Embed Size (px)
Citation preview

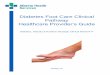
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:
Eating Disorder
Pre-
treat
men
t eva
luat
ion
Chem
10,
AST
/ALT
, GG
T, a
lkal
ine
phos
phat
ase,
ferr
itin,
% ir
on sa
tura
tion,
T4
& T
SH, a
lbum
in, p
re-a
lbum
in, t
rigly
cerid
es, C
BC w
/di
ffere
ntia
l, U
A, u
rine
for h
CG, 1
2-le
ad E
KG(if
test
s wer
e re
cent
ly co
mpl
eted
, use
pro
vide
r disc
retio
n w
heth
er o
r not
to re
peat
)
Adm
issio
n Cr
iteria
1
(1 o
r mor
e)
Patie
nt d
oes n
ot m
eet
inpa
tient
crit
eria
Cons
ider
beh
avio
ral h
ealth
co
nsul
t for
par
tial
hosp
italiz
atio
n pr
ogra
ms o
r ou
tpat
ient
coun
selin
g, a
nd
notif
y PC
P
May
alw
ays c
all P
sych
iatr
y or
Hos
pita
l Med
icin
e to
di
scus
s
Adm
it to
Hos
pita
l Med
icine
PC
P or
ED
prov
ider
revi
ews c
linic
al p
athw
ay m
anag
emen
t w
ith p
atie
nt a
nd fa
mily
2
ED
pro
vide
r giv
es p
atie
nt a
nd fa
mily
the
Patie
nt H
ando
ut
that
out
lines
exp
ecta
tions
dur
ing
the
adm
issio
n (s
ee
Appe
ndix
C)
If
patie
nt 1
8 ye
ars,
mus
t cal
l hos
pita
list t
o di
scus
s ad
miss
ion
Initi
al M
anag
emen
t
Patie
nt h
ando
ut to
be
revi
ewed
and
sign
ed b
y th
e pa
tient
an
d fa
mily
at t
ime
of a
dmiss
ion
(see
App
endi
x C)
Pl
ace
patie
nt in
1:1
obs
erva
tion
Pl
ace
patie
nt o
n co
ntin
uous
CR
mon
itorin
g
Ord
er st
rict I
/O s
Pl
ace
appr
opria
te c
onsu
lts. C
alls
for c
onsu
lts m
ay n
eed
tobe
pla
ced
the
follo
win
g m
orni
ng if
late
adm
issio
n.
Psyc
hiat
ry c
onsu
lt
Nut
ritio
n co
nsul
t
PCA
to p
rint N
ursin
g/PC
A Jo
b Ai
d (A
ppen
dix B
) and
N
ursi
ng/P
CA P
roto
col W
orks
heet
(App
endi
x I)
Plea
se co
ntin
ue to
pag
e 2
for s
peci
fics o
f inp
atie
nt
man
agem
ent.
1 Adm
issio
n Cr
iteria
<7
5% m
BMI O
R <8
0%m
BMI i
f < 1
0 ye
ar o
f age
or
pre-
men
arch
al
Acut
e fo
od re
fusa
l > 2
4hrs
HR
4
0 bp
m su
pine
&
rest
ing
(con
sider
if
45
with
oth
er c
riter
ia)
S y
stol
ic B
P <8
0 m
mH
g
Ort
host
atic
chan
ges i
n SB
P(>
20 m
mH
g)
Sync
ope
or p
re-s
ynco
pew
ith st
andi
ng
Elec
trol
yte
dist
urba
nces
(e
.g. h
ypok
alem
ia,
hypo
phos
phat
emia
, hy
pom
agne
sem
ia,
hypo
chlo
rem
ia)
De
hydr
atio
n
Tem
pera
ture
<36
°C
Arrh
ythm
ia (p
rolo
nged
Q
Tc)
In
trac
tabl
e vo
miti
ng o
r he
mat
emes
is
Failu
re o
f out
patie
nttr
eatm
ent
No
Yes
2 Exa
mpl
e sc
ript f
or E
D w
hen
notif
ying
of a
dmiss
ion:
You
r chi
ld is
bei
ng a
dmitt
ed
for m
edic
al st
abili
zatio
n fo
r m
alnu
triti
on d
ue to
di
sord
ered
eat
ing.
The
tr
eatm
ent r
equi
res a
st
ruct
ured
app
roac
h, w
ith
slow
and
gra
dual
re-
intr
oduc
tion
of n
utrit
ion
in a
sa
fe w
ay.
Ther
e is
an
initi
al
rest
rictio
n of
act
ivity
and
pr
ivile
ges
are
gain
ed th
roug
h co
mpl
ianc
e w
ith th
e tr
eatm
ent p
lan.
Inclu
sion
Crite
ria: D
isord
ered
eat
ing
and
mal
nutr
ition
Exclu
sion
Crite
ria: A
ctiv
e ga
stro
inte
stin
al p
atho
logy
cau
sing
mal
nutr
ition
PCP
and/
or ED
Ass
essm
ent
Hist
ory o
f: w
eigh
t los
s, bi
ngin
g/pu
rgin
g, d
iet (
inta
ke),
alco
hol o
r sub
stan
ce u
se, m
edic
atio
ns, e
xerc
ise,
sync
ope,
men
stru
al p
erio
ds
Phys
ical:
heig
ht &
wei
ght w
ith %
med
ian
BMI (
% m
BMI -
see
Appe
ndix
A),
orth
osta
tic B
P an
d HR
, hyd
ratio
n st
atus
, car
diac
and
pe
riphe
ral e
xam
, sig
ns o
f int
entio
nal v
omiti
ng (d
enta
l ero
sion,
knu
ckle
abr
asio
ns)
©2019 Connecticut Children’s. All rights reserved. 19-004
NEXT PAGE
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:
Eating Disorder
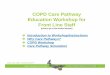
VITA
L SI
GN
SQ
4HR
LABS
& D
IAGN
OST
ICS
ACTI
VITY
& 1
:1
OBS
ERVA
TIO
N S
TATU
S
Ort
host
atic
s:
Obt
ain
1st se
t on
adm
issio
n
If or
thos
tatic
for B
Por
HR,
take
dai
ly
until
nor
mal
ized
Wei
ght:
W
eigh
pat
ient
QAM
af
ter 1
st v
oid
and
befo
re b
reak
fast
Wei
ght t
o be
don
ein
hos
pita
l gow
n on
ly (n
o so
cks,
un
derw
ear e
tc.)
N
eith
er p
atie
nt n
or
fam
ily a
re to
be
told
th
e w
eigh
t (m
ay b
e to
ld u
p, d
own
or
sam
e)
Obt
ain
grow
th
char
ts fr
om P
CP
Day
1:
Echo
card
iogr
am fo
r Ea
ting
Diso
rder
pa
tient
s
If no
t pre
viou
sly o
btai
ned
in
the
ED:
U
A
Urin
e hC
G (fe
mal
e pt
s)
Days
2-5
:
i-STA
T Ch
em 1
0 da
ilyfo
r 5 d
ays,
then
PRN
ba
sed
on ri
sk o
f re
feed
ing
synd
rom
e
Adva
ncem
ent b
ased
on
incr
easin
g m
edica
l sta
bilit
y.U
se o
rder
set t
o ch
ange
act
ivity
leve
l.
Leve
l 1 (s
tart
at a
dmis
sion
):
Stric
t bed
rest
due
to V
S in
stab
ility
O
OB
for b
athr
oom
use
onl
y
Plac
e on
1:1
obs
erva
tion
Leve
l 2:
Ad
vanc
e to
this
leve
l onc
e BP
and
orth
osta
tic sy
mpt
oms s
tabi
lize
O
OB
in ro
om fo
r mea
ls
OO
B in
whe
el c
hair
for l
imite
d sc
hedu
led
activ
ities
as
dete
rmin
ed b
y m
edic
al te
am
Show
er b
ased
on
med
ical &
psy
ch
clea
ranc
e
Cont
inue
1:1
obs
erva
tion;
co
nsid
er q
15 m
in c
heck
s ov
erni
ght w
hile
asle
ep
Leve
l 3:
Ad
vanc
e to
this
leve
l onc
e or
al
inta
ke p
rom
otes
wei
ght g
ain
or
wei
ght s
tabi
lity
Fi
rst,
ad li
b ac
tivity
in th
e ro
om
Then
, adv
ance
to 1
-3 fi
ve-m
inut
e w
alks
per
day
(may
adv
ance
mor
e slo
wly
or r
apid
ly b
ased
upo
n m
edic
al st
abili
ty)
Co
nsid
er 1
:1 o
bser
vatio
n on
ly
with
mea
ls an
d 1
hour
aft
er
MED
ICAT
ION
S
Anor
exia
& A
RFID
:
Com
plet
e m
ultiv
itam
in 1
ta
blet
dai
ly
Thia
min
e 10
0 m
g/da
y x7
day
sto
tal
Co
nsid
er T
ums f
or lo
wca
lcium
leve
ls
Cons
ider
ora
l pho
spho
rus
[Pho
s-N
aK co
ntai
ns 2
50m
g Ph
os, 1
60m
g (7
mEq
) Na,
28
0mg
(7.2
mEq
) K]
Co
nsid
er IV
pho
s su
pple
men
tif
phos
phat
e le
vel ≤
2m
g/dL
Bulim
ia:
Co
nsid
er IV
pho
s su
pple
men
tif
phos
phat
e le
vel ≤
2m
g/dL
Co
nsid
er so
dium
bic
arbo
nate
or o
ral B
icitr
a if
bica
rbon
ate
leve
ls ar
e lo
w
Cons
ider
pot
assiu
m
supp
lem
ent i
f low
seru
m K
and
norm
al p
H (i
ndic
ates
da
nger
ous
redu
ctio
n of
tota
l bo
dy K
)
NU
TRIT
ION
& F
LUID
S
Nut
ritio
n:Se
e Ap
pend
ix D
for A
nore
xia,
Ap
pend
ix E
for B
ulim
ia d
iet p
lans
, Ap
pend
ix F
for A
RFID
pla
ns
In
itiat
e m
eal p
lan
imm
edia
tely
afte
r adm
issio
nla
b re
sults
revi
ewed
Di
et a
dvan
ced
per R
D re
com
men
datio
ns
Afte
r eve
ning
sna
ck
com
plet
e, p
lace
nex
t day
’s di
et o
rder
St
art w
ith 2
4oz o
f fre
e w
ater
an
d th
en a
djus
t per
RD
reco
mm
enda
tions
Pl
ace
naso
gast
ric tu
be (N
GT)
afte
r sna
cks i
f not
100
%
com
plia
nt w
ith ca
loric
goa
ls
(per
App
endi
ces
D &
E &
F
rega
rdin
g N
GT fe
edin
gs)
Se
e Ap
pend
ix G
for E
nsur
e re
plac
emen
t gui
delin
e
IV F
luid
s:
Cons
ider
NS
bolu
s and
/or
cont
inuo
us IV
Fs if
mod
erat
e to
seve
re d
ehyd
ratio
n or
pa
tient
refu
sing
PO
flui
ds
PRIV
ILEG
ES
Adva
ncem
ent b
ased
on
com
plia
nce
with
the
diet
pl
an.
Use
ord
er se
t to
add
priv
ilege
s.
See
Appe
ndix
H fo
r list
of
priv
ilege
s;Se
e Ap
pend
ix I
for n
ursin
g/PC
A pr
otoc
ol w
orks
heet
Di
scus
s the
pat
ient
’sco
mpl
ianc
e fo
r the
day
af
ter 8
:30p
m sn
ack
If
100%
com
plia
nt w
ithbo
th so
lids &
liqu
ids
(incl
udes
wat
er a
nd
mak
e-up
liqu
id
nutr
ition
supp
lem
ent)
, pa
tient
can
iden
tify
the
next
day
’s p
rivile
ge
Ord
er th
e ne
xt d
ay’s
pr
ivile
ge to
beg
in th
e fo
llow
ing
day
at 9
am
Do n
ot s
tart
ho
mew
ork;
will
be
cons
ider
ed p
er P
sych
te
am
Disc
harg
e Cr
iteria
/Med
icat
ions
:
Med
ical
ly c
lear
ed w
ith st
able
labs
and
vita
l sig
ns
Patie
nt a
dher
ent t
o pr
escr
ibed
nut
ritio
n pl
an w
ith w
eigh
t gai
n, e
spec
ially
with
ad
lib a
ctiv
ity
Appr
opria
te p
lace
men
t arr
ange
d in
inpa
tient
, PHP
or o
utpa
tient
pro
gram
with
psy
chia
try
team
inpu
t
Med
icat
ions
at d
ischa
rge:
com
plet
e m
ultiv
itam
in; t
hiam
ine
(if 7
day
s not
com
plet
e)
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix A: Guide to Calculating % Median BMI
APPENDIX A: Guide to Calculating % Median BMI
Steps:
1. Find patient’s BMI using the following link (need patient’s height & weight):https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm
2. Using a CDC growth/BMI chart (or one of the links below):BOYS:
http://www.cdc.gov/growthcharts/data/set2clinical/cj41c073.pdfGIRLS:
http://www.cdc.gov/growthcharts/data/set1clinical/cj41l024.pdf
Find the BMI at the 50th percentile* for the patient’s age.
3. % Median BMI (mBMI) = Patient’s BMI ÷ BMI at 50th %* for age
Example:15 year old girl has a BMI of 14 (based on entering her height & weight in Step #1)BMI at 50th percentile for age = 20 (based on BMI chart in Step #2)
% mBMI = 14 ÷ 20 = 70%
* The dietitian and/or medical team may adjust the patient’s % mBMI to a different BMI %ile (other than 50th%ile)based on the patient’s previous growth history (e.g. if the patient has tracked at the 25th percentile prior to weightloss, use this for mBMI calculation).
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix B: Nursing/PCA Job Aid
APPENDIX B: Nursing/PCA Job Aid
Vital Signs: q4hr Orthostatic vital signs (“Orthostatics”) HR and BP when supine, sitting and standing:
• Obtain 1st set on admission• If Orthostatic for BP or HR, take daily until normalized
Weight: • Weigh patient qAM after 1st void and before breakfast• Weigh patient in hospital gown only (no socks, underwear etc.)• Neither patient nor family are to be told the weight (may be told up, down or the same)
Lowest heart rate per shift • PCA document the lowest heart rate noted each shift in the vital signs flowsheet in Epic
Nutrition and Fluids: • See Appendix C (Patient Handout) for detailed Meal Guidelines. See Appendix D for Anorexia meal
plan, Appendix E for Bulimia meal plan, & Appendix F for Avoidant Restrictive Food Intake Disorder(ARFID)
• Make-up liquid nutrition supplement will be offered with snacks 3 times per day as needed if not100% compliant with meals
• NG tube will be placed after each snack if not 100% compliant with make-up• NGT exceptions: Consider waiting in patients <11 years. Consider not removing/replacing if NGT is
needed twice or more regardless of age.
Activity Status: Patient will be admitted to Activity Level 1. Activity level is advanced based on increasing medical stability. Providers use the eating disorder order set to change activity level.
Level 1: • Strict bed rest due to vital sign instability• Out of Bed for bathroom use only• On 1:1 observation
Level 2: Advance to this level once BP and orthostatic symptoms stabilize • Out of bed in room for meals• Out of bed in wheelchair for scheduled floor activities as determined by medical team• Shower based on medical and psychiatric team clearance• Continue 1:1 observation; consider q15 min checks overnight while asleep
Level 3: Advance to this level once oral intake promotes weight gain • First, ad lib activity in room• Then, advance to 1-3 five-min walks per day (advancement based on medical stability)• Consider 1:1 observation only with meals and 1 hour after
Privileges: Advancement based on compliance with the diet plan. Order set used to add privilege. See Appendix H for list of privileges, see Appendix I for nursing/PCA protocol worksheet.
• Determine the patient’s compliance for that day right after the 8:30pm snack• If 100% compliant with both solids and liquids (includes water & make-up Ensure), patient can
identify the next day’s privilege in the evening to begin the following day at 9am• Do not start homework. Will be considered per psych team
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY: Eating Disorder Appendix C: Patient Handout
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19
APPENDIX C
Patient Handout You have been admitted to the hospital because your physician determined that it was medically necessary to hospitalize you to ensure your safety and restore your physical health. This protocol was developed to assure that your hospitalization achieves these goals. If you have any questions about this protocol, please discuss with your nurse or doctor. Your team will keep you up to date with your progress during your hospital stay.
Patient Protocol Wake Up/Dress Guidelines:
1. At the time of admission, you will be asked to dress in a hospital gown.2. You need to wake up, get weighed and be dressed prior to breakfast.3. Clothing per medical team determination.
Weight Guidelines: 1. You will need to be weighed daily before breakfast, after the first morning urination, in a hospital gown
only. No other clothing (i.e. underwear, socks, slippers, or shoes) will be worn.2. You will use the bathroom to urinate prior to being weighed.3. No jewelry is to be worn.4. You may not eat, drink, bathe, or brush your teeth before getting weighed.5. You must stand on the scale with your back toward the weight.6. Neither you nor your family will be told your actual weight, but you will be told the general trend of up,
down, or the same.
Meal Guidelines: 1. There will be 6 mini-meals per day. Each day, if you are 100% compliant, your meals will be advanced
through a system, as directed by your Registered Dietician (RD), who will be in charge of creatingbalanced meal plans that meet your nutritional and caloric needs. You will be allowed to pick 3 fooddislikes with the RD on the first full day, which will take into effect on the following day’s meal plan. Allmeals will be supervised by staff.
a. Food meal plans will be provided starting on the first full day on the protocol. If you are admittedin the evening hours or overnight, you will be provided crackers and liquid nutrition supplementsuch as Ensure for that meal time until the following morning. If you are admitted in the morningor mid-day, it will be determined by the medical team if you can start with food mealsimmediately.
2. There will be no visitors and no activities allowed during mealtime, unless receiving meal support from afamily member or the Patient Care Assistant (PCA). The readiness of a family member to provide mealsupport will be determined by the psychiatry team after initial evaluation, observation and education withthe family.
3. Staff will check your tray for accuracy prior to each meal. No food substitutions are allowed.4. You will have 30 minutes to complete each mini-meal. After that time, the tray will be removed from your
room.5. Approximate meal times are:
Breakfast = 8:00am – 8:30am Snack = 10:00am – 10:30am Lunch = 12:00pm – 12:30pm Snack = 2:30pm – 3:00pm Dinner = 5:00pm – 5:30pm Snack = 8:30pm – 9:00pm
6. Staff will record food intake on a protocol worksheet.7. No food, beverages, cups, or dishes are allowed in your room, including the food/beverage of family
members.

8. Meal plans are advanced in the evening based on compliance and will begin at breakfast the nextmorning.
9. 100% compliance with daily nutrition (food & water) is expected.10. If you are unable to meet 100% compliance, you will have the opportunity to take in the missed calories
from a meal at the next snack by drinking a nutrition supplement.11. If you are unable to make up the calories from the liquid nutrition supplement, a feeding tube, called a
Nasogastric Tube (NGT) will be considered. An NGT will be placed at the end of each snack time if youdo not consume the goal calories for that snack and the prior meal. The remainder of the calories will beprovided with a nutrition supplement via the NGT. The NGT will be taken out when it is completed. Youwill then have a “fresh start” to be able to achieve 100% compliance with the next meal and snack.
Unit Environment: 1. The family kitchen is off limits.2. Bedside curtains must be kept open, except when dressing.3. There is no bathroom use for 1 hour after all meals.4. Bathroom use is supervised by staff.5. Staff will measure urinary output after each void.6. You will be placed on constant observation on admission. This means there will be a PCA who sits
outside your door to provide safety and support, and monitor for any disordered eating behaviors.7. Inappropriate language or threatening behavior is not acceptable.8. All medications brought from home must be given to your nurse upon admission.9. We ask that families do not discuss meals, weight, or other eating-related topics, as these topics may
raise anxiety. The treatment team will help guide the family as to appropriate discussions and mealsupport.
Visiting: 1. Immediate family and clergy may visit at any time, except mealtime, unless otherwise ordered by the
team.2. Friends and extended family members may only visit after the privilege has been obtained per this
protocol.
Activity: 1. All patients are admitted on bedrest.2. You will be placed on a cardiac monitor upon admission. This means stickers on your chest will measure
your heart rate and breathing. The duration of cardiac monitoring depends on your medical condition.3. Vital signs (blood pressure, heart rate, breathing rate and temperature) will be taken at least every 4
hours, or more frequently, if your medical condition warrants.4. Any transports for medical care off the unit must be via wheelchair or stretcher.5. The patient and family will be updated daily regarding advancements in activity level. Activity level will be
advanced as the medical status improves. All patients are admitted on Activity 1 (bed rest) and activity isprogressed as nutritional status stabilizes and will be identified by level 1, 2, and 3 with increasing abilityto leave the room in a wheelchair and move about the room out of bed. Medical stability requirements foreach activity level can be described by the medical team in the sequence per protocol. If the family and/orpatient need clarification of a privilege or activity level, they are encouraged to check with the medicalteam, nurse, or PCA.
Privileges: 1. You will be admitted to a room without TV, phone, or other in-room activities. Throughout your hospital
stay, you may earn these “privileges” based upon 100% compliance with your daily meal plan. If you havebeen 100% compliant with all food and drink (includes water and make-up liquid nutrition supplement) forthe entire day, you will be able to earn a privilege (listed on the Privilege Menu) for the following day.
THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix C
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix C
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19
2. On any given day, if you are not 100% compliant, then you will not obtain an additional privilege.Previously obtained privileges will not be lost.
3. Privileges for the next day must be selected and communicated to the staff by 10:00pm and the staff willdocument the choice on the care plan.
4. Privileges advance at 9:00am the following day.
Date Reviewed with Patient:
Patient Signature: (signature indicates patient received a copy of this handout)

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix D: Meal Plan for a Child with Anorexia Nervosa
APPENDIX D: Meal Plan for a Child with Anorexia Nervosa
The goal of the meal plan for the first 4 days is to prevent further weight loss and to encourage patient to eat by mouth. The patient may not gain weight initially. Do not share calorie levels with patient.
No additional coffee, tea, diet soda, or juice. Free water as below.
Step One: (1500 total calories per day) 6 standardized meals. Meal plans per Clinical Nutrition to be determined on the first morning following admission. Prior to Clinical Nutrition consultation, each meal will be 230 ml of Ensure + 1 packet of saltine crackers which can be initiated and provided in ED or upon arrival to the floor. Minimum of 24oz of water per 24-hour period. Continue until patient complies with Step One. During Step One, the patient will be allowed to choose 3 food dislikes, but will be told that the Registered Dietician (RD) will choose the meal plan to meet the patient’s nutritional needs. The dislikes will be included on the next day’s meal plan.
Step Two: (1800 total calories per day) 6 standardized meals per Clinical Nutrition. Minimum of 24oz of water per 24-hour period. Continue until patient complies with Step Two.
Step Three: (2100 total calories per day) 6 standardized meals per Clinical Nutrition. Minimum of 24oz of water per 24-hour period.
Step Four: Increase intake by 20% or 200-300 kcal/day to a goal set by Clinical Nutrition. Step number continues to advance until reaching adequate intake, as determined by Clinical Nutrition.
The decision to begin nasogastric tube (NGT) feedings is based on medical necessity as determined by the multi-disciplinary team. If a patient does not finish an entire meal (breakfast, lunch, dinner), he/she will have the opportunity to take in the missed calories at the next snack by drinking a liquid nutrition supplement (Refer to Appendix G; consult with Diet Tech if needed). An NGT will be placed at the end of each snack time if the patient does not consume the goal calories for that snack and the prior meal. The remainder of the calories will be provided via the NGT. The NGT will then be removed when the feeding is completed. The patient will then be allowed a “fresh start” to be able to achieve 100% compliance with the next meal.
The decision to place an NGT in a patient < 11 years old will be determined by the multi-disciplinary team.
If a patient has needed an NGT more than twice, in consultation with psychiatry, consideration should be made to keep the NGT in place, particularly if there has been no progress in PO feeds after the NGT is pulled.
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix E: Meal Plan for a Child with Bulimia Nervosa
APPENDIX E: Meal Plan for a Child with Bulimia Nervosa
All meals/snacks should contain adequate fat and fiber to prevent excessive feelings of hunger.
The goal of the meal plan for the first 4 days is to prevent further weight loss and to encourage patient compliance. The patient may not gain weight initially. Do not share calorie levels with patient.
Allow additional fluids after eating the meal as planned. Restrictions on patients who are meeting meal goals are not recommended.
Step One: Starts with the first meal after admission (1500 total calories per day). Three meals + three snacks. Minimum of 24oz of water per 24-hour period. Patient selects foods from modified menu. Continue until patient complies with Step One.
Step Two: (1750 total calories per day) Three meals + three snacks. Minimum of 24oz of water per 24-hour period. Patient selects foods from modified menu. Continue until patient complies with Step Two.
Step Three: (2000 total calories per day) Three meals + three snacks. Minimum of 24oz of water per 24-hour period. Patient selects foods from modified menu.
Step Four through discharge: Increase intake by 20% or 100-200 kcal/day to achieve goal established by Clinical Nutrition.
The decision to begin nasogastric tube (NGT) feedings is based on medical necessity as determined by the multi-disciplinary team. If a patient does not finish an entire meal (breakfast, lunch, dinner), he/she will have the opportunity to take in the missed calories at the next snack by drinking a liquid nutrition supplement (Refer to Appendix G; consult with Diet Tech if needed). An NGT will be placed at the end of each snack time if the patient does not consume the goal calories for that snack and the prior meal. The remainder of the calories will be provided via the NGT. The NGT will then be taken out when the feeding is completed. The patient will then be allowed a “fresh start” to be able to achieve 100% compliance with the next meal.
If a patient has needed an NGT more than twice, in consultation with psychiatry, consideration should be made to keep the NGT in place, particularly if there has been no progress in PO feeds after the NGT is pulled.
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix F: Meal Plan for a Child with Avoidant Restrictive Food Intake Disorder (ARFID)
APPENDIX F: Meal Plan for a Child with Avoidant Restrictive Food Intake Disorder (ARFID)
The goal of the meal plan for the first 4 days is to prevent further weight loss and to encourage patient to eat by mouth. The patient may not gain weight initially. Do not share calorie levels with patient.
No additional coffee, tea, diet soda, or juice. Free water as below.
Step One: (1500 total calories per day) 6 standardized meals. Meal plans per Clinical Nutrition to be determined on the first morning following admission. Prior to Clinical Nutrition consultation, each meal will be 230 ml of Ensure + 1 packet of saltine crackers which can be initiated and provided in ED or upon arrival to the floor. Minimum of 24oz of water per 24-hour period. Continue until patient complies with Step One. During Step One, the patient will be allowed to choose 3 food dislikes, but will be told that the Registered Dietician (RD) will choose the meal plan to meet the patient’s nutritional needs. The dislikes will be included on the next day’s meal plan.
Step Two: (1800 total calories per day) 6 standardized meals per Clinical Nutrition. Minimum of 24oz of water per 24-hour period. Continue until patient complies with Step Two.
Step Three: (2100 total calories per day) 6 standardized meals per Clinical Nutrition. Minimum of 24oz of water per 24-hour period.
Step Four: Increase intake by 20% or 200-300 kcal/day to a goal set by Clinical Nutrition. Step number continues to advance until reaching adequate intake, as determined by Clinical Nutrition.
The decision to begin nasogastric tube (NGT) feedings is based on medical necessity as determined by the multi-disciplinary team. If a patient does not finish an entire meal (breakfast, lunch, dinner), he/she will have the opportunity to take in the missed calories at the next snack by drinking a liquid nutrition supplement (Refer to Appendix G; consult with Diet Tech if needed). An NGT will be placed at the end of each snack time if the patient does not consume the goal calories for that snack and the prior meal. The remainder of the calories will be provided via the NGT. The NGT will then be removed when the feeding is completed. The patient will then be allowed a “fresh start” to be able to achieve 100% compliance with the next meal.
The decision to place an NGT in a patient < 11 years old will be determined by the multi-disciplinary team.
If a patient has needed an NGT more than twice, in consultation with psychiatry, consideration should be made to keep the NGT in place, particularly if there has been no progress in PO feeds after the NGT is pulled.
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix G: Meal Plan Calorie Key for Ensure Replacement
APPENDIX G: Meal Plan Calorie Key for Ensure Replacement
For each food item not consumed, please replace with the following Ensure (30 kcal/oz) equivalent:
1 starch = 80 ml Ensure
1 protein = 45 ml Ensure
1 fat = 45 ml Ensure
1 dairy = 120 ml Ensure
1 fruit = 60 ml Ensure
1 vegetable = 30 ml Ensure
1 packet saltine crackers = 25 ml Ensure
* 1 calorie is equivalent to 1 ml of Ensure (30 kcal/oz)
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix H: Privilege Menu
APPENDIX H: Privilege Menu
Patient Name: Date:
One privilege may be added for each day of 100% compliance with all 6 mini-meals (this includes make-up Ensure). Please circle your choice by 10:00pm today. Your privilege will begin at 9:00am tomorrow.
Arts & Crafts Hospital phone in room (not personal mobile phone)
Writing Reading
TV & Movies Visitors
Games & Video Games Music (No wireless devices) (CD player, Keyboard, other)
(No wireless devices)
Wheelchair rides (Once medically stable = activity level 2 or greater) (Three 5-minute rides per day)
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19

THIS PATHWAY SERVES AS A GUIDE AND DOES NOT REPLACE CLINICAL JUDGMENT.
CLINICAL PATHWAY:Eating DisorderAppendix I: PCA Protocol Worksheet
APPENDIX I: PCA Protocol Worksheet
Patient Name: Date: Unit:
Date Day Wt (kg) Meal Plan Calories
100% Compliance
Privileges (*Patient Choice)
Activity Level (Assigned)
Comments Eating behaviors/exercise/other
Admit Yes / No Begin on Day 2 at 9:00am, if compliant
Advancement requires
physiologic stability +
weight neutrality or gain w/o IV
fluids
1 Yes / No N/A All patients start at Activity
Level 1
2 Yes / No
3 Yes / No
4 Yes / No
5 Yes / No
6 Yes / No
7 Yes / No
*PRIVILEGES are chosen by the patient. See Pathway and Appendix H for guidance.
©2019 Connecticut Children’s. All rights reserved. 19-004
RETURN TOTHE BEGINNING
CONTACTS: ALYSSA BENNETT, MD | CHRISTINE SKURKIS, MD | LISA NAMEROW, MD | DIANE SIEGEL, RD
LAST UPDATED: 05.22.19