Embed Size (px)
Citation preview

Dysregulation of the mevalonate pathwaypromotes transformationJames W. Clendeninga,b, Aleks Pandyraa,b, Paul C. Boutrosa,b,2, Samah El Ghamrasnia,b, Fereshteh Khosravia,Grace A. Trentina, Anna Martirosyana, Anne Hakema,b, Razqallah Hakema,b, Igor Jurisicaa,b,c, and Linda Z. Penna,b,1
aOntario Cancer Institute, Toronto, ON, Canada; and the Departments of bMedical Biophysics and cComputer Science, University of Toronto,Toronto, ON, Canada
Edited* by Tak Wah Mak, Campbell Family Institute for Breast Cancer Research, Ontario Cancer Institute at Princess Margaret Hospital,University Health Network, Toronto, ON, Canada, and approved July 13, 2010 (received for review September 14, 2009)
The importance of cancer metabolism has been appreciated formany years, but the intricacies of how metabolic pathways inter-connect with oncogenic signaling are not fully understood. Witha clearunderstandingofhowmetabolismcontributes to tumorigen-esis, we will be better able to integrate the targeting of thesefundamental biochemical pathways into patient care. The mevalo-nate (MVA) pathway, paced by its rate-limiting enzyme, hydroxy-methylglutaryl coenzyme A reductase (HMGCR), is required forthe generation of several fundamental end-products includingcholesterol and isoprenoids. Despite years of extensive researchfrom the perspective of cardiovascular disease, the contributionof a dysregulated MVA pathway to human cancer remains largelyunexplored. We address this issue directly by showing that dysre-gulation of the MVA pathway, achieved by ectopic expression ofeither full-length HMGCR or its novel splice variant, promotestransformation. EctopicHMGCRaccentuatesgrowthof transformedandnontransformedcellsunderanchorage-independent conditionsor as xenografts in immunocompromised mice and, importantly,cooperates with RAS to drive the transformation of primarymouse embryonic fibroblasts cells. We further explore whetherthe MVA pathwaymay play a role in the etiology of human cancersand show that high mRNA levels of HMGCR and additional MVApathway genes correlate with poor prognosis in a meta-analysisof six microarray datasets of primary breast cancer. Taken together,our results suggest that HMGCR is a candidate metabolic oncogeneand provide a molecular rationale for further exploring the statinfamily of HMGCR inhibitors as anticancer agents.
HMGCR ∣ hydroxymethylglutaryl coenzyme A reductase ∣ cancer ∣metabolic oncogene ∣ tumor metabolism
The classic hallmarks of cancer are intimately intertwined withan assortment of metabolic processes that a tumor cell effec-
tively hijacks to enable malignant transformation (1–3). Recentwork has highlighted the importance of fundamental metabolicgenes and pathways in tumor development and progression(1, 4–6). A better understanding of their contributions to tumor-igenesis, as well as how they can best be targeted for therapeuticintervention, will lead to improved cancer patient care.
As early as the 1920s (7), it has been known that many tumorcells rapidly metabolize glucose to supply their energetic require-ments, even under conditions of high oxygen. For tumor cells, akey benefit of relying on glycolysis is that glucose breakdownalso provides a carbon source for anabolic synthesis of criticalbiochemical precursors (8). In this manner, for example, acetyl-CoA is made available for the synthesis of several lipid buildingblocks, including mevalonate (MVA).
The MVA pathway is a complex biochemical pathway requiredfor the generation of several fundamental end-products includingcholesterol, isoprenoids, dolichol, ubiquinone, and isopentenyla-denine (9). At the heart of this pathway is the rate-limiting en-zyme, hydroxymethylglutaryl coenzyme A reductase (HMGCR).Both HMGCR and the MVA pathway received considerableattention decades ago, primarily through the Nobel Prize-winning
efforts of Goldstein and Brown and the development of the cho-lesterol-lowering drugs known as statins (9, 10). Statin inhibitionof HMGCR in normal cells triggers a robust homeostatic feed-back response that ensures the cells upregulate and restorethe MVA pathway (9), a mechanism that has been successfullyexploited for over 20 years to control hypercholesterolemia (11).
A number of tumors have been reported to have eitherdeficient feedback control of HMGCR, or increased HMGCRexpression and activity (12, 13). Exogenous MVA administered toxenograft-bearing mice was also shown to promote tumor growth(14). Finally, recent epidemiological studies have shown thatpatients taking certain statins for cholesterol control displayeda decreased risk of developing some cancers (15–21). Taken to-gether, these results suggest that HMGCRmay play an importantrole in human malignancies. Indeed, recent transcriptional pro-filing demonstrated that cholesterol and lipid metabolism arelinked to cellular transformation (22). However, it is not knownwhether dysregulation of HMGCR and theMVA pathway make acausal contribution to cancer etiology or whether their dysregula-tion occurs as a consequence of transformation.
In addition to being tightly regulated at many levels (9),HMGCR has also been shown to be alternatively spliced such thatthere are two isoforms: full-length HMGCR (HMGCR-FL) and aversion lacking exon 13 (HMGCR-D13) (23). Coding for a smallregion of the catalytic domain, exon 13 includes several residuesimportant for binding both substrates and statins (Fig. 1A).A func-tional SNP has been identified (rs3846662) that regulates the spli-cing of HMGCR (24). Interestingly, overall risk of developingcolorectal cancer was recently shown to correlate with genotypeat rs12654264, a SNP in linkage disequilibrium with rs3846662,in statin-users but not nonusers, suggesting that patients whosecells expressed more HMGCR-D13 did not experience as muchprotective benefit from statin use (21). Transcript expression ofHMGCR-D13 has also been associated with a decreased choles-terol-lowering response in lymphocytes exposed to simvastatin,suggesting it is refractory to inhibition by statins (25). Further workindicated that HMGCR-D13 is enzymatically inactive (24),prompting speculation that it may interfere with the regularactivity of HMGCR-FL (26). Investigations into the transformingactivities of either HMGCR-FL or -D13, however, have not beenreported. Therefore, we have explored the role HMGCR plays incancer and assessed whether dysregulation of the MVA pathwaycan be causal to transformation.
Author contributions: J.W.C., A.P., P.C.B., S.E.G., G.A.T., A.H., R.H., I.J., and L.Z.P. designedresearch; J.W.C., A.P., P.C.B., S.E.G., F.K., G.A.T., and A.M. performed research; J.W.C., A.P.,P.C.B., S.E.G., A.H., R.H., and L.Z.P. analyzed data; and J.W.C. and L.Z.P. wrote the paper.
The authors declare no conflict of interest.
*This Direct Submission article had a prearranged editor.1To whom correspondence should be addressed. E-mail: [email protected] address: Bioinformatics and Biocomputing Platform, Ontario Institute for CancerResearch, Toronto, ON, Canada M5G 0A3.
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.0910258107/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.0910258107 PNAS ∣ August 24, 2010 ∣ vol. 107 ∣ no. 34 ∣ 15051–15056
BIOCH
EMISTR
Y

ResultsTo detect both HMGCR transcripts independently and specifi-cally, we devised a real-time PCR strategy using exon junction-spanning primers (Fig. 1A). Additionally, to study HMGCR ina human system with a well-regulated MVA pathway, we choseto work with HepG2 cells that have been characterized exten-sively as an ideal model for the study of MVA pathway homeos-tasis (27, 28). We first determined that HMGCR-FL is expressedat higher levels than HMGCR-D13 in HepG2 cells (Fig. 1B).Next, to address whether transcript expression of these HMGCRisoforms is regulated similarly or differently, we exploited statinsas a tool to block HMGCR activity and trigger the feedbackresponse that up-regulates its expression (9). HepG2 cells wereexposed to 20 μM lovastatin for 4 to 48 h, and mRNA washarvested for real-time PCR analysis. Similar to total HMGCRtranscript expression (Fig. 1C), we show that both HMGCR-FL(Fig. 1D) and HMGCR-D13 (Fig. 1E) are upregulated in re-sponse to lovastatin exposure with similar magnitudes and ki-netics, suggesting that they are coregulated.
To determine whether dysregulation of the MVA pathway andHMGCR activity can drive transformation, expression constructswere generated to ectopically express each HMGCR isoform(Fig. 2A). To ensure that the constructs would be expressed ina deregulated state, only the catalytic domain was included(cHMGCR-FL and cHMGCR-D13), without their commontransmembrane domain that harbors negative regulatory ele-ments (29). Using real-time PCR we measured higher HMGCRtranscript levels in cell lines expressing the ectopic constructs(Fig. 2B). Though ectopic expression of cHMGCR-FL increasedtotal FL transcript levels about twofold, ectopic expression ofcHMGCR-D13 increased total D13 transcript levels about300-fold, to a roughly equal amount as FL. When exposed tolovastatin, only cells expressing HMGCR-FL showed a decreasein upregulation of total endogenous HMGCR transcript expres-sion (Fig. 2C). HepG2 cells expressing the cHMGCR-D13 variantupregulated total endogenous HMGCR transcript expression toa similar level as the GFP control cells.
Antibodies to human HMGCR are not well establishedbecause most previous work on the protein was conducted innonhuman systems.While a few are now available, their specificityhas not been thoroughly validated. We therefore characterizedtwo commercially available antibodies and showed one to bespecific (Fig. S1). This antibody was used to confirm ectopicexpression of our constructs (Fig. 2D).
To assess the impact of HMGCR-FL and -D13 on cancer cells,we assayed whether ectopic expression of either isoform couldalter the growth and proliferation of HepG2 cells. Using both
proliferation (Fig. 3A) and cell cycle analyses (Fig. 3B) we demon-strated that ectopic expressionof cHMGCR-FLor cHMGCR-D13does not affect the rate of cellular proliferation. Furthermore,when cells were exposed to common chemotherapy drugs,doxorubicin and taxol, we also showed that cHMGCR-FL andcHMGCR-D13 are not antiapoptotic in the same manner asBCL2 (Fig. 3C).
However, when cells were seeded in soft agar assays to assesstheir capacity for anchorage-independent growth we demon-strated that both the FL and D13 constructs increase transforma-tion (Fig. 3D). These results were confirmed in vivo when HepG2cells expressing either the empty GFP vector or one of the twocHMGCR constructs were injected into opposing flanks of sub-lethally irradiated severe combined immuno-deficient (SCID)mice. In both cases, we observed larger and faster-growing tumorsin the flanks of mice that had been injected with HepG2 cellsexpressing one of the two cHMGCR isoforms compared tothe GFP control (Fig. 3 E and F) and observed approximatelyequal levels of HMGCR ectopic protein expression in tumorextracts (Fig. S2).
To address the impact of HMGCR on cells of different origin,we assessed whether dysregulation of the MVA pathway could in-crease transformation in additional cell types. cHMGCR-FL andcHMGCR-D13 were introduced into transformed MCF7 breastcarcinoma cells (Fig. S3), which were then seeded in soft agarto assess their ability to grow in an anchorage-independentmanner (Fig. 4A). Ectopic expression of both cHMGCR-FLand cHMGCR-D13 increased the number of colonies formed.Interestingly, when cHMGCR-FL and cHMGCR-D13 were intro-duced into MCF10A cells (Fig. S3), we demonstrated that dysre-gulation of the MVA pathway could also drive transformationof immortalized, nontransformed breast cells (Fig. 4B). As wasobserved in HepG2 cells, we confirmed that ectopic expressionof cHMGCR did not inhibit cell death in breast cells (Fig. S4).To test the capacity of HMGCR to potentiate transformation inan entirely different model we introduced cHMGCR-FL andcHMGCR-D13 into normal murine bone marrow or fetal livercells. In this case, only cHMGCR-FL increased myeloid colonyformation in methylcellulose, whereas cHMGCR-D13 did not(Fig. 4C). Finally, we further evaluated the oncogenic potentialof HMGCR by determining if cHMGCR-FL or cHMGCR-D13could drive transformation and cooperate with conventionaloncogenes. To this end we performed a series of classic transfor-mation experiments in primary wild-typeMEF cells. Interestingly,both cHMGCR-FL and -D13 were able to cooperate with RAS,but not E1A, to promote foci formation (Fig. 4D). Together, these
Fig. 1. HMGCR-FL and HMGCR-D13 transcript levels are upre-gulated in response to lovastatin exposure. (A) A schematic re-presentation of HMGCR-FL and its splice variant, HMGCR-D13,at the genomic, transcript, and protein levels with real-timePCR primers used to assess total endogenous HMGCR and eachof HMGCR-FL and HMGCR-D13 specifically. (B) mRNA fromHepG2 cells was harvested for real-time PCR analysis of basaltranscript expression to show that HMGCR-FL is expressed athigher levels than HMGCR-D13. mRNAwas also harvested fromHepG2 cells exposed to either ethanol vehicle control or 20 μMlovastatin for the times indicated. Transcript expression of totalendogenous HMGCR (C), HMGCR-FL (D) and HMGCR-D13 (E) allincreased over time after lovastatin exposure. Data is expressedas log2 ratios of expression in lovastatin-exposed cells com-pared to ethanol-treated cells. * p < 0.05; one sample t-testcomparing to 0, i.e., no induced expression. All experimentswere performed a minimum of three times and data representmeans and standard deviations.
15052 ∣ www.pnas.org/cgi/doi/10.1073/pnas.0910258107 Clendening et al.

results clearly argue that HMGCR has oncogenic potential andsupport a causal role for HMGCR in tumorigenesis.
Having seen that ectopic HMGCR expression accentuatedtransformation of human breast cells (MCF-7 and MCF-10A),we next addressed the impact of HMGCR on breast cancerpatient survival by performing a meta-analysis of six large primarypatient microarray datasets, encompassing 865 patients (30–35).Patients were dichotomized on the basis of their HMGCR abun-dance and Kaplan–Meier survival curves were plotted with differ-ences in outcome evaluated using a Cox proportional hazards
model. This analysis complemented our cell line data by showingthat high HMGCR levels were associated with poor patient prog-nosis and reduced survival, with a hazard ratio of 1.5 (95% CI1.15 to 1.95; p ¼ 0.0029) (Fig. 5 Upper Left).
To further assess if mRNA levels of other MVA pathway genescould be correlated to patient survival we selected five additionalrepresentative genes [hydroxymethylglutaryl coenzyme A syn-thase 1 (HMGCS1), mevalonate diphosphate decarboxylase(MVD), farnesyl pyrophosphate synthase (FDPS), acetoacetyl-CoA thiolase 2 (ACAT2), and mevalonate kinase (MVK)]. Re-
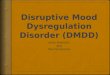
Fig. 3. Dysregulation of the MVA pathway by ectopiccHMGCR-FL and cHMGCR-D13 expression increases transforma-tion of HepG2 cells. HepG2 cells expressing the indicated con-structs were seeded in proliferation assays (A) or for cell cycleanalysis by fixed PI (B) but no difference in growth rate or cellcycle was observed. (C) Similarly, cells exposed to 2 μM doxor-ubicin or 10 nM taxol were not protected from cell death byexpression of either cHMGCR-FL or cHMGCR-D13, whereasBCL2 inhibited cell death significantly. Cell death was assessedby measurement of subdiploid DNA content (% pre-G1) in fixedPI assays combined with flow cytometry. * p < 0.05; student’st-test comparing ectopic construct expressing cell lines to theGFP control. Experiments were performed a minimum of threetimes and data represent means and standard deviations. (D)When seeded in soft agar assays, HepG2 cells expressing eithercHMGCR-FL or cHMGCR-D13 formed more colonies than cellsexpressing the empty GFP vector control, which was normalizedto 1 in each experiment. * p < 0.05; one sample t-test compar-ing ectopic construct expressing cell lines to the GFP control.Experiments were performed a minimum of three times anddata represent means and standard deviations. To addresstransformation in vivo, the flanks of sublethally irradiated SCIDmice were injected with HepG2 cells ectopically expressing theempty GFP vector and either cHMGCR-FL (E) or cHMGCR-D13(F). In each case, the cHMGCR construct-expressing cells grewlarger tumors more quickly than the GFP cells. * p < 0.05; stu-dent’s t-test comparing ectopic construct expressing cell lines tothe GFP control. Data represent means and standard errors ofthe mean.
Fig. 2. Ectopic expression of cHMGCR-FL andcHMGCR-D13 in HepG2 cells. (A) Schematic of theectopic HMGCR constructs. (B) Confirmation ofcHMGCR-FL and cHMGCR-D13 ectopic expression byreal-time PCR assessing both HMGCR-FL (left) andHMGCR-D13 (right) transcript expression. * p < 0.05;student’s t-test comparing ectopic construct expres-sing cell lines to the GFP control. Data representmeans and standard deviations. (C) Real-time PCRanalysis of endogenous HMGCR transcript levels inHepG2 cells expressing the indicated constructs andexposed to vehicle control or 20 μM lovastatin for16 hours. * p < 0.05; student’s t-test comparing lovas-tatin-exposed cells to ethanol-exposed cells. Datarepresent means and standard deviations. (D) Immu-noblot using Upstate/Millipore antibody #07-572detecting HMGCR protein expression in the indicatedHepG2 cell lines exposed to vehicle control or 20 μMlovastatin for 48 hours prior to being harvested forprotein lysates as described in the materials andmethods. 1—High molecular weight signal corre-sponding to oligomerizedHMGCR; 2—Approximately100 kDa band corresponding to endogenousHMGCR; 3—Approximately 60 kDa band corre-sponding to ectopic cHMGCR-FL; 4—Approximately55 kDa band corresponding to ectopic cHMGCR-D13.Tubulin was assayed as a loading control. All experi-ments were performed a minimum of three timesand one representative example is shown.
Clendening et al. PNAS ∣ August 24, 2010 ∣ vol. 107 ∣ no. 34 ∣ 15053
BIOCH
EMISTR
Y

markably, high levels of four out of five of these genes, HMGCS1,MVD, FDPS, and ACAT2, correlated with poor patient prog-nosis and reduced survival (Fig. 5). Whereas some of the genesare weakly correlated with each other (R between 0.2 and 0.4;Fig. S5), a multivariate model containing all genes (HR ¼1.22) is a weaker predictor of patient survival.
In summary, we have shown that deregulated HMGCR accent-uates transformation in tumor cells of different origin; promotescolony formation in nontransformed breast cells and normal,diploid hematopoietic cells; and cooperates with RAS to drivetransformation of primary MEFs. Furthermore, we showed thathigh mRNA levels of MVA pathway genes negatively impactedpatient prognosis. Taken together, our results demonstrate thatdysregulation of HMGCR and the MVA pathway plays a key rolein transformation and suggests that HMGCR is a candidatemetabolic oncogene.
DiscussionOur preliminary analysis of HMGCR isoforms has shown thatHMGCR-FL and HMGCR-D13 are coregulated at the mRNAlevel in response to lovastatin exposure (Fig. 1). Furthermore,HepG2 cells expressing ectopic cHMGCR-FL or cHMGCR-D13 showed decreased upregulation of basal, endogenousHMGCR protein (Fig. 2D). However, only the FL construct re-duced statin-induced upregulation of HMGCR transcript(Fig. 2C), suggesting the levels of regulation of these two isoformsare distinct and complex. The level of ectopic cHMGCR-D13transcript expression was comparable to the level of the ectopicFL transcript expression in the cell (Fig. 2B), suggesting that amechanism may be in place to ensure a certain maximal capacityof HMGCR expression is not exceeded in cells with intact regu-lation of the MVA pathway. Additionally, because transcriptlevels were roughly equal (Fig. 2B) and cHMGCR-FL proteinwas more highly expressed than cHMGCR-D13 (Fig. 2D), it ispossible that a D13 protein is relatively unstable and more readilydegraded. Thus, the regulation and interplay of HMGCR-FL and-D13 may influence MVA pathway function and statin sensitivity.
To further elucidate the role of HMGCR in cellular transfor-mation we conducted anchorage-independent growth assays intissue culture systems and xenograft models in mice. BothcHMGCR-FL and cHMGCR-D13 increased colony formation(Fig. 3D) and tumor growth in vivo (Fig. 3 E and F) using trans-formed HepG2 cells. We also showed that both deregulatedHMGCR isoforms increased transformation in transformedMCF7 cells (Fig. 4A) and nontransformed MCF10A breast cells(Fig. 4B), suggesting that HMGCR may have oncogenic poten-tial. In contrast, cHMGCR-FL, but not cHMGCR-D13, in-creased myeloid colony formation of cells derived from murinebone marrow or fetal liver (Fig. 4C), indicating that some differ-ence may exist in their transformative potential or tissue-specificactivities. Most remarkably, however, both cHMGCR-FL and-D13 cooperated with RAS, but not E1A, to transform primaryMEFs in traditional focus-formation assays.
To the best of our knowledge, no genes traditionally central tofundamental metabolic pathways have been shown to directlypromote transformation. Importantly, we provide evidence de-monstrating that dysregulation of the MVA pathway may havesufficient oncogenic potential to drive tumorigenesis as HMGCRitself appears to be capable of promoting the transformation oftransformed, nontransformed, and normal cells alike. How theMVA pathway and HMGCR become dysregulated is not yet welldefined but could occur at many levels (9). The MVA pathway asa whole is highly regulated in nontransformed cells, and loss ofany one of those regulatory mechanisms may contribute to dys-regulation of this critical pathway and ultimately drive tumorigen-esis. Recently, for example, it was determined that HMGCR canbe regulated through the transcriptional activity of hypoxia-inducible factor 1 alpha (36), a transcription factor that playsa fundamental role in the response to hypoxia and in tumor cellmetabolism. This suggests that activation of upstream signalingcascades may deregulate HMGCR and the MVA pathway. More-over, three different point mutations (generated by mutagenesis)have been shown to disrupt sterol-mediated degradation ofHMGCR and thereby increase its total enzymatic activity (37).
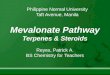
Fig. 4. Dysregulation of the MVA pathway demon-strates the oncogenic potential of HMGCR. (A) Ectopicexpression of either cHMGCR-FL or cHMGCR-D13 intransformed MCF7 cells potentiated anchorage-inde-pendent growth in soft agar. * p < 0.05; one samplet-test compared to normalized control. These experi-ments were performed a minimum of three timesand data representmeans and standard deviations. Re-presentative images of plate quadrants are shown(magnification 1.6×). (B) NontransformedMCF10A cellsformedsignificantlymore colonies in softagarwhenec-topically expressing either cHMGCR-FL or cHMGCR-D13. * p < 0.05; one sample t-test compared to normal-ized control. These experiments were performed aminimum of three times and data represent meansand standard deviations. Representative images ofplate quadrants are shown (magnification 1.6×). (C)cHMGCR-FL and cHMGCR-D13 constructs in MSCV-YFPvectors were introduced into either normal murinebone marrow or fetal liver cells. Cells were plated inmethylcellulose media containing myeloid cytokines.Three independent experiments (two with bone mar-row and one with fetal liver) yielded similar results inwhich cHMGCR-FL increased, and cHMGCR-D13 de-creased,myeloid colony formation. One representativeexperiment is shown; data represent means and stan-dard deviations between duplicate plates. (D) PrimaryMEFs were infected with retroviral constructs carryingthe indicated genes and drug-selected. Transformedfoci formed after approximately three weeks andwerecounted and imaged. Two to four plates of each genecombination were scored and representative imagesare shown.
15054 ∣ www.pnas.org/cgi/doi/10.1073/pnas.0910258107 Clendening et al.

Regardless of the mechanism by which it occurs, our resultsdemonstrate that dysregulation of the MVA pathway can makea causal contribution to cancer etiology.
As our work was in progress, three tissue microarray studiesreported that higher expression of HMGCR correlates withfavorable breast and ovarian cancer patient prognosis (38–40).However, the antibody used in their studies is one that we showedis unable to detect human HMGCR (Fig. S1). Therefore, to as-sess the impact of HMGCR expression on breast cancer patientprognosis in an independent manner, we performed a meta-ana-lysis encompassing 865 patients from six primary patient micro-array datasets that examined mRNA expression in breast cancers(30–35). Interestingly, high HMGCR mRNA levels correlatedwith poor patient prognosis and reduced survival (Fig. 5), sup-porting our cell work. The levels of four out of five additionalMVA pathway genes were also significantly correlated with poorprognosis, suggesting the entire pathway may be dysregulated andcontributing to tumor etiology.
These data are particularly provocative when considered withrecent epidemiological studies that controlled for specific covari-ates and showed the use of certain statins may be associated withdecreased risk of breast cancer (15–18). For example, use oflipophilic statins was associated with lower breast cancer inci-dence in a large group of over 150,000 postmenopausal women(15), and the risk of breast cancer recurrence decreased with in-creasing durations of postdiagnosis statin use (18). These studieslargely show that statin use reduces risk and/or severity of breastcancer and support our own data linking high HMGCR levels andpoor patient prognosis.
Finally, we also provide molecular rationale for the significanttumor-selective therapeutic index observed for statin-inducedapoptosis, arguing for further research toward exploiting the sta-tin family of inhibitors as anticancer agents. Our lab and others’have shown that a subset of tumor cells undergo apoptosis whentreated with physiologically achievable levels of statins (41–44),and we have recently shown that dysregulation of HMGCRand the MVA pathway can predict if multiple myeloma cellsare sensitive to statin-induced apoptosis (44). With a better un-
derstanding of the mechanisms by which HMGCR and the MVApathway are dysregulated, we will be poised to rationally andeffectively combine statins with other anticancer agents to thebenefit of patient care.
Although HMGCR and the MVA pathway have been thesubjects of extensive research, their function and regulation inhuman settings relevant to cancer have, up to now, remained un-known. Here we provide evidence that dysregulation of the MVApathway can promote transformation, suggesting that HMGCR isa candidate oncogene. Ultimately, we have also put HMGCR andthe MVA pathway into the broader context of tumor cell meta-bolism and have shown how they may contribute to the array ofmetabolic changes a normal or precancerous cell undergoes topromote transformation.
Materials and MethodsPlease refer to SI Text for detailed Materials and Methods.
Cell Culture, Vectors, and Reagents. HepG2 cells were cultured in DMEM H21and MCF7 cells in α-MEM; both supplemented with 10% FBS. MCF10A cellswere cultured in DMEM/F12 supplemented with 5% HS, 100 μg∕mL EGF,5 mg∕mL hydrocortisone, 1 mg∕mL cholera toxin, and 10 mg∕mL insulin.Retroviral particles were produced, and target cells infected, as describedpreviously (41). Approximately equal levels of GFP positive cells wereobtained after infection with all viral constructs as determined by flow cyto-metry. In all cases, pools of infected cells were used. To assess proliferation,5 × 103 cells were seeded subconfluently in 12-well plates and counted in tri-plicate wells over 4 d. For cell cycle, 5 × 105 cells were grown subconfluently in100 mm tissue culture plates, harvested, washed in cold PBS, and fixed in cold80% ethanol prior to propidium iodide staining and FACS analysis. Lovastatinpowder was a gift of Apotex Corp. (Mississauga, ON, Canada) and was acti-vated as described previously (43).
Real-Time PCR. Approximately 5 × 105 cells were treated as indicated and har-vested. RNA was extracted using TRIZOL Reagent (Invitrogen, Carlsbad, CA)and cDNAwas synthesized with SuperScript II (Invitrogen). Real-time PCR wasconducted using indicated primers (Table S1) and SYBR Green master mix(Applied Biosystems, Foster City, CA) in triplicate. Expression was determinedrelative to GAPDH.
Fig. 5. High mRNA levelsof MVA pathway genes cor-relate with poor prognosisand reduced survival ofbreast cancer patients. Ameta-analysis of six primarybreast cancer datasets en-compassing 865 patientswas performed to evaluatea relationship betweenpatient prognosis and themRNA expression ofHMGCR, hydroxymethylglu-taryl coenzyme A synthase 1(HMGCS1), mevalonate di-phosphate decarboxylase(MVD), farnesyl pyropho-sphate synthase (FDPS),acetoacetyl-CoA thiolase 2(ACAT2), and mevalonatekinase (MVK). Kaplan–Me-ier analysis demonstratesthat higher mRNA levels offive out of six gene productscorrelates with poor prog-nosis and decreased patientsurvival.
Clendening et al. PNAS ∣ August 24, 2010 ∣ vol. 107 ∣ no. 34 ∣ 15055
BIOCH
EMISTR
Y

Immunoblotting. Approximately 5 × 105 cells were treated as indicated. Cellswere pelleted, washed in cold PBS, lysed, and isolated from precipitatedcellular debris. DTT was added to a final concentration of 1M. 6× Laemmli’sloading dye was added at room temperature and samples were never boiledto limit aggregation of membrane proteins. Blots were probed with anti-HMGCR (Cat. #07-572; Millipore/Upstate, Billerica, MA; 1∶1;000 or Cat.#07-457; Millipore/Upstate; 1∶1;000; refer to Fig. S1 for characterization),antitubulin (Santa Cruz, Santa Cruz, CA; 1∶2;000), or anti-BCL2 (kindly pro-vided by David Andrews, Hamilton, ON, Canada; 1∶2;000).
Colony and Foci Formation Assays. To assess anchorage-independent growth,cells were plated in their respective media + 0.3% noble agar in 30-mm petridishes containing an agar plug. Images were taken and colonies were quan-tified using ImageJ software (NIH, Bethesda, MD). To assess the colony for-mation of murine myeloid cells, hematopoietic progenitor cells (HPCs) wereisolated from the bone marrow, followed by lysis of nonnucleated cells, orfetal liver, enriched for the CD24low population. HPCs were infected twicewith concentrated retroviral supernatant in a prestimulation cocktail andplated in methylcellulose containing myeloid cytokines for 7 d. To assessthe transformation of wild-type MEFs, cells were infected with retroviralparticles three times prior to selection with either puromycin (2 μg/mL) orhygromycin (140 μg/mL) until no more death was observed. After approxi-mately three weeks, plates were washed with PBS twice on ice and fixed withice cold methanol for 10 min on ice. Foci were scored and imaged using aTyphoon 9410 scanner (GE Healthcare, Uppsala, Sweden).
Xenografts. Seven-week-old male SCID mice (Ontario Cancer Institute) weresublethally irradiated (3 GY) and injected subcutaneously with 5 × 106 cellssuspended in 50% matrigel (BD Bioscience) to a final volume of 0.2 mL. Eachmouse was injected with GFP cells in one flank and either ectopic cHMGCR-FLor cHMGCR-D13 cells in the other flank. Resulting tumors were measuredusing digital calipers.
Primary Patient Expression Analysis. A meta-analysis of six breast cancer da-tasets (30–35) was performed, the details of which will be provided elsewhere(Boutros PC et al., in preparation). Briefly, the patients were dichotomizedand a multivariate, meta-analytic Cox proportional hazards model was fit.
ACKNOWLEDGMENTS. The authors would like to thank Dr. Garry Nolan andApoptex Corp. for providing necessary reagents, Christina Bros and AmandaWasylishen for important technical assistance, and all members of the Pennlab for helpful discussions and critical review of the manuscript. This researchwas undertaken, in part, thanks to funding from the Canada Research ChairsProgram (I.J., L.Z.P.), the Ontario Institute for Cancer Research throughfunding provided by the Province of Ontario (L.Z.P.), the Canadian BreastCancer Foundation, Ontario Region, Excellence In Radiation Research forthe 21st Century Strategic Training Initiative In Health Research award fromthe Canadian Institutes for Health Research (J.W.C., P.C.B.), scholarship andfellowship support from the Canadian Institutes for Health Research (A.P.,G.A.T.), a fellowship from the Leukemia and Lymphoma Society of Canada(A.M.), an Ontario Graduate Scholarship (J.W.C.), a Canadian GraduateScholarship from the Natural Sciences and Engineering Research Council(P.C.B.), the Canada Foundation for Innovation (I.J.), a grant from IBM(I.J.), and a grant from CIHR (R.H.).
1. Kroemer G, Pouyssegur J (2008) Tumor cell metabolism: Cancer’s Achilles’ heel. CancerCell 13:472–482.
2. Hanahan D, Weinberg RA (2000) The hallmarks of cancer. Cell 100:57–70.3. Pan JG, Mak TW (2007) Metabolic targeting as an anticancer strategy: dawn of a new
era? Sci STKE 2007:pe14.4. Menendez JA, Decker JP, Lupu R (2005) In support of fatty acid synthase (FAS) as a
metabolic oncogene: Extracellular acidosis acts in an epigenetic fashion activatingFAS gene expression in cancer cells. J Cell Biochem 94:1–4.
5. Morrish F, Neretti N, Sedivy JM, Hockenbery DM (2008) The oncogene c-Myc coordi-nates regulation of metabolic networks to enable rapid cell cycle entry. Cell Cycle7:1054–1066.
6. Dang CV (2010) Rethinking the Warburg effect with Myc micromanaging glutaminemetabolism. Cancer Res 70:859–862.
7. Warburg O, Posener K, Negelein E (1924) Über den Stoffwechsel der Tumoren.Biochem Z 152:319–344.
8. DeBerardinis RJ, Lum JJ, Hatzivassiliou G, Thompson CB (2008) The biology of cancer:Metabolic reprogramming fuels cell growth and proliferation. Cell Metab 7:11–20.
9. Goldstein JL, Brown MS (1990) Regulation of the mevalonate pathway. Nature343:425–430.
10. Endo A (1992) The discovery and development of HMG-CoA reductase inhibitors.J Lipid Res 33:1569–1582.
11. Davidson MH (2001) Safety profiles for the HMG CoA reductase inhibitors: Treatmentand trust. Drugs 61:197–206.
12. Larsson O (1996) HMG-CoA reductase inhibitors: Role in normal and malignant cells.Crit Rev Oncol Hematol 22:197–212.
13. Mo H, Elson CE (2004) Studies of the isoprenoid-mediated inhibition of mevalonatesynthesis applied to cancer chemotherapy and chemoprevention. Exp Biol Med229:567–585.
14. Duncan RE, El-Sohemy A, Archer MC (2004) Mevalonate promotes the growth oftumors derived from human cancer cells in vivo and stimulates proliferation in vitrowith enhanced cyclin-dependent kinase-2 activity. J Biol Chem 279:33079–33084.
15. Cauley JA, et al. (2006) Statin use and breast cancer: Prospective results from theWomen’s Health Initiative. J Natl Cancer Inst 98:700–707.
16. Kumar AS, et al. (2008) Estrogen receptor-negative breast cancer is less likely to ariseamong lipophilic statin users. Cancer Epidem Biomar 17:1028–1033.
17. Kochhar R, Khurana V, Bejjanki H, Caldito G, Fort C (2005) Statins reduce breast cancerrisk: a case control study in US female veterans. J Clin Oncol 23:514.
18. Kwan ML, Habel LA, Flick ED, Quesenberry CP, Caan B (2008) Post-diagnosis statin useand breast cancer recurrence in a prospective cohort study of early stage breast cancersurvivors. Breast Cancer Res Treat 109:573–579.
19. Solomon KR, Freeman MR (2008) Do the cholesterol-lowering properties of statinsaffect cancer risk? Trends Endocrinol Metab 19:113–121.
20. Karp I, Behlouli H, Lelorier J, Pilote L (2008) Statins and cancer risk. Am J Med121:302–309.
21. Lipkin SM, et al. (2010) Genetic variation in 3-hydroxy-3-methylglutaryl CoA reductasemodifies the chemopreventive activity of statins for colorectal cancer. Cancer Prev Res3:597–603.
22. Hirsch HA, et al. (2010) A transcriptional signature and common gene networks linkcancer with lipid metabolism and diverse human diseases. Cancer Cell 17:348–361.
23. Johnson JM, et al. (2003) Genome-wide survey of human alternative pre-mRNAsplicing with exon junction microarrays. Science 302:2141–2144.
24. Burkhardt R, et al. (2008) Common SNPs in HMGCR in micronesians and whitesassociated with LDL-cholesterol levels affect alternative splicing of exon13. Arterios-cler Thromb Vasc Biol 28:2078–2084.
25. Medina MW, Gao F, Ruan W, Rotter JI, Krauss RM (2008) Alternative splicing of 3-hy-droxy-3-methylglutaryl coenzyme A reductase is associated with plasma low-densitylipoprotein cholesterol response to simvastatin. Circulation 118:355–362.
26. Medina MW, Krauss RM (2009) The role of HMGCR alternative splicing in statinefficacy. Trends Cardiovas Med 19:173–177.
27. Molowa DT, Cimis GM (1989) Co-ordinate regulation of low-density-lipoprotein recep-tor and 3-hydroxy-3-methylglutaryl-CoA reductase and synthase gene expression inHepG2 cells. Biochem J 260:731–736.
28. Clerc T, et al. (1996) Differences in hypolipidaemic effects of two statins on Hep G2 cellsor human hepatocytes in primary culture. Br J Pharmacol 118:1862–1868.
29. DeBose-Boyd RA (2008) Feedback regulation of cholesterol synthesis: Sterol-acceler-ated ubiquitination and degradation of HMG CoA reductase. Cell Res 18:609–621.
30. Pawitan Y, et al. (2005) Gene expression profiling spares early breast cancer patientsfrom adjuvant therapy: Derived and validated in two population-based cohorts. BreastCancer Res 7:R953–964.
31. Bild AH, et al. (2006) Oncogenic pathway signatures in human cancers as a guide totargeted therapies. Nature 439:353–357.
32. Desmedt C, et al. (2007) Strong time dependence of the 76-gene prognostic signaturefor node-negative breast cancer patients in the TRANSBIG multicenter independentvalidation series. Clin Cancer Res 13:3207–3214.
33. Loi S, et al. (2008) Predicting prognosis using molecular profiling in estrogen receptor-positive breast cancer treated with tamoxifen. BMC Genomics 9:239.
34. Miller LD, et al. (2005) An expression signature for p53 status in human breast cancerpredicts mutation status, transcriptional effects, and patient survival. Proc Natl AcadSci USA 102:13550–13555.
35. Sotiriou C, et al. (2006) Gene expression profiling in breast cancer: Understandingthe molecular basis of histologic grade to improve prognosis. J Natl Cancer Inst98:262–272.
36. Pallottini V, et al. (2008) Regulation of HMG-CoA reductase expression by hypoxia.J Cell Biochem 104:701–709.
37. Lee PC, Nguyen AD, Debose-Boyd RA (2007) Mutations within the membrane domainof HMG-CoA reductase confer resistance to sterol-accelerated degradation. J Lipid Res48:318–327.
38. Borgquist S, et al. (2008) Prognostic impact of tumour-specific HMG-CoA reductaseexpression in primary breast cancer. Breast Cancer Res 10:R79.
39. Borgquist S, et al. (2008) HMG-CoA reductase expression in breast cancer is associatedwith a less aggressive phenotype and influenced by anthropometric factors. Int J Can-cer 123:1146–1153.
40. Brennan DJ, et al. (2010) Tumour-specific HMG-CoAR is an independent predictor ofrecurrence free survival in epithelial ovarian cancer. BMC Cancer 10:125.
41. Wong WW, et al. (2007) Determinants of sensitivity to lovastatin-induced apoptosis inmultiple myeloma. Mol Cancer Ther 6:1886–1897.
42. Newman A, Clutterbuck RD, Powles RL, Catovsky D, Millar JL (1997) A comparisonof the effect of the 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductaseinhibitors simvastatin, lovastatin and pravastatin on leukaemic and normal bonemarrow progenitors. Leukemia Lymphoma 24:533–537.
43. Dimitroulakos J, et al. (1999) Increased sensitivity of acute myeloid leukemias tolovastatin-induced apoptosis: A potential therapeutic approach. Blood 93:1308–1318.
44. Clendening JW, et al. (2010) Exploiting the mevalonate pathway to distinguishstatin-sensitive multiple myeloma. Blood 115:4787–4797.
15056 ∣ www.pnas.org/cgi/doi/10.1073/pnas.0910258107 Clendening et al.