Embed Size (px)
Citation preview

ECG Rounds: Pulmonary ECG Rounds: Pulmonary EmbolismEmbolism
Todd RingTodd Ring
Jan 08/04Jan 08/04

CaseCase
• 72 yo male with CLL
• Unwell for 4-5 days with fatigue
• SOB x’s 2 days, abrupt onset, progressively worse
• Denies CP
• Mild respiratory distress
• HR 113 RR 34 BP 135/60 SaO2 85 % RA

CaseCase
• CVS: pulse reg, S1 S2 (wide split) II/VI SEM
• Chest: Clear
• Ext: tender L popliteal fossa
• TNT: 2.8
• D-Dimer: 4.79


BackgroundBackground
• The initial electrocardiographic finding of PE first reported in 1935 was the traditional S1Q3T3
• 21 different ECG manifestations of PE• ECG changes are best seen in those patients with
massive or submassive embolization• Studies have shown that 15% to 27% of ECG
were normal• The most common abnormalities are nonspecific
ST segment-T wave changes with sinus tachycardia

PathophysiologyPathophysiology
• Clinical and ECG changes related to the response of the right ventricle to the PE
• Majority of findings result from the right-sided heart strain patternthe increase in right-sided heart pressures creates an increased right
ventricular afterloadincreased right-sided myocardial wall tensionrapidly dilates, with an increase in chamber size and eventual contractile
dysfunction reduction in right heart cardiac output (ie, a reduction the preload for the left
ventricle) which ultimately produces a decrease in left heart cardiac outputas right-sided ventricular dysfunction worsens, right ventricular infarction
and circulatory collapse may occur

ECG ChangesECG Changes
• Arrhythmia (sinus tach, atrial tach, atrial fib, atrial flutter, PAC)
• Nonspecific ST segment/T wave changes• T wave inversions in the right precordial leads• Rightward QRS complex axis shift and other axis
changes• S1Q3 or S1Q3T3 pattern• RBBB• Acute cor pulomnale defined by S1Q3T3 pattern,
right axis deviation, and RBBB

““Normal ECG”Normal ECG”
• Sinus rhythm between 60 and 100 beats/min• Normal conduction, axis, and P wave, QRS
complex, and ST segment/T wave morphologies
• An entirely normal ECG has been found in approximately 10% to 25% of PE patients• a number of such patients will continue to manifest
a normal ECG during hospitalization

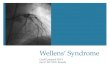
Sinus TachycardiaSinus Tachycardia
• Sinus tachycardia is the most frequent rhythm encountered on presentation to the ED in the patient with PE
• The rate is usually between 100 to 125 beats/min
• Likely related to the physiologic demand to increase cardiac output• as left-sided stroke volume decreases, heart rate must
increase to maintain cardiac output.

Sinus TachycardiaSinus Tachycardia

Atrial TachyarrhythmiaAtrial Tachyarrhythmia
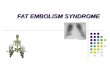
• Primarily atrial fibrillation and atrial flutter, also PAC’s
• Likely results from atrial enlargement

Atrial FibrillationAtrial Fibrillation

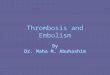
RBBBRBBB • Variable incidence reported 6 – 67 % (25 % often citied)• Transient and often resolves with the restoration of
normal right-sided hemodynamic parameters• May persist ultimately resolving 3 months to 3 years
after the index • New RBBB is suggestive of PE but still nonspecific and
therefore not diagnostic• May also be associated with ST segment elevation and
prominent, upright T waves in lead V1 and/or V2, potentially mimicking anterior or posterior infarct pattern

RBBBRBBB

QRS Axis DeviationQRS Axis Deviation
• Right, left, and indeterminant QRS axis changes n reported in acute PE
• Although right axis deviation (RAD) is described as the classic axis change associated with PE, left axis deviation (LAD) actually occurs more often• may be secondary to pre-existing axis deviation • in the Urokinase-Pulmonary Embolism Trial (UPET), the
investigators report that LAD occurred more frequently than RAD in the PE study population however when those individuals with pre-existing cardiopulmonary disease were excluded, the incidence of LAD and RAD was equivalent

P-PulmonaleP-Pulmonale
• Increase in the P wave amplitude greater than 2.5 mV in lead II
• Classically associated with PE, likely resulting from right atrial hypertrophy or enlargement associated with acute obstruction from clot
• Reported in 2% to 30% of PE patients

P-PulmonaleP-Pulmonale

S1Q3T3S1Q3T3
• Characterized by an S wave in lead I, a Q wave in lead III, and shallow T wave inversions in one or more of the inferior leads
• ST segments may be slightly elevated in the inferior leads
• Although this finding is consistent with right-sided cardiac changes, it remains unclear if this finding actually predicts PE
• The S1Q3T3 pattern is usually short-lived, resolving within 2 weeks after PE

S1Q3T3S1Q3T3
• Mistakenly considered pathognomonic for acute PE by many clinicians
• 15% to 25% of patients ultimately diagnosed with PE have this pattern
• The UPET reveals that approximately 12% of patients with angiographically documented acute PE initially had the electrocardiographic S1Q3T3
• Often considered strongly suggestive for PE when, in fact, poor specificity—approximately 50%—for the diagnosis of PE

S1Q3T3S1Q3T3

S Wave ChangesS Wave Changes
• S wave in lead I greater than 1.5 mm and/or an R wave-S wave ratio greater than 1 in leads I and aVl was noted in 73% of patients diagnosed with PE
• A more subtle finding is a slurred S wave in leads V1 and/or V2.

S Wave in V1S Wave in V1

ST SegmentsST Segments• May be either depressed or elevated • Minimal ST segment depression is a common finding • More pronounced depression may also be
encountered in the anterior, inferior, and lateral distributions• likely represents myocardial ischemia resulting from the
physiologic strain of the PE itself
• The S1Q3T3 pattern may be associated with ST segment elevation in the inferior leads. The RBBB pattern may present with ST segment elevation in the right precordial leads

ST Depression V2-V6ST Depression V2-V6

ST Elevation V2-V5ST Elevation V2-V5

T Wave InversionT Wave Inversion
• Anterior subepicardial ischemia caused by PE manifests as inverted T waves in the right to mid precordial leads (leads V1 to V3)
• Early studies attributed this pattern to coronary insufficiency
• More recent studies suggest either cathecholamine- or histamine-induced ischemia
• Diffuse T wave inversion rarely is diagnostic for PE

T Wave Inversion V1-V4T Wave Inversion V1-V4

Evidence?Evidence?
• Nielsen et al. found 82% of cases of documented had electrocardiographic changes suggestive of acute right ventricular strain. These findings included:• Incomplete right bundle branch block; • S1Q3T3 pattern; • Q wave in lead III; • Inverted T waves in leads III, V2 and V3; and/or• Increase in the frontal QRS axis of >20 degrees.
Nielsen et al: Changing electrocardiographic findings in pulmonary embolism in
relation to vascular obstruction. Cardiol 1989;76:274-284

Evidence?Evidence?
• Sreeram suggests that PE should be considered when 3 or more of the following electrocardiographic changes are encountered:• Incomplete or complete RBBB; • Large S waves in leads I and a VL; • A shift in the transition zone in the precordial leads to V5• Q waves in leads III and aVF (not lead II); • Right-axis deviation; • A low voltage QRS complex in limb leads; and/or • T wave inversion in inferior and anterior leadsSreeram et al.: Value of the 12-lead electrocardiogram at hospital admission in the
diagnosis of pulmonary embolism. Am Cardiol 1994; 73:298-303

Evidence?Evidence?• Petruzzeli et al. studied 21 electrocardiographic abnormalities
in 245 patients with suspected PE—60% of patients ultimately had PE. Those patients diagnosed with PE were found to manifest the following patterns more commonly:• PR segment displacement; • Delayed R wave (lead aVr); • Slurred S wave (leads V1 or V2); • S1Q3T3 pattern; • T wave inversion (leads V1 or V2); and/or • Diffuse T wave inversionsPetruzzelli et al.: Routine electrocardiography in screening for pulmonary embolism. Resp
1986; 50:233-43

Evidence?Evidence?
• Nazeyrolas studied 70 patients with suspected PE and found only an S wave in lead I and Q wave in lead III significantly more common among those with confirmed PEPanos et al. The electrocardiographic manifestations of pulmonary embolism. Emerg Med 1988; 6:301-7

Canadian Evidence?Canadian Evidence?
• Rodger et al. studied the ECGs of 246 patients with suspected PE (49 with PE) comparing the frequency of 28 different ECG findings of PE • only found sinus tachycardia and incomplete RBBB
significantly more common in PE patients• Sreeram's guide of 3 or more findings on the ECG had only a
26.7% sensitivity and 57.1% positive predictive value for PE • the S1Q3T3 pattern was equally prevalent among those with
and without PE
Rodger et al. Diagnostic value of the electrocardiogram in suspected pulmonary
embolism. Am Cardiol 2000; 86:807-9



Fig. 7.