Embed Size (px)
Citation preview
Page 1 of 36
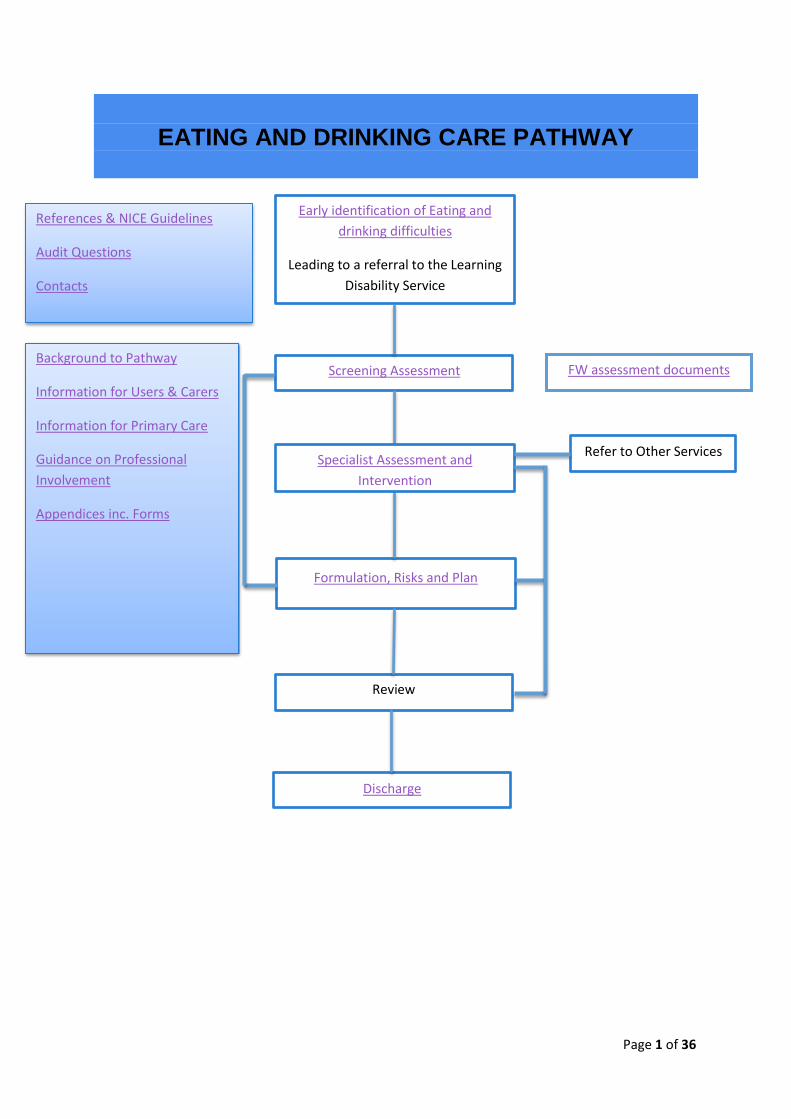
EATING AND DRINKING CARE PATHWAY
Early identification of Eating and
drinking difficulties
Leading to a referral to the Learning
Disability Service
Screening Assessment
Formulation, Risks and Plan
Review
Discharge
References & NICE Guidelines
Audit Questions
Contacts
Background to Pathway
Information for Users & Carers
Information for Primary Care
Guidance on Professional
Involvement
Appendices inc. Forms
Specialist Assessment and
Intervention
Refer to Other Services
FW assessment documents
Page 2 of 36
Page
Section 1: Introduction to the Safe Eating and Drinking Pathway 3
1.1 Care pathway 3
1.2 Definitions 4
1.3 Prevalence 5
1.4 Conditions resulting in dysphagia 5
Section 2: The Safe Eating and Drinking Pathway Process 7
2.1 Early identification of eating and drinking difficulties 7
2.2 Referrals 7
2.3 Foundation worker assessment 8
2.4 Specialist assessment 11
2.5 Formulation and care plan 12
2.6 Evaluation and discharge 13
Section 3: Guidance on professional roles in the Safe Eating and Drinking 14
Pathway
3.1 Competencies and roles 14
Section 4: Information for users and carers 22
Section 5: Audit 23
Section 6: Responsibilities of the care co-ordinator for Safe Eating and 25
Drinking Pathway for an individual
Section 7: Contact list 25
Section 8: Appendices 26
Section 9: Reference list 34
Page 3 of 36
1.1 Care Pathway.
The pathway is particularly based upon guidelines from
NICE guidelines (32) :Nutrition support of adults: Oral nutrition support, enteral tube
feeding and parenteral nutrition (2014)
Ensuring safer practice for adults with learning disabilities who have dysphagia.
National Patient Safety Agency (2007)
Inter Professional Dysphagia Framework Boaden, E. and Davies, S. (2007)
Royal College of Speech and Language therapists Dysphagia and Competency
framework (2014)
Leicestershire Partnership Trust (LPT) policy (2013) : Adult Nutrition and Hydration
Policy for Community Use
In addition the Mental Capacity Act (2005), and Deprivation of Liberty Safeguards (Dols)
(2007) are also key documents. Assessments of mental capacity should be decision and
time specific. These may need to be carried out in relation to any number of decisions for an
individual as appropriate.
The Pathway requires health and social services to work together in a coordinated way so
that there are clear actions at each stage of the pathway. The Care Pathway depends on a
coordinator to oversee the process, be a point of contact, to enable all parties to be involved
in the decision making processes, and to ensure that all information is organised in an
effective way.
Difficulty in eating, drinking or swallowing can lead to malnutrition, dehydration, reduced
quality of life and choking (NPSA). The Pathway aims to assess and minimise risks when
eating and drinking to safety, nutrition and hydration and to ensure an enjoyable eating and
drinking.
This pathway covers recommendations for working with adults with LD who have difficulties
eating and drinking. It does not cover eating disorders or Pica (ingestion of non-edible
objects). The pathway works in relation with other pathways, so is not exclusive.
The Pathway focuses on ways of delivering a service that is:
Fair – equally available to all, taking account of their personal circumstances, culture, and diversity. Personalised – tailored and adapted to an individuals’ needs and preferences and
which includes and involves patients and family and carers throughout assessment
and management.
Effective – delivers evidence based care and outcomes that are valid.
Safe – ensures risks are minimised.
Accountable – through audit and monitoring of outcomes and standards included in the Pathway.
Go back to Pathway
Page 4 of 36
People with eating and drinking difficulties present as a significant population with great
clinical need. The Care Pathway aims to support the service to respond to this need in a
coherent, consistent and effective way. It is strongly recommended that clinicians read this
section before using the Care Pathway.
It is clear that eating and drinking difficulties often have wide ranging personal and social
consequences. These may include: impairing the health and/or quality of life of the
person, those who care for them and those who live or work in close proximity;
isolation, depression and neglect (Emerson 2001).
For example,
A family may have stopped going out for social meals because the person
eats too slowly, or coughs and splutters.
A person’s swallowing difficulties may affect how much medication is taken.
A person may have extreme anxiety about eating because they are aware of
their difficulties.
A person with dysphagia may suffer recurrent chest infections or pneumonias,
causing repeated period of hospitalisation (hospital admissions that shouldn’t
happen)
1.2 Definitions
The terms Eating and Drinking difficulties and dysphagia are often used interchangeably.
Specifically, the term dysphagia refers specifically to swallowing difficulties or swallowing
disorders. Dysphagia is defined as
‘Difficulty in eating, drinking or swallowing. It can lead to malnutrition, dehydration,
reduced quality of life and choking. Asphyxia and respiratory-related mortality are
known to be disproportionately high in people with learning disabilities’. (NPSA 2007)
Eating and drinking difficulties are more commonly defined by the manifestations of the difficulty
‘Some signs and symptoms of swallowing difficulties or dysphagia include the inability to recognise food, difficulty placing food in the mouth, inability to control food or saliva in the mouth, difficulty initiating a swallow, coughing, choking, frequent chest infections, unexplained weight loss, gurgly or wet voice after swallowing, regurgitation, and client complaint of swallowing difficulty’ (NPSA 2007)
Aspiration is defined as the entry of food or liquid into the airway below the level of the true vocal folds. (Logemann 1998). Saliva, refluxed materials and vomit may also be aspirated. Penetration and aspiration can lead to clinical symptoms such as coughing, wheezing, but may be silently aspirated, where no symptoms are apparent. All types of aspiration can lead to chest infections and aspiration pneumonia. Choking is the partial or full occlusion of the airway. Both are usually acute episodes causing anoxia and can require urgent medical attention.
Go back to Pathway
Page 5 of 36
This pathway is holistic and person-centred, addressing all aspects of eating and drinking from preparation and anticipation of the meal to food passing into the oesophagus. It aspires to make the whole drink or mealtime experience as safe, nutritious and enjoyable as possible. It addresses sensory needs, communication, independence and support needs, swallowing, positioning, medication, behaviour and mental and physical health needs with regard to eating and drinking difficulty.
1.3 Prevalence:
Dysphagia is more prevalent in people with learning disability (LD) than normal a population (Heslop et al 2013).The prevalence of eating and drinking difficulties in the UK is difficult to quantify as different studies may include or exclude parts of the eating and drinking sequence. There are limited studies of the prevalence of dysphagia. Estimates range around 8% of the LD population, 40% of whom experience recurrent respiratory tract infections (Emerson et al 2011), and 30% in the hospital-based population of people with LD (Chadwick et al 2006). Leslie et al (2009) quote 36% to 73% of an inpatient population. Chadwick et al 2003 (cited in RCSLT, CQ3 2006), found that 5.27% of all adults with learning disability were referred for advice regarding dysphagia. People with ID are at a higher risk of choking than the general population (Samuels and Chadwick 2006; Thacker 2007, Glover and Ayub 2010) When looking at the causes of death amongst people with learning disabilities, Glover and Ayub found that lung inflammation caused by solids or liquids, and foreign bodies in the windpipe, were involved 14% of people with learning disabilities or possibly associated conditions. In other people they were involved in just over 2% (Glover and Ayub 2010). PWLD and cerebral palsy, 22% of identified deaths involved solids or liquids in the windpipe or lungs.
1.4 Conditions resulting in dysphagia
‘Dysphagia can occur as a result of either a single medical problem, e.g. stroke, progressive
neurological condition, or as a result of:
• oropharyngeal structural problems;
• motor processing difficulties;
• central nervous system disorders;
• pharyngo-oesophageal problems;
• poor oral health;
• the psychological effects of institutionalisation;
• mental health problems;
• the effects of medication’. (NPSA 2007)
Go back to Pathway

Page 6 of 36
These are described in more detail by the NPSA (2007) in Table 1 below
End of box
1.5 Next Steps.
The reader is advised to read the following section outlining guidance for each step in the
Pathway. Assessment and understanding eating and drinking difficulties can be a complex
process and it may be helpful to seek further advice as outlined in the competency
documents (Boaden et al 2007, RCSLT 2014).
Table 1 Conditions associated with dysphagia.
1.1 Oropharyngeal structural problems, involving the palate, teeth and tongue, which may be associated with certain syndromes e.g. Down’s Syndrome, Williams Syndrome, Fragile X Syndrome, Rubinstein Taybi Syndrome (Howlin et al., 1998).
1.2 Motor processing difficulties, giving rise to muscle spasm, changes in muscle tone or
muscle unco-ordination, including abnormal tongue movements, affecting people with cerebral palsy (Waterman, et al., 1992), epilepsy, and syndromes including Down`s Syndrome, Fragile X (O`Brien et al.,1995), and Noonan`s syndrome (Shah et al., 1999).
1.3 Mental health disorders, including anxiety and depression (Stavrakaki, 1999) 1.4 Problems arising from the effects of medication .”Polypharmacy is common in both
institutional settings and community care” (Beange, 2003, p. 4) Side effects from medication may include: (a) altering levels of alertness, for example, antipsychotic and anticonvulsant medications and Benzodiazepines (Whyllie et al., 1986); (b) altering muscle tone/ co-ordination, for example, Baclofen and some anti depressants. (c) delaying the swallowing process or changes in salivation rates (Hughes et al.,1994, Sokoloff et al.,1997) (d) changes to appetite and taste.
1.5 Medical disorders
a) Central Nervous System disorders which give rise to dysphagia in this client group in common with the general population. In the survey of SLT caseloads in March 2004, CVA, Cerebral Tumour, Parkinsons disease, Motor Neurone Disease, Multiple Sclerosis, Dementia and other progressive conditions were recorded (See Appendix 1) (Watson, 2004). The incidence of dementia is high among older adults with learning disabilities (21.6%, compared to the figure within the general population of 5.7%, Cooper, 1997).
b) Pharyngo-oesophageal problems which include laryngeal pharyngeal reflux and gastro oesophageal reflux, thought by some authors to have a prevalence as high as 50% in this client group (Bohmer et al., 2000). Also hiatus hernia, systemic sclerosis and upper intestinal cancers (O`Brien et al., 2002; Duff et al., 2001)
1.6 Higher levels of poor oral health are recorded among people with learning disabilities
(Shapira et al.,1998) Respiratory pathogens present in the dental plaque of individuals with very poor dental hygiene may be aspirated, and predispose the individual to the development of lung infections (Malmstrom et al., 2002).
1.7 The psychological effects of institutionalisation which make this population more
susceptible to choking incidents e.g. eating too quickly and cramming food (Samuels & Chadwick, 2006).
1.8 There is evidence that those people with the highest support needs are most likely to
have eating, drinking and swallowing problems (Bohmer et al., 1996; Chadwick et al., 2003). (NPSA 2007)
Go back to Pathway
Page 7 of 36
2.1 Early identification of eating and drinking difficulties Dysphagia can present in many ways, and the person may demonstrate one or several of the following symptoms:
Food spillage from lips
Taking a long time to finish a meal
Poor chewing ability
Dry mouth
Saliva management difficulties or drooling
Nasal regurgitation
Food sticking in the throat
Poor oral hygiene
Coughing and choking
Breathlessness or gurgly voice during or after meals.
Regurgitation
Unintended weight loss
Repeated chest infections
Repeated hospitalisation for pneumonia
Anxiety at mealtimes
Food refusal
If any of the above are observed then a referral should be made.
2.2 Referrals The Learning disability service has an open referral system to access the team. Referrals are considered for any eligible adult (over 17yrs) with an LD when received on the current referral form (see website) from any person, family member, carer or professional. Referrals should be sent to the referral management team, contact number 0116 295 4545 (until September 2016) and from September 2016 this changes to 0116 295 5200. Advice for referring GPs is given by the NPSA (2007) Referrals for eating and drinking or swallowing assessment should be made by contacting the Referral Management Team, contact above, describing the difficulties you or the person is having at mealtimes or when drinking. This may include:
- Unintended weight loss - Choking or coughing at meals - Difficulty feeding oneself - Coughing after meals - Repeated chest infections
The referral management team allocate to the appropriate geographical and professional team according to identified need within one working week. This triggers a screening assessment for the pathway, known as the Initial Assessment which will take place within two working weeks from allocation to the team. Go back to Pathway
Page 8 of 36
Variance: the only times this process is not followed is
If the referral is clearly marked as Nil by Mouth, on receipt, the referral can be passed straight to the Speech and Language therapy (SLT) department.
The pathway is not written to provide emergency service as this is not provided by the LD service currently.
2.3 Foundation Worker Assessment
Screening for an eating and drinking difficulty within the Care Pathway is carried out by a
healthcare worker with enhanced eating and drinking training known as a Foundation
Worker, when an eating and drinking difficulty is first suspected. The screen may identify
difficulties which can be resolved at the initial screening stage. Mild
behaviour/communication issues such as pacing or focussing on the meal may be managed
by simple practical solutions. Signposting to other services such as dentistry can also be
done at this point and the person discharged as appropriate. However, if the screen reveals
difficulties in specialist areas and practical solutions to the presenting problem have not been
sufficient then the individual would be referred to the appropriate Specialist Services for a
formal diagnostic assessment and management.
When a person is referred to the Eating and Drinking Care Pathway, a FW will contact the
person or carers to arrange to carry out a Screening Assessment which includes:
Consent
First Assessment
Mealtime Observation
Recording and addressing risks (completing Eating and Drinking Risk Assessment
(EDRA))
This information is summarised for you and copied to your GP
Consent
Before any observation or case history taking, the professional will seek to gain consent from
the person. An accessible form for gaining consent is available (NPSA 2007). The
professional will use adapted communication wherever appropriate. If the person is unable
to give verbal consent, this may be implied for observation unless the person demonstrates
they are uncomfortable in which case the observer will review the situation.
First Assessment
This tool aims to ensure a structured, systematic approach in establishing important
information about an individual’s health, eating and drinking risks and identifies contributing
physical causations. The MUST nutrition screening tool is also completed at this stage.
Previous and current documents, such as eating and drinking plans, communication
passport, health checks and hospital grab sheets are considered. The first assessment
documents any previous history of mental health or physical health concerns, major life
events, recent or significant hospital admission. Any health needs arising from the First
Assessment should be addressed as far as possible.
Go back to Pathway
Page 9 of 36
Other relevant documents may include:
Fluid diary
Food diary
General Health charts (BMI/weight, menstrual cycle, diabetes, bowel charts, sleep
cycles).
cough charts
Food preference records
Menu sheets
Medication charts
Mealtime Observation
Mealtime observations are conducted in conjunction with the First Assessment. They are
conducted, in environment(s) accessed by the client for meal times. Mealtime observations
provide information on the
physical and social environment:,
communication between the person and others present,
Swallowing skills observed
Positioning
levels of carer support needed and independence skills
Nutrition risks
Recording and Addressing Risks
This document is left after all initial visits at the time of the visit. It addresses any concerns
immediately within the worker’s competence and lists the actions to meet those which need
specialist care. It can also be used after visits to document changes to management
recommended.
The Foundation worker uses the protocol guidelines and their experience and training to
interpret the assessment and choose appropriate strategies to manage the risks identified.
There may be immediate strategies that can be used such as shared decisions about how to
support the person to eat at a safe pace. (decision support tool for working together on
pacing when eating). There may be other resources which can be used such as leaflets (see
below) to discuss strategies or give information
The Foundation worker completes the ‘E&D Risk Assessment’ (EDRA) which describes the
baseline of skills and agrees the course of action to progress management of risks. A copy
of this is left at the home/service at the time of the first observation. The Foundation Worker
may recommend strategies for managing risks such as pacing, positioning or behaviour
management strategies at a general level (See Competences). The Foundation Worker may
leave general information leaflets or may work through general management strategies with
the carers/person.
For some people this intervention and care plan is sufficient to manage low level risks. In this
case, the plan is marked as the final copy and sent with a discharge letter to the GP and
referrer. If a Foundation worker felt there may not be a need for any more intervention, the
Foundation Worker would discuss the case and assessment with the MDT or appropriate
professional and together the decision would be made.
Go back to Pathway
Page 10 of 36
Generic advice leaflets from early intervention which may be used at screening
assessment
Foods which give a high risk of choking
Supporting people who eat and drink too fast
Communicating at meals
What is Dysphagia?
Supporting people with Dementia to eat and drink
Rushing whilst eating and overfilling the mouth is a common difficulty (Chadwick 2006). A
pacing decision support tool is available to facilitate carers, the person (if appropriate) and
the professional to jointly make and agree decisions about how to support the person to use
an appropriate pace for the meal/drink.
Communication with the GP and team.
A copy of the EDRA is sent to the GP immediately. The FW feeds back the results of the first
assessment to the locality team and onwards referrals are made as necessary:
Internally within the team: other professionals, Occupational Therapy,
Physiotherapy, Psychiatry, Psychology, Speech and language therapy, community
nursing
To other health services: dietetic service, mental health services, mainstream
services Primary Care Liaison Nurse, dentistry/specialist dentistry, GP, Acute Liaison
nurse, acute services such as Acute Adult SLT service, Radiology, respiratory clinic
To other services: for example, Wheelchair services.
For more detail on specialist assessment by profession, see the section on roles
and competences.
Discharge from Foundation Worker
The Foundation worker would not make the decision to discharge alone. The Foundation
worker would meet with either an appropriate member of the team or the full team to discuss
in depth the findings and agree the outcome. If there is agreement to discharge, the
discharge letter and a copy of the Eating and Drinking Risk assessment is sent to the GP
and referrer.
Screening Assessment Outcomes
Discharge
If there are no further actions needed
after the screening assessment,
discharge letter is sent from the
Locality Learning Disability Team to
the referrer and copied to the person
and GP
Further action needed after screening
will result in referral on to the
appropriate professional members of
the Locality Learning Disability Team
for specialist assessment
Go back to Pathway
Page 11 of 36
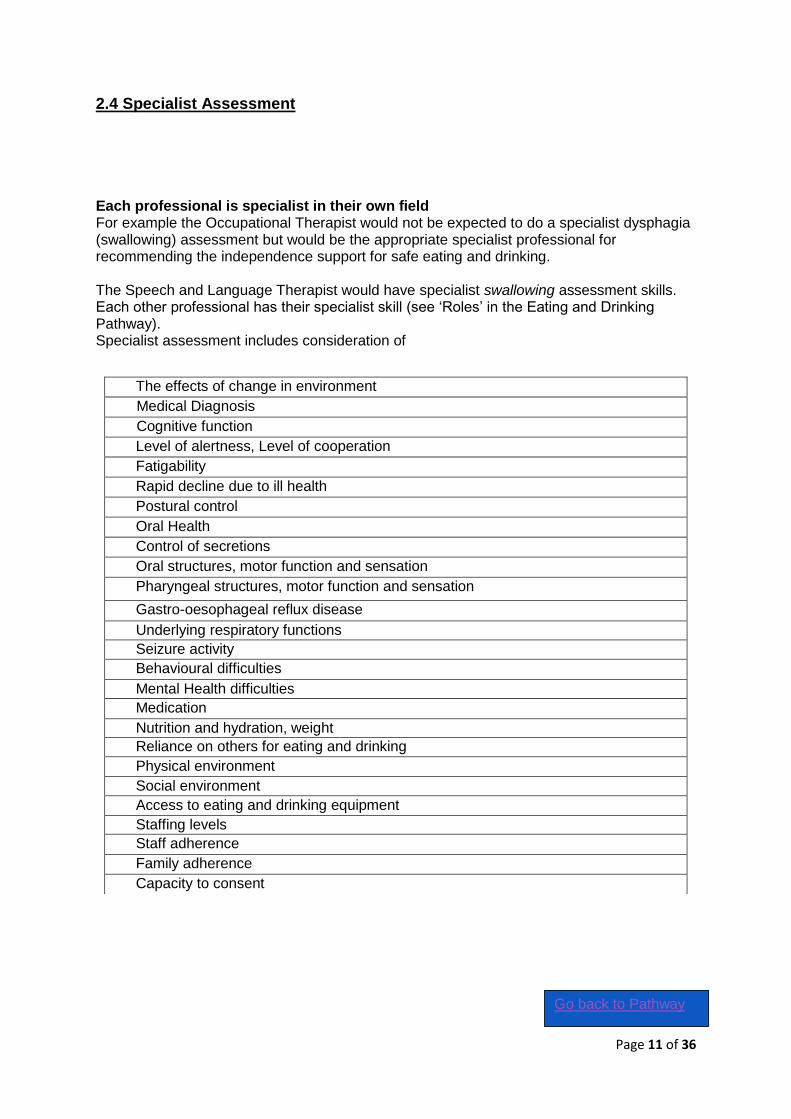
2.4 Specialist Assessment
Each professional is specialist in their own field For example the Occupational Therapist would not be expected to do a specialist dysphagia (swallowing) assessment but would be the appropriate specialist professional for recommending the independence support for safe eating and drinking. The Speech and Language Therapist would have specialist swallowing assessment skills. Each other professional has their specialist skill (see ‘Roles’ in the Eating and Drinking Pathway). Specialist assessment includes consideration of
The effects of change in environment
Medical Diagnosis
Cognitive function
Level of alertness, Level of cooperation
Fatigability
Rapid decline due to ill health
Postural control
Oral Health
Control of secretions
Oral structures, motor function and sensation
Pharyngeal structures, motor function and sensation
Gastro-oesophageal reflux disease
Underlying respiratory functions
Seizure activity
Behavioural difficulties
Mental Health difficulties
Medication
Nutrition and hydration, weight
Reliance on others for eating and drinking
Physical environment
Social environment
Access to eating and drinking equipment
Staffing levels
Staff adherence
Family adherence
Capacity to consent
Go back to Pathway
Page 12 of 36
2.5. Formulation and Care Plan
Eating and Drinking Plans identify:
Risks around eating and drinking
Communication strengths and needs
Positioning strength and needs
Equipment needs
Food modification/ choice/cultural needs
Support needs.
Maintenance of the plan
What signs or symptoms may indicate changing needs
When and how to re-refer
Who has a copy of the plan (at minimum the person, the referrer and GP)
How the plan has been cascaded/carers trained/plan shared
The eating and drinking plan will additionally advise on best practice Sackett (2000) in
relation to the client’s specific needs, for example using research/ evidence/ national
guidelines (e.g. NSF, NICE guidelines, DOH).
The plan will
Clearly outline strategies to reduce risks around eating and drinking.
Inform the person of the risks when eating and drinking and explain the Eating and Drinking Risk Assessment.
Inform carers of the best way to assist someone to eat and drink to minimise these risks.
Be written in consultation with the person and their family/carers and would take account of quality of life, personal preferences and cultural and dietary needs and wants.
Be personalised to involve and inform the person as much as possible. This may mean writing one or more additional accessible versions as well as a carer version of the plan.
Professionals have an obligation to give advice but it is recognised that it is the responsibility
of the person and carers to follow the recommendations. Other forms of the Eating and
drinking plan may be made available in supporting formats such as placemat or accessible
format. Both forms would be personalised. Examples are available
Accessible plan example Placemat plan template
This list is not exhaustive.
Any additional risks may be recorded in the specialist risk assessment. Wherever
possible the assessing team works together to avoid unnecessary repetition; sharing
documents, completing documents jointly and joint visits.
Specialist assessments include mini trials of strategies to see if they are effective and
provide more detailed analysis
Go back to Pathway
Page 13 of 36
2.6 Evaluation and discharge
Plans are evaluated according to clinical judgement by the professional(s) involved.
The plan is reviewed until the person is stable and eating and drinking risks are minimised
and all training needs have been met.
Discharge is considered when
The person is stable and eating and drinking risks are minimised
Carers are confident and competent to carry out the Eating and Drinking Plan
Carers know how to monitor the Eating and Drinking Plan and know how and when to re-refer.
When all these criteria are met, the person is discharged and the relevant information is sent to the GP and/or referrer.
It is acknowledged that services/carers following eating and drinking plans may
affect the validity of any professional assessment. However it is unethical not to give
advice where advice can be given which immediately reduces risk to the client and
others.
Go back to Pathway
Page 14 of 36
Click here for the stepped care approach
3.1 Competences and roles
The Responsibilities of the Care Pathway Co-ordinator
If the person is on care programme approach (CPA), the Care Co-ordinator is responsible for co-ordinating care, maintaining contact with the service user ensuring that the CPA care plan is delivered and reviewed as required. (CPA policy) The Care Co-ordinator will be a qualified individual with the requisite knowledge, skills and experience and will in most cases be registered to a profession and be the person “best placed” to oversee care planning and resource allocation. The Care Co-ordinator can be of any discipline depending on capability and capacity.
Lead Profession (non-CPA) role: The lead professional is responsible for co-ordinating care, maintaining contact with the service user ensuring that the care plan (or other care plan for managing eating and drinking difficulties), is delivered and reviewed as required. The lead professional will be a qualified member of staff with appropriate training to fulfil this role.
Foundation Worker
Foundation Workers are trained according to the Interdisciplinary Dysphagia Framework (2007).Foundation workers have identified competence and knowledge base.
‘This role describes practitioners who are not specialists in dysphagia, but who have a
responsibility for providing care for individuals who may present with difficulties swallowing liquids and solids (dysphagia). They demonstrate skills in
the recognition and identification of dysphagia, initial protocol-guided assessment and implementation of the protocol-guided actions. The practitioner will implement a review process according to local protocols. They are autonomous practitioners working within the team but should consult with more experienced practitioners in order to ensure that their competence is commensurate with best practice .Foundation dysphagia practitioners will recognise the potential health risks presented by the signs of dysphagia, acknowledge the urgency of the referral and, if appropriate, refer to a more experienced/qualified dysphagia practitioner The practitioner should undertake a period of training and be assessed on their underpinning knowledge and clinical competence. They will be able to train other staff, relatives and carers to awareness/assistant practitioner levels This includes practitioners who work across primary and secondary healthcare, social services and education. (IDDF Boaden et al 2007)
Foundation Workers receive initial one day training. Different members of the adult LD
Team give information about their role and the knowledge base for the screening
assessment. The foundation worker practises assessment and interpretation of results in a
small group. The foundation worker practices completion of the relevant documentation and
is made aware of supporting resources. Foundation workers are encouraged to ‘buddy up’
with joint visits with other FW or professionals until they feel confident using the assessment.
Foundation Workers must attend an annual update which focusses upon
Go back to Pathway
Page 15 of 36
- Updating on new process and new theory - Peer support and feeding back into the pathway - Key topics identified by the Eating and Drinking Steering Group and Foundation
Workers throughout the year - Maintaining skills and knowledge. - Topic –based learning e.g 2011 diet and nutrition. 2012 choke reporting, 2013
equipment, 2014 food modification
A Foundation Worker may be any member of the Locality Team who has undertaken the
training and maintains their competence.
Specialist Dysphagia practitioner (SLT) see appendix 1
Health Care Professionals Tier 2 Psychiatry (Tier 2/3) Education and Support
Offer advice to SLT re: medication and swallowing difficulties
Involvement would be indirect / advice to colleagues Psychology (Tier 2/3/4)
Infrequent referrals for clinical psychologists re this pathway. However eating disorder/bulimia/anorexia and psychological formulations/ interventions used sometimes, usually in conjunction with mental health or ASD pathway.
Assessment and Formulation if Psychology factors identified
Safeguarding Strong / prolonged adjustment reaction,
o (if not resolved after 6 months)
Consultation
Mental capacity assessment/advice
Supporting Eating Disorders Service re: LD issues
If linked to Mental Health, or some other complex issue, may be additional hours, depending on assessment
General consultation / advice Community Nursing Education and support:
To primary care and direct carers information awareness.
Prevention/early identification/guided or supported self-management. Health promotion – general access.
Enabling access to mainstream services. Working with primary care/capacity/contributory issues. Info for carers and professionals. Dysphagia foundation work. Support to implement plan.
Assessment:
Triage, MUST, Waterlow, basic food diary, SSKIN, capacity assessment. Intervention:
Signposting support to implement plan. Go back to Pathway
Page 16 of 36
Speech and Language Therapy Education and support:
A range of education, supervision and mentoring activities to enable mainstream services to address the communication and dysphagia needs of people with learning disability.
The aim is to enable them to make reasonable adjustments and meet the 5 Good Communication standards and safe eating and drinking guidelines.
Signposting and providing general communication information for people with learning disabilities
Assessment:
Provide a brief assessment of the specific communication environment in relation to the 5 Good Communication Standards.
Provide tools to support services to develop a basic communication passport for an individual.
Skilling staff to recognise communication and eating and drinking issues and make appropriate referrals.
Intervention:
Onward referral and signposting
Provide findings of an individual’s communication or eating and drinking assessment to support mainstream services to address their communication or eating and drinking needs. Provide mentoring and support for staff working in main stream services to enable them to make reasonable adjustments in relation to communication and learning disabilities.
Provide general advice, information and resources to support safe eating and drinking
Provide information and guidelines on best practice. Share resources and tools to support good communication.
Joint working with staff from other services.
Support the development and use of communication passports to inform other staff of the best ways of communicating with individuals.
Occupational Therapy Education and Support:
Basic eating and drinking awareness training for carers/family. Assessment:
Gather Foundation Worker eating and drinking history and initial observation Intervention:
Interim meal time plan / recommendations
Refer to suitable profession
Input into eating and drinking plan
Go back to Pathway
Page 17 of 36
Physiotherapy Education and support:
Encouragement to look back at previous advice given.
Provide client with the information required to access relevant generic service
Signpost to ventilation clinic when appropriate. Tier 3 Education and support: FW training – access to more specialist services. Assessment: Detailed dysphagia FW assessment. Intervention:
Develop eating and drinking plan.
Competency assessment.
Monitor implementation of plan. Speech and Language Therapy Education and support:
Specific training to support learning disability environments to meet the communication or eating and drinking needs related to learning disabilities.
Individualised communication or eating and drinking training for staff supporting individuals referred to the service.
Assessment:
To provide a detailed description of an individual’s communication needs and priorities
To inform a formulation
To provide a diagnosis of communication impairment
To contribute to or initiate a wider diagnosis
To inform capacity assessments and best interest approaches How
Formal assessments
Informal assessments
Observations across a range of environments
Collecting information from key communication partners and other professions
Communication environment assessment Areas covered
Comprehension
Ways
Programmatic skills
Functional communication
Barriers to communication
Reasons and opportunities
Go back to Pathway
Page 18 of 36
Diagnosis and Formulation Aim
To provide a framework for describing any communication issues and allow for the development of an action plan underpinned by clinical reasoning.
How
By completing a formulation, which is a process of collecting and integrating information gathered from SLT assessment, relevant documentation, academic studies and articles and from interview with the individual, their carers and other members of the MDT.
Intervention:
Intervention may involve working with the individual in order to enhance current, or develop new, communication skills. It may involve supporting carers to enhance or develop new communication skills.
It may additionally involve recommending environmental changes to better support the individual’s communication.
Interventions will be framed within the Royal College of Speech and Language Therapists’ (2014) Five Good Communication Standards.
To support colleagues in areas such as
assessing capacity
How to involve people Occupational Therapy Assessment
The Occupational Therapist considers the impact of physical, cognitive, perceptual, sensory and behavioural factors in the assessment and management of individuals with eating and drinking difficulties.
This also reflects the environmental and social factors which affect the individual’s skills.
Intervention
Guidelines for an individual’s positioning needs to identify the use of appropriate seating and other physical supports to facilitate safe and effective eating and drinking.
Facilitation of independence through guidelines to identifying adaptive equipment and education of individuals and their carers.
Guidelines to manage the impact of the individual’s behaviour, psychological and other social factors in order to promote safe and effective eating and drinking.
A guideline for meeting individual’s sensory skills and needs.
Guidelines regard environmental needs.
Occupational Therapists will work as part of the MDT Care Pathway for eating and drinking.
Go back to Pathway
Page 19 of 36
Physiotherapy Education and support:
Education of the physiotherapy role with in the Eating and Drinking care pathway for Foundation worker training.
Postural management recommendations/advice – to clients/families/carers, colleagues and other agencies.
Assessment:
General Physiotherapy Assessment and Postural Management assessment.
Consider assessment of posture for safe eating and drinking (joint work with SALT and/or OT).
Positioning for management of chest secretions. Intervention:
Assessment and provision of seating for optimal positioning for safe eating and drinking (jointly assessed with SALT).
Work in conjunction with specialist respiratory services, SALT, Specialist mobility Service, Specialist equipment companies (equipment reps)
Recommendations for positioning to aid clearance of chest secretions.
Facilitating clients to access ventilation clinics.
Tier 4 Psychiatry Education and Support
Offer advice to SLT re: medication and swallowing difficulties
Involvement would be indirect / advice to colleagues Assessment
Consideration of medication causing swallowing difficulties
Mental health assessment to rule out causes for not eating such as depression Intervention
Involvement in Mental Capacity Act meetings
Involvement will be time limited, if requested by members of team who suspect or wish to rule out mental health causes of swallowing difficulty.
Community Nursing Education and support:
Intensive support in the community or inpatient care by specialist LD services. Desensitisation.
Assessment:
SALT role re: intensive assessment. Intervention:
Intense competency assessment – change of care provider, new enteral tube fitted. Desensitisation to attend clinics.
Speech and Language Therapy As Tier 3 but with a need for greater mulita-disciplinary working, cases may be more urgent and complex requiring more intensive input
Go back to Pathway
Page 20 of 36
Physiotherapy Education and support:
Education of the physiotherapy role with in the Eating and Drinking care pathway for Foundation worker training.
Postural management recommendations/advice – to clients/families/carers, colleagues and other agencies.
Assessment:
General Physiotherapy Assessment and Postural Management assessment.
Consider assessment of posture for safe eating and drinking (joint work with SALT and/or OT).
Positioning for management of chest secretions. Intervention:
Work in conjunction with specialist respiratory services, SALT, Specialist mobility Service, Specialist equipment companies (equipment reps).
Develop and undertake treatment plan to include the assessment and provision of equipment with clients and carers.
Delegation of treatment plans as appropriate
Joint working with MDT and signpost as necessary
Go back to Pathway
Page 21 of 36
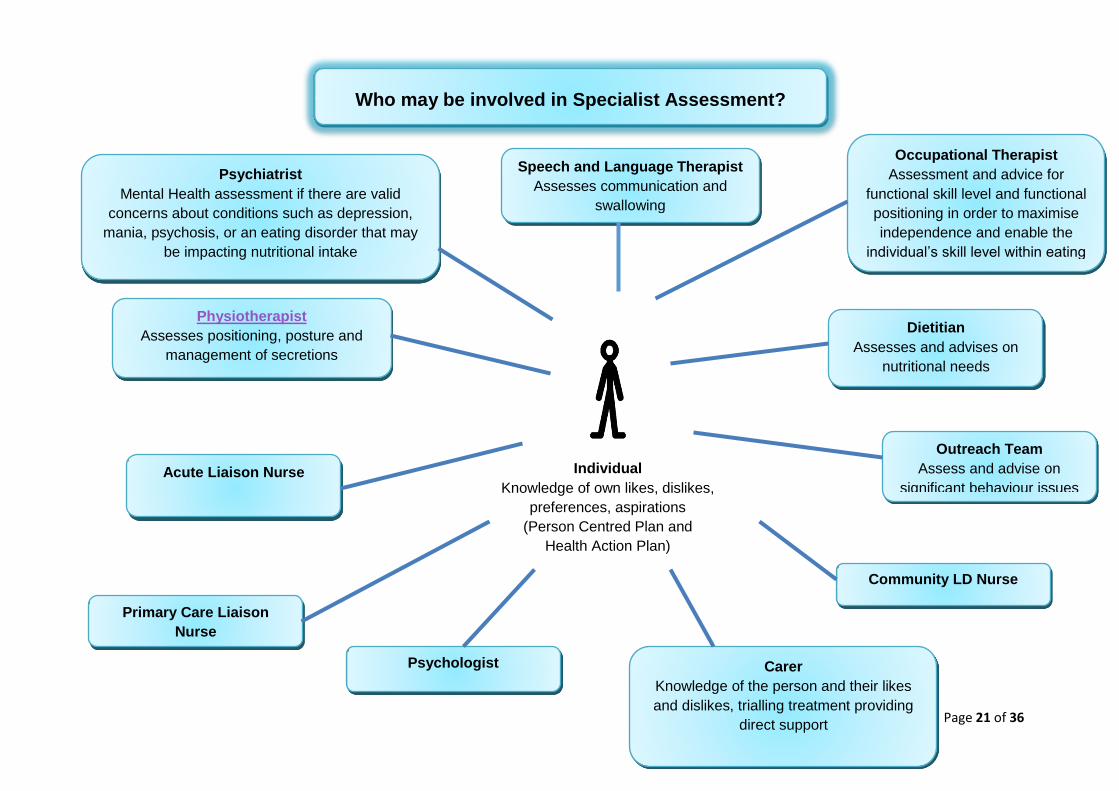
Individual
Knowledge of own likes, dislikes,
preferences, aspirations
(Person Centred Plan and
Health Action Plan)
Speech and Language Therapist
Assesses communication and
swallowing
Occupational Therapist
Assessment and advice for
functional skill level and functional
positioning in order to maximise
independence and enable the
individual’s skill level within eating
and drinking
Dietitian
Assesses and advises on
nutritional needs
Outreach Team
Assess and advise on
significant behaviour issues
Community LD Nurse
Carer
Knowledge of the person and their likes
and dislikes, trialling treatment providing
direct support
Psychologist
Primary Care Liaison
Nurse
Psychiatrist
Mental Health assessment if there are valid
concerns about conditions such as depression,
mania, psychosis, or an eating disorder that may
be impacting nutritional intake
Acute Liaison Nurse
Physiotherapist
Assesses positioning, posture and
management of secretions
Who may be involved in Specialist Assessment?
Page 22 of 36
Leaflets NPSA – Problems Swallowing for Carers NPSA – Problems Swallowing for Professionals Useful Websites NPSA www.npsa.nhs.uk
MENCAP www.mencap.org.uk
Alzheimers society www.alzheimers.org.uk
Caroline Walker trust www.cwt.org.uk
BILD www.bild.org.uk
Rett UK www.rettuk
Leicestershire Nutrition and Dietetic Service www.lnds.nhs.uk
Go back to Pathway
Page 23 of 36
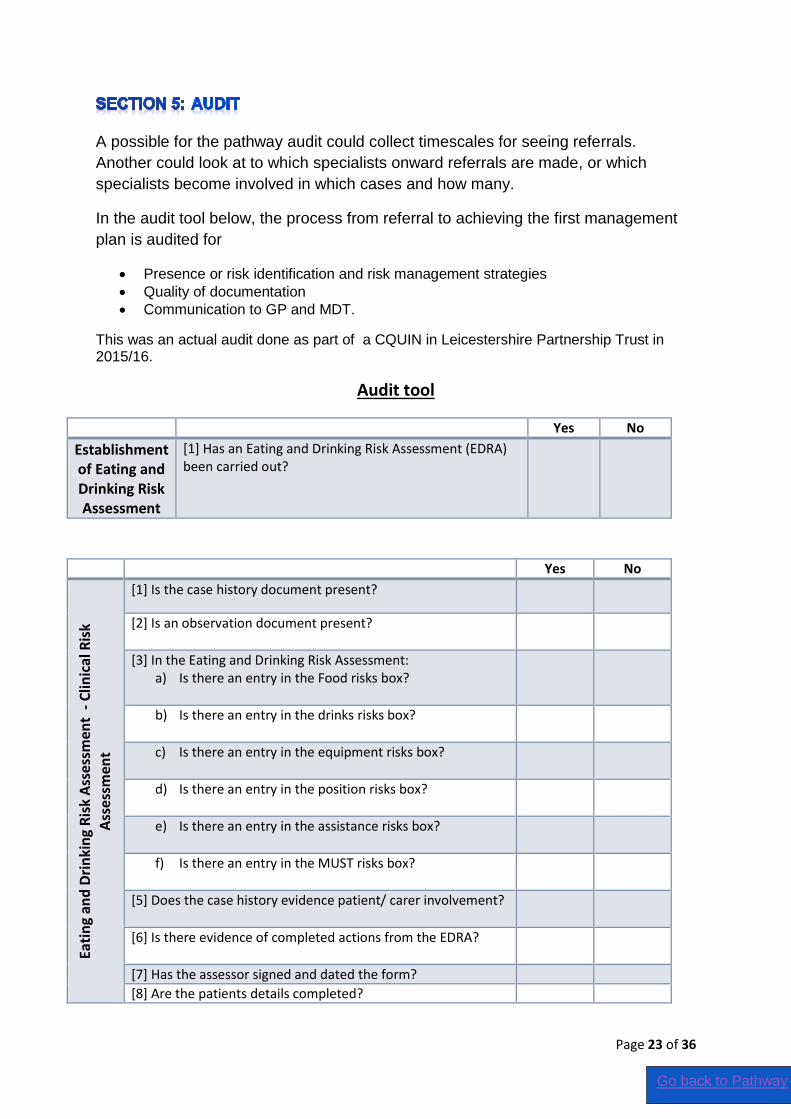
A possible for the pathway audit could collect timescales for seeing referrals.
Another could look at to which specialists onward referrals are made, or which
specialists become involved in which cases and how many.
In the audit tool below, the process from referral to achieving the first management
plan is audited for
Presence or risk identification and risk management strategies
Quality of documentation
Communication to GP and MDT.
This was an actual audit done as part of a CQUIN in Leicestershire Partnership Trust in 2015/16.
Audit tool
Yes No
Establishment of Eating and Drinking Risk Assessment
[1] Has an Eating and Drinking Risk Assessment (EDRA) been carried out?
Yes No
Eati
ng
and
Dri
nki
ng
Ris
k A
sse
ssm
ent
- C
linic
al R
isk
Ass
ess
men
t
[1] Is the case history document present?
[2] Is an observation document present?
[3] In the Eating and Drinking Risk Assessment: a) Is there an entry in the Food risks box?
b) Is there an entry in the drinks risks box?
c) Is there an entry in the equipment risks box?
d) Is there an entry in the position risks box?
e) Is there an entry in the assistance risks box?
f) Is there an entry in the MUST risks box?
[5] Does the case history evidence patient/ carer involvement?
[6] Is there evidence of completed actions from the EDRA?
[7] Has the assessor signed and dated the form?
[8] Are the patients details completed?
Go back to Pathway
Page 24 of 36
Yes No
Dev
elo
pm
ent
of
ind
ivid
ual
ise
d
care
pla
ns
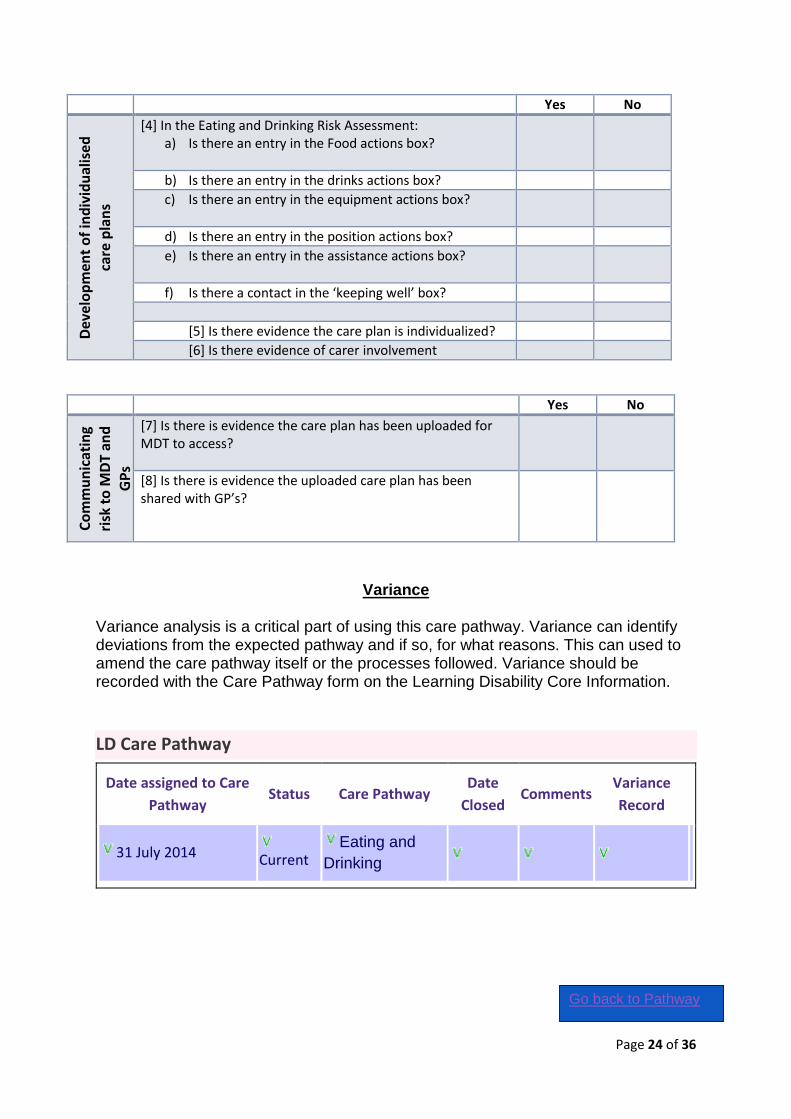
[4] In the Eating and Drinking Risk Assessment:
a) Is there an entry in the Food actions box?
b) Is there an entry in the drinks actions box?
c) Is there an entry in the equipment actions box?
d) Is there an entry in the position actions box?
e) Is there an entry in the assistance actions box?
f) Is there a contact in the ‘keeping well’ box?
[5] Is there evidence the care plan is individualized?
[6] Is there evidence of carer involvement
Yes No
Co
mm
un
icat
ing
risk
to
MD
T an
d
GP
s
[7] Is there is evidence the care plan has been uploaded for MDT to access?
[8] Is there is evidence the uploaded care plan has been shared with GP’s?
Variance
Variance analysis is a critical part of using this care pathway. Variance can identify deviations from the expected pathway and if so, for what reasons. This can used to amend the care pathway itself or the processes followed. Variance should be recorded with the Care Pathway form on the Learning Disability Core Information.
LD Care Pathway
Date assigned to Care
Pathway Status Care Pathway
Date
Closed Comments
Variance
Record
31 July 2014 Current Eating and
Drinking
Go back to Pathway
Page 25 of 36
The Responsibilities of the Care Pathway Co-ordinator
If the person is on care programme approach (CPA), the Care Co-ordinator is responsible for co-ordinating care, maintaining contact with the service user ensuring that the CPA care plan is delivered and reviewed as required. (CPA policy) The Care Co-ordinator will be a qualified individual with the requisite knowledge, skills and experience and will in most cases be registered to a profession and be the person “best placed” to oversee care planning and resource allocation. The Care Co-ordinator can be of any discipline depending on capability and capacity.
Lead Profession (non-CPA) role: The lead professional is responsible for co-ordinating care, maintaining contact with the service user ensuring that the care plan (or other care plan for managing eating and drinking difficulties), is delivered and reviewed as required. The lead professional will be a qualified member of staff with appropriate training to fulfil this role.
Mrs Jennifer Worsfold, Speech and Language Therapist 0116 225 5200
Mrs Katie Crowfoot, Occupational Therapist 0116 295 4007
Mrs Nicky Calow, Dietician 0116 225 3735
Mrs Julia Kew, Primary Care Liaison Nurse 0116 225 5291
Mrs Fiona Brettell, Speech and Language Therapist 0116 225 5331
Thank you to Tracey Charity for her work over the years on the pathway
Go back to Pathway
Page 26 of 36
Appendices 1) Specialist Dysphagia Workers 2) Screening Assessment
a. Eating and Drinking First Assessment b. Protocol Guidelines c. Food Diary d. Mealtime Observation e. MUST Screening Tool f. Cough Recording Chart g. Medications that may Affect Swallowing h. Other Useful Leaflets
3) Skills and Competency Framework 4) Intervention Package and Case Studies 5) Patient Related Outcome Measures (PROM)
Go back to Pathway
Page 27 of 36
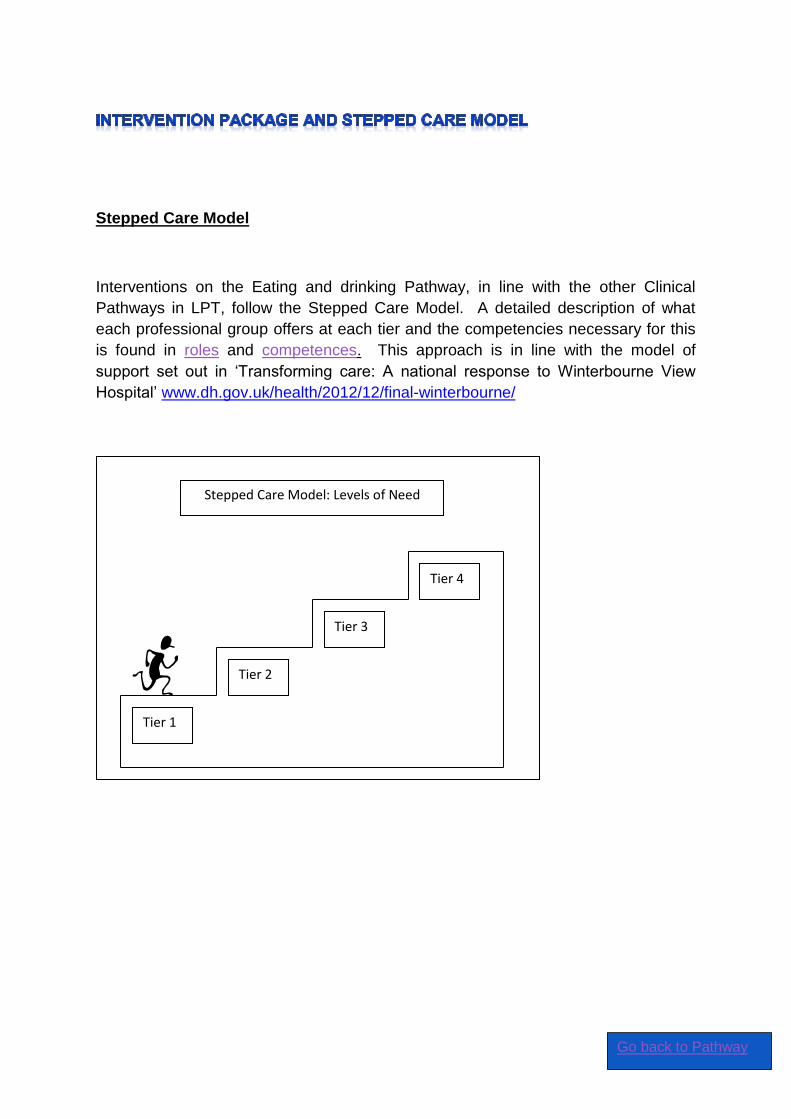
Stepped Care Model
Interventions on the Eating and drinking Pathway, in line with the other Clinical
Pathways in LPT, follow the Stepped Care Model. A detailed description of what
each professional group offers at each tier and the competencies necessary for this
is found in roles and competences. This approach is in line with the model of
support set out in ‘Transforming care: A national response to Winterbourne View
Hospital’ www.dh.gov.uk/health/2012/12/final-winterbourne/
Tier 1
Tier 2
Tier 3
Tier 4
Stepped Care Model: Levels of Need
Go back to Pathway
Page 28 of 36
P
r
a
c
t
i
c
a
l
P
r
o
b
l
e
m
S
o
l
v
i
n
g
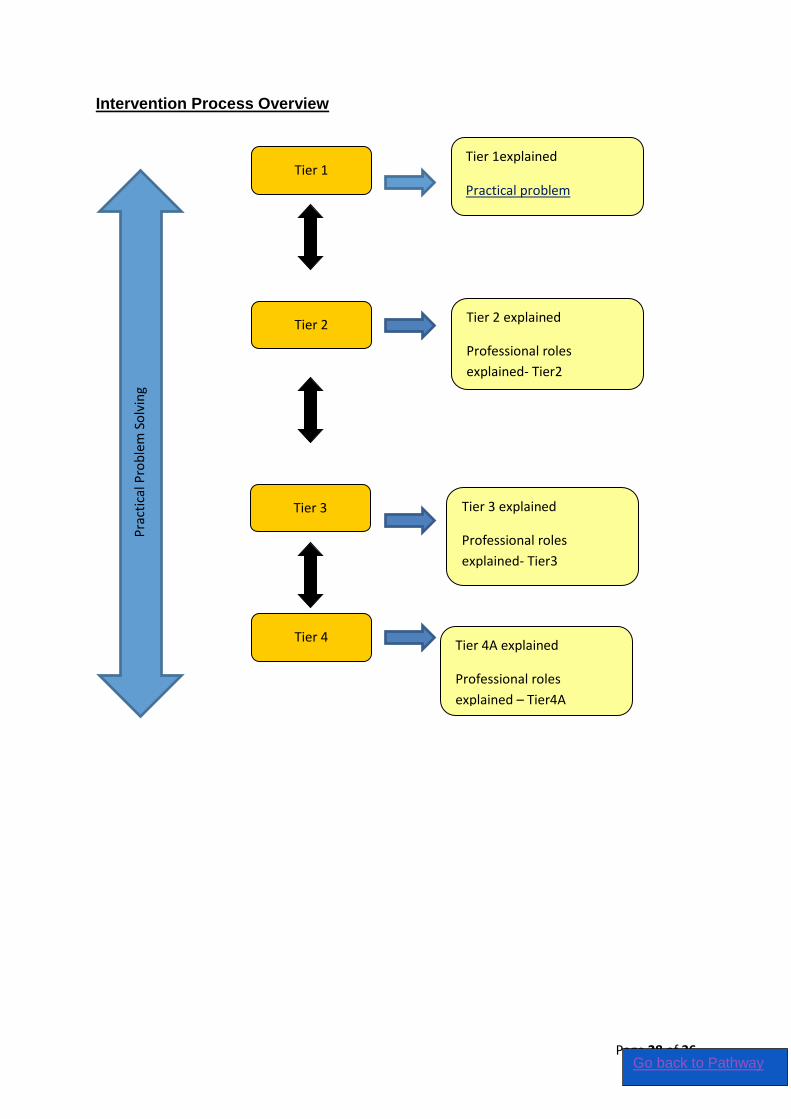
Intervention Process Overview
Tier 1
Tier 2
Tier 3
Tier 4
Tier 1explained
Practical problem
Solving explained
Tier 2 explained
Professional roles
explained- Tier2
Tier 3 explained
Professional roles
explained- Tier3
Tier 4A explained
Professional roles
explained – Tier4A
Pra
ctic
al P
rob
lem
So
lvin
g
Go back to Pathway
Page 29 of 36
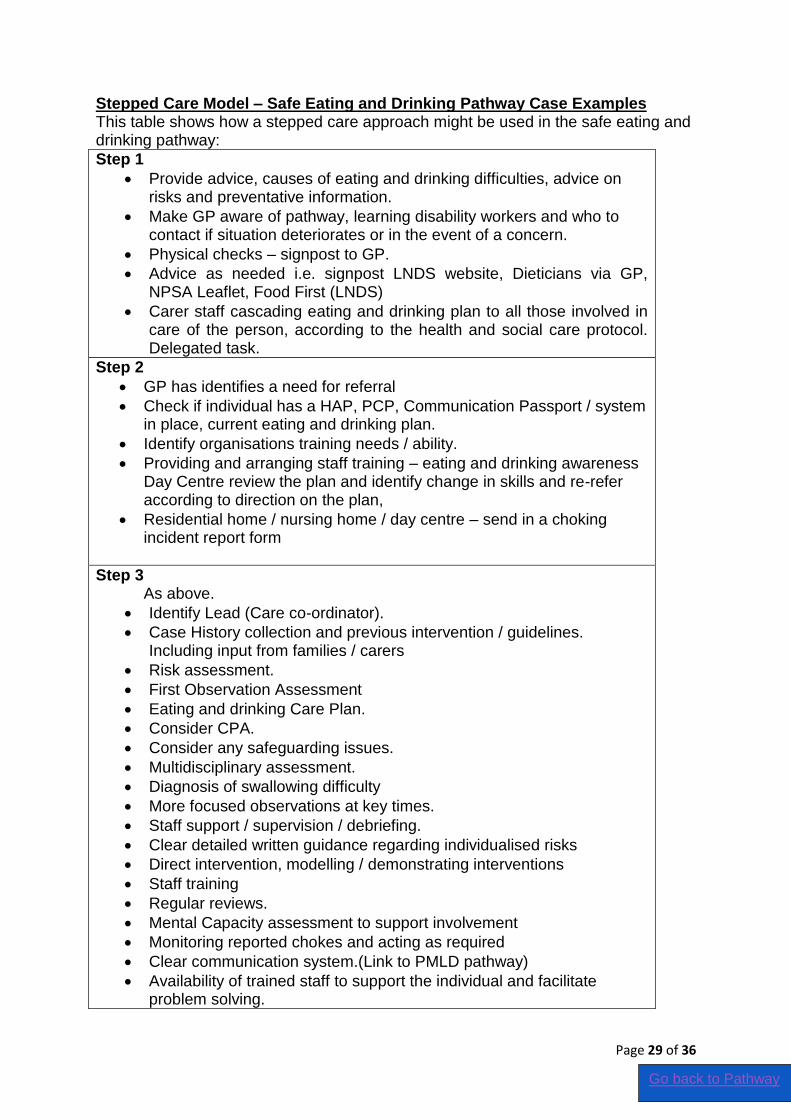
Stepped Care Model – Safe Eating and Drinking Pathway Case Examples This table shows how a stepped care approach might be used in the safe eating and drinking pathway:
Step 1
Provide advice, causes of eating and drinking difficulties, advice on risks and preventative information.
Make GP aware of pathway, learning disability workers and who to contact if situation deteriorates or in the event of a concern.
Physical checks – signpost to GP.
Advice as needed i.e. signpost LNDS website, Dieticians via GP, NPSA Leaflet, Food First (LNDS)
Carer staff cascading eating and drinking plan to all those involved in care of the person, according to the health and social care protocol. Delegated task.
Step 2
GP has identifies a need for referral
Check if individual has a HAP, PCP, Communication Passport / system in place, current eating and drinking plan.
Identify organisations training needs / ability.
Providing and arranging staff training – eating and drinking awareness Day Centre review the plan and identify change in skills and re-refer according to direction on the plan,
Residential home / nursing home / day centre – send in a choking incident report form
Step 3 As above.
Identify Lead (Care co-ordinator).
Case History collection and previous intervention / guidelines. Including input from families / carers
Risk assessment.
First Observation Assessment
Eating and drinking Care Plan.
Consider CPA.
Consider any safeguarding issues.
Multidisciplinary assessment.
Diagnosis of swallowing difficulty
More focused observations at key times.
Staff support / supervision / debriefing.
Clear detailed written guidance regarding individualised risks
Direct intervention, modelling / demonstrating interventions
Staff training
Regular reviews.
Mental Capacity assessment to support involvement
Monitoring reported chokes and acting as required
Clear communication system.(Link to PMLD pathway)
Availability of trained staff to support the individual and facilitate problem solving.
Go back to Pathway
Page 30 of 36
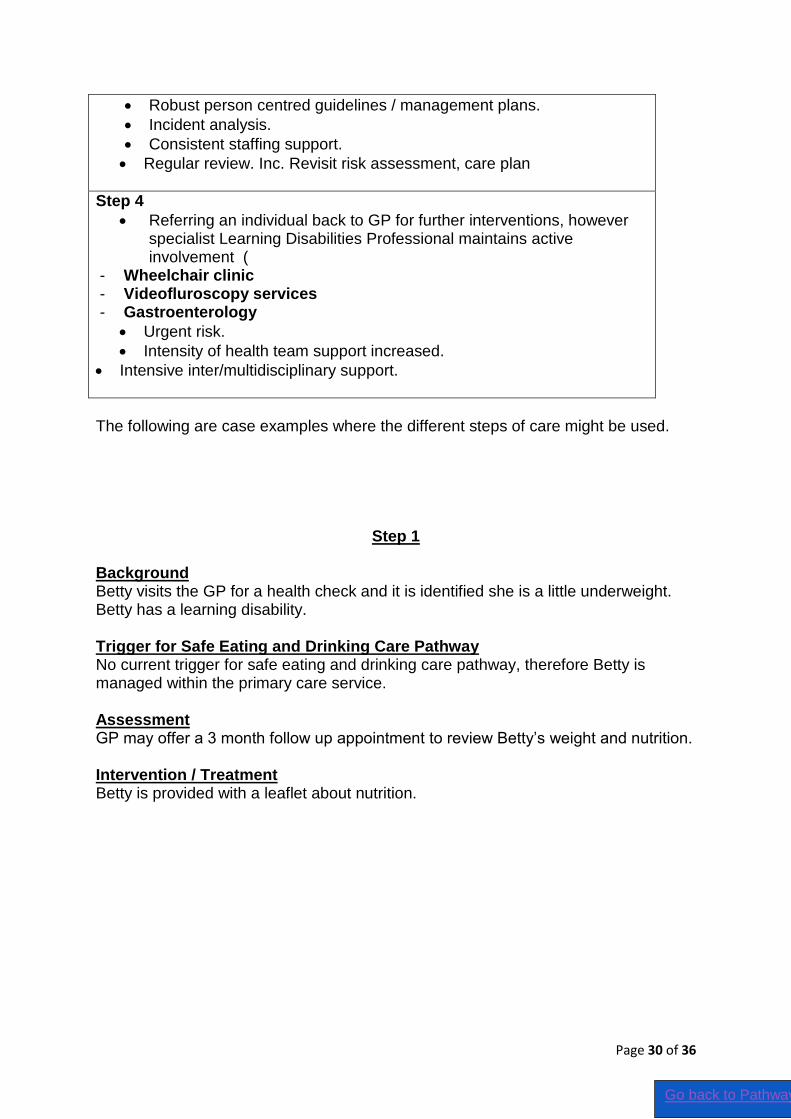
Robust person centred guidelines / management plans.
Incident analysis.
Consistent staffing support.
Regular review. Inc. Revisit risk assessment, care plan
Step 4
Referring an individual back to GP for further interventions, however specialist Learning Disabilities Professional maintains active involvement (
- Wheelchair clinic - Videofluroscopy services - Gastroenterology
Urgent risk.
Intensity of health team support increased.
Intensive inter/multidisciplinary support.
The following are case examples where the different steps of care might be used.
Step 1 Background Betty visits the GP for a health check and it is identified she is a little underweight. Betty has a learning disability. Trigger for Safe Eating and Drinking Care Pathway No current trigger for safe eating and drinking care pathway, therefore Betty is managed within the primary care service. Assessment GP may offer a 3 month follow up appointment to review Betty’s weight and nutrition. Intervention / Treatment Betty is provided with a leaflet about nutrition.
Go back to Pathway
Page 31 of 36
Step 2 Background Betty has returned for her follow-up appointment 3 months later with her GP. Betty has brought along her carer for support. Betty has lost weight and her carer reports that she is taking longer to eat. Trigger for Safe Eating and Drinking Care Pathway
Unintended Weight loss
Changes in meal time ability / skill
Eating and drinking difficulty Assessment GP compares Betty’s weight loss from previous appointment GP completes a blood test to identify any underlying physical health needs Intervention / Treatment GP referrer to the Adult Learning Disabilities for a detailed assessment of Betty’s eating and drinking needs. GP refers to the food first guidance available within her residential home. Step 3 Background Betty, a 62yr old lady with Dementia and Down’s syndrome is referred because she is refusing to eat and her levels of alertness have dropped considerably. Trigger for Safe Eating and Drinking Care Pathway
Refusing to eat
Weight loss
Dementia Assessment The Foundation Worker is sent to assess the situation. The FW takes a full case
history and observational assessment as per the protocol. The FW and the main carer screen Betty using the MUST tool and Nutritional screen. Betty’s weight is to be monitored by the carer in future as her weight loss is currently not significant to refer to the dietician. The FW from the initial assessments refers on to the :
OT because Betty is not using cutlery well and doesn’t eat all the plateful of food, leaving ½ the plate untouched.
SLT because Betty coughed 3 times during the meal so a swallow assessment would be indicated. Also Betty is obviously confused and not understanding information told to her. She is using ‘yes’ as a generic response to most questions, making her vulnerable.
Go back to Pathway
Page 32 of 36
The Community nurse because Betty needs a review of her medication as soon as possible and review on the Dementia Care pathway.
The FW documents Betty current E&D skills and situation on the Interim plan. She documents who she will refer on to in the team. She gives carers the ‘Supporting people with dementia to eat and drink’ leaflet. Intervention / Treatment The OT does a full assessment of Betty’s mealtime skills and makes
recommendations about using cues in the environment to help her to understand that it’s a meal time and using specialised equipment to help her to maintain self feeding. Working together with the SLT, they make recommendations about how best to support her to feed herself using gesture and touch prompts, giving different levels of support to be employed according to how Betty is, still involving her in choices about her meal wherever possible.
The SLT completes a swallow assessment and gives recommendations to reduce Betty’s risk of choking and demonstrates to two members of staff how to prepare her meals. She also advises the staff on good oral hygiene, making recommendations for encouraging Betty to clean her own teeth or to cooperate in having them cleaned. She advises about the possible deterioration in skills and advises about when to re-refer; what to look out for and what will put Betty at risk of choking or aspiration. The SLT completes a communication assessment and provides recommendations about how best to communicate with Betty. The Community nurse liaises with the GP and consultant psychiatrist. Together changes are made to Betty’s medication and she is involved as much as possible in understanding the changes.
The care coordinator ensures the relevant professionals contribute to the risk management plan and arranges for the plan to be demonstrated if to the carer.
The carer now knows how to prepare Betty’s food, collect Betty’s specialized equipment, prepare Betty for the meal and support her through it. The carer knows to monitor Betty’s weight and what to look out for as Betty’s illness progresses. She knows good ways to communicate with Betty and involve her as much as possible in mealtimes to maintain safety, adequate nutrition dignity, enjoyment and choice. She trials the eating and drinking plan and negotiates with the E&D team to ensure the plan is personalised, relevant and meeting Betty’s needs for safe, nutritious, enjoyable eating and drinking. She signs the plan to agree to cascade the information to other staff in the home who may also assist Betty to eat and drink. Follow up A discharge summary would be provided along with the Eating and Drinking plan. Within this there would be clear identification of when and how to re-refer. A copy would also be sent to the GP for their records.
Go back to Pathway
Page 33 of 36
Step 4 Background Betty is re-referred back to the adult learning disabilities service via her residential home following a significant decline of her eating and drinking abilities and change with her dementia. Betty has been noticed to store food in her mouth, Betty’s wheelchair is not supporting her and therefore Betty head is not supported and therefore she choking on her food.
Trigger for Safe Eating and Drinking Care Pathway
Urgent risk of choking (Ongoing / high frequency)
Swallowing difficulties
Poor positioning Assessment The referral is triaged as urgent due to the high risk of choking foundation worker (FW) assessment is completed as per Step 3. Following initial assessment the foundation worker urgently refers onto other services. Intervention / Treatment The SLT picks up the referral and does the initial assessment. She completes a Case history and does a full swallow assessment which includes observation. Betty is found to have differing skill levels in different places. It becomes clear that
There is poor consistency in interpreting Betty’s communication.
There is poor consistency in how to position Betty when eating and drinking.
Additionally different cups are used by different people, putting Betty at medium risk of aspiration and choking.
The SLT decides to
refer on to the OT because Betty does not have consistent, safe cups for drinking
Refer to the physio for advice on positioning
She decides to do swallow assessment in all the places where Betty eats and drinks and with a variety of carers and an in-depth communication assessment.
Liaise with the community nurse (who is already involved because of other medical issues) over whether there are issues at home.
The SLT records all her decisions in the Interim plan, and the draft plan is then compiled by the contributing professionals. The E&D team work with the carers to adjust the plan to meet Betty’s needs personally and reduce risks as trialled. During the assessment period, it becomes clear that Betty is not drinking sufficiently. A referral is made to the dietician who does a full assessment. The E&D team decide to consider whether alternative means of hydration would be indicated. The E&D team gather the relevant information and host a MCA meeting choosing to follow Best Interest guidelines to involve her in the decision.
Go back to Pathway
Page 34 of 36
The team use the communication passport which the SLT compiled to involve Betty wherever possible. The outcome is to have Betty assessed for PEG insertion to support hydration. The community nurse liaises with the Specialist nurse for LD and Gastroenterology department at the local hospital. The operation is subsequently recommended by the surgeon. Following another Best interest meeting, the operation goes ahead. The Community nurse sets up training and assessing for competency to administer a PEG feed for the home day service and respite care. The community nurse works closely with the HENS dietetic service in implementing the first few feeds at home and day care. The physiotherapist works with wheelchair services to explore positioning to maximise socialisation and positioning for PEG due to Betty’s stature.
Patient Reported Outcome Measure
Reference List
1. Accessible Information Standard (2015) NHS https://www.england.nhs.uk/wp-content/uploads/2015/07/access-info-upd-er-july-15.pdf accessed 24.3.2016
2. Aldridge, K and Taylor, N. (2012) Dysphagia is a common and serious problem for Adults with Mental Illness. Dysphagia 27:124-137 http://www.rcslt.org/speech_and_language_therapy/commissioning/dysphagia_manual_ accessed Dec 2014
3. Adherence to Eating and Drinking Guidelines for Adults with Intellectual Disabilities and Dysphagia. Chadwick, Jolliffe and Goldbart (May 2003) American journal on mental retardation, vol. 108, no. 3, pp. 202-211
4. Clinical Commissioning Guide 2013 Improving the Health and Wellbeing of People with Learning Disabilities: An Evidence-Based Commissioning Guide for Clinical Commissioning Groups (CCGs) Accessed at http://www.rcgp.org.uk/learningdisabilities/~/media/Files/CIRC/LD%20Commissioning/RCGP%20LD%20Commissioning%20Guide%20v1%200%202012%2009%2024%20FINAL%20pdf.ashx on 29th April 2015
5. Confidential Inquiry into premature deaths of people with learning disabilities (CIPOLD) Heslop, Blair, CIPOLD 2013 Accessed http://www.bristol.ac.uk/media-library/sites/cipold/migrated/documents/fullfinalreport.pdf on 29th April 2015
6. Death by indifference, MENCAP (2007)
7. Emerson, E., & Robertson, J. (2008). Commissioning person-centred, cost-effective,
local support for people with learning difficulties. London: Social Care Institute for
Excellence.
8. Emerson, E., Baines, S., Allerton, & Welsh, V. (2011). Health Inequalities and
People with Learning Disabilities 2011. Improving Health and Lives Learning
Go back to Pathway
Page 35 of 36
Disabilities Public Health Observatory
http://www.improvinghealthandlives.org.uk/publications/978/Health_Inequalities_&_
People_with_Learning_Disabilities_in_the_UK:_2011
9. Evaluation and Treatment of Swallowing Disorders. Second Ed. Logemann,J Pro-Ed,Texas. 1998
10. How people with Learning Disabilities die Glover and Ayub 2010 accessed https://www.improvinghealthandlives.org.uk/publications/928/How_people_with_learning_disabilities_die on 29.5.2014
11. Kelly, A. (2000) Adults with Learning Disabilities, Chapter 6, Speechmark
12. Kindell, J. (2002) Feeding and Swallowing Disorders in Dementia., Speechmark
13. Predictors of Aspiration Pneumonia: How important is Dysphagia? Langmore, Terpenning. Schork, Chen, Murray, Lopatin, Loesche (1998) Dysphagia 13:69–81
14. Leslie, P. Crawford, H and Wilkinson (2009) People with a learning disability and dysphagia: A Cinderella Service?. Dysphagia 24.
15. Mansell, J (1998) Healthcare for people with learning disabilities Tizard Learning
Disability review Vol 3 Issue 4
16. Michael, J (2008). Healthcare for all: Independent Inquiry into Access to Healthcare for People with Learning Disabilities Sir Jonathan Michael (2008)
17. National Patient Safety Agency (2007). Problems swallowing? Ensuring safer practice for adults with learning disabilities who have dysphagia
18. NICE clinical guidelines CG32 :Nutritional support in adults 2006 Published 2006, Review 2014 and not for changes. Available at https://www.nice.org.uk/guidance/cg32 Accessed 29th April 2015
19. Reducing the risk of choking for people with a learning disability A Multi-agency review in Hampshire 2012 Accessed http://documents.hants.gov.uk/adultservices/safeguarding/Reducingtheriskofchokingforpeoplewithalearningdisability.pdf April 29th 2015
20. Six lives :the provision of public services to people with learning disabilities (2009) Health Ombudsman
21. Thacker, A. Abdelnoor, A. Anderson, C. White, S. Hollins, S.(2007) Indicators of
choking risk in adults with learning disabilities: A questionnaire survey and interview
study. Disability and rehabilitation, 30 (15): 11312-1138.
22. Watson, Chadwick, Stobbart and Kelly.Dysphagia in Adults with learning disabilities
: Findings from the dysphagia working party National Patient Safety Agency 2006
Go back to Pathway

Page 36 of 36
23. Wright D, Beavon N, Branford D, Griffith R, Harding C, Howseman T, Rasmussen J,
Sandhu B, Shmueli U, Smith A, White A (2012) Guideline for the identification and
management of swallowing difficulties in adults with learning disability RCGP
Go back to Pathway