Embed Size (px)
Citation preview

Management of early and locally advanced breast cancer
Abhilash
Early breast cancer
• Stage I
• Stage II A
• Subset of Stage II B (T2N1)
Locally advanced breast cancer• Stage II B
• Stage IIIA to IIIC

Early breast cancer
Primary Surgery for breast and regional nodes–Lumpectomy or Mastectomy +/-RT
• BCSMastectomy
Adjuvant treatment if needed based on tumor characteristics.
• Tumor size
• Tumor grade
• ER/PR/HER2
• LN status

Breast conserving surgery
• To preserve the breast without sacrificing oncological outcome
BCS= LUMPECTOMY + adjuvant RT
Goals of BCS1. Cosmetically acceptable2. Survival comparable to mastectomy3. Low recurrence rates
Patient selection for BCS
• Comorbid conditions/ Age is not a contraindication.
• Nipple, skin retraction is not a contraindication – but resection of NAC should be factored in decision making.
• Extensive intraductal component is not a contraindication.
• Lymph node positivity is not a contraindication.
• Tumor location is not a contraindication.
• Not contraindicated in dense breast tissue.
• Large tumor in a small breast is a relative contraindication
• Collagen vascular disease is a contraindication.

Absolute contraindication for BCS
●Multicentric disease
●Large tumor size in relation to breast
●Presence of diffuse malignant-appearing calcifications on imaging (ie, mammogram or MRI)
●Prior history of chest wall RT
●Persistently positive margins despite attempts at re-excision

Role of neoadjuvant therapy in BCS
• Chemotherapy or hormonal therapy to reduce size of the tumor
• Clip placement in tumor bed.
• Not to be considered if multicentric with extensive skin changes and dermal lymphatic involvement.
Indications for mastectomy in early breast cancer
• Not a candidate for BCS.
• Patient choice.

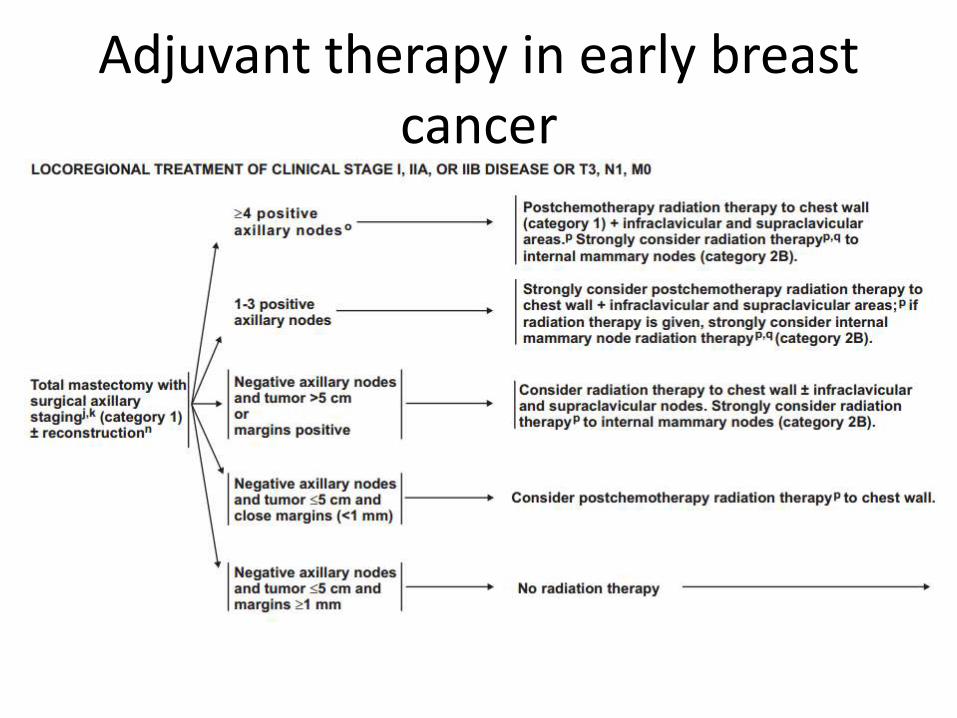
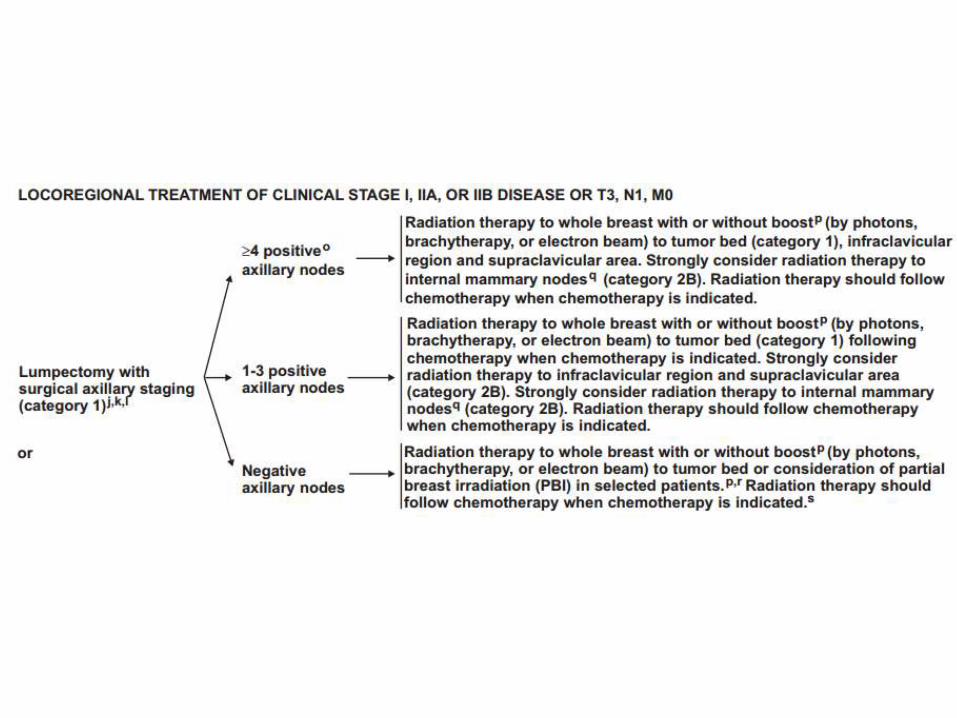
Adjuvant therapy in early breast cancer

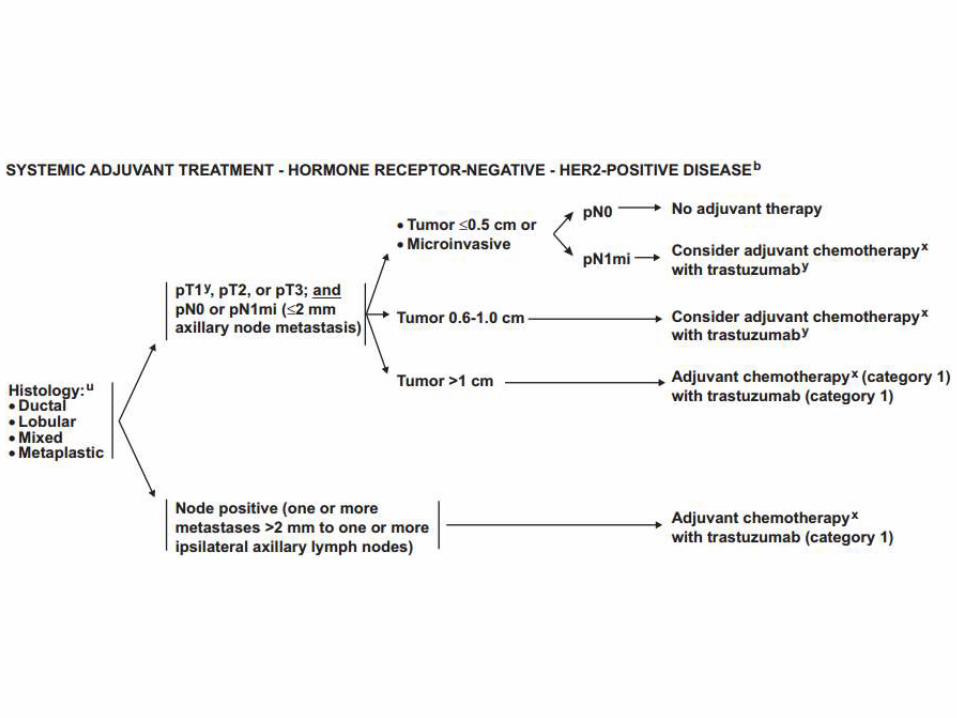
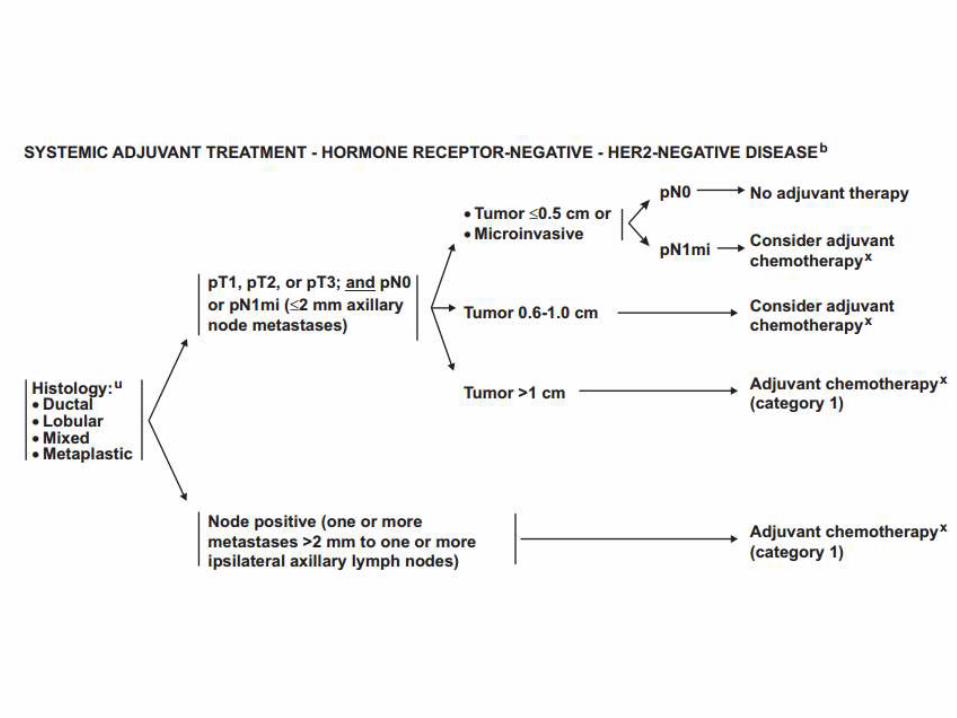
Adjuvant chemotherapy


Locally advanced breast cancer
Goal of neoadjuvant chemotherapy
• Reduce risk of distant recurrence.
• Improve surgical outcome in patients
– Inoperable disease.
– Operable disease desiring breast conservation
Candidates for neoadjuvanttherapy
• T4 lesions.
• HER2 positive – high pCR to NACT with transtuzumab.
• Triple negative disease – High pCR rates compared to HER2 negative ER/PR+ (27-45% vs 10%)
• Breast cancer in pregnancy.
• Early disease if BCS not possible due to small breast.

Pretreatment evaluation before NACT
• Core biopsy – ER/PR/HER2
• Radio-opaque clips to be placed for subsequent assessment of surgical specimen and for RT planning.
• Metastatic workup.
• Axillary node evaluation and staging has to be done. SLNB/axillary US with FNA - to be done if no palpable nodes or FNA from palpable node is negative.

Neoadjuvant treatment options
• Triple negative disease – NACT BCS/mastectomy.
• Post menopausal women – if not a candidate for chemo/surgery Hormonal therapy.
• HER2 positive – NACT + transtuzumab
Neoadjuvant endocrine therapy
• Aromatase inhibitor or tamoxifen
• 4-6 months.
• May be as effective as NACT in postmenopausal women.

Adjuvant RT
• For all BCS
• For post total mastectomy with high risk of recurrence.
1. Positive margins,
2. lymphovascular invasion,
3. >4 axillary nodes with tumour,
4. size > 5 cm
5. high grade tumour.
Adjuvant chemotherapy
• Lymph nodes positive
• Tumour > 1 cm
• Grade 2 or 3
• ER/PR negative

Adjuvant therapy
• If post NACT Surgery –
– ER/PR + , hormonal therapy
– ER/PR - ,Chemotherapy
– HER2 , transtuzumab
• If post neoadjuvant endocrine therapySurgery endocrine therapy +/- NACT
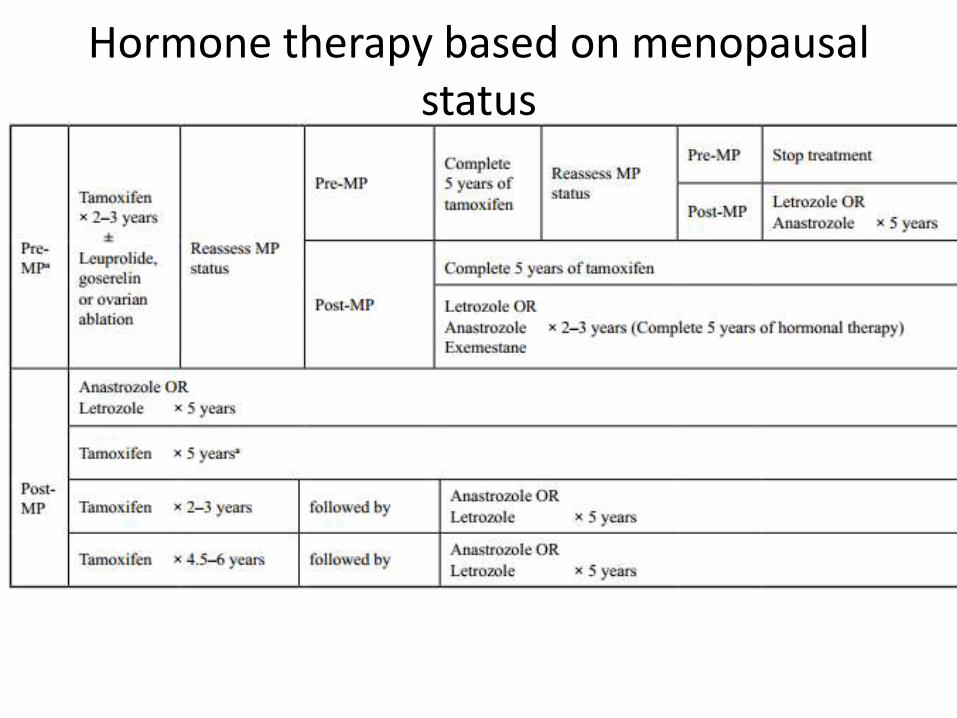
Hormone therapy based on menopausal status

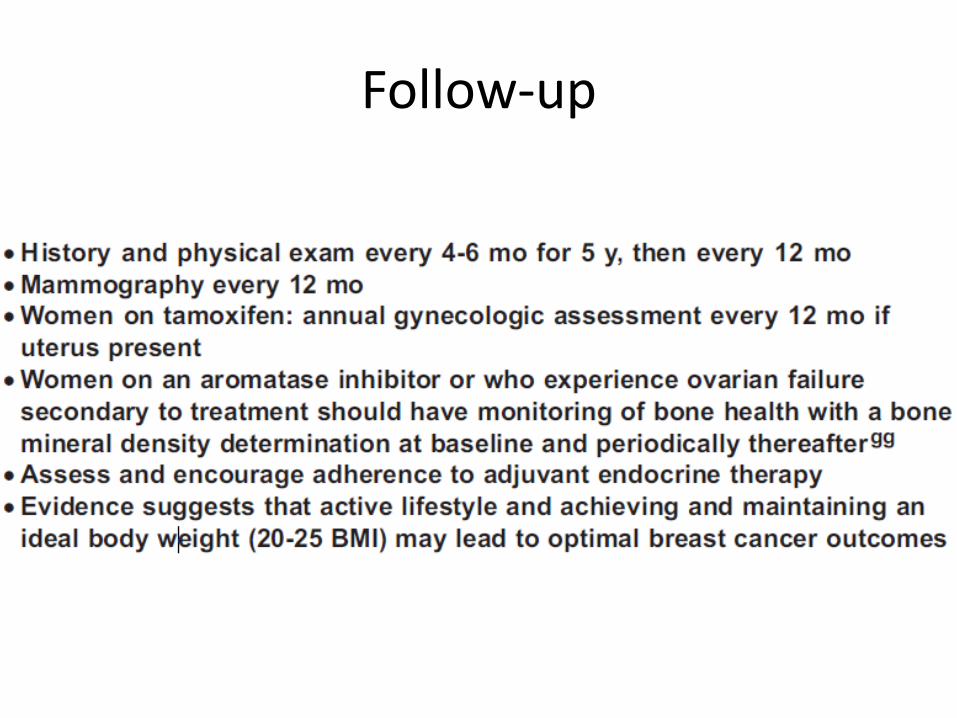
Follow-up





























