Embed Size (px)
Citation preview

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 1/18
Early diagnosis and treatment of hepatocellular carcinoma
Josep M. Llovet MD
Senior Researcher
Jordi Bruix* MD
Consultant
Liver Unit, Institut de Malalties Digestives, Hospital Clõ Ânic, IDIBAPS, University of Barcelona, Spain
The incidence of hepatocellular carcinoma is increasing world-wide. Although there are norandomized controlled trials showing bene®ts from surveillance programmes, these strategieshave been widely practised by hepatologists, and most early tumours are diagnosed in thesetting of such a policy. In this chapter we summarize the surveillance schedule and recall the
policy applied in our Unit.Diagnosis at an early stage is crucial to allow the application of curative treatments that arethe only hope for increasing the life expectancy of the patient. Surgical resection and livertransplantation are considered the ®rst-line options for early tumours, although there is noagreement on which is the best approach. Resection is limited by the high recurrence rate,whereas the increasing waiting times have decreased the intention-to-treat outcomes of transplantation. Percutaneous treatments are reserved for patients with single non-surgicaltumours. Clinical trials assessing treatments for patients with advanced tumours have notshown any survival bene®ts.
Key words: hepatocellular carcinoma; surveillance; resection; liver transplantation; percuta-
neous ethanol injection; thermal ablation; randomized controlled trials; arterial embolization;survival; prognosis.
Hepatocellular carcinoma (HCC) is a neoplasm with increasing incidence world-widethat a�ects patients with liver cirrhosis, mainly cirrhosis due to chronic hepatitis B andC viral infections.1 The age-adjusted incidence ranges between 5 and 15 cases/105
habitants in Europe and the United States to 27±36 cases/105 habitants in Eastern
Asia.2
Data in patients with chronic liver disease are even more striking because 5% of asymptomatic cirrhotics present with this neoplasm, whereas the prevalence increasesto 15±20% in cirrhotics with acute liver decompensation.3,4 Follow-up studies reporteda 3±6% annual incidence rate5±9 and it is highly controversial whether previous anti-viral therapy with interferon may decrease the cancer development rate.10 The
1521±6926/00/060991�18 $35.00/00 *c 2000 Harcourt Publishers Ltd.
BaillieÁ re's Clinical GastroenterologyVol. 14, No. 6, pp. 991±1008, 2000doi:10.1053/bega.2000.0143, available online at http://www.idealibrary.com on
8
*Address for correspondence: Liver Unit, Institut de Malalties Digestives, Hospital Clõ Ânic, University of Barcelona, Villarroel 170, 08036-Barcelona, Catalonia, Spain.

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 2/18
prognosis for HCC patients depends on tumour stage and degree of liver function thatwill determine the tolerance to invasive treatments.11 Diagnosis at an early stage iscrucial to allow the application of curative treatments that are the only hope of increasing the life expectancy of the patient because at advanced stages there are notreatments that improve survival.
The present chapter analyses the usefulness of surveillance programmes for earlydetection of HCC among cirrhotics, and their cost-e�ectiveness. We describe thesurveillance schedule currently applied in our Unit. Subsequently, results fromtreatments available for HCC are critically reviewed. We focus particularly on theselection of candidates for resection and liver transplantation (OLT) as well as thebene®ts of anti-tumoral treatments during the waiting time for OLT. Moreover, thecurrent knowledge of the bene®ts of percutaneous ablation and other medicaltherapies applied to patients either at an early or an advanced stage of disease will beevaluated.
EARLY DIAGNOSIS OF HCC
Early diagnosis of HCC has become the key point to increase the applicability of curative therapies that are the main chance for improving the life expectancy of HCCpatients. Nowadays, about 25% of HCC patients may bene®t from these therapies3,11,and most of the tumours have been recognized in the setting of surveillanceprogrammes, a policy that is a common practice among hepatologists. The object of these programmes is to reduce the disease-speci®c mortality. However, prospective
clinical trials assessing the e�cacy of such strategies are lacking12, and cost±bene®t dataare still scarce.13 Thus, data to aid decision-making come from non-randomizedsurveillance programmes, either population-based or clinic-based, that provideinformation of its usefulness, but are often limited by speci®c design biases.5±9
Criteria for applying surveillance programmes in HCC
Prorok14 described the following criteria that should be satis®ed in order torecommend a surveillance programme for a speci®c entity. (1) The disease must be
common, with a clear-cut population at risk. (2) There must be a non-invasive accuratediagnostic method. (3) There must be an established e�ective therapy. (4) Thescreening programme should be cost-e�ective. HCC is the kind of tumour that maybene®t from surveillance.
Target population
Surveillance programmes for the early detection of HCC should be addressed to awell-selected population at risk. Several epidemiological studies showed that the mainrisk factors for HCC are older age, male gender and cirrhosis of any aetiology (mainly
related to chronic HBV or HCV infection, or alcohol), which is the most importantfactor.2 In our area, cirrhosis underlies HCC in more than 90% of the cases. The annualincidence of HCC among cirrhotics ranges between 3 and 5%, and 5% of compensatedcirrhotics are diagnosed with HCC if intentionally explored ± a percentage that risesto 15±20% when studying cirrhotics bleeding from gastroesophageal varices or withspontaneous bacterial peritonitis.3,4 In addition, necropsic studies carried out in Japan,Italy and the United States have shown a prevalence of HCC among cirrhotics ranging
992 J. M. Llovet and J. Bruix

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 3/18
from 20 to 80%.15 The heterogeneous geographical distribution of HCC is probablyrelated to the di�erent prevalence of risk factors among di�erent areas of the world.
According to these epidemiological data, in Western countries clinic-basedprogrammes should be conducted in cirrhotic patients. Conversely, implementationof screening programmes in non-cirrhotic patients would not lead to a potential
bene®t. Furthermore, when assessing surveillance programmes in terms of survivalimprovement or cost-e�ectiveness (marginal cost per years of life saved), the earlydetection plans should be restricted to subjects who would be treated with curativetherapies if diagnosed with HCC. Therefore, restrictive criteria of age, stage of liverdisease or baseline conditions that would preclude radical therapies should be assumedwhen surveillance programmes are organized.
Screening test
The most used screening tests for HCC are alpha-fetoprotein (AFP) determination andultrasonography (US). Ultrasonography has shown high sensitivity, speci®city andpredictive values, while AFP lacks acceptable sensitivity in terms of earlydetection.5,7,12 Other tumoral markers which are used have either not yet provento be e�ective or are clearly uneconomical. The interval between screening tests willa�ect both the proportion of HCC detected and the cost of the programme.According to the data published on growth rates of HCC16, it seems reasonable thatthe interval between US varies from 4 to 6 months. Some authors have suggested thatcirrhotic patients with persistent elevated serum AFP levels6 or with liver celldysplasia in cirrhotic tissue are at a specially high risk of developing HCC.17 Whether
these patients would bene®t from a special screening schedule or would be the onlyones in whom screening could be cost-e�ective is unknown.
E�ective therapy
There are no randomized controlled trials (RCT) unequivocally demonstrating that anytherapy is better than standard management for HCC patients. Comparison betweencohort studies may be futile and di�cult to interpret because of the phenomenon of lead-time bias. However, data obtained from cohort studies reported throughout the
last decade suggest that surgical resection, OLT and even percutaneous treatmentsmay change the natural course of the disease and thus can be considered `e�ective' inwell selected patients. Details of these data are described below.
Cost-e�ectiveness
The economical bene®ts of surveillance programmes have been assessed only onthe basis of theoretical models. In that regard, it was suggested that bi-annual screen-ing using AFP and US may provide substantial bene®t (mean gain in life expectancy of 3±9 months) only in well-targeted subgroups of patients (Child±Pugh's status A).13 The
cost-e�ectiveness of these strategies ranged from $26 000 to $55 000 for each additionallife-year gained, even when considering surgical resection as the sole radical option.These cost-e�ectiveness ratios are below the standard threshold quoted as cost-e�ective ($50 000/QALY), and compare favourably with other medical interventionsconsidered reasonable, such as haemodialysis ($42 000/QALY).18 Further studiesassessing all the curative options (including OLT and percutaneous treatments) forHCC are awaited.
Hepatocellular carcinoma 993
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 4/18
Surveillance programmes in HCC and common biases
As previously stated, there are no RCTs assessing the usefulness of surveillance in theearly detection of HCC and its potential bene®t in patients' survival. Nowadays, such
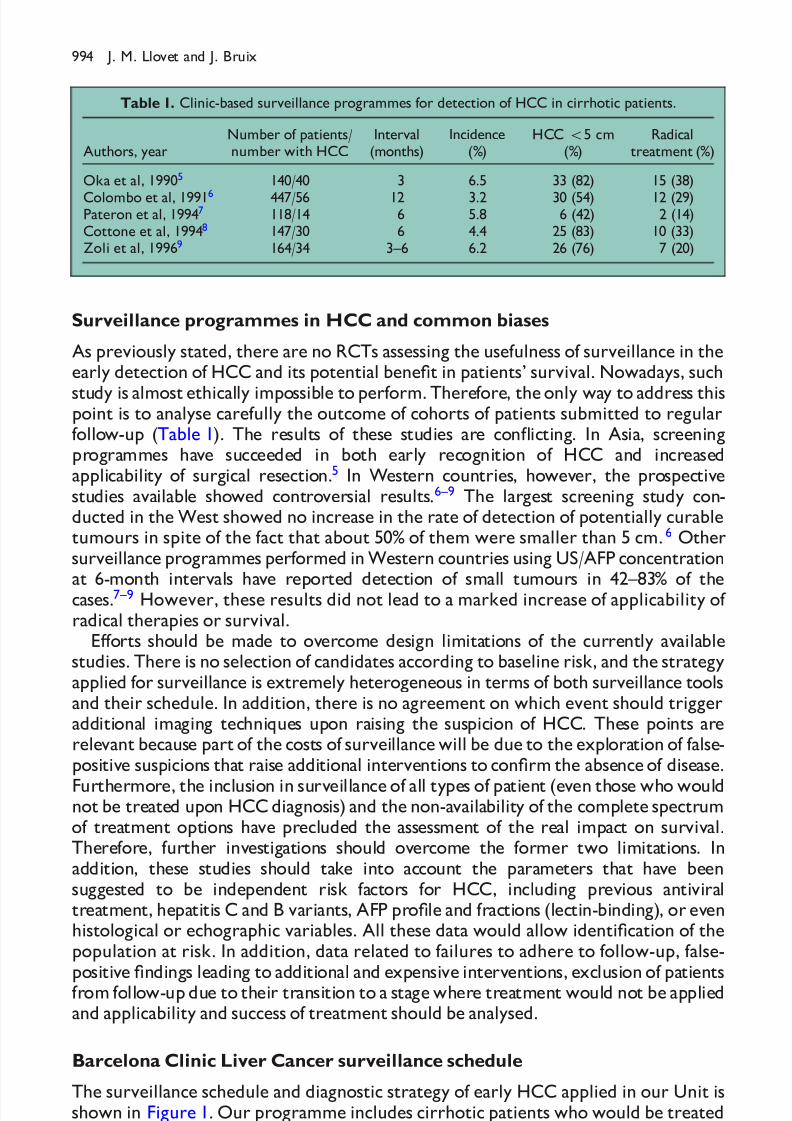
study is almost ethically impossible to perform. Therefore, the only way to address thispoint is to analyse carefully the outcome of cohorts of patients submitted to regularfollow-up (Table 1). The results of these studies are con icting. In Asia, screeningprogrammes have succeeded in both early recognition of HCC and increasedapplicability of surgical resection.5 In Western countries, however, the prospectivestudies available showed controversial results.6±9 The largest screening study con-ducted in the West showed no increase in the rate of detection of potentially curabletumours in spite of the fact that about 50% of them were smaller than 5 cm.6 Othersurveillance programmes performed in Western countries using US/AFP concentrationat 6-month intervals have reported detection of small tumours in 42±83% of thecases.7±9 However, these results did not lead to a marked increase of applicability of radical therapies or survival.
E�orts should be made to overcome design limitations of the currently availablestudies. There is no selection of candidates according to baseline risk, and the strategyapplied for surveillance is extremely heterogeneous in terms of both surveillance toolsand their schedule. In addition, there is no agreement on which event should triggeradditional imaging techniques upon raising the suspicion of HCC. These points arerelevant because part of the costs of surveillance will be due to the exploration of false-positive suspicions that raise additional interventions to con®rm the absence of disease.
Furthermore, the inclusion in surveillance of all types of patient (even those who wouldnot be treated upon HCC diagnosis) and the non-availability of the complete spectrumof treatment options have precluded the assessment of the real impact on survival.Therefore, further investigations should overcome the former two limitations. Inaddition, these studies should take into account the parameters that have beensuggested to be independent risk factors for HCC, including previous antiviraltreatment, hepatitis C and B variants, AFP pro®le and fractions (lectin-binding), or evenhistological or echographic variables. All these data would allow identi®cation of thepopulation at risk. In addition, data related to failures to adhere to follow-up, false-positive ®ndings leading to additional and expensive interventions, exclusion of patientsfrom follow-up due to their transition to a stage where treatment would not be appliedand applicability and success of treatment should be analysed.
Barcelona Clinic Liver Cancer surveillance schedule
The surveillance schedule and diagnostic strategy of early HCC applied in our Unit isshown in Figure 1. Our programme includes cirrhotic patients who would be treated
Table 1. Clinic-based surveillance programmes for detection of HCC in cirrhotic patients.
Authors, yearNumber of patients/number with HCC
Interval(months)
Incidence(%)
HCC 55 cm(%)
Radicaltreatment (%)
Oka et al, 19905 140/40 3 6.5 33 (82) 15 (38)
Colombo et al, 19916 447/56 12 3.2 30 (54) 12 (29)Pateron et al, 19947 118/14 6 5.8 6 (42) 2 (14)Cottone et al, 19948 147/30 6 4.4 25 (83) 10 (33)Zoli et al, 19969 164/34 3±6 6.2 26 (76) 7 (20)
994 J. M. Llovet and J. Bruix

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 5/18
if diagnosed with early HCC. Most of them are patients belonging to Child±Pugh'sclass A or B, without associated severe disease. Diagnosis of cirrhosis is based on liverhistology or clinical criteria. This last point include patients with chronic liver diseaseof known aetiology associated with clinically relevant portal hypertension (de®ned aseither (a) the presence of oesophageal varices, (b) splenomegaly with platelet count4100 000/mm3, or (c) hepatic venous pressure gradient 510 mmHg in the hepatichaemodynamic study).19
At baseline, all patients are examined by conventional biochemical analysis (includingAFP) and US in order to rule out unknown HCC. Follow-up consists of regular US andAFP determination every 6 months. This interval is based on the available data ontumour growth during the early stages. US is performed by experienced observers toregister the ®ndings and con®dently establish the presence/absence of suspiciousnodules. Any nodule detected during surveillance is registered and the policy to followdepends on the size of the detected foci. During follow-up, patients are withdrawn fromthe programme when any exclusion criteria at entry have emerged ± for example,Child±Pugh's C class or associated diseases.
Criteria for raising suspicion of HCC
Suspicion of HCC is raised upon detecting an hepatic nodule 510 mm by US or asigni®cant increase in AFP. This last criterion is de®ned by doubling baseline AFP levels520 ng/ml if previously normal, or AFP levels 450 ng/ml if previously unknown.These patients will be further explored by spiral CT and/or US-guided biopsy. Patientspresenting a detectable hepatic nodule 510 mm are followed for 3 months to detectfurther growth or to monitor its stability. Upon detecting tumour growth or anincrease in AFP concentration, HCC suspicion is con®rmed by additional explorations.
Cirrhotic patients* Surveillance (US+AFP/6 m)
Liver mass No liver mass
US+AFP/3 m Spiral CT
No HCC
HCC Surveillance US+AFP/6 m
>1 cm
FNAB/Spiral CT
MRI and/or
Angiography
<1 cm Increased AFP** Normal AFP
Figure 1. Barcelona Clinic Liver Cancer (BCLC) surveillance schedule. *Cirrhotic patients suitable forcurative treatments if diagnosed with HCC. **Doubling baseline AFP levels520 ng/ml if previously normal,or AFP levels 450 ng/ml if previously unknown. FNAB, ®ne needle aspiration biopsy.
Hepatocellular carcinoma 995

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 6/18
Diagnosis con®rmation and tumour staging
The ®nal diagnosis of HCC is based on cyto-histological ®ndings. Non-histologicaldiagnosis of HCC remains controversial. In our Unit, in case of negative histologicalresults, all the following criteria are requested for the diagnosis. (1) Focal lesion
demonstrated by at least two imaging techniques out of four (US, spiral CT, angio-graphy or magnetic resonance imaging (MRI)), with characters compatible with HCC,on an otherwise established cirrhosis due to ethanol, HCV, HBV or haemo-chromatosis. (2) AFP levels higher than 100 ng/ml.
Patients with con®rmed HCC are further staged according to their liver functionand health status and on the de®nition of the tumour extent. This last point isestablished by ultrasonography, spiral CT (or MRI) and angiography, if not contra-indicated by clotting disorders.
TREATMENT
Treatment of early HCC
There is no agreement on how early tumours should be de®ned. In our view, it shouldbe assumed that early HCC are those tumours that are expected to achieve successfulresults when treated by radical options (resection, OLT, percutaneous treatments).
Surgery: resection versus liver transplantation
Surgical resection and OLT are considered the ®rst-line options for early HCC,although there is no agreement on which is the best treatment approach.3,20 Resectionprovides excellent results in a small subgroup of cirrhotic patients with HCC.European and Japanese series have reported 5-year survival rates of 60±70% whenapplying extremely restrictive selection of candidates.21,22 We have shown that optimalcandidates are those with well preserved liver function, normal serum bilirubin values,absence of clinically relevant portal hypertension (detected either by clinical data or bydirect measurement of wedge hepatic venous pressure23), and small asymptomatictumours. These patients achieve 5-year survival rates of 70%, whereas patients with
portal hypertension and abnormal bilirubin, or those with both adverse predictors,will achieve 5-year survival rates of 50 and 25%, respectively (Figure 2).22
Despite proper selection of patients, resection has several limitations. First, tumourrecurrence complicates half of the patients at 3 years.2 Recurrence may represent anew HCC site (metachronous tumour) or metastatic spread of neoplastic cells fromthe primary tumours. Prevention of tumour recurrence is an important issue wheresolid data are still sparse. Both retinoids and intra-arterial I131-labelled lipiodol24,25 havebeen claimed to be e�ective in preventing recurrences after resection in two RCTs,but given the controversial statistical assessment of these studies these results requirefurther con®rmation. Even less information is available regarding the treatment of
recurrences, although theoretically it should mimic the treatment strategy of theprimary tumour. Second, the applicability of resection is particularly low in Westerncountries where liver cancer develops upon well-established cirrhosis. In this settingabout 5% of HCC patients diagnosed may ®t into the category of excellent candidates,this representing less than half of Child±Pugh's A cirrhotics. In the remaining patientssurgery will prompt the appearance of liver decompensation with reduction of theiroutcomes to ®gures even below the natural history of the disease.23,26 The applicability
996 J. M. Llovet and J. Bruix

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 7/18
of resection in Eastern countries could be higher, perhaps re¯ecting a less advancedliver disease related to HBV chronic infection or a higher recognition of HCV-positiveindividuals with silent cirrhosis among the community.
Nowadays, most hepatologists favour OLT as the ®rst-line option for early HCC.27,28
This procedure will, theoretically, remove the whole pre-neoplastic disease togetherwith the tumour itself, and can be applied to patients with impaired liver functionalreserve. The ®rst series of OLT reported disappointing results in terms of survival
and tumour recurrence because of the lack of restrictive selection criteria.29 However,more recent data have shown that the restriction of OLT to patients with singletumours45 cm or three nodules43 cm provides excellent long-term results (5-yearsurvival of 75%) with marginal recurrence rates (Table 2).28,30±33 These ®ndings havebeen reproduced throughout Europe and the United States, providing support for theuse of these criteria in the standardized selection of HCC OLT candidates.Nonetheless, despite the evidence that OLT has changed the strategy of HCC,
100
80
60
40
20
00 12 24 36 48 60 72 84 96
Months
P r o b a b i l i t y ( % )
Log rank 0.00001
Figure 2. Actuarial survival of HCC patients treated by resection, dividing them according to the prognosticfactors. Absence of relevant portal hypertension (n � 35, solid line). Presence of portal hypertension, butnormal bilirubin (n � 15, dotted line). Presence of portal hypertension and abnormal bilirubin (n � 27,dashed line). Reproduced from Llovet et al (1999, Hepatology 30: 1434±1440) with permission.
Table 2. Survival of HCC patients treated by OLT. Results applying restrictive selection criteria.
Authors (year) n Selection criteria
Survival (%)
1-year 5-year
Yokoyama et al, 199030 28 Single4 5 cm 77 68McPeacke et al, 199331 14 Single4 4 cm 85 57Mazzaferro et al, 199632 48 Single4 5 cm
3 nodules4 3 cm90 75*
Llovet et al, 199833 58 Single4 5 cm 84 74Bismuth et al, 199928 45 Single4 5 cm
3 nodules4 3 cm82 74
*Four-year survival.
Hepatocellular carcinoma 997

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 8/18
there remain certain caveats. First, it should be noted that the best results wereobtained in the era of short waiting time (46 months), when programmes were not asdonor-limited as they are now.33 The waiting time for OLT has progressivelylengthened during the last 5 years, currently ranging from 6 to 24 months.Considering that the 1-year probability of tumour progression is 70%26, it is likely thatmany untreated patients will face disease progression precluding OLT. Data regardingthe probability of drop-out in this setting are surprisingly scarce. Results from ourgroup show a 23% probability of drop-out rate with a median waiting time of 6months21, but other authors have reported even higher rates (30±50%) in waiting listsexceeding 1 year.34 All these striking ®gures reinforce the need for analysing outcomesof OLT according to intention-to-treat.
We have recently described an intention-to-treat analysis of OLT for early HCC
comparing a short waiting time period (no drop-outs) with a recent period of a longerwaiting time (23% drop-out rate). The 2-year survival ®gures decrease from 85% to lessthan 60% using an intention-to-treat analysis (Figure 3).21 This noteworthy loss of survival emphasizes the necessity of focusing new e�orts on reduction of the drop-outrate. There are two ways to decrease the impact of this emerging problem. First,improve the number of organ donors either through an increase in the donation rateor through the use of marginal livers, split liver transplantation or liver from livingdonors. Second, reduce the drop-out rate by treating tumours during the waitingperiod. Despite several e�orts to treat HCC patients waiting for a donor ± mainly
with chemoembolization ± there is no evidence of its bene®t in terms of reduction of drop-out rate, HCC recurrence or impact on survival.27,28,32 RCTs in this setting arelacking, and due to the complexity of the problem they appear unfeasible. Cost± bene®t analyses are of interest to overcome these limitations and to provide theeconomical basis for clinical decision-making and to allocate health care resources. In arecent cost-e�ectiveness analysis we have shown that active treatment during thewaiting list for OLT (resection of percutaneous ablation) increases the probability of
100
80
60
40
20
00 12 24
Months
Log rank 0.003Breslow 0.01
P r o b a b i l i t y
( % )
42
4
1989-95 (Drop-out=0; n=50)
1996-97 (Drop-out=23%; n=37)
44
19
Patients at risk
Figure 3. Intention-to-treat survival of HCC patients considered for OLT, according to the presence of drop-outs. 1989±1995, 50 patients, no drop outs (solid line), and 1996±1997, 37 patients, eight drop outs(23%) (dotted line). Reproduced from Llovet et al (1999, Hepatology 30: 1434±1440) with permission.
998 J. M. Llovet and J. Bruix

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 9/18
being transplanted and the overall survival compared to conservative managementwhile simultaneously having an acceptable cost-e�ectiveness ratio in long waitingtimes.35 In brief, in waiting times exceeding 1 year, active treatment provided net gainsin life expectancy higher than 3 months, with a cost e�ectiveness ratio of about$50 000/per QALY for resection and less than $30 000/per QALY for percutaneous
ablation. Thus, in patients with short waiting periods (56 months) OLT o�erencouraging results, and there may be almost no bene®t in applying treatments todiminish the risk of tumour progression. By contrast, in patients facing long-waitingperiods e�ective pre-transplant treatments are recommended.
Percutaneous treatments
Percutaneous ethanol injection (PEI) has become one of the most widely usedtreatments for HCC due to its reduced economic cost associated with a high
antitumoral e�cacy in small solitary tumours.36±40
After repeated injections onseparate days the tumour nodule is completely in®ltrated, and colicuative necrosis andvascular thrombosis are achieved, thus leaving an avascular necrotic area. This is bestassessed by dynamic CT at least 2 weeks after treatment, in which the absence of contrast enhancement is assumed to re ect complete tumour necrosis. On thecontrary, the existence of intratumoral contrast uptake would re¯ect tumourpersistence and therefore, treatment failure. Angiography or MRI could also be usedfor this purpose, but they are more invasive and expensive, whereas informationregarding contrast-enhanced US is still limited.
PEI is well tolerated, the most frequent side-e�ects being pain during ethanol
injection and fever due to tumour necrosis. The passage of ethanol into the vascularvessels may induce thrombosis that may resolve spontaneously. Less than 5% of thepatients develop a self-limited haemoperitoneum, and there are a few reports of patients with tumour seeding along the needle tract. The low number of reducedseverity of the complications explain the almost absent treatment-related mortality.
Several studies have shown that the response rate depends on tumour size.36±38
Ethanol injection is highly e�ective for tumours 43 cm in which an 80% completeresponse could be expected.36,37 On the contrary, HCC exceeding this size will be lesslikely to achieve a total tumour necrosis, the complete response rate being about 50%
in tumours between 3 and 5 cm, and sharply lower in larger nodules.36±39
The treat-ment failures are due to poor ethanol in®ltration related to inadequate placement of the needle and/or to the presence of intratumoral septa. To increase the rate of complete tumour necrosis some authors propose the injection of a larger volume of ethanol, or to combine arterial embolization with ethanol injection. Despite someencouraging reports describing complete response rates above 50%, the long-termbene®ts of these approaches have never been clearly assessed within an RCT. We haverecently reported a phase II study combining arterial embolization and PEI in patientswith single non-surgical tumours of 3 to 7 cm in size.40 Despite the complete responseachieved in up to 60% of patients, the complete maintained response rate decreased to
30% and its achievement was not associated with any survival improvement.Survival of ethanol-treated patients depends on the degree of liver function
impairment at the time of treatment and on the success of therapy. The strati®cationaccording to liver function is usually based on the Child±Pugh's stage, and it has beenshown that the survival of Child±Pugh's A patients, in whom the treatment has beensuccessful, may be 50%.37 In these patients a large proportion of deaths occur in theabsence of neoplastic disease and are due to the underlying liver cirrhosis or associated
Hepatocellular carcinoma 999
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 10/18
diseases. These data suggest a potential survival improvement in selected candidates,while in subjects with advanced liver disease (Child±Pugh's B or C) elimination of thetumour may not counteract the grim prognosis due to the underlying cirrhosis, thebene®t of treatment being unclear.
Tumour recurrence after complete response may exceed 50% at 3 years, a ®gure
similar to that reported after resection of small solitary tumours.36±39 In that regard, ithas been suggested that surgery would eliminate not only the tumour, but also thesurrounding liver tissue which may contain the unrecognized microscopic satellitesthat will give rise to recurrence during follow-up. Because there are no RCTscomparing both treatment options, this assumption would have to be proved, but thecomplex design of such studies make them almost unfeasible.
Thermal ablation by radiofrequency (RF) has emerged as the best alternative toethanol injection among local therapies for HCC.41,42 It requires an electrical generatorand disposable probes. These are advanced into the tumour under US guidance and
the increase in temperature up to 708C induces a necrotic area of at least 3 cm in justone treatment session lasting less than 1 hour. The antitumoral e�ect does not dependon tissue di�usion. This characteristic and the single session nature represent themajor advantages of RF when compared to ethanol injection. However, the probesused to treat the tumours are larger and less ¯exible than the needles used for PEI,and thus their use may be associated with a higher rate or even more severe side-e�ects. Furthermore, the location of the HCC may contraindicate the application of thermal ablation.
The available studies suggest that RF may achieve a therapeutic e�cacy similar toPEI, or even an e�cacy 10% higher in the number of completely ablated tumour
nodules, and that the tumour ablation is achieved in fewer treatment sessions.41 In thatsense, recent data reported complete response rates of 90, 49 and 11% for singletumours of 53 cm, from 3 to 5 cm, and from 5 to 9 cm in size, respectively.41,42
However, these studies assessed initial responses rather than complete maintainedresponses or survival bene®ts. Therefore, complete information regarding the bene®tsof RF are limited, and this aspect will have to be clari®ed within RCTs comparing bothtechniques.
Treatment of intermediate±advanced HCC
Despite the implementation of surveillance programmes for HCC in most Liver Unitsin Western countries, half of the patients are still diagnosed at an intermediate± advanced tumour stage.3,11,43 These patients will not bene®t from curative therapiesowing to the high failure rates, and thus have to be assessed for palliative locoregionalor systemic treatments.
The world-wide increasing incidence of HCC has not been followed by thepublication of substantial investigations from large RCTs assessing antitumoral agentsfor HCC. About 50 RCTs have been published for HCC in cirrhosis, but most of themeither include a small number of patients or lack a non-treated arm, that is mandatory
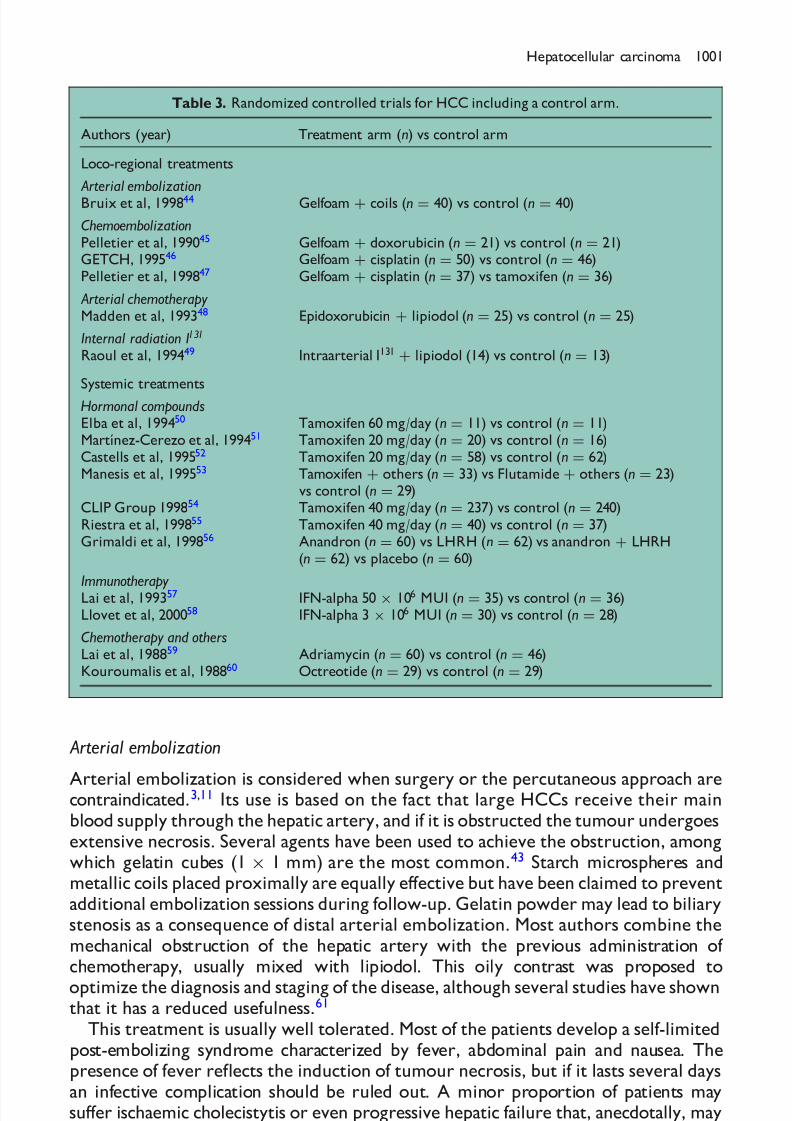
to demonstrate a bene®cial e�ect on survival. The scarcity of well designed trials formost of the therapies also preclude the assessment of survival bene®ts by means of pooled data in the setting of meta-analysis, in spite of the e�orts recently reported. Asmall number of RCTs published as full papers contain a control arm of conservativemanagement (Table 3).44±60 Ten of them are devoted to the controversial survivalbene®ts of arterial embolization44±47 and tamoxifen50±55, and provide enough data forthe evaluation of potential survival bene®ts.
1000 J. M. Llovet and J. Bruix
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 11/18
Arterial embolization
Arterial embolization is considered when surgery or the percutaneous approach arecontraindicated.3,11 Its use is based on the fact that large HCCs receive their mainblood supply through the hepatic artery, and if it is obstructed the tumour undergoesextensive necrosis. Several agents have been used to achieve the obstruction, amongwhich gelatin cubes (1 Â 1 mm) are the most common.43 Starch microspheres andmetallic coils placed proximally are equally e�ective but have been claimed to preventadditional embolization sessions during follow-up. Gelatin powder may lead to biliarystenosis as a consequence of distal arterial embolization. Most authors combine themechanical obstruction of the hepatic artery with the previous administration of chemotherapy, usually mixed with lipiodol. This oily contrast was proposed to
optimize the diagnosis and staging of the disease, although several studies have shownthat it has a reduced usefulness.61
This treatment is usually well tolerated. Most of the patients develop a self-limitedpost-embolizing syndrome characterized by fever, abdominal pain and nausea. Thepresence of fever re¯ects the induction of tumour necrosis, but if it lasts several daysan infective complication should be ruled out. A minor proportion of patients maysu�er ischaemic cholecistytis or even progressive hepatic failure that, anecdotally, may
Table 3. Randomized controlled trials for HCC including a control arm.
Authors (year) Treatment arm (n) vs control arm
Loco-regional treatments
Arterial embolizationBruix et al, 199844 Gelfoam � coils (n � 40) vs control (n � 40)
ChemoembolizationPelletier et al, 199045 Gelfoam � doxorubicin (n � 21) vs control (n � 21)GETCH, 199546 Gelfoam � cisplatin (n � 50) vs control (n � 46)Pelletier et al, 199847 Gelfoam � cisplatin (n � 37) vs tamoxifen (n � 36)
Arterial chemotherapyMadden et al, 199348 Epidoxorubicin � lipiodol (n � 25) vs control (n � 25)
Internal radiation I131
Raoul et al, 199449 Intraarterial I131� lipiodol (14) vs control (n � 13)
Systemic treatments
Hormonal compoundsElba et al, 199450 Tamoxifen 60 mg/day (n � 11) vs control (n � 11)Martõ Ânez-Cerezo et al, 199451 Tamoxifen 20 mg/day (n � 20) vs control (n � 16)Castells et al, 199552 Tamoxifen 20 mg/day (n � 58) vs control (n � 62)Manesis et al, 199553 Tamoxifen � others (n � 33) vs Flutamide � others (n � 23)
vs control (n � 29)CLIP Group 199854 Tamoxifen 40 mg/day (n � 237) vs control (n � 240)Riestra et al, 199855 Tamoxifen 40 mg/day (n � 40) vs control (n � 37)Grimaldi et al, 199856 Anandron (n � 60) vs LHRH (n � 62) vs anandron � LHRH
(n � 62) vs placebo (n � 60)
ImmunotherapyLai et al, 199357 IFN-alpha 50 Â 106 MUI (n � 35) vs control (n � 36)Llovet et al, 200058 IFN-alpha 3 Â 106 MUI (n � 30) vs control (n � 28)
Chemotherapy and othersLai et al, 198859 Adriamycin (n � 60) vs control (n � 46)Kouroumalis et al, 198860 Octreotide (n � 29) vs control (n � 29)
Hepatocellular carcinoma 1001
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 12/18
even lead to death. Major contraindications for these procedures are an impairment inthe portal ¯ow (portal thrombosis, hepatofugal ¯ow) and advanced liver failure
(Child±Pugh's C stage).43
Arterial embolization has a marked antitumoral e�ect. Several phase II studieshave shown that half of the patients present objective responses (450% reduction intumour mass), there being even some isolated reports of complete response aftertreatment.62 These results are achieved with both embolization alone and in combina-tion with chemotherapy (chemoembolization) ± regardless of the agent used ± therebeing no evidence that the latter provides any bene®t in terms of tumour progressionor survival.63
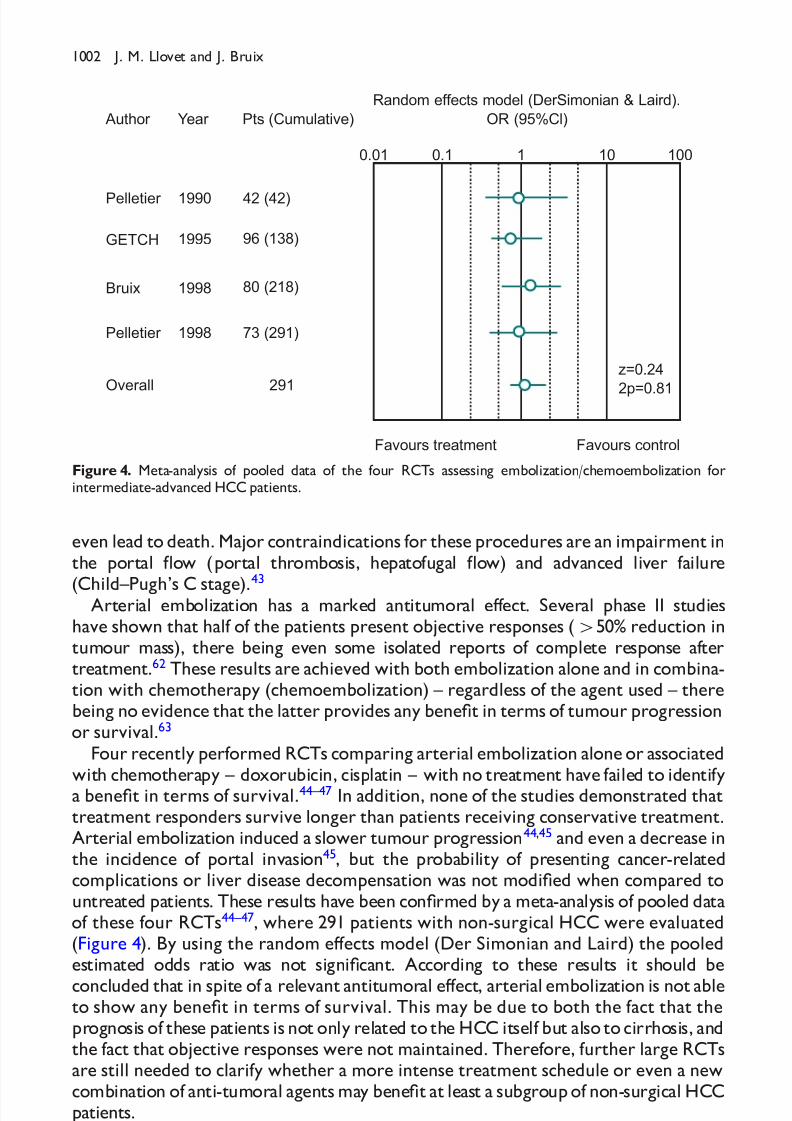
Four recently performed RCTs comparing arterial embolization alone or associatedwith chemotherapy ± doxorubicin, cisplatin ± with no treatment have failed to identifya bene®t in terms of survival.44±47 In addition, none of the studies demonstrated thattreatment responders survive longer than patients receiving conservative treatment.Arterial embolization induced a slower tumour progression44,45 and even a decrease inthe incidence of portal invasion45, but the probability of presenting cancer-relatedcomplications or liver disease decompensation was not modi®ed when compared tountreated patients. These results have been con®rmed by a meta-analysis of pooled dataof these four RCTs44±47, where 291 patients with non-surgical HCC were evaluated(Figure 4). By using the random e�ects model (Der Simonian and Laird) the pooledestimated odds ratio was not signi®cant. According to these results it should be
concluded that in spite of a relevant antitumoral e�ect, arterial embolization is not ableto show any bene®t in terms of survival. This may be due to both the fact that theprognosis of these patients is not only related to the HCC itself but also to cirrhosis, andthe fact that objective responses were not maintained. Therefore, further large RCTsare still needed to clarify whether a more intense treatment schedule or even a newcombination of anti-tumoral agents may bene®t at least a subgroup of non-surgical HCCpatients.
Author Year Pts (Cumulative)
Pelletier
GETCH
Bruix
Pelletier
Overall
1990
1995
1998
1998
42 (42)
96 (138)
80 (218)
73 (291)
291
0.01 0.1 1 10 100
Favours treatment Favours control
z=0.24
2p=0.81
Random effects model (DerSimonian & Laird).
OR (95%Cl)
Figure 4. Meta-analysis of pooled data of the four RCTs assessing embolization/chemoembolization forintermediate-advanced HCC patients.
1002 J. M. Llovet and J. Bruix

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 13/18
The only circumstance in which arterial embolization has been shown to be highlyuseful is for the treatment of spontaneous haemoperitoneum secondary to tumourrupture into the peritoneal cavity.64 The obstruction of the hepatic artery blood ¯owmay stop the bleeding, and after recovering from the episodes the patients may beconsidered even for radical treatment on an elective basis.
Hormone therapy
The presence of oestrogen receptors in tumoral hepatocytes gave the rationale toassess the usefulness of anti-oestrogen therapy in non-surgical HCC. The e�cacy of thistreatment approach has been controversial since the ®rst studies suggested a survivalbene®t for patients treated by tamoxifen.50,51 In 1995 we reported a large double-blindRCT in which results were clearly negative because anti-oestrogen therapy was not
related to any antitumoral or survival e�ect.52
In fact, our negative results were latercon®rmed by other RCTs.54,55 The lack of tamoxifen e�cacy may be due to theexpression of mutated oestrogen receptors or low expression of oestrogen receptor inadvanced HCC. Therefore, tamoxifen is not e�ective in prolonging survival of non-surgical HCC patients, and in our view no additional RCTs are needed in this arena.Other hormone therapies, such as anti-androgen treatments have been evaluated inthe setting of a large RCT with negative results.56
Other treatmentsChemotherapy. HCC is one of the most resistant tumours to antineoplastic agents.Several phase II trials have described an overall partial response rate of less than 20% forsystemic chemotherapy by intravenous route using either single agents (adriamycin,cisplatin, mitomicin-C, 5-¯uorouracil) or combined agents. Some authors suggest thatresponses may increase when applying the agent through the intra-arterial route as aresult of both antitumoral e�ect and ischaemia due to arterial endothelitis. However,nowadaysthere is no evidence of any impact in tumour progression or survival using thisroute, and thus it is not recommended in daily clinical practice.65
Immunotherapy. Interferon therapy has been assessed with positive results favouring thetreatment arm either compared to placebo or adriamycin in Eastern patients.57 In orderto con®rm these results in the West, we performed a RCT comparing IFN-a (3 MU/three times a week/1 year) versus control. Interferon was not properly tolerated incirrhotic patients with advanced HCC (discontinuation in 43% of patients) and itsadministration prompted no bene®t in terms of tumour progression and survival.58
External radiation. Conventional external radiotherapy has not been extensively usedin the treatment of HCC because of the risk of radiation hepatitis. The use of internal radiation therapy, mainly by lipiodol coupled with I131, is well tolerated, but isassociated with only a minimal response rate.49 There are no RCTs assessing theusefulness of this procedure, and its e�ects on survival have been compared only withthat of chemoembolization, showing no survival advantage.65 Therefore, the potentialbene®t of this treatment has not been proved.
Hepatocellular carcinoma 1003

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 14/18
Treatment strategy
We have recently proposed a treatment schedule to guide the decision-making in HCCpatients (Figure 5) that was linked to a new prognostic classi®cation.11 This treatmentapproach may apply for the majority of HCC patients, although individual decisionsshould be considered in speci®c cases, mainly in candidates for OLT because of end-stagecirrhosis. Patients in early stages (stage A) are evaluated for radical therapies. Resectionis recommended as the ®rst therapeutic option in stage A1 patients (single tumours,absence of relevant portal hypertension and normal bilirubin). An hepatic venouspressure gradient 510 mmHg is clearly the best predictor of an optimal survival.
Patients bearing an intermediate risk (stage A2 � single tumours, relevant portalhypertension, but normal bilirubin) are ®rst considered for OLT when notcontraindicated because of advanced age or associated diseases. In long waiting times,resection can be of bene®t in these patients while waiting for a donor. Those with bothadverse predictors ± relevant portal hypertension and increased bilirubin ± andpresenting solitary HCC 45 cm (stage A3) should not be resected because their lifeexpectancy will not be improved, and are thus evaluated for OLT, as well as thosepatients with three nodules smaller than 3 cm (stage A4). In these cases, percutaneoustreatments are recommended while waiting for a donor. If OLT is contraindicated, these
patients are considered for percutaneous treatments, either PEI or radiofrequency.Patients not ful®lling criteria for curative approaches should be selected for palliativetherapies within phase II studies or RCTs assessing medical treatments. Asymptomaticpatients with non-invasive tumours (stage B) may be entered into RCTs assessingloco-regional therapies such as arterial embolization ± associated or unassociatedchemotherapy ± whereas those presenting an adverse pro®le (stage C) are the bestcandidates to receive new antitumoral agents. Finally, patients diagnosed at a terminal
HCC
Radical therapies Randomized controlled trialsSymptomatic
treatment
Resection Orthotopic liver transplantation
PEI/RF TAE/TACE New agents
Okuda 1-2PST 0-2
Okuda 3PST 3-4
Early stage(Stage A)
Intermediate stage(Stage B)
Advanced stage(Stage C)
Terminal stage(Stage D)
Single 3 nodules <3 cm PST 0 andmultinodular
PST 1-2 or portalinvasion/M1
ortal pressure/bilirubin
Increased Associated diseases
Normal No Yes
Figure 5. Treatment schedule according to the BCLC staging classi®cation. Reproduced from Llovet et al(1999, Seminars in Liver Disease 19: 329±339) with permission.
1004 J. M. Llovet and J. Bruix
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 15/18
stage (stage D � performance status test 42 or Okuda stage III) should be excludedfrom therapeutic investigations and receive symptomatic treatment.
SUMMARY
Although there are no RCTs showing bene®t from surveillance programmes in termsof disease-speci®c reduction mortality, these strategies have been widely applied, andmost early tumours are diagnosed in the setting of such procedures. Surveillance forHCC should include only cirrhotic patients who would be treated if diagnosed withearly tumours. Diagnosis at an early stage is crucial to allow the application of curativetreatments that are the only hope for increasing the expectancy of the patient. Surgicalresection and liver transplantation are considered the ®rst-line options for early
tumours, although there is no agreement on which is the best treatment approach.Resection achieves excellent results in patients with single tumours, absence of portalhypertension and normal bilirubin, but is limited by the high recurrence rate. Livertransplantation also achieves excellent results in patients with single tumours smallerthan 5 cm or even three nodules smaller than 3 cm. However, this procedure ishampered by the shortage of donors and the increasing waiting times that havereduced their intention-to-treat outcomes. Treatment while waiting for a donor iscontroversial, but radical anti-tumoral therapies seem cost-e�ective in long waitingtimes. Percutaneous therapies are reserved for patients with single non-surgicaltumours. Clinical trials assessing treatments for patients with advanced tumours, such
as chemoembolization, hormonal therapies, interferon and chemotherapy have notshown any survival bene®ts.
Acknowledgement
Supported by a grant SAF 004-98 from the Comisio n Interdepartamental de Ciencia yTecnologõ Âa.
REFERENCES
1. El-Serag H & Mason A. Rising incidence of hepatocellular carcinoma in the United States. New England Journal of Medicine 1999; 340: 745±750.
2. Bosch X, Ribes J & BorraÁ s J. Epidemiology of primary liver cancer. Seminars in Liver Disease 1999; 19:271±285.
* 3. Bruix J. Treatment of hepatocellular carcinoma. Hepatology 1997; 25: 259±262.4. Llovet JM, Moitinho E, Sala M et al. Prevalence and prognostic value of hepatocellular carcinoma in
cirrhotic patients presenting with spontaneous bacterial peritonitis. Journal of Hepatology 2000; 33:423±429.
5. Oka H, Kurioka N, Kim K et al. Prospective study of early detection of hepatocellular carcinoma inpatients with cirrhosis. Hepatology 1990; 12: 680±687.
6. Colombo M, De Franchis R, Del Ninno E et al. Hepatocellular carcinoma in Italian patients withcirrhosis. New England Journal of Medicine 1991; 325: 675±680.
7. Pateron D, Ganne-Carrie N, Trinchet JC et al. Prospective study of screening of hepatocellularcarcinoma in Caucasian patients with cirrhosis. Journal of Hepatology 1994; 20: 65±71.
8. Cottone M, Turri M, Caltagirone M et al. Screening for hepatocellular carcinoma in patients with child'sa cirrhosis: an 8-year prospective study by ultrasound and alphafetoprotein. Journal of Hepatology 1994;21: 1029±1034.
Hepatocellular carcinoma 1005

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 16/18
9. Zoli M, Magalotti D, Bianchi G et al. E�cacy of a surveillance program for early detection of hepatocellular carcinoma. Cancer 1996; 78: 977±985.
10. Ba�s V, Shrier I, Sherker A et al. Use of interferon for prevention of hepatocellular carcinoma incirrhotic patients with hepatitis B or hepatitis C virus infection. Annals of Internal Medicine 1999; 131:696±701.
*11. Llovet JM, Bru  C & Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classi®cation.
Seminars in Liver Disease 1999; 19: 329±339.*12. Sherman M. Screening for hepatocellular carcinoma. Baillie Áre's Clinical Gastroenterology 1999; 13: 623±635.
13. Sarasin FP, Giostra E & Hadengue A. Cost-e�ectiveness of screening for detection of small hepatocellularcarcinoma in Western patients with Child±Pugh Class A cirrhosis. American Journal of Medicine 1996; 171:422±434.
14. Prorok PC. Epidemiologic approach for cancer screening. Problems in design and analysis of trials.American Journal of Pediatric Hematology and Oncology 1992; 14: 117±128.
15. Okuda K. Hepatocellular carcinoma: recent progress. Hepatology 1992; 15: 948±963.16. Sheu J, Sung J, Chen D et al. Growth rates of asymptomatic hepatocellular carcinoma and its clinical
implications. Gastroenterology 1985; 89: 259±266.17. Borzio M, Bruno S, Roncalli M et al. Liver cell dysplasia is a major risk factor for hepatocellular carcinoma
in cirrhosis. A prospective study. Gastroenterology 1995; 108: 812±817.18. Tengs TO, Adams ME, Pliskin JS et al. Five-hundred life-saving interventions and their cost-e�ectiveness.
Risk Analysis 1995; 15: 369±390.19. Garcia-Tsao G, Escorsell A, Zakko M et al. Predicting the presence of signi®cant portal hypertension and
varices in compensated cirrhotic patients. Hepatology 1997; 26: 360A.
20. Llovet JM, Bruix J & Gores GJ. Surgical resection versus transplantation for early hepatocellularcarcinoma: clues for the best strategy. Hepatology 2000; 31: 1019±1021.
*21. Llovet JM, Fuster J & Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellularcarcinoma: resection versus transplantation. Hepatology 1999; 30: 1434±1440.
22. The Liver Cancer Study Group of Japan. Predictive factors for long term prognosis after partialhepatectomy for patients with hepatocellular cancer in Japan. Cancer 1994; 74: 2772±2780.
23. Bruix J, Castells A, Bosch J et al. Surgical resection of hepatocellular carcinoma in cirrhotic patients.Prognostic value of preoperative portal pressure. Gastroenterology 1996; 111: 1018±1022.
24. Muto Y, Moriwaki H, Ninomiya M et al. Prevention of second primary tumors by an acyclic retinoid,polyprenoic acid, in patients with hepatocellular carcinoma. New England Journal of Medicine 1996; 334:1561±1567.
25. Lau WY, Leung TW, Ho SK et al. Adjuvant intra-arterial iodine-131-labelled lipiodol for resectablehepatocellular carcinoma: a prospective randomised trial. Lancet 1999; 353: 797±801.
*26. Llovet JM, Bustamante J, Castells A et al. Natural history of untreated nonsurgical hepatocellularcarcinoma: Rationale for the design and evaluation of therapeutic trials. Hepatology 1999; 29: 62±67.
27. Mor E, Tur Kaspa R, Sheiner P & Shwartz ME. Treatment of hepatocellular carcinoma associated withcirrhosis in the era of liver transplantation. Annals of Internal Medicine 1998; 129: 643±653.
*28. Bismuth H, Majno PE & Adam R. Liver transplantation for hepatocellular carcinoma. Seminars in Liver
Disease 1999; 19: 311±322.29. Ringe B, Pichlmayr R, Wittekind C & Tusch G. Surgical treatment of hepatocellular carcinoma:
experience with liver resection and transplantation in 198 patients. World Journal of Surgery 1991; 15:270±285.
30. Yokoyama I, Todo S, Iwatsuki S & Starzl TE. Liver transplantation in the treatment of primary livercancer. Hepato-Gastroenterology 1990; 37: 188±193.
31. McPeake JR, O'Grady JG, Zaman S et al. Liver transplantation for primary hepatocellular carcinoma:tumor size and number determine outcome. Journal of Hepatology 1993; 18: 226±234.
*32. Mazzaferro V, Regalia E, Doci R et al. Liver transplantation for treatment of small hepatocellularcarcinomas in patients with cirrhosis. New England Journal of Medicine 1996; 334: 693±699.
33. Llovet JM, Bruix J, Fuster J et al. Liver transplantation for treatment of small hepatocellular carcinoma:
The TNM classi®cation does not have prognostic power. Hepatology 1998; 27: 1572±1577.34. Schwartz M, Sung M, Emre S et al. Liver transplantation for hepatocellular carcinomas45 cm diameter:results of a multimodality protocol. In Abstracts of the 23rd Annual Meeting of the American Society of Transplant Surgeons, Chicago, May 1997.
35. Llovet JM, Mas X, Aponte J et al. Radical treatment of hepatocellular carcinoma during the waiting listfor orthotopic liver transplantation: a cost-e�ectiveness analysis on an intention-to-treat basis. Hepatology1999; 30: 223A.
36. Vilana R, Bruix J, Bru  C et al. Tumor sizes determines the e�cacy of percutaneous ethanol injection fortreatment of small hepatocellular carcinoma. Hepatology 1992; 16: 353±357.
1006 J. M. Llovet and J. Bruix
8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 17/18
37. Llovet JM, Bruix J, Capurro S et al. Long-term survival after ethanol injection for small hepatocellularcarcinoma in 100 cirrhotic patients. Relevance of maintained success. Journal of Hepatology 1999; 30: 100A.
38. Livraghi T, Giorgio A, Marin G et al. Hepatocellular carcinoma and cirrhosis in 746 patients: long-termresults of percutaneous ethanol injection. Radiology 1995; 197: 101±108.
39. Castellano L, Calandra M, Del Vecchio Blanco C & de Sio I. Predictive factors of survival and intrahepaticrecurrence of hepatocellular carcinoma in cirrhosis after percutaneous ethanol injection: analysis of 71
patients. Journal of Hepatology 1997; 27: 862±870.40. Llovet JM, Sala M, Suarez Y et al. Two-step treatment of large solitary hepatocellular carcinoma (HCC)
by arterial embolization followed by ethanol injection. Journal of Hepatology 2000; 32: 88A.*41. Livraghi T, Goldberg SN, Lazzaroni S et al. Small hepatocellular carcinoma: treatment with radio-
frequency ablation versus ethanol injection. Radiology 1999; 210: 655±661.42. Livraghi T, Goldberg SN, Lazzaroni S et al. Hepatocellular carcinoma: radio-frequency ablation of
medium and large lesions. Radiology 2000; 214: 761±768.43. Bruix J & Llovet JM. Locoregional treatments for hepatocellular carcinoma. Baillie Áre's Clinical
Gastroenterology 1999; 13: 611±622.44. Bruix J, Llovet JM, Castells A et al. Transarterial embolization versus symptomatic treatment in patients
with advanced hepatocellular carcinoma. Results of a randomized controlled trial in a single institution.Hepatology 1998; 27: 1578±1583.
45. Pelletier G, Roche A, Ink O et al. a randomized trial of hepatic arterial chemoembolization in patientswith unresectable hepatocellular carcinoma. Journal of Hepatology 1990; 11: 181±184.
*46. Group d'Etude et de Traitement de Carcinome Hepatocellulaire. A comparison of lipiodol chemo-embolization and conservative treatment for unresectable hepatocellular carcinoma. New England Journalof Medicine 1995; 332: 1256±1261.
47. Pelletier G, Ducreux M, Gay F et al. Treatment of unresectable hepatocellular carcinoma with lipiodolchemoembolization: a multicenter randomized trial. Journal of Hepatology 1998; 29: 129±134.
48. Madden M, Kringe J, Bailey S et al. Randomized trial of targeted chemotherapy with lipiodol and5-epidoxorubicin compared with symptomatic treatment for hepatoma. Gut 1993; 34: 1598±1600.
49. Raoul JL, Guyader D, Bretagne JF et al. Randomized controlled trial for hepatocellular carcinoma withportal vein thrombosis: intra-arterial iodine-131-iodized oil versus medical support. Journal of Nuclear
Medicine 1994; 35: 1782±1787.50. Elba S, Giannuzi V, Misciagna G & Manghisi OG. Randomized controlled trial of tamoxifen versus
placebo in inoperable hepatocellular carcinoma. Italian Journal of Gastroenterology 1994; 26: 66±68.51. Martinez Cerezo FJ, Tomas A, Donoso L et al. Controlled trial of tamoxifen in patients with advanced
hepatocellular carcinoma. Journal of Hepatology 1994; 20: 702±706.52. Castells A, Bruix J, Bru  C et al. Treatment of hepatocellular carcinoma with tamoxifen: a double-blind
placebo-controlled trial in 120 patients. Gastroenterology 1995; 109: 917±922.53. Manesis E, Giannoulis G, Zoumboulis P et al. Treatment of hepatocellular carcinoma with combined
suppression and inhibition of sex hormones: a randomized, controlled trial. Hepatology 1995; 21:1535±1542.
54. CLIP Group. Tamoxifen in treatment of hepatocellular carcinoma: a randomized controlled trial. Lancet1998; 352: 17±20.
55. Riestra S, Rodriguez M, Delgado M et al. Tamoxifen does not improve survival of patients with advancedhepatocellular carcinoma. Journal of Clinical Gastroenterology 1998; 26: 200±203.
56. Grimaldi C, Bleiberg H, Gay F et al. Evaluation of antiandrogen therapy in unresectable hepatocellularcarcinoma: results of a European Organization for Research and Treatment of Cancer. Multicentricdouble-blind trial. Journal of Clinical Oncology 1998; 16: 411±417.
57. Lai CL, Lau JYN, Wu PC et al. Recombinant interferon-alpha in inoperable hepatocellular carcinoma:A randomized controlled trial. Hepatology 1993; 17: 389±394.
58. Llovet JM, Sala M, Castells LI et al. Randomized controlled trial of interferon treatment for advancedhepatocellular carcinoma. Hepatology 2000; 31: 54±58.
59. Lai CL, Wu PC, Chan GCB et al. Doxorubicin versus no antitumor therapy in inoperable hepatocellularcarcinoma. A prospective randomized trial. Cancer 1988; 62: 479±483.
60. Kouroumalis E, Skordilis P, Thermos K et al. Treatment of hepatocellular carcinoma with octreotide:a randomised controlled study. Gut 1998; 42: 442±447.
61. Bizollon T, Rode A, Bancel B et al. Diagnostic value and tolerance of Lipiodol-computed tomography forthe detection of small hepatocellular carcinoma: correlation with pathologic examination of explantedlivers. Journal of Hepatology 1998; 28: 491±496.
62. Bruix J, Castells A, MontanyaÁ X et al. Phase II study of transarterial embolization in European patientswith hepatocellular carcinoma: need for controlled trials. Hepatology 1994; 20: 643±650.
63. Kalayci C, Johnson PJ, Raby N et al. Intraarterial adriamycin and lipiodol for inoperable hepatocellularcarcinoma: a comparison with intravenous adriamycin. Journal of Hepatology 1990; 11: 349±353.
Hepatocellular carcinoma 1007

8/6/2019 Early Dianosis and Treatment Carcinoma 2000
http://slidepdf.com/reader/full/early-dianosis-and-treatment-carcinoma-2000 18/18





























