Embed Size (px)
DESCRIPTION
Dr. Neena Raina Regional Advisor, Child and Adolescent Health WHO/SEARO. Early Childhood Development in South East Asia. Are you aware that. At birth there are 1 billion brain cells Brain of a six month old is half and that at 8 years is 90% that of an adult in weight - PowerPoint PPT Presentation
Citation preview

Early ChildhoodDevelopment
in South East Asia
Dr. Neena RainaRegional Advisor,
Child and Adolescent HealthWHO/SEARO

Are you aware that
• At birth there are 1 billion brain cells• Brain of a six month old is half and that at 8 years is
90% that of an adult in weight • Most of the synaptic connections (wiring) takes
place during the early years of life. Rewiring cannot take place later in life
• Maturity of brain is characterized by pruning . Excess of neurons and synapses are eliminated. This pruning is guided by the environment during the early years of life

Rethinking of the brain
Old thinking New thinking • Brain development depends
on the genes • Experiences before 3 years
age have a limited impact on later development and personality
• Secure relationship with a caregiver helps early development and learning
• Brain development is linear • Early brain development is
slow as compared to an adult
• Brain development depends on the interaction between genes and the experiences
• Early experiences influence architecture of the brain and extent of adult capacity
• Secure relationship with a care giver affects early development and wiring of brain
• Brain development is maximal in early years (including pregnancy)
• Brain is twice as active at three as compared to college student

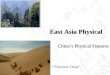
03-012 Synaptic Density
Rethinking the Brain, Families and Work Institute, Rima Shore, 1997.
At Birth 6 Years Old 14 Years Old



Reversing the developmental effects associated with stunting
(low height for age)
• 31% of children under 5 years of age in developing countries are stunted (SOWC 2007), 46% in India (Status of the World’s Children 2006)
• Stunting is associated with – Poor developmental attainment in young children (Walker, et al., 2007)– Up to 46% less income
earned as adults due to poorer schoolachievement and lower intelligence levels (Bundy, 1996; Hoddintott, et al., 2008)

Bogotá Project: Effects of supplementation and stimulation
on growth and weight (results at age 7)
0%
1%
2%
3%
4%
5%
6%
7%
height weight
% i
ncr
ea
se o
f m
ea
nco
mp
are
d t
o c
on
tro
lgro
up
Supplementation
Maternal tutoring
Both
Van der Gaag, J. School Performance and Physical Growth of Underprivileged Children: Results of the Bogotá Project at Seven Years. (1983). World Bank, Washington D.C.

Bogotá study (continued)
• At age 7, children who had received supplementation and stimulation in early childhood
– Physical growth: Less than 20% were stunted, compared to 50% in the control group
– Development:• Better reading readiness scores• Better mathematics scores and basic knowledge
(preschool achievement test scores)• Results especially strong for chidren of fathers of
low to moderate levels of education and literacy (a proxy for SES)

The Jamaica StudyGrantham-McGregor, et al. , 1991
• Looked at the effects of nutritional supplementation and psychosocial stimulation on stunted children aged 9-24 months
• An experimental intervention study • 129 children from poor neighboorhoods were randomly assigned to four
groups:
– Control– Supplemented only – Stimulated only– Supplemented plus stimulated
• And a matched comparison group of non-stunted children

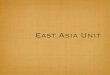
Jamaica Project:Effects of supplementation and stimulation on the mean development quotient of
stunted groups compared with non-stunted groups
85
90
95
100
105
110
Baseline 6 12 18 24
Months of the intervention
Dev
elop
men
t Q
uoti
ent
Non- stunted
Supplemented andstimulated
Stimulated
Supplemented
Control
Development quotient includes practical reasoning, eye and hand coordination, hearing and speech, and performance. S.M. Grantham-McGregor, et al. (1991).

Jamaica Study:The effects of the stimulation intervention at age 17-18 years
UNICEF
standard scores
.1
.02
.1
.02
.05
.02
0.1.001.01
Walker, et al. (2005)
p (significance)

Findings from the Lancet series on child development (2007)
• An estimated over 200 million children under age 5 are not developing their full potential
• The cost in economic potential is 20-29% of each adult worker’s income per year
• The best documented risks are stunting, iron deficiency, iodine deficiency, and lack of stimulation
• Poor growth and poor development are closely related

Key messages Lancet 2011Biological and psychosocial risks affects the developing brain. Risks are
poverty, malnutrition and lack of stimulation. Breast feeding, cognitive stimulation and maternal education are important to tackle the risks.
Inequalities in child development begin prenatally and in the first years of life, and increase over time. Reducing inequalities requires early integrated interventions that reduce risks and promote child development. The most effective and cost-efficient time to prevent inequalities is early in life.
Parenting interventions and center-based programmes (preschools) can improve children’s development. Quality in Early Child Development programmes can be maximized through design, curriculum, parent involvement, and training and supervision for workers
Increasing preschool enrolment in each low- and middle-income country would result in a benefit of between US $10 - $34 billion

Sensitivity (Care giver)
• The caregiver is aware of the infant’s signals and interprets them accurately
• The caregiver accepts the child’s interests, gives physical affection, is positive
• To be sensitive, the caregiver must be able to – Regard the child as a separate person– See things from the child’s point of view

Responsiveness of the care giver
• The response of the mother depends on, or is triggered by, the child’s signal This should be recognized early and matched by a response by the care giver
• To be responsive, the caregiver must be sensitive

Responsiveness to child language affects language development
0
20
40
60
80
100
120
13 15 17 19 21
Months
% k
now
ing a
t le
ast
50
word
s
Children ofhighlyresponsivemothers
Children oflowresponsivemothers
Tamis-LeMonda, et al. 2001

Sensitivity and responsiveness (care giver) :
• To be effective in caring for a young child—sick or well, e.g.: – Breastfeed on demand, feed responsively– Protect a child from imminent harm– Recognize and seek care when the child is
sick– See cause and effect in the environment
and in social relationships– Learn to speak, solve problems

Attachment
• Primarily a process of the infant forming a relationship with his or her mother (infant to mother): attachment is reinforced by the responses of the mother (or other primary caregiver)
• Occurs in first two years of life, but especially between 2 and 7 months of age
• Child develops a personal communication system with the primary caregiver……by receiving an appropriate response from the caregiver

Consequences of poor attachment
• A break leads to:– Confusion (‘lost in a strange country without
an interpreter’)– Lack of trust– Increasing rage or depression – Shutting down—’non-organic failure to thrive’
• When there is no primary caretaker, child attaches to things, environment, routines, etc. and has difficulty adapting to any change

Bonding
• The process of a mother forming a relationship with her new infant (mother to infant)
• Begins during the first few hours after birth

High risk conditions for bonding • Mother
– Separated from infant for a period after birth – Poor health, for example, as many as 40% of
mothers are depressed after delivery, • Characteristics of child
– About a quarter of low birth weight babies were abused and failure to bond was the reason)
– -children with illness or undernourished children frequently are abused due to lack of bonding

ECD and long term effects
• In an unstimulating, emotionally and physically unsupportive environment their brain development is affected in adverse ways. Many problems in adult life have their origins in pathways that begin in childhood.
• In the short term, ECD influences ‘readiness for school’. Over the first and the second decade of life it influences school success, social success or rejection, stunting, early criminality and the prospects for a successful transition to citizenship.

ECD and long term effects
• By the third and fourth decade of life it influences mental health (depression and anxiety disorders), physical health (obesity, blood pressure, heart disease, non-insulin dependent diabetes), and socioeconomic mobility.
• From the fifth decade onward, it influences a wide range of chronic diseases as well as the prospect of healthy aging

Why invest in early childhood development ?
• At the most basic level it improves child survival• ECD helps development, goes beyond survival, builds
social capital with return of seven times• Helps to break the intergeneration cycle of poverty
and malnutrition• Contributes to reduction of gender inequities • ECD builds social capital • Helps build community networks to improve self care • First line of defense in dealing with developmental
delays and disability

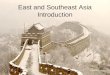
Optimal Investment Levels
Preschool School Post School
Age0
Mismatch between Investment and Opportunity
Cumulative Public Investment
Source: Carneiro & Heckman, Human Social Policy (2003)
Evidence

Age 1 week up to 6 months: Talk to your child and get a conversation going with sounds or gestures

Age 12 months up to 2 years:
Give your child things to stack up, and to put into containers and take out.


Adults are children’s first teachers



What can be achieved through CCD
• Reduction in deaths • Children will be healthier• Improved nutritional status • School readiness, improved performance in
school • Greater adult productivity and income • The gains are maximal if CCD can be focused
on underprivileged groups in the society

Why ECD should be in the Health Sector?
• Health: Overall well being
• Established MCH services: to support the critical period from prenatal period to first three years of life
• Synergy of good care and mother-child interaction for survival, growth, and development
• Tradition of health care providers as advisors for families
Regional Strategy: WHO-SEARO

9 Jan 2010 35
Entry points in Health Care System
• Sick child visit (e.g. IMNCI)• Well-baby clinics• Prenatal and newborn services (e.g. breastfeeding support)• Nutrition clinics or feeding programmes• Child care centers• Mothers, groups• Home visits: Community health workers• Special services for children at risk
Care and nutrition intervention, both areneeded and can be delivered together

More Opportunities in Health Sector
• Home Visits for Newborn Care:– Community Health Workers to visit homes for
supporting post-natal care
• Community Case Management:– Treatment of diarrhea and pneumonia– Counselling on feeding and immunization
Opportunity to integrate ECD activities

STRATEGIC DIRECTIONS
Goal:• To ensure that all children are able develop
their full potential, recognizing that development is integrally related to child health and nutrition.
• Improving one without improving the other will not achieve the goal for ECD: A benefit for society

STRATEGIC DIRECTIONS • All families receive information and guidance
• Special care given to disadvantaged and special
needs children
• ECD incorporated at each level of the health system
– Child health policies
– Community health programmes
– Health care facility

IMPLEMENTING ECD AT SCALE
• Advocacy for ECD with Policy makers
• Define the Vision and Goals for ECD in country
• Set up Coordinating Mechanism
• Develop Costed Plans
• Pilot programme models - Scale up
• Monitoring and evaluation plan