Embed Size (px)
Citation preview

NASOPHARYNGEAL NASOPHARYNGEAL CARCINOMACARCINOMA
NASOPHARYNGEAL NASOPHARYNGEAL CARCINOMACARCINOMA
Cancer Growing Health ProblemCancer Growing Health Problem
World incidence: 8,068,404 people affected World incidence: 8,068,404 people affected in 1998in 1998 Female: 3,782,881Female: 3,782,881 Male: 4,286,523Male: 4,286,523
MalaysiaMalaysia Female: 10, 680Female: 10, 680 Male: 10,990Male: 10,990
Common sites affectedCommon sites affected
MALE MALE LungLung Colon/RectumColon/Rectum StomachStomach LiverLiver Nasopharynx (885)Nasopharynx (885)
FEMALEFEMALE BreastBreast Colon/RectumColon/Rectum Cervix/UterusCervix/Uterus LungLung OvaryOvary StomachStomach ThyroidThyroid Nasopharynx (370)Nasopharynx (370)
1998
Surgical Anatomy of NasopharynxSurgical Anatomy of Nasopharynx
4cm high, 4cm wide and 3cm in length4cm high, 4cm wide and 3cm in length Anterior Anterior -choanal orifice and posterior -choanal orifice and posterior
margin of nasal septummargin of nasal septum FloorFloor - upper surface of the soft palate - upper surface of the soft palate Roof and posterior wallRoof and posterior wall
Body of the sphenoid, BasiocciputBody of the sphenoid, Basiocciput First two cervical vertebraeFirst two cervical vertebrae
Lateral wallLateral wall Eustachian Tube orificeEustachian Tube orifice Fossa of ROSSENMULLERFossa of ROSSENMULLER
Anatomical relation of FORAnatomical relation of FOR
AnteriorlyAnteriorly Eustachian tube and levator palatiniEustachian tube and levator palatini
PosteriorlyPosteriorly Pharyngeal wall mucosa overlying Pharyngeal wall mucosa overlying
pharyngobasilar fascia & retropharyngeal spacepharyngobasilar fascia & retropharyngeal space MediallyMedially
Nasopharyngeal cavityNasopharyngeal cavity SuperiorlySuperiorly
Foramen lacerum & floor of carotid canalForamen lacerum & floor of carotid canal PosterolateralPosterolateral
Carotid canal & petrous apex, foramen ovale Carotid canal & petrous apex, foramen ovale and spinosumand spinosum
Epidemiology of NPCEpidemiology of NPC
Geography and RaceGeography and Race Distinctive epidemiological patternDistinctive epidemiological pattern IncidenceIncidence
Southern China (Kwantung province)Southern China (Kwantung province) Hong KongHong Kong TaiwanTaiwan South-East Asian races (Malay, Kadazan, Iban, South-East Asian races (Malay, Kadazan, Iban,
Bidayuh, Indonesians and Thais)Bidayuh, Indonesians and Thais) Eskimos, North Africa, TunisiaEskimos, North Africa, Tunisia
Aetiology of NPCAetiology of NPC
Environmental factorsEnvironmental factors Geographical clustering in Southern ChinaGeographical clustering in Southern China Time Trend: High risks among Chinese in Time Trend: High risks among Chinese in
Southern ChinaSouthern China Incidence in Hong Kong, Singapore Incidence in Hong Kong, Singapore
virtually remained unchanged 50 yrsvirtually remained unchanged 50 yrs 2nd and 3rd generation born in USA 2nd and 3rd generation born in USA
shows declineshows decline NPC constitute 16% of all malignant NPC constitute 16% of all malignant
tumors among the chinesetumors among the chinese
Smoking and Alcohol consumptionSmoking and Alcohol consumption OccupationalOccupational
Exposure to nickel, chromiumExposure to nickel, chromium Radioactive metalRadioactive metal Inhalation of chemical fumesInhalation of chemical fumes
IngestionsIngestions Salted fish - NitrosamineSalted fish - Nitrosamine Smoked foodSmoked food
DrugsDrugs Chinese herbal medicineChinese herbal medicine
Cooking habitsCooking habits Household smoke and fumesHousehold smoke and fumes
Religious practiceReligious practice Incense and joss stick smokeIncense and joss stick smoke
Socioeconomic statusSocioeconomic status Nutritional deficiencies eg. Vitamin A & CNutritional deficiencies eg. Vitamin A & C
Aetiological role of Epstein-Barr virus in NPCAetiological role of Epstein-Barr virus in NPC
More than 90% of patients having elevated More than 90% of patients having elevated antibody titres to Epstein-Barr virus are antibody titres to Epstein-Barr virus are those who have NPC of the those who have NPC of the undifferentiated / poorly differentiated undifferentiated / poorly differentiated formsforms
Moderate to well differentiated NPC are Moderate to well differentiated NPC are devoid of Epstein-Barr virus antigendevoid of Epstein-Barr virus antigen
Thus the role of virus in NPC is still Thus the role of virus in NPC is still controversialcontroversial
Immunogenetics of NPCImmunogenetics of NPC
Prominent genetic susceptibilityProminent genetic susceptibility High risk among southern Chinese populationHigh risk among southern Chinese population Differential high risk in emigrant Chinese Differential high risk in emigrant Chinese
compared to indigenous populationcompared to indigenous population Family clustering of NPC in ChineseFamily clustering of NPC in Chinese Elevated risk in people having genetic Elevated risk in people having genetic
admixture with Chineseadmixture with Chinese Low risk in other racial groups despite living in Low risk in other racial groups despite living in
high-risk countries eg. Indians in high-risk countries eg. Indians in Malaysia/SingaporeMalaysia/Singapore
Histocompatibility Locus Antigen (HLA)Histocompatibility Locus Antigen (HLA)
HLA patternHLA pattern
AW 19-B17AW 19-B17
A2-BW 46A2-BW 46
A2 without B17 or B46A2 without B17 or B46
Clinical behavior & Clinical behavior & survivalsurvival
Short term survivalShort term survival Age<30 yearsAge<30 years Died<2yrsDied<2yrs
Intermediate term survivalIntermediate term survival Age>30 yrs.Age>30 yrs.
Long term survivalLong term survival 5years survival:40%5years survival:40%
Clinical FeaturesClinical Features
Mostly seen in 5th to 7th decades Mostly seen in 5th to 7th decades but not uncommon to see in the but not uncommon to see in the twenties and thirtiestwenties and thirties
Males - 3 times more prone that Males - 3 times more prone that femalesfemales
Symptoms and SignsSymptoms and Signs
Bewildering array of symptoms and signsBewildering array of symptoms and signs
““ALWAYS a challenging problem, both from ALWAYS a challenging problem, both from diagnostic and therapeutic standpoint, diagnostic and therapeutic standpoint, malignant lesions of the nasopharynx are malignant lesions of the nasopharynx are perhaps most commonly misdiagnosed, perhaps most commonly misdiagnosed, most poorly understood, and most most poorly understood, and most pessimistically regarded of all tumors of pessimistically regarded of all tumors of the upper part of the respiratory tract”the upper part of the respiratory tract”
That statement is still true.That statement is still true.
Neck lump - 60%Neck lump - 60% Block sensation of ear - 41%Block sensation of ear - 41% Hearing loss - 37%Hearing loss - 37% Nasal bleeding - 30%Nasal bleeding - 30% Nasal obstruction - 29%Nasal obstruction - 29% Headache - 16%Headache - 16% Ear pain - 14%Ear pain - 14% Neck pain -13%Neck pain -13% Weight loss 10%Weight loss 10% Diplopia - 10%Diplopia - 10%
Cervical Lymphadenopathy (60%)Cervical Lymphadenopathy (60%)
NPC - commonest mode of presentation is NPC - commonest mode of presentation is neck swellingneck swelling Tendency for Early Lymphatic SpreadTendency for Early Lymphatic Spread Retropharyngeal group of L.N. (Rouviere) Retropharyngeal group of L.N. (Rouviere)
1st lymphatic filter not palpable1st lymphatic filter not palpable Commonest palpable node - Commonest palpable node -
jugulodiagastric, L2/L3/L5 leveljugulodiagastric, L2/L3/L5 level Contralateral lymph nodes metastasis Contralateral lymph nodes metastasis
(nasopharynx is midline structure)(nasopharynx is midline structure)
Aural SymptomsAural Symptoms
NPC leads to eustachian tube occlusion Sensation of a blocked earSensation of a blocked ear Impaired hearingImpaired hearing TinnitusTinnitus Serous Otitis MediaSerous Otitis Media
““Adult Chinese patients with unresolving Adult Chinese patients with unresolving unilateral serous otitis media have to be unilateral serous otitis media have to be presumed to have nasopharyngeal presumed to have nasopharyngeal carcinoma until proven otherwise”carcinoma until proven otherwise”
Epistaxis and Nasorespiratory SymptomsEpistaxis and Nasorespiratory Symptoms
Blood stained nasal dischargeBlood stained nasal discharge Blood stained saliva on hawkingBlood stained saliva on hawking Profuse epistaxisProfuse epistaxis Nasal obstructionNasal obstruction Ozanea due to tumor necrosisOzanea due to tumor necrosis
Neurological PalsiesNeurological Palsies
Most frequently involved are:Most frequently involved are: VI - Lateral rectus palsy - Diplopia & squintVI - Lateral rectus palsy - Diplopia & squint III, IV, VI - are commonly affected together III, IV, VI - are commonly affected together
(opthalmoplegia)(opthalmoplegia) V - High neck & pacial pain & paraesthesiaV - High neck & pacial pain & paraesthesia IX, X & XI - Jugular Foramen SyndromeIX, X & XI - Jugular Foramen Syndrome
Isolated single C.N. palsy common with Isolated single C.N. palsy common with nerves V & VInerves V & VI
Pain and HeadachePain and Headache
Hallmark of terminal diseaseHallmark of terminal disease Erosion of skull base (intracranial Erosion of skull base (intracranial
extension)extension) Sepsis - sphenoidal sinusitisSepsis - sphenoidal sinusitis
TrismusTrismus Inviltration of pterygoid musclesInviltration of pterygoid muscles
Diagnostic EvaluationDiagnostic Evaluation
Anterior Rhinoscopy ExaminationAnterior Rhinoscopy Examination Difficult to assess NP spaceDifficult to assess NP space Blood stain nasal discharged Blood stain nasal discharged Tumour extending into nasal cavityTumour extending into nasal cavity
Diagnostic EvaluationDiagnostic Evaluation
Post-Nasal ExaminationPost-Nasal Examination Post nasal mirror - can assess NP space and Post nasal mirror - can assess NP space and
tumourtumour Difficult to perform in sensitive patientsDifficult to perform in sensitive patients
Diagnostic EvaluationDiagnostic Evaluation
Head and Neck ExaminationHead and Neck Examination Lymph node Lymph node
L2, L3, L5 levelL2, L3, L5 level Progressively enlarging, hard, fixed, Progressively enlarging, hard, fixed,
painless swellingpainless swelling
Diagnostic EvaluationDiagnostic Evaluation
Aural ExaminationAural Examination OtoscopyOtoscopy Examination under microscopeExamination under microscope
Retracted tympanic membraneRetracted tympanic membrane Fluid in the middle earFluid in the middle ear
Diagnostic EvaluationDiagnostic Evaluation
Cranial Nerve ExaminationCranial Nerve Examination
Diagnostic EvaluationDiagnostic Evaluation
Diagnostic Nasal EndoscopyDiagnostic Nasal Endoscopy Rigid Nasal EndoscopeRigid Nasal Endoscope
Inspection of the nasopharynx spaceInspection of the nasopharynx space Localisation and extent of tumourLocalisation and extent of tumour Biopsy under visionBiopsy under vision
PathologyPathology
Grossly the tumour presents in 3 forms:Grossly the tumour presents in 3 forms: Proliferative growth causing nasal Proliferative growth causing nasal
obstructionobstruction Ulcerative causing epistaxisUlcerative causing epistaxis Infiltrative which causes cranial nerve Infiltrative which causes cranial nerve
involvementinvolvement
Diagnostic EvaluationDiagnostic Evaluation
Diagnostic Nasal EndoscopyDiagnostic Nasal Endoscopy Flexible Nasal EndoscopeFlexible Nasal Endoscope
Diagnostic EvaluationDiagnostic Evaluation
Fine Needle Aspiration Cytology of the Fine Needle Aspiration Cytology of the neck lymph nodeneck lymph node
Diagnostic EvaluationDiagnostic Evaluation
CT ScanCT Scan Extent of tumorExtent of tumor Neck node involvementNeck node involvement
Bone ScanBone Scan Skeletal metastasis- thoracolumbar regionSkeletal metastasis- thoracolumbar region
MRIMRI
Distant MetastasisDistant Metastasis
Incidence rate is about 30%Incidence rate is about 30% Sites commonly involved:Sites commonly involved:
Skeletal - Thoracolumbar spine > 50%Skeletal - Thoracolumbar spine > 50% Lung metastasisLung metastasis Liver metastasisLiver metastasis
90% of patients die within the 1st year of 90% of patients die within the 1st year of diagnosis of the first metastasisdiagnosis of the first metastasis
Staging of NPC- TNM ClassificationStaging of NPC- TNM Classification
Primary TumourPrimary Tumour T1 - tumour confined to one site of T1 - tumour confined to one site of
nasopharynx or positive biopsy onlynasopharynx or positive biopsy only T2 - tumour involving two sitesT2 - tumour involving two sites T3 - tmour extending into nasal cavity or T3 - tmour extending into nasal cavity or
oropharynxoropharynx T4 - tumour invasion of skull or cranial T4 - tumour invasion of skull or cranial
nerve involvement or bothnerve involvement or both
Staging of NPC- TNM ClassificationStaging of NPC- TNM Classification
N - Cervical Lymph NodesN - Cervical Lymph Nodes N0 - no clinically positive nodeN0 - no clinically positive node N1 - single clinically positive homolateral N1 - single clinically positive homolateral
node 3cm or less in diameternode 3cm or less in diameter N2 - single clinically positive homalateral N2 - single clinically positive homalateral
node > 3cm but < 6cm or multiple clinically node > 3cm but < 6cm or multiple clinically positive homolateral nodes > 6cm in positive homolateral nodes > 6cm in diameterdiameter
N3 - massive homolateral node(s), bilateral N3 - massive homolateral node(s), bilateral nodes or contralateral node(s)nodes or contralateral node(s)
Staging of NPC- TNM ClassificationStaging of NPC- TNM Classification
M - Distant MetastasisM - Distant Metastasis MX - not assessedMX - not assessed M0 - no (known) distant metastasisM0 - no (known) distant metastasis M1 - distant metastasis presentM1 - distant metastasis present
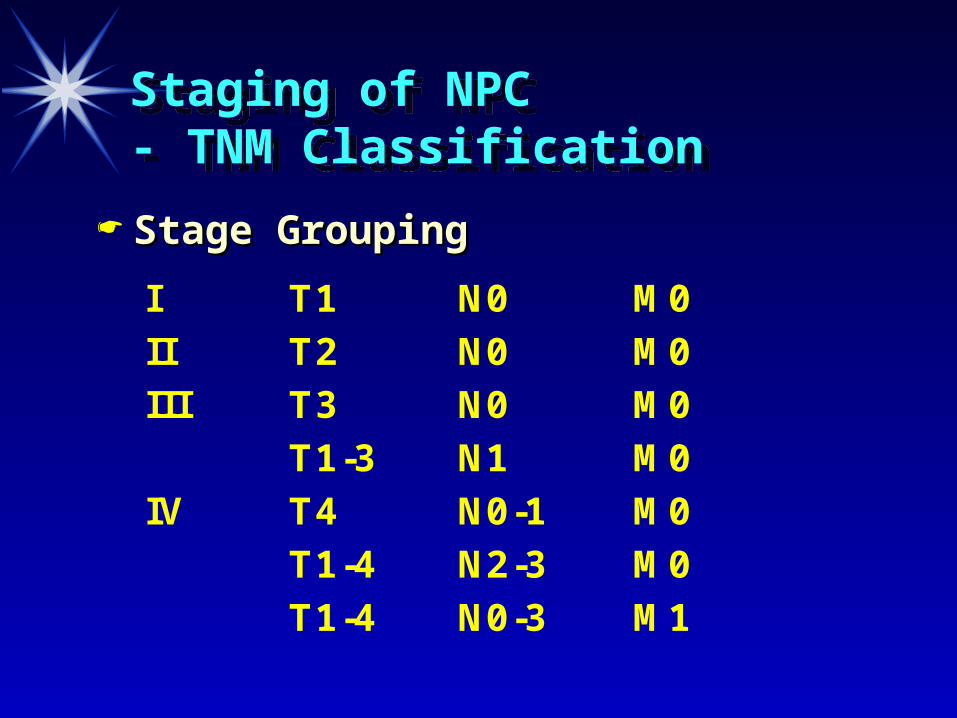
Staging of NPC- TNM ClassificationStaging of NPC- TNM Classification
I T1 N0 M0II T2 N0 M0III T3 N0 M0
T1-3 N1 M0IV T4 N0-1 M0
T1-4 N2-3 M0T1-4 N0-3 M1
Stage GroupingStage Grouping
Treatment PolicyTreatment Policy
Chemo-RadiotherapyChemo-Radiotherapy Primary modality of treatmentPrimary modality of treatment
Radiotherapy- 6000 radsRadiotherapy- 6000 rads.. ChemotherapyChemotherapy
Cisplatin and 5-flurouracilCisplatin and 5-flurouracil SurgerySurgery - limited role - limited role
Biopsy of the nasopharyngeal mucosaBiopsy of the nasopharyngeal mucosa Radical neck dissection for radioresistant Radical neck dissection for radioresistant
lymph nodeslymph nodes
Recurrent NPCRecurrent NPC
BrachytherapyBrachytherapy 22ndnd course of radiation course of radiation
Chemotherapy Chemotherapy For distant metastasisFor distant metastasis Failed radiationFailed radiation
ConclusionConclusion
Early diagnosis of NPC (stage I)Early diagnosis of NPC (stage I) Early treatmentEarly treatment Good prognosis (>5years)Good prognosis (>5years) Patients should be followed up regularlyPatients should be followed up regularly
1st year: once a month1st year: once a month 22ndnd year: every 2 year: every 2ndnd month month 33rdrd year: every 3 months year: every 3 months 44thth year: every 6 months year: every 6 months >5years: Once a year>5years: Once a year

THANK YOU
THANK YOU