Embed Size (px)
Citation preview
Dysplas'c Barre-’s Esophagus: Cut, Burn, Freeze or Watch Very Very Closely
Felice Schnoll-‐Sussman, MD, FACG Director, Jay Monahan Center
Associate Professor Clinical Medicine Weill Cornell Medical Center
We just want to do the right thing but…
• Only 7% of the 10,000 EC dx in USA are iden'fied by screening or surveillance
• 40% of people with EC do not have reflux • 90% of people with EC did not know they had Barre-’s
• Screening and surveillance of BE have not been proven to prevent deaths
• Fatal cases nearly as likely to have received surveillance (55.3%) as were controls (60.4%)
Nature Reviews Gastro & Hep 2015; 12;243 Gastro 2013;142:312
Before you treat it, you must find it
Surveillance must be done me'culously and systema'cally • BE early dysplasia oeen presents as subtle flat Paris type II-‐b
• Direct correla'on between 'me inspec'ng each cm of BE and neoplasia detec'on
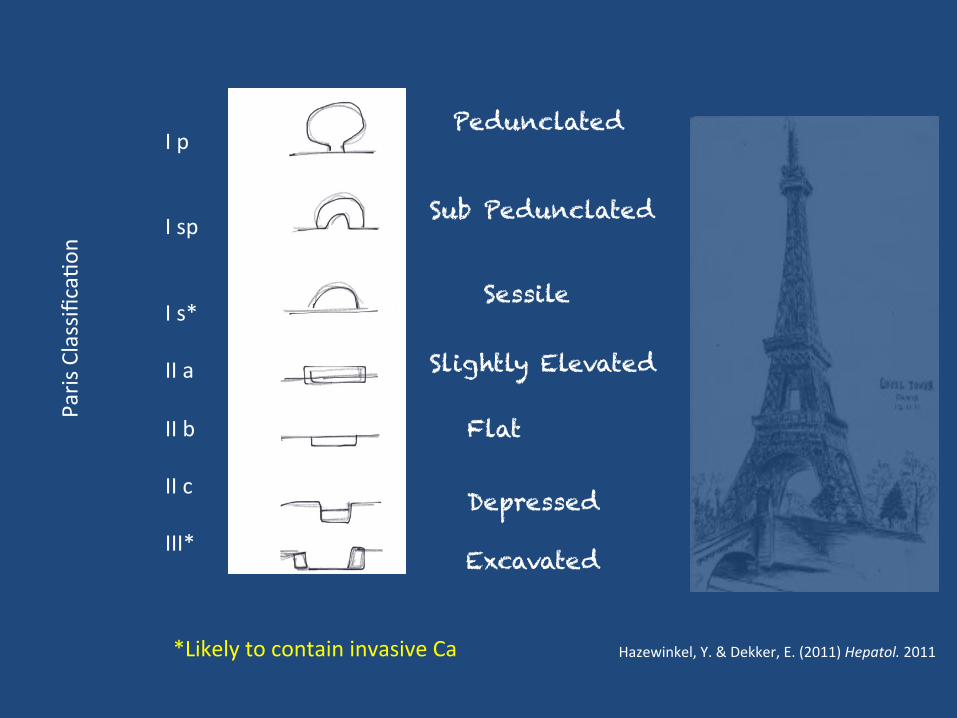
Hazewinkel, Y. & Dekker, E. (2011) Hepatol. 2011 *Likely to contain invasive Ca
Pedunclated
Sub Pedunclated
Sessile
Slightly Elevated
Flat
Depressed
Excavated
I p I sp I s* II a II b II c III*
Paris Classifica'o
n
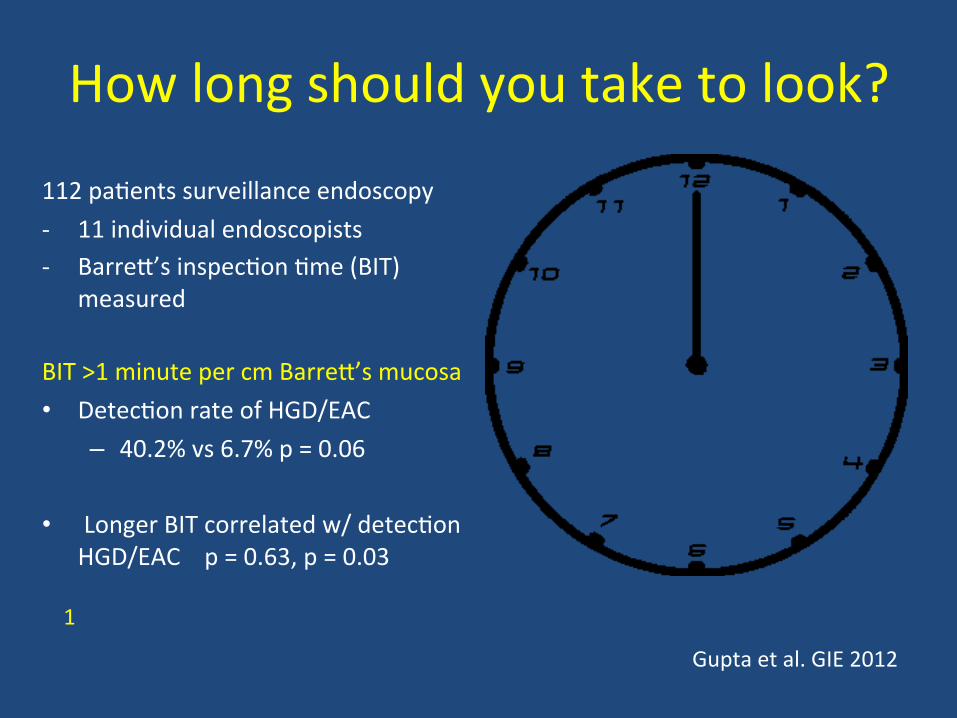
How long should you take to look?
112 pa'ents surveillance endoscopy -‐ 11 individual endoscopists -‐ Barre-’s inspec'on 'me (BIT)
measured
BIT >1 minute per cm Barre-’s mucosa • Detec'on rate of HGD/EAC
– 40.2% vs 6.7% p = 0.06
• Longer BIT correlated w/ detec'on HGD/EAC p = 0.63, p = 0.03
1
Gupta et al. GIE 2012
What should we be repor'ng?
Repor'ng should include: 1. Barre-' segment length – Prague Criteria 2. Document presence and size of hiatal hernia 3. Document presence of esophagi's above BE
segment
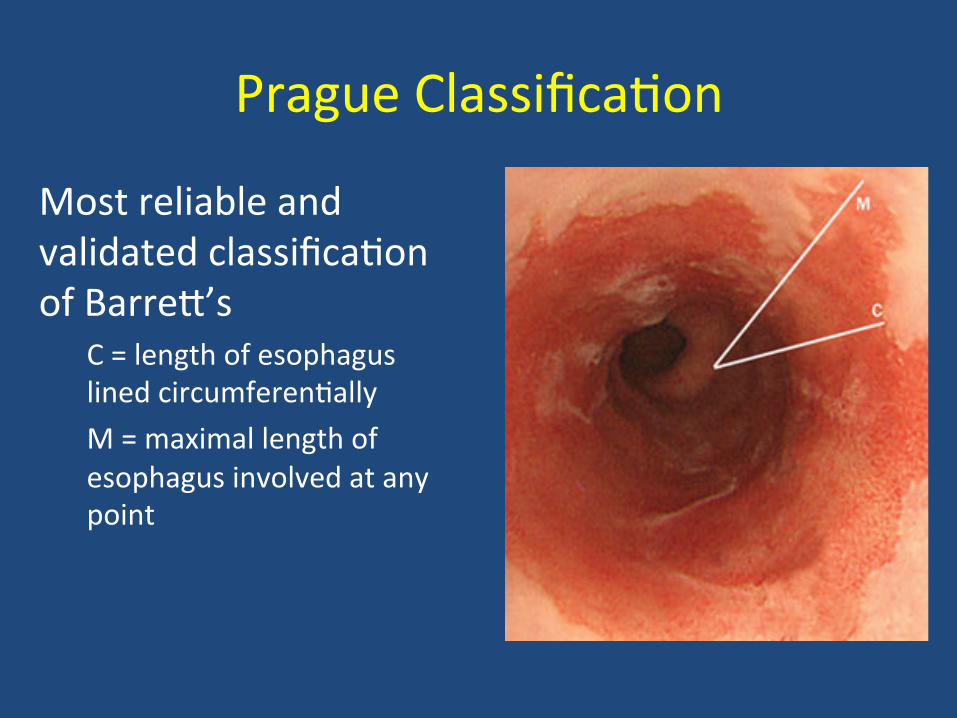
Prague Classifica'on
Most reliable and validated classifica'on of Barre-’s
C = length of esophagus lined circumferen'ally M = maximal length of esophagus involved at any point
History of an endoscopist’s ‘view’ of Barre-’s Esophagus
• 2001-‐2010 – regular light, bx, bx, bx, bx • 2009 – High defini'on white light…bx, bx, bx, bx • 2011 – HDWL + NBI+ EMR…bx,bx,bx • 2012 – HDWL +NBI +EMR + pCLE + WATS...bx,bx • 2013 – HDWL + EMR + pCLE + OCT + WATS…bx
“Look longer...look be-er…(maybe) biopsy less”
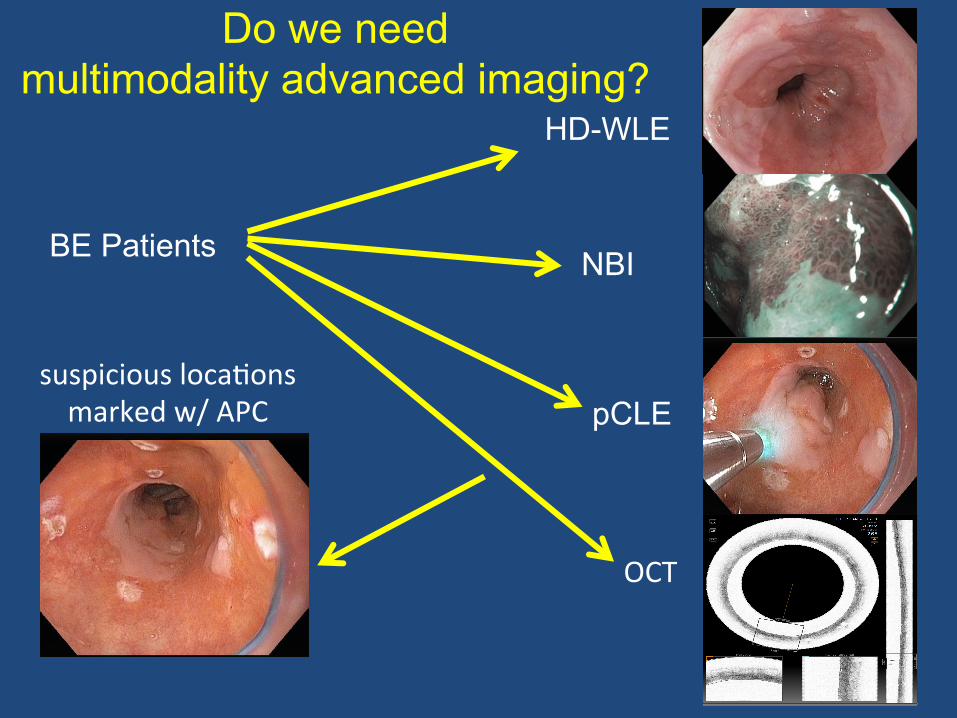
BE Patients
HD-WLE
NBI
suspicious loca'ons marked w/ APC
Do we need multimodality advanced imaging?
pCLE
OCT
Do we need mul'modality imaging?
• HR-‐WLE is 2-‐5 fold superior quality than SD-‐WLE – Expert opinion: HR-‐ WLE minimum standard
• HR + dye-‐based (ace'c,indigo carmine, methylene blue) – Time consuming, tedious, need high-‐magnifica'on – Limited added benefit to HR-‐WLE alone
• Op'cal chromoendoscopy (NBI, FICE, I-‐Scan) – NBI w/target bx = detec'on rate IM vs. HR w/standard bx – NBI detects higher propor'on dysplasia (30% vs 21%, P=.01) – Requires fewer biopsies (3.6 vd 7.6 p<.0001) – Useful as adjunc've tool to HR-‐WLE
Benne- C. Gastro 2012;143:336-‐46 (Delphi Process) Sharma P Gut 2013:62:15-‐21
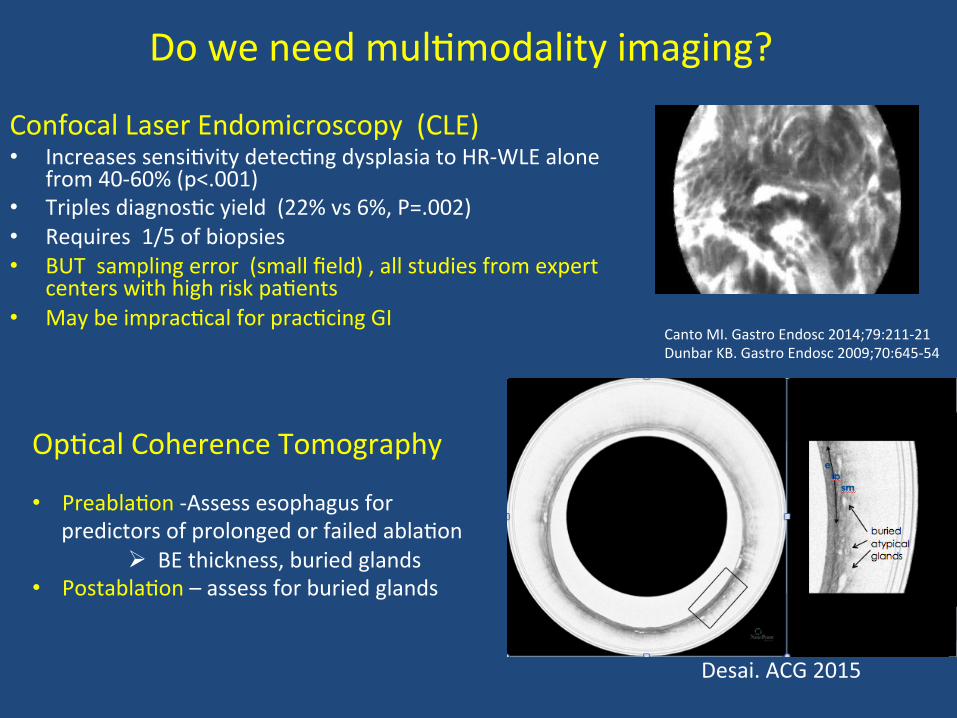
Do we need mul'modality imaging?
Confocal Laser Endomicroscopy (CLE) • Increases sensi'vity detec'ng dysplasia to HR-‐WLE alone
from 40-‐60% (p<.001) • Triples diagnos'c yield (22% vs 6%, P=.002) • Requires 1/5 of biopsies • BUT sampling error (small field) , all studies from expert
centers with high risk pa'ents • May be imprac'cal for prac'cing GI
Op'cal Coherence Tomography
Canto MI. Gastro Endosc 2014;79:211-‐21 Dunbar KB. Gastro Endosc 2009;70:645-‐54
• Preabla'on -‐Assess esophagus for predictors of prolonged or failed abla'on
Ø BE thickness, buried glands • Postabla'on – assess for buried glands
Desai. ACG 2015
What is the Best Biopsy Protocol? 1. Erosive esophagi's should be healed before
biopsy – Inflamma'on causes cytologic atypia in crypts; mimics dysplasia
2. Four quadrant biopsy every 1-‐ 2 cm (Sea-le) – Each segment submi-ed in separate containers
3. Samples from any visible abnormali'es (nodules or suspicious areas )
4. Wide angle transepithelial sampling (WATS3D) The Sad Truth: Biopsy guidelines followed in only 51.2% of pa'ents in community sexng
• Na'onal pathology database of 2200 surveillance cases Abrams. Clin Gastro Hep 2009;7(7);736
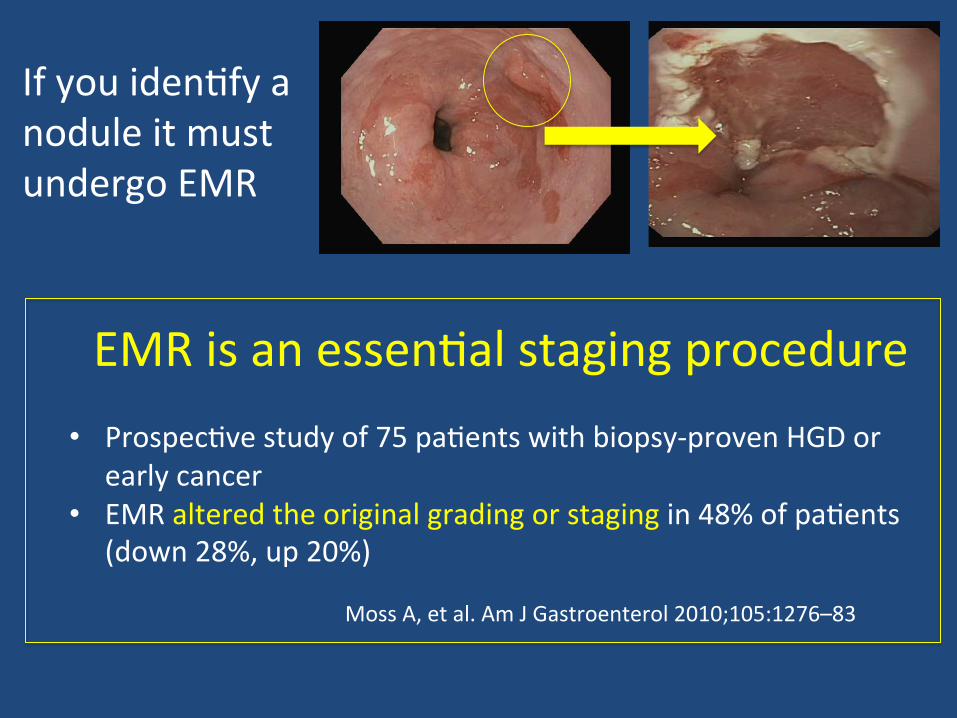
If you iden'fy a nodule it must undergo EMR
EMR is an essen'al staging procedure • Prospec've study of 75 pa'ents with biopsy-‐proven HGD or
early cancer • EMR altered the original grading or staging in 48% of pa'ents
(down 28%, up 20%) Moss A, et al. Am J Gastroenterol 2010;105:1276–83
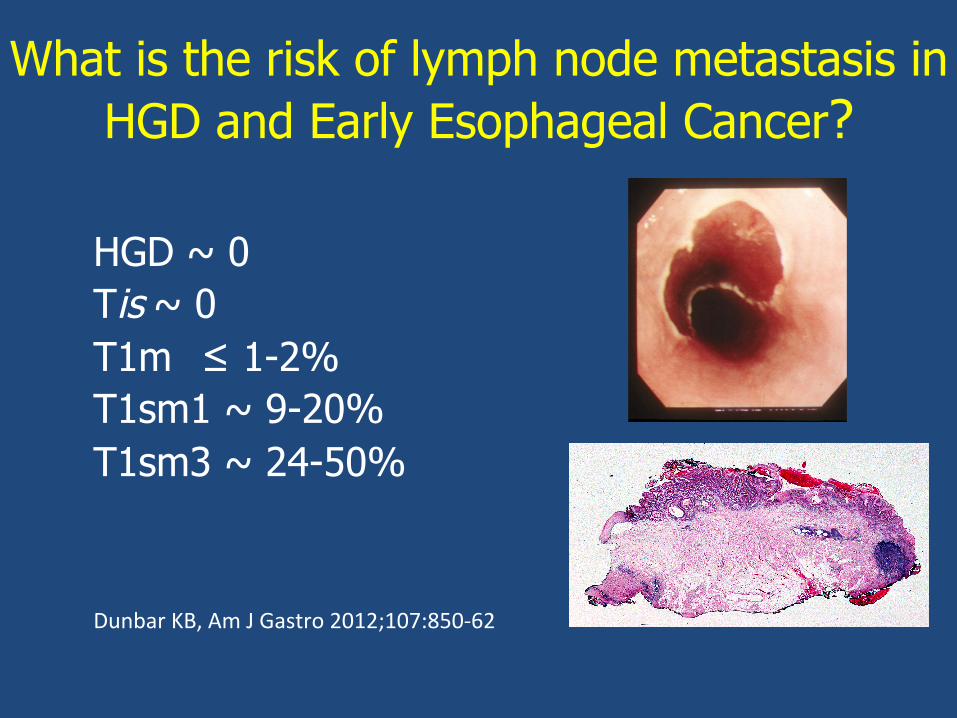
What is the risk of lymph node metastasis in HGD and Early Esophageal Cancer?
• HGD ~ 0 • Tis ~ 0 • T1m ≤ 1-2% • T1sm1 ~ 9-20% • T1sm3 ~ 24-50%
• Dunbar KB, Am J Gastro 2012;107:850-‐62
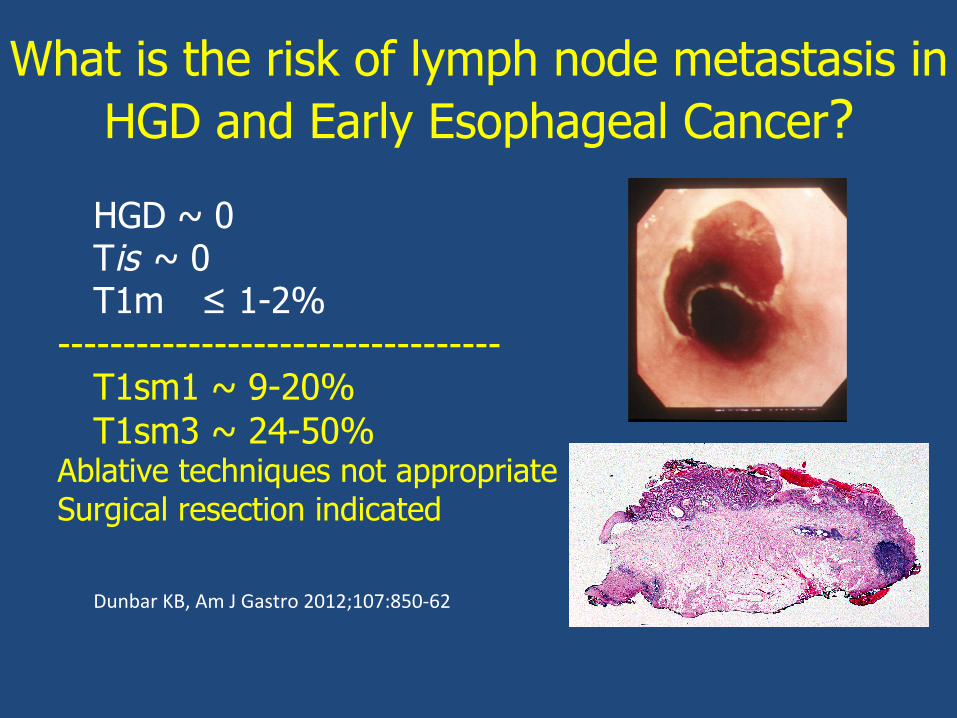
What is the risk of lymph node metastasis in HGD and Early Esophageal Cancer?
• HGD ~ 0 • Tis ~ 0 • T1m ≤ 1-2% ---------------------------------- • T1sm1 ~ 9-20% • T1sm3 ~ 24-50% Ablative techniques not appropriate Surgical resection indicated
• Dunbar KB, Am J Gastro 2012;107:850-‐62
The Barre-’s Dysplasia Paradox
Accurate diagnosis and staging is essen'al
Interobserver agreement among expert pathologists can be less than 50%
What Really is Low-‐Grade Dysplasia?
• 147 subjects with a diagnosis of LGD made in a community prac'ce in the Netherlands
• Path reviewed by 2 expert pathologists – Disagreements resolved by consensus
• 85% of cases were down-‐graded • In remaining 15%: incidence rate of HGD or EAC was 13.4%/pt-‐yr (mean f/u: 51 mo)
Curvers WL et al. Am J Gastroenterol 2010
Is EUS Necessary in Staging?
Virtually no risk of LN metastasis in HGD 1-‐2% risk in ImCa Factors that predict risk of LN metastasis
1) Depth of tumor invasion (sm1 and deeper) 2) Tumor diameter > 3 cm 3) Lymph vascular invasion on ER specimen 4) Degree of differen'a'on (poorly or G3 tumor biology) Consider EUS in conjunc'on with EMR if concern for LNs or tumor has high risk features
Dunbar KB, Am J Gastro 2012;107:850-‐62
Pardigm Shie in BE Treatment
Those who treat pa'ents with Barre-’s must think of themselves not only as gastroenterologists but as:
“Gastro-‐oncologicalsurgeons”
Accurate staging = Appropriate treatment
Now that you have… detected dysplasia and staged it correctly
what should you do?
1. EMR resec'on of all nodular disease -‐ Diagnos'c and therapeu'c
2. Ablate all remaining Barre-’s mucosa 3. Control acid 4. Lifelong surveillance
Endoscopic Eradica'on Therapies
A. Endoscopic resec'on 1. EMR – focal or complete 2. ESD
B. Endoscopic abla'on 1. Radiofrequency abla'on 2. Cryotherapy 3. Photodynamic therapy 4. Argon plasma coagula'on
Endoscopic Eradica'on Therapies
A. Endoscopic resec'on 1. EMR – focal or complete 2. ESD
B. Endoscopic abla'on 1. Radiofrequency abla'on 2. Cryotherapy 3. Photodynamic therapy 4. Argon plasma coagula'on
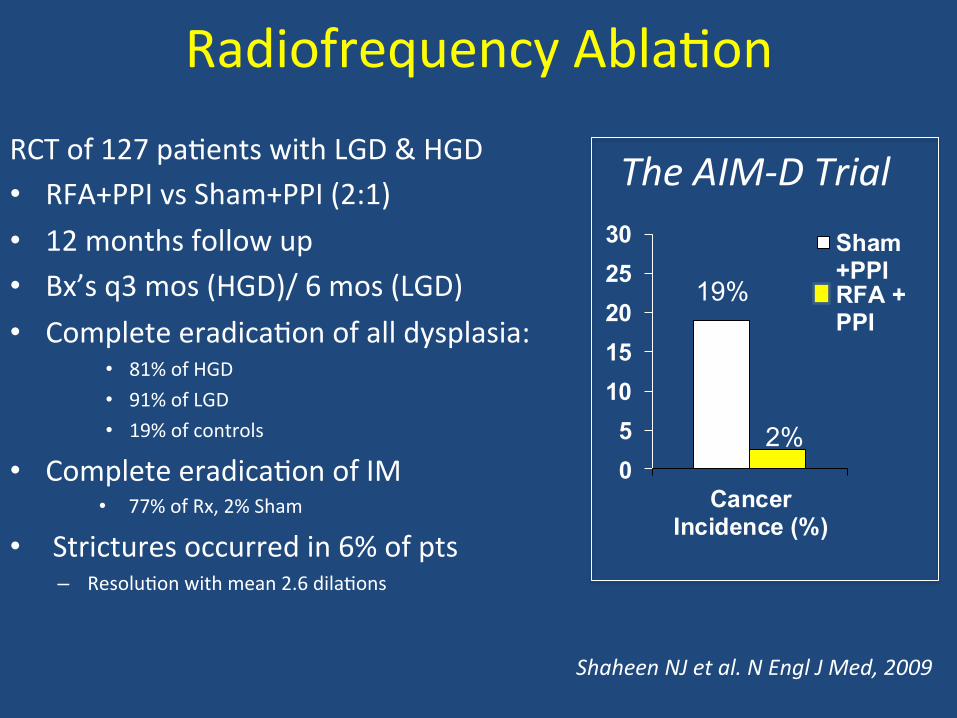
Radiofrequency Abla'on RCT of 127 pa'ents with LGD & HGD • RFA+PPI vs Sham+PPI (2:1) • 12 months follow up • Bx’s q3 mos (HGD)/ 6 mos (LGD) • Complete eradica'on of all dysplasia:
• 81% of HGD • 91% of LGD • 19% of controls
• Complete eradica'on of IM • 77% of Rx, 2% Sham
• Strictures occurred in 6% of pts – Resolu'on with mean 2.6 dila'ons
05
1015202530
CancerIncidence (%)
Sham+PPIRFA +PPI
Shaheen NJ et al. N Engl J Med, 2009
The AIM-‐D Trial
19%
2%
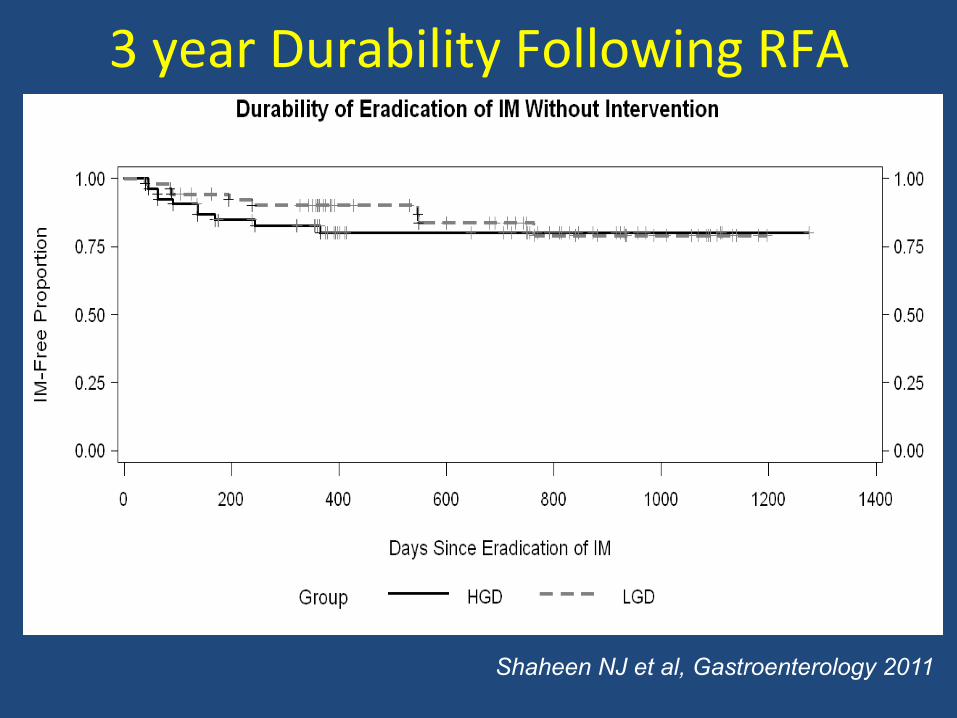
3 year Durability Following RFA
Shaheen NJ et al, Gastroenterology 2011
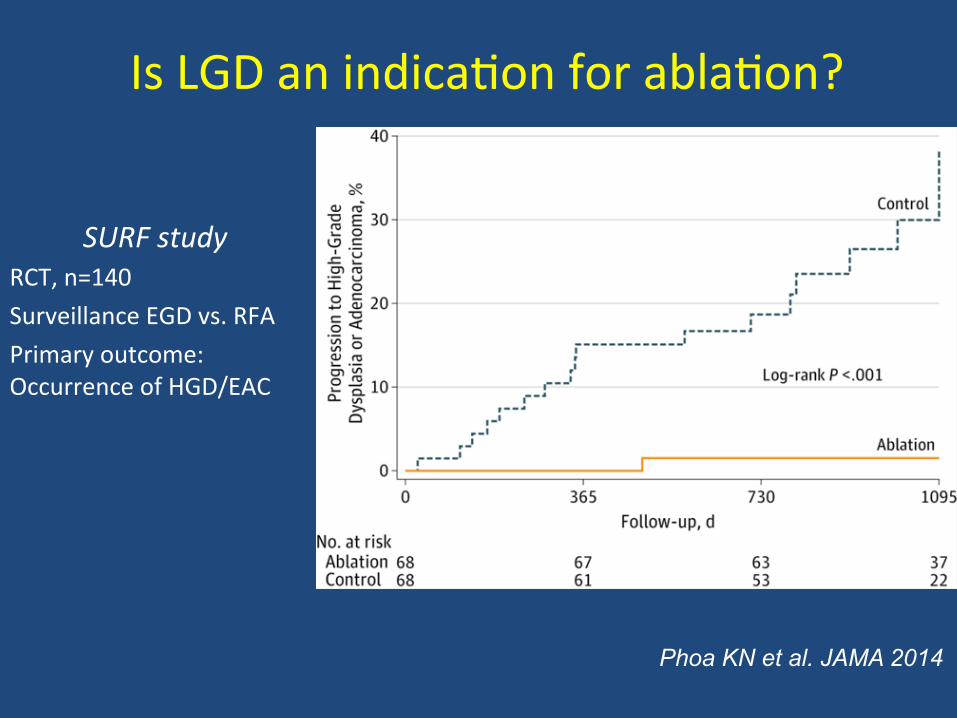
Is LGD an indica'on for abla'on?
SURF study RCT, n=140 Surveillance EGD vs. RFA Primary outcome: Occurrence of HGD/EAC
Phoa KN et al. JAMA 2014
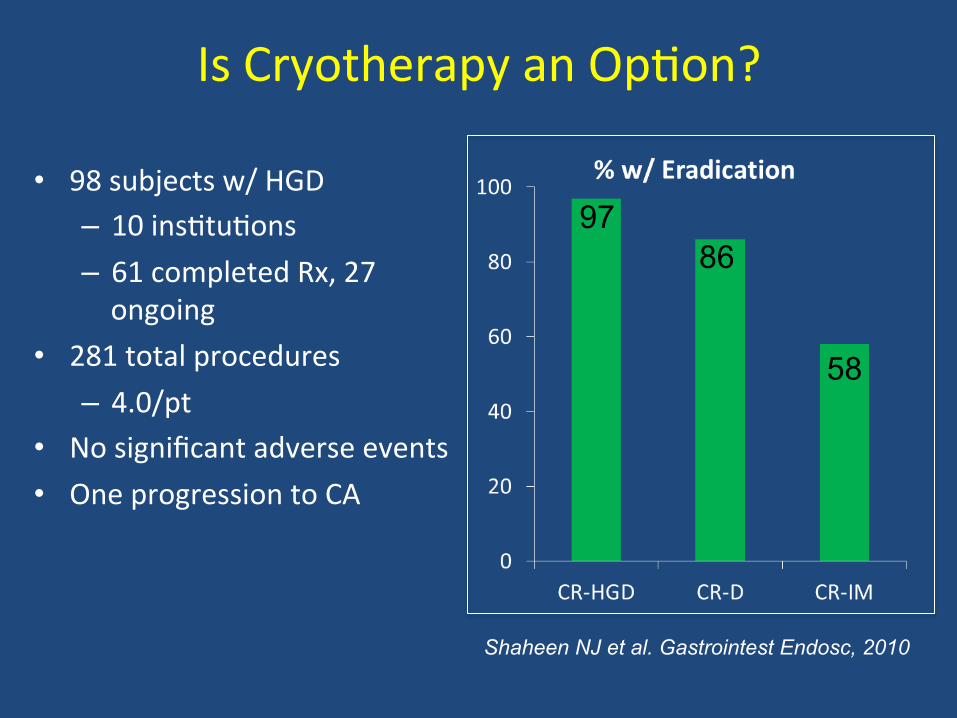
Is Cryotherapy an Op'on?
• 98 subjects w/ HGD – 10 ins'tu'ons – 61 completed Rx, 27 ongoing
• 281 total procedures – 4.0/pt
• No significant adverse events • One progression to CA
97 86
58
Shaheen NJ et al. Gastrointest Endosc, 2010
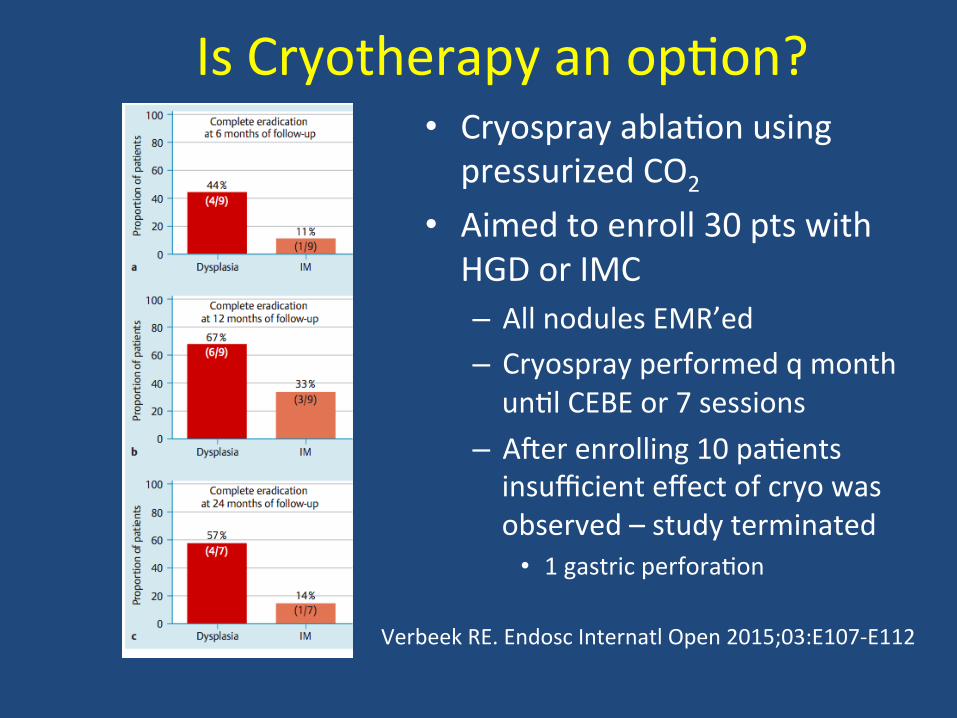
Is Cryotherapy an op'on? • Cryospray abla'on using pressurized CO2
• Aimed to enroll 30 pts with HGD or IMC – All nodules EMR’ed – Cryospray performed q month un'l CEBE or 7 sessions
– Aeer enrolling 10 pa'ents insufficient effect of cryo was observed – study terminated
• 1 gastric perfora'on
Verbeek RE. Endosc Internatl Open 2015;03:E107-‐E112
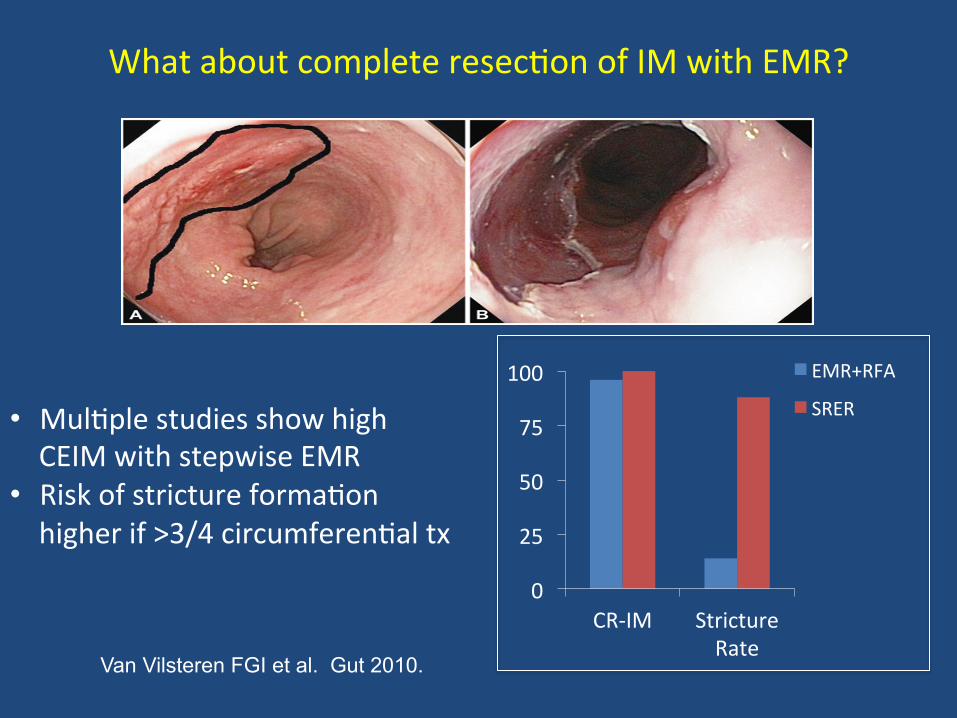
0
25
50
75
100
CR-‐IM Stricture Rate
EMR+RFA
SRER
Van Vilsteren FGI et al. Gut 2010.
• Mul'ple studies show high CEIM with stepwise EMR
• Risk of stricture forma'on higher if >3/4 circumferen'al tx
What about complete resec'on of IM with EMR?
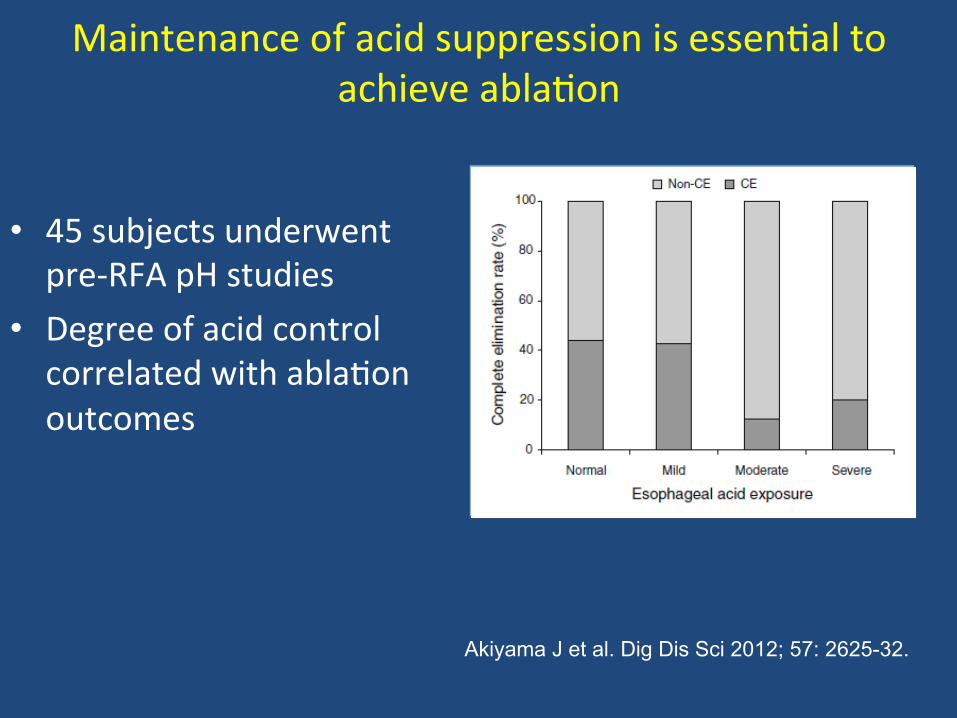
Maintenance of acid suppression is essen'al to achieve abla'on
• 45 subjects underwent pre-‐RFA pH studies
• Degree of acid control correlated with abla'on outcomes
Akiyama J et al. Dig Dis Sci 2012; 57: 2625-32.
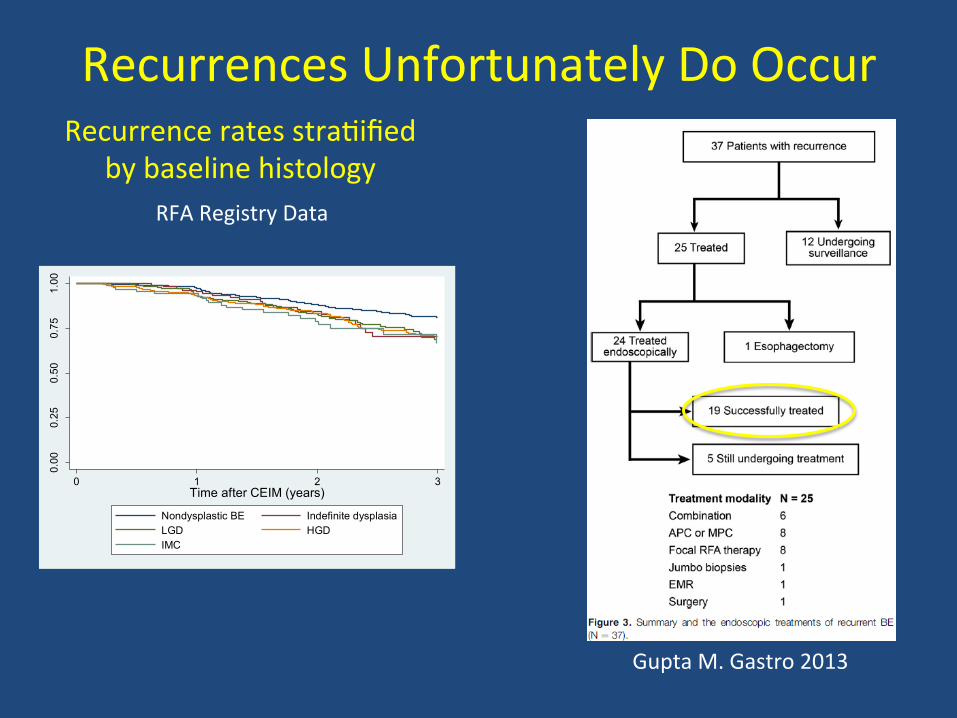
Recurrences Unfortunately Do Occur 0.
000.
250.
500.
751.
00
0 1 2 3Time after CEIM (years)
Nondysplastic BE Indefinite dysplasiaLGD HGDIMC
Recurrence rates stra'ified by baseline histology
RFA Registry Data
Gupta M. Gastro 2013
�
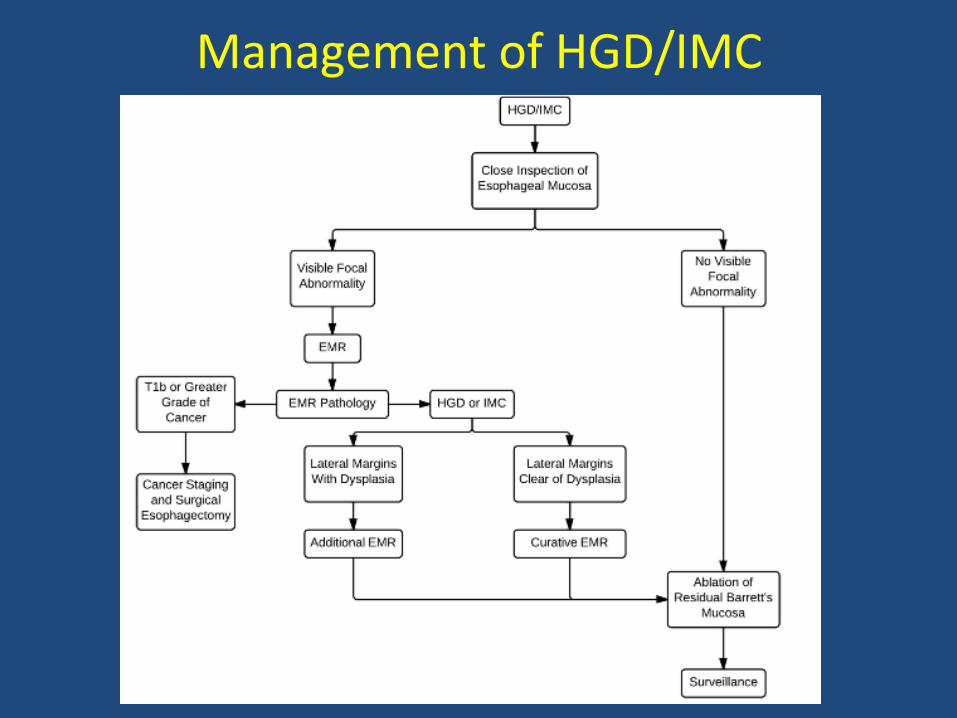
Management of HGD/IMC
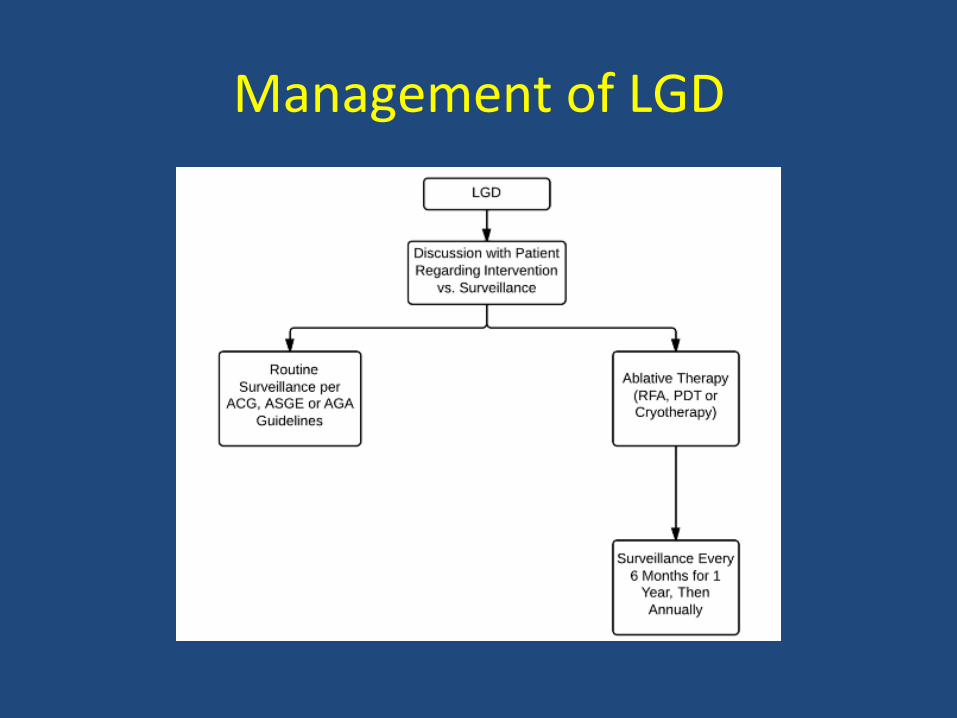
Management of LGD
What have we learned?
• High quality EGD essen'al to correctly stage • Mul'modality advanced imaging helpful but may not be essen'al
• Endoscopic management of low and high grade dysplas'c BE is effec've
• Endotherapy with mul'modality approach, combining 'ssue-‐acquiring and abla've techniques
• Following eradica'on, surveillance and acid suppression must con'nue
• Recurrence can be managed endoscopically









![SIDEROPHILE ELEMENT ABUNDANCES IN KARAVANNOE: … · 2014. 4. 1. · that of CV metal (20.4, [5]). Because the bulk ICP data of [6] are systemacally lower in compable elements and](https://img.pdfslide.us/doc/110x75/5fc2a2066c22a174c05b9617/siderophile-element-abundances-in-karavannoe-2014-4-1-that-of-cv-metal-204.jpg)



















