Embed Size (px)
Citation preview
212 BRIT. J. SURG., 1964,
current forms of primary therapy comprise local attacks on the primary tumour and its regional lymphatic drainage depots. Various extensions and refinements of the surgical and radiotherapeutic methods have increased local control significantly, but this improvement has not been as marked in the overall salvage rate. The great levelling influence of systemic spread is still an unsolved problem.
Despite the limitations of our present techniques of primary therapy, they must be used to the utmost
Vol. 51, No. 3, MARCH
for want of a better alternative. A desperate need remains for the development of an effective systemic treatment for breast cancer.
REFERENCES AUCHINCLQSS, H., jun. (1958), Cancer, I I, 611. HANDLEY, R. S., and THACKRAY, A. C. (1954), Brit. med.
TURNER-WARWICK, R. T. (1959), Brit. J . Surg., 46, 574. URBAN, J. A. (1956), Surg. Clin. N. Amer., 36, 1065.
J., I, 61.
EARLY CANCER OF THE BREAST
BY JOHN BRUCE AND IAN TOUGH DEPARTMENT 0 1 ’ CLINICAL SURGERY, UNIVERSITY OF EDINBURGH
IN 1940 the surgeons in Edinburgh and in the districts that constitute its clinical hinterland agreed, together with their radiotherapeutic colleagues, to investigate the treatment of cancer of the breast by simple mastectomy and radiotherapy. The programme, variously referred to as the ‘Edinburgh’, or the ‘ McWhirter’, technique, aroused and continues to stimulate controversy. Some of the criticisms have been bitter, some irrelevant, and some have been based on a misunderstanding of the objective and the theoretical nature of the policy. The situation has not been particularly helped by the fact that the results have generally been reported in radiological literature, and the surgeons participating have remained behind a cloak of anonymity.
This contribution seeks to remedy this in part by presenting the results of a series of breast cancers treated in 1946-55 in a number of units with which the senior contributor was associated, and we are grateful to Professor McWhirter for access to the records of his department which have allowed us to complete a very accurate follow-up.
The Background of the Investigation.-It is important, in reaching an assessment of the value of the Edinburgh investigation, to appreciate the back- ground against which it was conducted.
Until 1940 the orthodox treatment for breast cancer in Edinburgh was the Halsted type of radical mastec- tomy. The results were as disquieting as elsewhere, and it should be remarked that Sampson Handley, with his radium needles in the intercostal spaces; Keynes, with his radium-needle technique; and Mitchiner, with his simple excision of the turnour, were obviously also disturbed by the shortcomings of the conventional treatment. How well founded these misgivings were has only become evident with increasing knowledge of the natural history of breast cancer; but in comparing old and new techniques it is worth while recalling that in the early decades of the century virtually the only course open to the majority of surgeons was a radical mastectomy, and the operation was carried out on many patients whom subsequent studies and greater knowledge have shown to be completely outwith the justifiable range of radical surgery.
The cause of death in the majority of patients was disseminated cancer, but in addition a number had
local recurrences also, and there was a general impression that in the patients with more advanced local disease the operation stimulated both local recrudescence and systemic spread.
The obvious courses open to thoughtful surgeons were : ( I ) T o employ the orthodox radical operation only in more suitable cases, i.e., to select the appro- priate patients; or (2) T o design a still more radical line of attack.
Eventually the surgeons in Edinburgh opted for the second of these alternatives, and designed a treatment policy in which the destruction of disease beyond the breast was to be accomplished by radiation rather than by the scalpel.
It is only fair to emphasize that in concept the Edinburgh policy was not a more conservative approach but a more radical one. The choice of radiotherapy rather than surgery may well have been influenced by an impression that at a certain stage of the disease operation was definitely harmful, and by the evidence that postoperative therapy already appeared to diminish the incidence of chest-wall recurrences after the orthodox radical operation.
Unfortunately, the policy was not submitted to a controlled trial. Controlled trials were not then in vogue, however, and the now considerable experience of the Edinburgh method must therefore be regarded as no more than a domestic record of one particular therapeutic approach.
Comparison of the results of the new policy with those of orthodox radical mastectomy are, in fact, worthless. In most of the published reports of the radical operation the patients were ‘staged’ in the light of the pathological findings in the axilla, and, while this has its own fallacies, they are as nothing compared with the fallacies of preoperative clinical staging, where there may be a 30-40 per cent dis- crepancy between different observers of the same patient.
I t has been suggested, in order to obviate the inaccuracies of staging, that comparison between different series should be on the basis of the survival rates in all cases of the disease, at all stages, treated and untreated, in the appropriate geographical area. While this may gratify the statistically inclined, it is not particularly helpful to the surgeon confronted with the woman with ‘early’ breast cancer.
SYMPOSIUM ON EARLY CARCINOMA OF T H E BREAST 213
Haagensen and Cooley Watson Dahl-Iversen Butcher Handley and Thackray Williams and Curwen Kaae and Johansen Kennedy and Miller
Nevertheless, such a comparison is possible between the Edinburgh series and that reported from Saskat- chewan by Watson (1959) (Table IZI). In the latter series the standard operation was a radical mastec- tomy, and the record seems to show a slight superi- ority over the Edinburgh series.
PRESENT INVESTIGATION In the series we have reviewed, which is, of
course, included in the more complete reports by
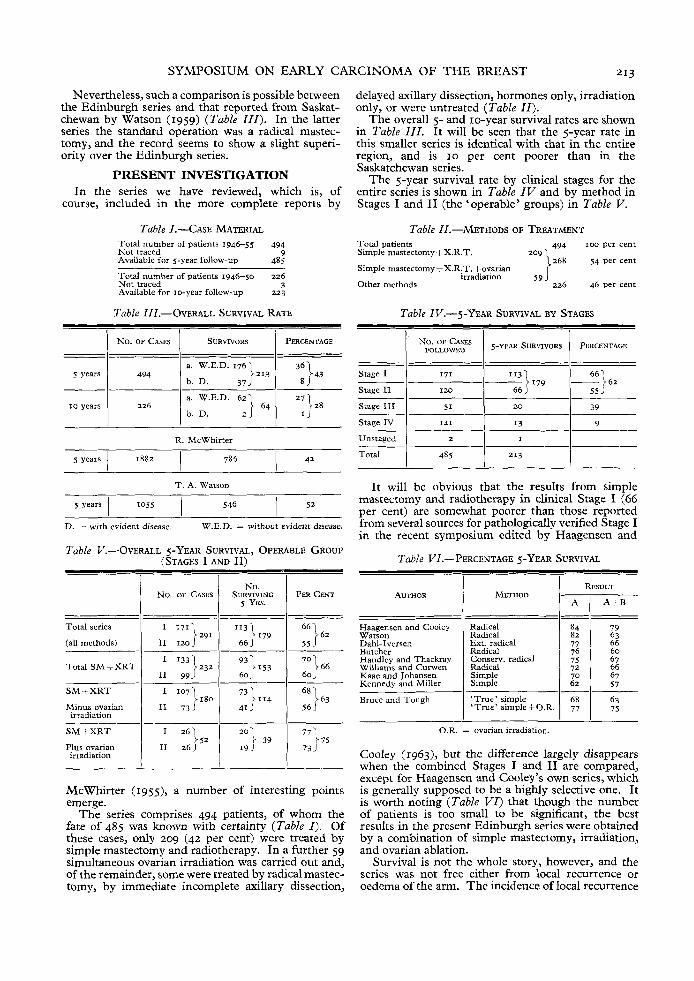
Table I.-CASE MATERIAL Total number of patients 1946-55 494 Not traced 9 Available for 5-year follow-up 485
Total number of patients 1946-50 226 Not traced 3 Available for 10-year follow-up 223
Table III.-OVERALL SURVIVAL RATE
1 No. OF CASES 1 SURVIVoRs I PERCENTAGE
-_ Radical Radical Ext. radical Radical Conserv. radical Radical Simple Simple
a. W.E.D. 176)213 I 3;) 43 I 494 I b. D. 37
s years
- - ~ - ~ _ _ _ 84 79 82 63 77 66 76 60 75 67 72 66 70 67 62 57
b. D. I J
SM2 XRT
Minus ovarian irradiation
SM i XRT
Plus ovarian irradiation
---__
R. McWhirter
786 1 42 I 5 years 1 18x2
1 6 3 I 107]180 731114 68 II 73 41 J 56 J
I 261 77175 73J
2ol 39 > 52 I1 26J I9 J
~~ ~~
T. A. Watson
D. - with evident disease. W.E.D. = without evident disease.
Table V.-OVERALL 5-YEAR SURVIVAL, OPERABLE GROUP (STAGES I AND 11)
Total series
(all methods)
McWhirter (1955), a number of interesting points emerge.
The series comprises 494 patients, of whom the fate of 485 was known with certainty (Table I) . Of these cases, only 209 (42 per cent) were treated by simple mastectomy and radiotherapy. In a further 59 simultaneous ovarian irradiation was carried out and, of the remainder, some were treated by radical mastec- tomy, by immediate incomplete axillary dissection,
delayed axillary dissection, hormones only, irradiation only, or were untreated (Table I I ) .
The overall 5- and 10-year survival rates are shown in Table I I I . It will be seen that the 5-year rate in this smaller series is identical with that in the entire region, and is 10 per cent poorer than in the Saskatchewan series.
The 5-year survival rate by clinical stages for the entire series is shown in Table IV and by method in Stages I and I1 (the ‘operable’ groups) in Table V.
Table II.-METHODS OF TREATMENT Total patients 494 IOO per cent Simple mastectomv I X.R.T. 209 1 . .
Simple mastectomy+X.R.T. +ovarian }268 54 per cent
226 46 per cent Other methods irradiation 5 9 J
Table IV.-S-YEAR SURVIVAL BY STAGES
Stage IV 1 141 1 I 3 I 9
Unstaaed 1 2 1 1 I I Total ~ I 485 1 213
It will be obvious that the results from simple mastectomy and radiotherapy in clinical Stage I (66 per cent) are somewhat poorer than those reported from several sources for pathologically verified Stage I in the recent symposium edited by Haagensen and
Table VI.-PERCENTAGE S-YEAR SURVIVAL ~
AUTHOR METHOD I RESULT 1 A 1 A t B
~ ~ ~~
Bruce and Tough ‘True’ simple 63 7s 1 ‘True’simplet0.R. 1 ;; I
O.R. = ovarian irradiation.
Cooley (1963)~ but the difference largely disappears when the combined Stages I and I1 are compared, except for Haagensen and Cooley’s own series, which is generally supposed to be a highly selective one. It is worth noting (TabZe V I ) that though the number of patients is too small to be significant, the best results in the present Edinburgh series were obtained by a combination of simple mastectomy, irradiation, and ovarian ablation.
Survival is not the whole story, however, and the series was not free either from local recurrence or oedema of the arm. The incidence of local recurrence
214 BRIT. J. SUEPG., 1964, Vol. 51, No. 3, MARCH
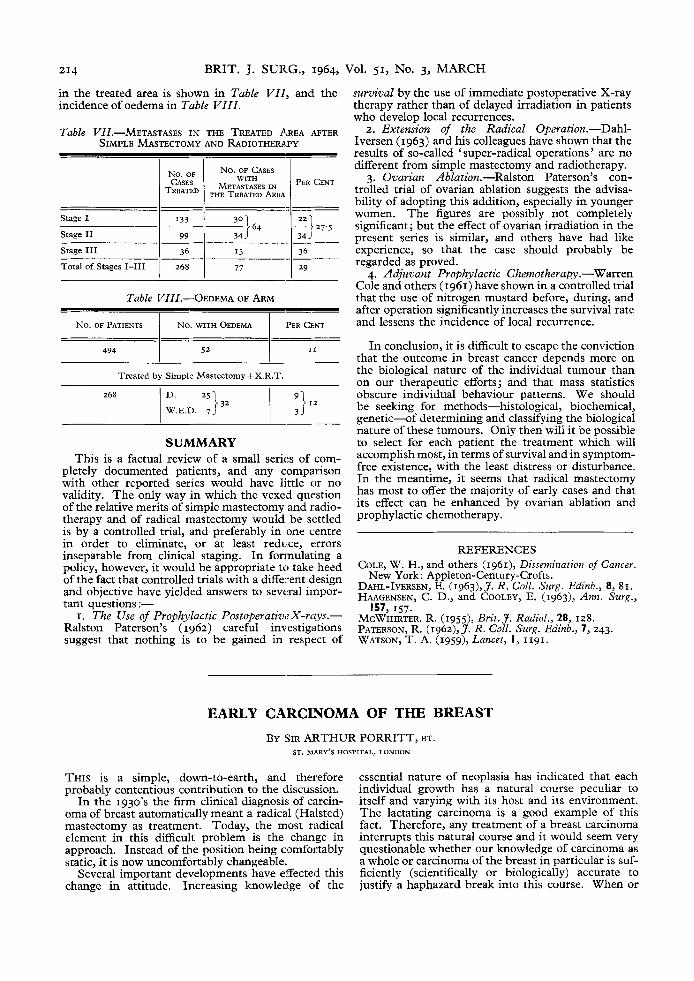
in the treated area is shown in Table VIl , and the incidence of oedema in Table VIII .
Table VZZ.-METASTASES IN THE TREATED AREA AFTER SIMPLE MASTECTOMY AND RADIOTHERAPY
No, OF No. OF CASES 1 1 M E T E k . E s I N 1 CENT TREATED THE TREATED AREA
Stage I
Stage I1 34J
__- I 77 Total of Stages 1-111 I 268
Table VZZZ.-OEDEMA OF ARM
No. OF PATIENTS No. WITH OEDEMA PER CENT
494 I t
Treated by Simple Mastectomy tX .R .T
SUMMARY This is a factual review of a small series of com-
pletely documented patients, and any comparison with other reported series would have little or no validity. The only way in which the vexed question of the relative merits of simple mastectomy and radio- therapy and of radical mastectomy would be settled is by a controlled trial, and preferably in one centre in order to eliminate, or at least redwce, errors inseparable from clinical staging. In fonnulating a policy, however, it would be appropriate to take heed of the fact that controlled trials with a different design and objective have yielded answers to several impor- tant questions :-
I. The Use of Prophylactic Postoperativt. X-rays.- Ralston Paterson’s (1962) careful investigations suggest that nothing is to be gained in respect of
survival by the use of immediate postoperative X-ray therapy rather than of delayed irradiation in patients who develop local recurrences.
2. Extension of the Radical Operation.-Dahl- Iversen (1963) and his colleagues have shown that the results of so-called ‘ super-radical operations ’ are no different from simple mastectomy and radiotherapy.
3. Ovarian Ablation.-Ralston Paterson’s con- trolled trial of ovarian ablation suggests the advisa- bility of adopting this addition, especially in younger women. The figures are possibly not completely significant; but the effect of ovarian irradiation in the present series is similar, and others have had like experience, so that the case should probably be regarded as proved.
4. Adjuvant Prophylactic Chemotherapy.-Warren Cole and others (1961) have shown in a controlled trial that the use of nitrogen mustard before, during, and after operation significantly increases the survival rate and lessens the incidence of local recurrence.
In conclusion, it is difficult to escape the conviction that the outcome in breast cancer depends more on the biological nature of the individual tumour than on our therapeutic efforts; and that mass statistics obscure individual behaviour patterns. We should be seeking for methods-histological, biochemical, genetic-of determining and classifying the biological nature of these tumours. Only then will it be possible to select for each patient the treatment which will accomplish most, in terms of survival and in symptom- free existence, with the least distress or disturbance. In the meantime, it seems that radical mastectomy has most to offer the majority of early cases and that its effect can be enhanced by ovarian ablation and prophylactic chemotherapy.
REFERENCES COLE, W. H., and others (1961), Dissemination of Cancer.
DAHL-IVERSEN, E. (1963),J. R. Coll. Surg. Edinb., 8, 81. HAAGENSEN, C. D., and COOLEY, E. (1963), Ann. Surg.,
MCWHIRTER. R. (1955), Brit.J. Radiol., 28, 128. PATERSON, R. (1962),J. R. Coll. Surg. Edinb., 7, 243. WATSON, T. A. (1959), Lancet, I, 1191.
New York: Appleton-Century-Crofts.
157, 157.
EARLY CARCINOMA OF THE BREAST
BY SIR ARTHUR PORRITT, BT. ST. MARY’S HOSPITAL, LONDON
THIS is a simple, down-to-earth, and therefore probably contentious contribution to the discussion.
I n the 1930’s the firm clinical diagnosis of carcin- oma of breast automatically meant a radical (Halsted) mastectomy as treatment. Today, the most radical element in this difficult problem is the change in approach. Instead of the position being comfortably static, it is now uncomfortably changeable.
Several important developments have effected this change in attitude. Increasing knowledge of the
essential nature of neoplasia has indicated that each individual growth has a natural course peculiar to itself and varying with its host and its environment. The lactating carcinoma is a good example of this fact. Therefore, any treatment of a breast carcinoma interrupts this natural course and it would seem very questionable whether our knowledge of carcinoma as a whole or carcinoma of the breast in particular is suf- ficiently (scientifically or biologically) accurate to justify a haphazard break into this course. When or