr:taeh S. Trou iwch E. Van Praagh R. Double-orifice mitral \al\e: a srutl! of 17 postnwnem ca\s\ with dewlopmrntal. diagnostic and ~ul-@I conaidcrationr. ,\III J (‘urdiol IYXX:h I: I .52-l 60. 32. Becker AE. Andrraon RI I. Atrio\cntricular valve IllalfoITlliltions. In: Patholo- gy 01 Coneenital llcwt Disraae. 1st ed. I.ondon: Butterworth. IYXI :1-U&142. 33. L)i Se& F.. I.cw S. Shap~r;~ 11. Kaplinsky E. Double mitral \al\e ortficc. Pedi- (111 (‘lrrdr~d I ‘)X6:6:2 I%? Ii. 34. Parr GVS. Fripp RR. Whitman V. Bharati S. Ixv M. Anomalou\ mitrttl arcade: echoc;lr~lil,Fr;lplllc imd angii~graphic recognition. t’nhrr (irrdir~l 19X3:1: I63-I 65.








![Echocardiographic evaluation of mitral valve regurgitation · Pathological abnormality of any one of these components can lead to MR [Figure 1][3,4]. For instance, MR can occur due](https://img.pdfslide.us/doc/110x75/5fbd982e7e367a27283bfb68/echocardiographic-evaluation-of-mitral-valve-regurgitation-pathological-abnormality.jpg)