Embed Size (px)
Citation preview

GastroenterologiaJaponica Vol. 16, No. 5 Copyright �9 1981 by The Japanese Society of Gastroenterology Printed in Japan
- - O r i g i n a l A r t i c l e - -
EARLY C A R C I N O M A OF T H E G A L L B L A D D E R
Toshio SATO, M.D., F.A.C.S., F .A.C.G. , Kenji KOYAMA, M.D.,
Hidemi YAMAUCHI, M.D. and Seiki MATSUNO, M.D.
The First Department of Surgery, Tohoku University School of Medicine, Sendai, Japan
Summary
Twenty five curatively operated patients with carcinoma of the gallbladder were studied to determine the early stage of this cancer according to the depth of invasion. Patients with cancer invasion limited to the proper muscle layer, should be designated as cases with early cancer of the gallbladder and in these cases, metastasis or further invasion was rare and a good postoperative survival rate was obtained. However, if the early cancer was of the nodular or infiltrative type macroscopically, and of tubular adenocarcinoma or adeno- squamous carcinoma histologically, the chances of long-term postoperative survival were poor. Based upon our results, it is suggested that extended cholecystectomy should be performed even in patients with early gall- bladder cancer.
Key Words: early gallbladder cancer, simple cholecystectomy, extended cholecystectomy, right hepatic lo bectomy.
Compared to patients with gastric or colorec-
tal cancer, the prognosis of surgically treated
patients with gallbladder cancer is very poor
and only a few reported long-term postopera-
tive suvivall). Therefore, the early diagnosis
and t reatment are essential to obtain better re-
sults in patients with carc inoma of the gallblad-
der. In gastric cancer, established staging of
the disease facilitates its diagnosis and treat- ment2). In the early stage, invasion is limited to
the mucosal or submucosal layer and radical
surgery has resulted in excellent prognosisS).
Therefore, an at tempt was made in the present
study to determine the possibility of staging of
carc inoma of the gal lbladder according to the
depth of invasion. It is reported herein for the
characteristics of early carc inoma of the gall-
Received March 17, 1981. Accepted June 8, 1981. Address requests for reprints to: Toshio Sato, M.D., 1st
Department of Surgery, Tohoku University School of Medi- cine, Seiryo-machi 1-1, Sendai, 980 Japan.
bladder classified f rom the delSth of invasion
and the results of patients curatively operated
in our department .
Patients and Methods
During the past 20 years, 100 patients with
carcinoma of the gal lbladder were treated in
our department; 25 underwent curative and 31
non-curative resection, 44 patients were un-
resectable. Of the 25 curatively operated pa-
tients, 9 were treated by extended cholecystec-
tomy, 15 by simple cholecystectomy and one by extended right hepatic lobectomy.
These cases classified into 3 groups, m, pm,
and s, according to whether the mucosal layer
only, the proper muscle layer, or the subserosa
or serosa beyond the proper muscle layer, was
invaded by the cancer. There were 4 patients in
group m, 5 in group pm and 16 in group s. The gallbladder wall was histologically examined in
all of these cases to determine the presence or

460 T. SATO ET AL. Vol. 16, No. 5
absence of cancer invasion to the veins, lym-
phat ics and pe r ineura l space, and to ascer ta in
t h e g r o w t h type and sp read of the cancer .
Cases with cancer involvement of mul t ip le
veins in the ga l lb l adde r wall were defined as v~;
those in which a few veins were involved, vl;
and those with no venous involvement, v0.
Similarly, cancer invasion of the lymphat ics
and per ineura l space was des ignated ly2, 1 D, ly0
and ne~, nea, ne0, respectively. The pa t t e rn of
growth and spread of cancer was classified into
three types, which were t e rmed INF , , INFe a n d
I N F , . INF , , refers to the growth and spread of
expansive with relat ively clear boundary , a n d
in INFs of infi l trat ive wi thout c lear bounda ry
and INFe of in te rmedia te .
Surgically removed lymph nodes and l iver
specimens were examined to study for metas ta-
sis and invasion and the operat ive results were
c o m p a r e d among the groups classified accord-
ing to dep th of cancer invasion and the type of
cancer growth and spread .
R e s u l t s
Morphological Classification of the Gallblad- der Cancer
Types of the cancer classified macroscopica l -
ly and microscopical ly in these pat ients are
shown in T a b l e 1. Pat ients of m and p m groups
const i tu ted macroscopica l ly pap i l l a ry type and
pap i l l a ry adenoca rc inoma in histology.
Invasion and Type of Cancer Spread As shown in T a b l e 2, none of the pa t ien ts in
group m mani fes ted inf i l t ra t ion to the veins,
the lymphat ics or the pe r ineura l space of the
ga l lb l adde r wall. T h e type of spread in these
pat ients was I N F , . In the p m group, only one
of 5 pat ients showed invasion (ly 0 and except
for this pat ients , the type of spread was INFa.
On the other hand , of 16 pat ients in the s g roup
showed venous, lympha t i c a n d / o r pe r ineura l
invasion and the type of cancer sp read was
INF~ in 10 pat ients .
Metastasis and Infiltration of the Gallbladder Cancer
L y m p h nodes metastasis was not no ted in
g roup m and g roup p m pat ients . In g roup s, 6
pat ients (38%) mani fes ted lymph node
metastasis. Of these, 5 had metastasis to the
pa racho ledocha l nodes, 2 to the hepa t ic ar-
ter ial and to the super ior r e t ropancrea t i c
nodes. Inf i l t ra t ion to the liver was not observed
Table 1. Morphological classification of gallbladder cancer
Depth of No. of Macroscopic Classification Microscopic Classification
Invasion patients papillary nodular infiltrative papillary tubular adenosquam. adenoca, adenoca, ca.
in 4 4 0 0 4 0 0 pm 5 4 0 1 4 1 0 s 16 5 4 7 6 8 2
Table 2. Infiltration and spread of cancer in gallbladder wall
Venous Lymphatic Perineural Pattern of Depth of No. of infiltration infiltration infiltration growth and spread invasion patients (v) (ly) (ne) (INF)
Vo vx v~ lyo lyl lyz neo nel ne2 a fl y
m 4 4 0 0 4 0 0 4 0 0 4 0 0 pm 5 5 0 0 4 1 0 5 0 0 0 4 1 s 16 9 7 0 3 8 5 10 6 0 0 6 10

October 1981 Early Carcinoma of the Gallbladder 461
in groups m and pm. In s group, however, 7 patients showed infiltration to the liver. Liver
metastasis was not noted in all groups.
Fesults of Operation Table $ shows the correlation between the
depth of invasion and the operative results.
There were no operative mortalities (within 1
month after surgery) or late deaths among
group m patients; one patient in group pm
died 2 years 3 months after simple cholecystec-
tomy due to the recurrence. In group s, there
were 4 operative mortalities and 11 late deaths;
the longest postoperative survival period was 2
years 10 months.
Cancer Type and Prognosis The correlation between the type of cancer
classified macroscopically and histologically
Tab le 3. Operative results of the patients with gallbladder cancer
Dep tho f No. of Operative Survival period invasion patients death 1 yr. 3yrs. 5yrs.
m 4 0 4 /4 4/4 3/3 pm 5 0 3/3 1/2 1/2 s 16 4 6/12 0/10 0/7
Figures of denominators and numerators indicate the numbers of patients with available postoperative periods and of survival patients, respectively.
and prognosis is shown in Table 4. The prog-
nosis of patients with papillary in macroscopy
and papillary adenocarcinoma in histology was
good, while that of patients with nodular or in-
filtrative in macroscopy and with tubular
adenocarcinoma or undifferentiated carcino- ma, determined histologically, was poor.
Definition of early Carcinoma of the Gallblad- der
Present study revealed that among 25 cura-
tively resected patients, no patients in group m
and pm manifested lymph node metastasis. On
the other hand, in group s, 6 patients had
metastasis to the regional lymph nodes and 7
manifested hepatic cancer invasion. Further-
more, in this group there were 7 patients with
venous and/or lymphatic invasion in the ab-
sence of metastasis to the liver and/or lymph
nodes. Death due to postoperative cancer re-
currence occurred in aa of group s patients and
only one survived for more than 2 years after
surgery. Based upon these results, it might be
accepted that cancers of groups m and pm are
defined as early cancer of the gallbladder.
Clinicopathological Picture of Early Gallblad- der Cancer
Table 5 presents the symptoms, diagnostic parameters, and operative results in the 9 cura-
Table 4. Survival rate vs morphological classification of the gallbladder cancer
No. of Operative Survival period patients death I yr. 3 yrs. 5 yrs.
Macroscopic classification: papillary 13 1 8/10 5/9 4/6 nodular 4 0 2/4 0/4 0/3 Infiltrative 8 3 3/5 0/3 0/3
Microscopic classification:
Papillary 14 5 7/9 5/8 4/6 adenocarcinoma Tubular
9 0 6/9 0/7 0/5 adenocarcinoma
Adenosquamous 2 1 0/1 0/1 0/1 cell carcinoma
Figures of denominators and numerators indicate the numbers of patients with available postoperative periods and of survival patients, respectively.

462 T. S A T O E T A L . Vol. 16, No. 5
Table 5. Clinicopathological data of the patients with gallbladder cancer in groups m and pm
Patients Age Size Macro. Micro. Duration of Survival No. & (cm) class, class, illness DIC Surgery period
Sex
1 27, m 0.9x0.6 pap. pap.ad. 4mos FD CHOL. 6yrs. alive
2 37, f 0.7• pap. pap.ad. 4mos FD CHOL. 3yrs.5mos. alive
5yrs. 5mos. 3 50, f 0.6x0.4 pap. pap.ad. 8mos Stone CHOL. alive
4 64, f 2xl.3 pap. pap.ad. 2mos NV CHOL. 9yrs.5mos. alive
5 43, f 3x2.5 pap. pap.ad. 5mos FD EX.CHOL. 6yrs.7mos. alive
6 66, f 3x2.5 pap. pap.ad. 2mos NV EX.CHOL. 13yrs.lmo alive
7 67, f 3x2 Inf. tub.ad. 10yrs FD CHOL. 2yrs.3mos. died
4mos. 8 67, f 2xl pap. pap.ad. 5mos NV CHOL. alive
7mos. 9 77, m 2x2 pap. pap.ad. 2mos NV EX.CHOL. alive
Abbreviations: pap.; papillary type, nod.; nodular type, Inf.; infiltrative type, pap.ad. ; papillary adenocarcinoma, tub.ad. ; tubular adenocarcinoma, FD; filling defect, NV; not visualized, CHOL.; cholecystectomy, EX.CHOL. ; extended cholecystectomy.
Remarks: No. 1-4; group m, No. 5 9; group pro. All cases had no infiltration and metastasis to liver and lymphnodes. Patients of No. 3, 4 and 7 had cholecystolithiasis.
tively resected pat ients of groups m and pm; all
bu t one pa t ien t are alive and in good hea l th at
present .
T h e most c o m m o n symptom was pa in in the
epigastr ic or r ight hypochondr ic region; it was
un re l a t ed to the presence or absence of gal l-
b l a d d e r stones.
Dr ip infusion cho lang iography (DIC) visu-
alized the ga l lb l adde r in 5 pat ients , 4 of these
exh ib i ted filling defect . A l though in 3 of the
l a t t e r pat ients g a l l b l a d d e r tumors could have
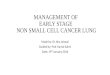
been suspected, only one (No. 5) who showed a
large filling defect (F ig . 1) was preopera t ive ly
d iagnosed as ga l l b l adde r ca rc inoma. Ultra-
sonography (US) was pe r fo rmed in 2 pat ients
(No. 5 and 9) and s t rong echo without acoustic
shadow was ob ta ined in bo th cases. In 3 pa-
t ients subjected to celiac ang iography (CA),
hypervascular i ty was no ted in pe r iphera l
b ranches of the cystic artery; findings on the
t runk of the cystic a r te ry were equivocal in
these pat ients . Only 3 of 9 pat ients with ear ly
ca rc inoma of the g a l l b l a d d e r were correct ly
d iagnosed before surgery; the r ema in ing 6 pa -
t ients were not d iagnosed unt i l they were ex-
amined histologically.
Extended cholecystectomy was pe r fo rmed in
the preopera t ive ly d iagnosed pat ients , the
others underwent s imple cholecystectomy. In
macroscopic examina t ion , none of these 9 pa -
tients showed invasion or metastasis to the liver
and regional l ymph nodes. On the other hand ,
microscopic examina t i on revealed that , except
a pa t ien t in g roup p m with lymphat ic infi l tra-
t ion (lyl) and INFv, all pa t ients demons t r a t ed
v0, ly0, ne0, INF~ in g roup m and v0, ly0, ne0,
INFa in g roup pm.

October 1981 Early Carcinoma of the Gallbladder 463
Fig. 1. Cholecystogram of case No. 5 obtained by drip infusion cholangiography. Filling defect (arrow) is ob- served at the fundus of the gallbladder.
Discussion
Early gastric cancer is defined as that stage in
which the depth of invasion is limited to the
submucosal layer2). However, in carcinoma of
the gallbladder, this definition is not applica-
ble, because the submucosal layer of this organ
is very thin and frequently lacking. Moreover,
unlike the stomach, the gallbladder has no
lamina muscularis mucosa, which forms a
boundary between the mucosal- and proper
muscle layer, thereby representing a defense
wall against cancer invasion. Therefore, in pa-
tients with cancer of the gallbladder, if the sub-
mucosal layer is involved, the proper muscle
layer is also affected. For this reason, the depth
of invasion of gallbladder cancer was classified
into m, pm and s. Based upon the present
studies, it was proposed that patients in groups
m and pm should be subsumed under the cate-
gory of early cancer of the gallbladder.
Nevin et el.4) classified carcinoma of the gall-
bladder into 5 stages. Stage I involves only
mucosa, stage II, the mucosa and muscularis
layer, stage III , all three layers, and stage IV,
V show metastasis to lymph nodes or liver. Our
definition of early cancer of the gallbladder
coincides with their first two stages. Late results
reported by them revealed that all patients in
stage I and II survived for 5 years; in contrast,
only 7 % of stage I I I patients survived for this
period. As their results are similar to ours, it
might be reasonable to include the patients of
m and pm as the category of early gallbladder
cancer. There was one patient in the p m group who
died 2 years 3 months after the surgery due to the recurrence. The type of cancer was macro-
scopically infiltrative and histologically tubular
adenocarcinoma. In addition, lymphatic vessel
invasion was noted and the cancer spread was of type INF, . This suggests that even in cases
classified as early gallbladder cancer, long-
term postoperative survival may not be ob-
tained if the cancer is of nodular or infiltrative
appearance and of tubular adenocarcinoma or
adenosquamous carcinoma.
Nevin et al. 4) also classified gallbladder can-
cer into 3 types according to histological grades of differentiation. They obtained a 5-year sur-
vival rate of 60 % for cancers of the well-differ-
entiated type. Al though our histological clas-
sification was somewhat different from theirs,
our results were similar.
Present studies indicate that DIC, ultrasono-
g raphy and ar ter iography are valuable diag-
nostic tools in patients with early gallbladder
cancer. A small filling defect in the gallbladder
shadow, obtained f rom careful inspection of
DIC, a strong echo with the absence of an

464 T. S A T O E T A L . Vol. 16, No. 5
acoustic shadow on ultrasonography, and hypervascularity of peripheral branches with- out encasement of the trunk of the cystic artery in angiography may be indicative of early car-
cinoma of the gallbladder. However, if cancer involvement is limited to the mucosal layer, it has little chance to make a diagnosis preopera- tivelyS.6). Therefore, we stress the importance of examining the gallbladder wall during operation. If cancer is suspected, intraopera- tive histological examination of the resected specimen is mandatory.
It is suggested that extended cholecystectomy should be the standard surgical treatment of patients with early cancer of the gallbladder. In our series of early cancer patients under- taken simple cholecystectomy, the survival rate was satisfactory. However, this does not war- rant the conclusion that this type of surgical therapy is adequate in patients with early gall- bladder cancer. The possibility cannot be ruled out that the patient of group pm who died of
recurrence in a short period after simple chole- cystectomy may have survived longer if ex- tended cholecystectomy had been performed. Further detailed examination of the gallblad- der, liver and lymph node specimens, obtained by extended cholecystectomy, may be signifi- cant to study for the characterization of early gallbladder cancer.
References
1) Piehler JM, et al: Primary carcinoma of the gallblad- der. Surg Gynecol Obstet 147: 929, 1978
2) Japanese Research Society for Gastric Cancer: The general rules for the gastric cancer. Jpn J Surg 3: 61, 1973
3) Murakami T: Surgical Treatment of Gastric Cancer, in "Gastroenterology", 3rd ed, Vol I, by Bockus EL, WB Saunders, Philadelphia, 1974, p 983
4) NevinJE, et al: Carcinoma of the gallbladder. Cancer 37: 141, 1976
5) Albores-Saavedra J, et al: The precursor lesions of in- vasive gallbladder carcinoma. Cancer 45: 919, 1980
6) Laito M: Early carcinoma of the gallbladder. Beitr Path 158: 159, 1976







![Squamous Cell Carcinoma of the Middle Ear …temporal bone malignancy, especially squamous cell carcinoma[14]. The early symptoms of temporal bone carcinoma closely resemble those](https://img.pdfslide.us/doc/110x75/5f027ff47e708231d4049179/squamous-cell-carcinoma-of-the-middle-ear-temporal-bone-malignancy-especially-squamous.jpg)