Embed Size (px)
Citation preview

Gut, 1983, 24, 193-201
Dysfunction of the continent ileostomy: clinical featuresand bacteriology*DARLENE G KELLY, S F PHILLIPS. K A KELLY,W M WEINSTEIN, AND MARY J R GILCHRIST
From the Gastroenterology Unit and Department of Laboratorv Medicine, Mayo Clinic and MayoFoundation, Rochester, Minnesota, and the Departmlent of Medicine, University of California, Los Angeles,California, USA
SUMMARY The pathogenesis and treatment of dysfunction of the continent ileostomy was
investigated in 12 patients, five of whom had asymptomatic malabsorption and seven of whomhad acute complaints. The number of anaerobic bacteria in jejunal aspirates was increased inpatients with pouch malfunction (range 103 to 108/g aspirate), but the microbiology of ilealeffluent and the morphology of the ileal mucosa could not be correlated with dysfunction. Bileacid breath tests and lactose tolerance tests were not, however, reliable indicators of jejunalbacterial overgrowth. The symptoms, the malabsorption, and the number of jejunal and ilealanaerobic bacteria decreased in patients during treatment with metronidazole, implicatingovergrowth of anaerobic bacterial flora in the pathogenesis of the syndrome.
The continent ileostomy (ileal pouch), devised byKock,' has been used as an alternative to con-ventional ileostomy for selected patients withulcerative colitis and familial polyposis.2-5 Thereservoir functions satisfactorily in most patients,but malfunction of the 'nipple valve' may occur in upto a third of patients and lead to incontinence.Improved surgical techniques appear, however, tohave decreased the incidence of valvulardysfunction ;2 5 furthermore, better selection ofpatients should decrease the need for revision ofprolapsed valves.6 Because Crohn's disease mayrecur after construction of a pouch,2 5 we believethat this diagnosis is a contraindication to theoperation.2 5 TMore recently other syndromes of ileostomy
dysfunction have been reported. These are
described variably as: 'stafnant loop syndrome',9'enteritis' ,7 'pouchitis', " and 'non-specificileitis'. 5 "I The corresponding clinical features mayinclude diarrhoea,5 l0l2 malabsorption of fat and
* Supported in part by grants from the National Foundation for lleitis andColitis. and the National Institutes of Health. Bethesda. Maryland (AM 69(08.AM 2(06(15. AM (16342-Il1. RR 585). A preliminary report of this work was
presented at the American Gastroenterological Association annual meeting.May 198(1.Address for correspondence: Dr S F Phillips. Gastroenterology Unit. MayoClinic. Rochester. MN 559(05. USA.
Received for publication 2(0 August 1982
vitamin B12,9 12 proliferation of anaerobic bacteriain the pouch,9 inflammation in the pouch,7incontinence,"' difficulty with intubation,1' andbloody discharge.5 We previously reporteddiarrhoea with some features of malabsorption inapproximately one-third of asymptomatic patientswith continent ileostomies. 12 Here, we extend thesestudies to include patients with symptoms ofileostomy dysfunction; we also examined thepossible mechanisms for dysfunction and thesymptomatic response to metronidazole.
Methods
PATIENTS WITH POUCH DYSFUNCTION (Table 1)These patients were selected on the basis of docu-mented malabsorption and/or symptoms of amalfunctioning pouch. Five subjects (nos 1-5) withdiarrhoea and malabsorption had been identifiedearlier. 12 Their pouches were 'mature' (32-51months postoperative, mean 40 months). Onrestudy, these five still had excess outputs of volume(>1000 g/day) and/or fat (Table 1). Seven patients(nos 6-12) had symptoms of dysfunction of thepouch (Table 1); these included bleeding from thepouch, diarrhoea, peristomal discomfort, minorleakage, and difficulties with intubation. In five, theonset of symptoms was during the first year after
193
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

194 Kelly, Phillips, Kelly, Weinstein, and Gilchrist
Table 1 C'linic(allfatures of pantient.s with ileostomrv dvsflulntioino
Schilling tie.vt$After lleuomn Faecal wit/i intrinsic
Age operatiotn resected wveight IieI' t fiictorPatienti (vr) Sex (montls) (cm) (g/24 hi ('/,241i('I in uirinte) SSymptomns
I 61) F 51 22 898 23 6 Bone pain; otherwise asymptomatic2 39 F 35 14 1508 20 9 Asymptomatic3* 48 M 36 70 1785 10 12 Asymptomaitic4 33 M 35 8 994 15 32 Asymptomiatic5 72 M 50 6 763 11 6 Asymptomatic6 24 F 32 4 905 5 18 Blceding from pouch. RLQ pain7* 32 F 33 1(-2() 1166 6 12 Difficult intuhation. pouch pain8 18 F 8 10)32 4 2 Bleeding from pouch. RLQ paiin9* 19 F 9 5 1052 9 12 Nausea. diarrhoea. abdominal craimps10 21 M 8 3 1485 11 26 Difficult intubation. pouch pain. diarrhoea11* 35 F 6 <10 1332 5 24 Bleeding from pouch. cramps. diarrhoea12 46 F 1 4 856 8 3 Nausea. diarrhoea. RLQ pain
Secondary conversion of Brooke ilcostomy.t Expressed as pcrcentage dietary intake, approximate fait was l (N) g/day. Upper limit of normal. 7'ih.t Normal >9%.
operation (range, one to nine months; mean, five ileostomies constructed 2() to 58 months (mean, 38months). Two were studied 32 and 33 months after months) previously.operation. All patients in the study had proctocolectomies
performed for chronic ulcerative colitis. All gaveCONTROL PATIENTS (Table 2) written, informed consent for the protocol that hadIn five patients (nos 13-17) with continent been approved by the Human Studies Committee ofileostomies, we had documented in a previous Mayo Clinic. The patients were hospitalised in thestudy12 normal pouch effluents (weight <1000 g/24 h Clinical Research Center. They were given constantand faecal fat <7 gl24 h), both of which were diets of known composition, designed to be similarconfirmed. These subjects had had their pouches for to the usual dietary pattern at home, and including35 to 63 months (mean, 50 months). A second 100 g fat. None was taking medication. One patientcontrol group (Table 2) consisted of eight patients (no. 4), who was taking salicylazosulphapyridine,(nos 18-25) who had conventional (Brooke) discontinued the drug two weeks before the study.
Table 2 Clinicalfeatures ofpatients in control groups
Schilling te.sttwith intrinsic
Age After operation lleum resected Faecal weight Faecalfat* factorPatient (yr) Sex (months) (cm) (g/24 h) (Cc/24 h) (Mc in urine)
lleal pouch - normal function13 38 F 51 1() 743 4 1614 27 F 61 2 267 1 3615 28 F 63 0 546 4 1616 51 F 35 7 453 2 2317 43 F 40 4 543 3 17
Conventional ileostomy18 72 M 58 38 1073 5 2419 52 M 31 6 629 4 2120 20 M 30 17 613 2 2721 25 F 54 3 355 3 2322 50 M 20 8 603 2 1623 35 M 22 30 958 3 3124 49 M 36 5 719 2 1725 37 M 55 6 424 2 24
* Expressed as percentage dietary intake excreted per day; approximate dietary fat was 100 g/day. Upper limit of normal. 7%.t Normal >9%.
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

Di.stu, ( tiott ofc(oltinlelt ileostootin1
STUDIES OF II.EOSTOMY EFFILUENT
lleostomy effluent was collected for 48 hours, andthe weight of the specimen was recorded. Allspecimens were frozen immediatelv upon collectionand thawed only for homogenisation andpreparation of aliquots, which were processedwithout delay. The fat content of effluents was
determined by the method of van de Kamer' 3and an
output of <7% of the daily fat intake was con-
sidered normal.
VITAMIN B12 ABSORPTION TEST
Standard Schilling tests were performed by simul-taneous jngestion of 0(25 ,ug cyanocobalamin con-
taining 0O8 MCi '8Co cyanocobalamin and of 0.25 1ugcyanocobalamin containing 0.5 ,Ci 57Co cyano-cobalamin bound to human gastric juice (AmershamCorporation Dicopac Kit). A loading dose of 1 mgunlabelled vitamin B12 was given intramuscularly 1,to two hours after the oral dose. Urinary excretionof >9%/24 h of each isotope was taken as normal.
JEJUNAL BIOPSIESJejunal biopsies were obtained from the region ofthe ligament of Treitz with the Quinton Multi-purpose Biopsy Tube. Biopsies were oriented, fixedin modified Bouin's fixative (1% glacial acetic acid),and processed for light microscopy (haematoxylinand eosin) as previously described. '4 Jejunalhistology was evaluated by one of us (WMW)without previous knowledge of the clinical featuresof the patients. Histological findings were
categorised into normal jejunum, abnormalarchitecture (villous blunting). and the presence or
absence of mucosal inflammation. Mucosal inflam-mation was defined as an unequivocal increase inlymphocytes and plasma cells ('round' cells) and/orthe presence of polymorphonuclear leucocytes.Mucosal biopsy samples were also frozen for subse-quent determination of mucosal sucrase and lactaseactivity. '
MICROBIOLOGICAL ANALYSIS OF BOWEL
CONTENTSAfter an overnight (12 hour) fast, aspirates ofproximal small intestinal content were obtainedfrom the region of the ligament of Treitz, using a
sterile tube. In addition, ileostomy effluent was
collected from ileal pouches or appliances (Brookeileostomies), approximately 14 hours after theprevious evacuation. Bowel contents were
immediately transferred to C02-filled vials forquantitative microbiological studies. Ten-folddilutions through 10-8 were made using sterileRinger's lactate as a diluent. For isolation of aerobicorganisms, sheep blood agar, eosin methylene blue
agar, and colistin-nalidixic acid agar plates wereinoculated and incubated at 35°C. For isolation ofanaerobes, phenethylalcohol agar, rabbit blood agarwith gentamicin and vancomycin, and laked sheepblood agar were inoculated and incubated in GasPak jars (Baltimore Biological Laboratories)containing catalyst and Gas Pak envelopes for thegeneration of hydrogen and carbon dioxide. After48, 72, and 96 hours of incubation at 35°C, colonieswere picked to aerobic and anaerobic conditions sothat strict anaerobes could. be differentiated andfurther identified to the genus or species level.Statistical comparisons of numbers of organismswere made between groups using the Wilcoxon'srank sum test for unpaired data.The intestinal contents were examined for faecal
pathogens by appropriate enrichment techniques.Campylobacter fetus ssp jejuni, Salmonella, andShigella were sought specifically. Direct visualexamination for presence of parasites wasperformed on each specimen. Faecal samples fromnine of the patients with stomal dysfunction wereexamined for Clostridium difficile toxin (testsperformed in the laboratory of Drs J W Chang andS L Gorbach).
BREATH TESTSBile acid breath tests were performed according tothe method of Fromm and Hofmann. '6 Patientswere fasted for 12 hours before receiving an oraldose of 5 uCi 1-4C-cholyl glycine in 240 ml Ensure(Ross Laboratories). Expired air was collected inhydroxide of hyamine before administration of theisotopes and then hourly for four hours after the bileacid was given. Trapped 14C02 was suspended in aPerma-fluor, Carbasoda (Packard Instruments) andquantified by counting against an external gammastandard in a Beckman LS 250 Scintillation Counter(Beckman Instruments).Hydrogen breath tests were carried out after an
oral dose of 50 g lactose in distilled water.'5 17Expired air was collected for five minutes before andat hourly intervals for four hours after adminis-tration of lactose. Breath hydrogen was determinedby gas chromatography. Simultaneous capillaryblood samples were obtained before and at 15, 30,and 60 minutes after lactose. Glucose concen-trations were measured using the hexokinase assay(Hexokinase Kit, Beckman Instruments).
ENDOSCOPY AND BIOPSY OF ILEOSTOMYIleal pouches and their valves were examined usinga Fujinon model FG, QBF fibreoptic endoscope.Biopsies were obtained under direct vision at severalseparate sites with an ACMI 7035A biopsy forceps.The posterior wall of the pouch directly opposite the
195
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

Kellv, Phillips, Kelly, Weinstein, and Gilchrist
valve was avoided, as it is the region most likely tosuffer trauma from the catheter used to empty thepouch. Tissue for histology was prepared asdescribed for jejunal biopsies and was alsoevaluated by WMW.
RESPONSE TO TREATMENTPatients with pouch dysfunction were treated withmetronidazole (250 mg tid) and measurements offaecal weight, faecal fat, and the Schilling test withintrinsic factor were repeated at the end of a sevenor 14 day course of the antimicrobial.
Results
CLINICAL FEATURES (Tables 1 and 2)Patients 1-5 had laboratory features of malabsorp-tion but were essentially asymptomatic. Even onspecific questioning, only minor or no symptomscould be elicited. Except for one patient (no. 6),patients with symptoms (nos 6-12) had high faecalweights (>1000 g/24 h) and/or excessive faecal fat.All control patients (Table 2) had normal faecalweights and fat excretions except patient no. 18 whohad an increased faecal weight. Four patients (nos 1,5, 8, 12) had abnormal Schilling tests (<9% ingesteddose). All patients had normal serum vitamin B12levels. Other laboratory tests were normal orshowed changes expected after proctocolectomy(mild systemic acidosis, mild hyperchloraemia).Two patients (nos 2 and 4) had abnormalitiescompatible with a diagnosis of liver diseaseassociated with ulcerative colitis; these were long-standing and antedated proctocolectomy.
Jejunal histology was normal in all patients fromwhom tissue was available for interpretation, withone exception. Patient no. 2 had normal villousarchitecture but a mild increase of inflammatory(round) cells in the lamina propria and a single cryptabscess. Jejunal histology was not evaluated fromthree control patients (nos 17, 19, 24) and two in thedysfunction group (nos 8 and 11).
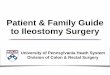
MICROBIOLOGY OF JEJUNUM AND ILEAL EFFLUENTIn jejunal aspirates the numbers of total bacteria,aerobic and anaerobic, were larger for the patientswith dysfunction than for either of the controlgroups. Numbers of anaerobic bacteria are shown inFig. 1; patients with pouch dysfunction differedfrom those with normally functioning continent(p<005), or conventional ileostomies (p=0.05).Counts of aerobic organisms reached 10 -109/g insubjects with malfunctioning ileostomies, 0-104/g inpatients with conventional ileostomies (p<005),and 102-107/g in controls with ileal pouches (NS).The major bacteria identified were of oral and
1fl10r
108
-E
E 104aWU)
0
100
0
0g Continent ileostomywith dystunction
Fig. 1 Total anaerobic bacteria (l3acteroides, Clostridium,Peptostreptococcus. Fusobacterium. Veillonella, Propionticbacterium. Euibacterium) in jejutnal aspirates fromt1 patientswith conventional (Brooke) and continent (Kock)ileostomies. Control continent were asvtnptoimatic wit/lolaevidence of dysfunction. treatment given was mnetronidazole250 mg tid. Shaded area represents upper limit of normal inhealthy subjects. Values are expressed as nuiimbers oforganisms per gram or millilitre of aspirate.
pharyngeal origin - that is, Streptococcus viridans,Bacteroides oralis, Veillonella parvula, Neisseriaspecies - with a notable absence of characteristic'faecal' flora. While aerobic bacteria are normallyfound in the proximal bowel in concentrationsof 102-104/g,'8 the numbers of such organismswhich were observed in patients with dysfunction(105-109/g) exceeded the numbers usually encoun-tered in the upper small intestine.On the other hand, no major differences were
seen among groups when bacteria in the stomaleffluents were quantified (Fig. 2). Flora in ileostomyeffluent was primarily colonic in nature (Bacteroidesfragilis, Escherichia coli, group D streptococci) inthe three groups of patients with no apparentqualitative or quantitative differences beingrecognised among groups. Faecal bacterialpathogens, parasites, and Clostridium difficilecytotoxin were universally absent.
BILE ACID BREATH TESTS (Fig. 3)Eight of the 12 patients with malfunctioningileostomies had bile acid breath tests within normallimits (<50 Fromm-Hofmann units) at two hours,and 10/12 had normal levels (<150 Fromm-Hofmann units) at four hours. Two patients (nos 1
1'96
*v
-
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

D'.sfunticutlioI of (Onltinenllt illeostoiv197
& Continern ileostomywith dysfunction
Fig. 2 Total anaerobic bacteril (Bacteroides. Clostridium.Peptostreptococcus. Fulsobacterium. Veillonella, Propionicbacterium, Eubacterium) in stomnal effluent fromti patietitswith conventional (Brooke) and contitnent (Kock)ileostomies. Control continent were as! mptomati( withoutevidence of dvsfuinction, treatment given was metronid.azole250mg tid.
and 3) displayed clearly abnormal curves throughoutthe test. A common finding (10/12 patients),however, was a high level of 14CO0 in expired air atone hour, which in eight patient represented thepeak value for the test. Control patients exhibitedsimilar patterns with a peak value at one hour beingobserved in five patients (two with continentileostomies and three with conventionalileostomies). In addition, two control patients with
ileal pouches (nos 13 and 17) and two with conven-tional ileostoniles (ilos 18 and 19) had levelsconisidcered to be abnormnal at either two or fourhours.
1 E1S 01 CC\RBOIIYDRA1E TO1FRANCEAfter a lactose load. excretion of hvdrogen in thebreath was normal (less than 0(2 mllmin) in thesecond hour in all patients. Lactose tolerance to the50 g dose was abnormal in one patient in thedysfunction group (no. 7. peak rise of 12 mg/dl at 6(0minutes) and borderline in another (no. 3. peak riseof 21 mg/dl at 15 minutes). All other patients had anormal peak rise (>25 mg/dl).'' Lactase activitv injejunal biopsies was abnormal in the same twopatients with dysfunction (nos 3 and 7) and in twocontrols (nos 16 and 18). The values were 0(3. 0(6,0)*6, and 0( 1 U/mg wet weight respectively; all otherlevels were within the normal ralnge (0.7-1 11U mg).'
II.EAI MORPHOLOGY (Table 3)Endoscopic appearances were normail in aill controlpatients and in four patients with ileostomydysfunction; these individuals (nos 1. 2. 3. 5) hadmalabsorption, but no symptoms of dysfunction.Abnormal endoscopic findings included mild tomoderate erythema. friability without discretelesions (nos 8 and 10), and pinpoint erosions (nos 6,9. 1 1). Correct postoperative anatomy of the 'nipplevalve' was confirmed in all patients.
Tissue fr-om the ileal pouch was adequate forinterpretation in 11112 patients (17 biopsies) withpouch dvsfunction. Seven patients had an abnormalarchitecture (characterised by villous blunting) andnine of 11 showed mild to moderate inflammatorychanges. The inflammatory cells were predominantlyround cells (plasma cells and lymphocytes), butpolymorphonuclear leucocytes were often present as
Control groups Dysfunction group
Fig. 3 Bile acid breath testsfor patients with continentileostomies (-) and for thosewith con ventional ileostomies(----). Normal levels aredemonstrated bv the shadedareas (16). Most patientsexhibited a peak `CO,expiration at one hourregardless of clinical status.
14CCO2 expired(Fromm Hofrr.nn Uf
0 1 2 3Time (hours)
4 1 2 3T ime (hours)
19)7
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

198
TIiblc 3 M1orpholog of'ilell/in
demn VI11i blmln Noj,//Elltis/rmal} }}i I))'O(E(
llcostotiix, til,stutinctio)1lBctor-. ntihmnatl 2/11 7 11 1) 11 412Atitci- nt hint '/28 ( X XX
lital potich cntrnk 2 5' coto.('onncntonnti Ilusontivm 57 2 7 2 7 X/X
well (nos 1, 2, 5. 6. 8, 9). Granulation tissue wasprominent in two patients (nos 2 and 7). Cryptabscesses were identified in two (nos 6 and 9).Ten biopsies were available from the five 'pouch
controls' and tissue was obtained'from seven con-ventional ileostomies. Four of the 12 controls hadabnormal architecture and three of 12 showedinflammatory changes. In neither control group,however, was the frequency and severity of morpho-logical features significantly different (X2 test) frombiopsies obtained from patients with dysfunction.Moreover, histological change was certainly not areliable indication of ileostomy dysfunction in anyindividual (Fig. 4). Normal tissue was obtained frommalfunctioning ileostomies and, conversely,abnormal appearances were seen in controls.Furthermore, examination of serial sectionsrevealed variability of morphological change withinindividual biopsies, emphasising the patchy natureof abnormalities.
RESPONSE TO TREATMENT (Table 4)After metronidazole there was symptomaticimprovement in all patients (nos 6-12) who
presented with complaints of pouch dysfunction. Inall instances there was relief of pain, cramps. ornausea, correction of the difficulty with intubation.and cessation of bleeding. All patients had areduction in faecal weight, and, in addition, faecalfat decreased to normal or near normal values inpatients 4. 5, and 1(; three of the four patients withan abnormally low Schilling test returned to thenormal range.As expected, metronidazole decreased the
number of anaerobic organisms in both jejunal andstomal specimens (Figs 1 and 2). Aerobic bacteriadiminished in jejunal aspirates but increased in ilealeffluent.
Eleven biopsies of pouch mucosa were obtainedfrom eight patients after metronidazole. One patient(no. 1) whose pretreatment mucosal biopsy revealedinflammation had a normal biopsy after treatment.All others were unchanged by treatment.
FOLLOW-UP
Responses to a follow-up questionnaire indicatedthat four of 12 patients (nos 3. 4, 5. 8) hadmaintained a decreased ileal output without further
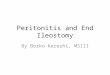
Fig. 4 A. Case3 (Table 1). Normal villousarchitecture in biopsyfrom ilealpouch. Thispatient had diarrhoea and mild steatorrhoea.B. Case 16 (Table 2). Marked villous bluntingin biopsyfrom ilealpouch. This patient hadnormalpouchfunction. Both Hand E, x 120(original magnification).
KellY, Phillips, KellY, Weltistein, and Gilchrist
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

l)!s/uieuio f.(0eo icl i/eosti,nvl19
'ldhlcrlt 4 ,AbI.tti,Ut ti/c lliFUietil /1o1 iu ll( * /te
/'lti (1('iifiii ZIt I (iei i(lii/( I ii ii1 it/i //'
2)4 hi iii,!'iti(C li I' i lrilli)
I)iitii'nlt I/c/we4¢ Iut(J I/i(/inc( I8/et} I/c/toi -I/rl
I S7)0S 1007t 43A9 0s2 '(tS 11)07? 2)) 43R 9) I)1'S' 1A'- It4 12 12 17
4 9(4 941 1 9 2 Is7(6 IS 1 S ( ')
6 9)1' 41) IS 30t7 11 ( 6'6(4 6 . 1I.S 1B_ (C' 4 _ _ 13
Itt 145' 1090) 6 26 NL)II 1 332 664 ND 24 NI)12' S, 6o4; 5 S 3 4
NI) = l donett)1t
courses of antimicrobials. Eight have requiredadditional treatment with various antibiotics, andtwo have also been treated with salicylazosulpha-pvridine. All control patients have continued tohave no symptoms with their ileal pouches.
Discussion
Dvsfunction of ileal pouches is due most often topartial or complete reduction of the 'nipple valve`;valve prolapse leads to a characteristic svndrome ofincontinence and difficult intubationis.' Althoughimprovements in operative techniques and betterselection of patients- have lowered the incidenceof valve failure. 5-10%7r of patients will still developthis complication. Pouch dvsfunction which is due tonon-mechanical causes can. however, producesimilar symptoms and it is important clinically todistinguish between these causes. Anatomicaldefinition of the valve. by endoscopy and a barium.pouchogram'. will usually suffice. Our patients withpouch dysfunction all had normal anatomy but were
otherwise a mixed and unselected group. some witha spectrum of symptoms and others havingasymptomatic diarrhoea and/or malabsorption.We observed an impressive response to metronid-
azole in the patients with dysfunction of thecontinent ileostomv. In part this mav be explainedby the unexpected finding of bacterial overgrowth ofthe proximal small bowel. Even some patients withnormal pouch function. however. had an apparentincrease in jejunal flora. Thus, the presence of a
stagnant reservoir within the pouch may predisposeto bacterial overgrowth in the jejunum in allpatients. and it is possible that a subtle qualitativedifference in the flora determines whether mal-
absorption or pouch dysfunction develops. Theidentities of the predominant organisms in our studvdid not reveal a specific micro-organism which couldaccount for the difference. The response tometronlidazole with its anaerobic spectrum ofactivity suggests that anaerobes or their byproductsmight be responsible for the clinical effects. Patientswho have required subsequent treatment, however,have responded to a variety of antibiotics.commonly ampicillin. Thus, an antibiotic with abroader spectrum might have been even moreuseful. Follow-up has indicated the necessity forrepeated courses of antibiotics, a feature consistentwith the diagnosis of 'contaminated bowelsvndrome'.Among other groups that have observed
diarrhoea or dysfunction in patients with ilealpouches, Schj0nsby" and Loeschke` impli-cated bacterial overgrowth in the pouch itself. Ourbacterial counts in ileostomy effluent were notdifferent among patients with pouch dysfunction.and those with normally functioning pouches orconventional ileostomies. The results reported herefor conventional ileostomies are comparable withthose of Gorbach et a121 and Finegold.2' Ourbacterial counts from conventional and continentileostomies are. however, one to two log units lowerthan those of Schj0nsby.' Thus, our findings do notsuggest that quantitative microbiology of ileostomyeffluent is of value diagnostically.
It should be noted that the jejunal flora wasqualitatively that of the proximal gut, and did notreflect the content of the pouch. Factors responsiblefor jejunal bacterial overgrowth are uncertain, butreflux of pouch contents' into the ileum (andbeyond) seem unlikely. Altered motility of theproximal intestine, secondary to distension of thepouch, is suggested by the finding of slowed transitof a liquid meal.22 Reduced motility in the proximalsmall bowel might well impair clearance oforopharyngeal organisms from the jejunum.
In an attempt to identify other associations withbacterial overgrowth, we examined jejunal histologyand disaccharidase activity and sought evidence ofbile acid deconjugation. Bile acid breath tests wereof limited benefit in predicting bacterial overgrowthof the proximal small intestine. Patients with bothcontinent and conventional ileostomies, regardlessof clinical status, had abnormal breath tests at theend of the first and second hours, suggesting rapidcontact of bile acids with a flora capable ofdeconjugation. The test did not separate fromcontrols the patients with increased numbers ofbacteria in the proximal small bowel. The presenceof faecal flora in the ileum would be expected toproduce this pattern, making the application of
199
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

200 KellY, Phillips, K/llY, Weinstein, alnd Gichrist
traditional normal values obtained from healthysubjects of questionable validity. Only two of the 12patients with pouch dysfunction had clearlyabnormal bile acid breath tests throughout the fourhour test.The apparent discrepancy of the various indices of
lactose absorption is, perhaps. not surprising inthese patients who lack a colon. The failure ofbreath hydrogen excretion to increase may reflectthe absence of a faecal flora able to metaboliseunabsorbed lactose. This possibility is supported bythe presence of flat lactose tolerance curves anddecreased jejunal lactase activity in two patientswho had normal hydrogen breath tests. Depletion ofmucosal lactase and lactose intolerance are con-sistent with a diagnosis of bacterial overgrowth, -3but are not prerequisites. These biochemicalabnormalities were infrequent and not associatedwith an abnormal morphology in our patients. Onlyone patient (no. 2) had a definite, but mild.non-specific histological lesion in the jejunum.Many have reported a non-specific inflammation
of the pouch mucosa associated with symptomaticmalabsorption. 71(') II> We found a poor correla-tion between the endoscopic appearances of thepouch and the presence or absence of abnormalitieson light microscopy. Thus, an abnormal endoscopicappearance of a pouch, though dramatic, may be oflittle significance. Mucosal histology was also oflittle help diagnostically; tissue was abnormal insome patients with well-functioning pouches andnormal in some with dysfunction. In part, thesefindings may reflect patchy changes and theproblems of obtaining representative samples. Ourfindings are in agreement with Nilsson andcolleagues26 who reported slight to moderate inflam-matory reaction in the lamina propria of pouches inseven of 13 patients, even though histochemicallythe mucosa was normal.There are several practical implications of the
present study. When pouch function is disturbed,mechanical failure of the 'nipple valve' should besought by endoscopy and barium studies. A positivediagnosis requires corrective re-operation. Endo-scopy might also suggest an alternative aetiologyand, although histology is not a reliable guide toinflammation in the pouch, biopsies should beobtained to look for recurrent Crohn's disease.Quantitative faecal outputs of fat and volume shouldbe performed to document malabsorption if present.Faecal cultures and microscopy will be needed toexclude specific pathogens27 and/or toxins but wefound that the identification of faecal ecology wasunhelpful in contrast with the experience ofothers.9 9 Empirical treatment of pouchdysfunction with antimicrobials may be reasonable,
though efficacy should be monitored by repeatingappropriate studies after treatment. If one antibioticfaills, another may succeed and some patients willrequire repeated courses of antibiotics. Given that alifetime with an ileal pouch is to be expected, theoccurrence of evenl borderline malabsorption cannotbe ignored though the significance is still uncertain.
The authors are grateful to Anne Haddad. JenniferBouska. an(l Carol McLimans of the Mayo Clinic,Colleen Murdoch of the Universitv of Alberta, andEsther Braden of UCLA for technical assistance,and to the staff of the Clinical Research Center,Mayo Clinic, for care of the sublijects. Dr SherwoodGorbach's laboratory performed assays forclostridial toxins. Mary' I lancnberger providedexpert secretarial help.
References
1 Kock NGi. Intra-abdominal reservoir in patients withpermanent ileostomy. Agrchmg 1969. 99: 223-31.
2 Dozois RR. Kelly KA. Beart RW. Beahrs OH.Improved results with continenlt ilcostonmy. Anini Slmg1980; 192: 3 19-24.
3 King SA. Qualitv of life - the continent ileostomn. AniniSurg 1975: 182: 29-32.
4 Kock NG. Darle N. Kewenter J. Mvrvold H. PhilipsonB. The quality of life after proctocolectomy andileostomy: a study of patients with conventionalileostomies converted to continent ileostomies. Di.sColon Rectum 1974; 17: 287-9'2.
5 Kock NG. Darle N. Hulten L. Kewenter J. Mvrvold HI.Philipson B. Ileostomv Clurr Prob Suirg 1977; 14: 1-52.
6 Dozois RR. Kelly KA. llstrup D, Beart RW. BeahrsOH. Factors influencing revision rate after continentileostomy. Arch Su,rg 1981; 116: 610-3.
7 King SA. Enteritis and continent ileostomy. C(onn Medl1977; 41: 477-9.
8 Myrvold HE. Kock NG. Continent ilcostomy inpatients with Crohn's disease. (Abstract.) Gastro-enterology 1981; 80: 1237.
9 Schjonsby H. Halvorsen JF. Hofstad T. Hovdenak N.Stagnant loop syndrome in patients with continentileostomy (intra-abdominal ileal reservoir). Guit 1977;18: 795-9.
10 Gelernt IM. Continent ileostomy forum. OstomYn Q1979; 16: 56-9.
11 Halvorsen JF, Hermann P, Hoel R, Nygaard K. Thecontinent reservoir ileostomy: review of a collectiveseries of thirty-six patients from three surgicaldepartments. Surgery 1978; 83: 252-8.
12 Kelly DG. Branon ME. Phillips SF. Kelly KA.Diarrhoea after continent ileostomv. G(ut 1980: 21:711-6.
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from

D)'sfiuntionI of onitineni ilco.Sto,x. 20()1
13 Van der Kamer JiH, ten Bokkell. Iluininkl.\[C\rHA. Rapid method for determination o ffats in eces. JBiol Chem 1949: 177: 347-55.
14 Perera DR. Weinstein WM, Rubin CE. Smill hoselbiopsy. Huim Pathol 1975: 6: 157-217.
15 Newcomer AD, McGill DB. Thomras PJ. 1lofwonnAF. Prospective comparison of indlirect methorlslodetecting lactase deficiency. EngI J M/cd 1(75: 293:1232-6.
16 Fromm H, Hofmrann AF. Breatlh test for alteredbile-acid metabolism. Lanmet 1971: 2: -S
17 Levitt MD. Donaldson RM. UJs of respiratorxhydrogen (H,) excretion to detect carbohydrate 1m;al-absorption. J Lab (Clin Md 197(1: 75: 937-45.
18 Donaldson RM Jr. The relation of cnteric bacterialpopulations to gastrointestinal function and disease. In:SIcisinger MH. Fordtran JS. eds. GJ.%iroi,ucshildDisease, 2nd edn. Philadelphia: Saunders. 1978.
19 Loeschke K. Bolkert T. Kieflhaber P. Ruckdeschel G.Lohrs V. Bark, S. Schaudig A. Bacterial overgrowth inilcal reservoirs (Kock pouch): extended functionalstudies. Hepao-Gia.stroentierol 19801; 27: 31(1-6.
2(0 Gorbach SL. Nahas L. Weinstein L. Studies ofintestinal microflora. IV. The microflora of' ilcostomveffluent: a unique microbial ecology. Ga,stroemterolog-x,1976: 53: 874-80.
21 Finegold SM. Sutter VL. Bolc JD. Shimnada K. The
nornial llora oiol antdurxaid ransxerscolostom 5etllticnts. .1 InlI/c 1)1% 197): 122: 376-81
22 Kelly 1)DK. S'hillipsSF. Kelly KA. Weinstein WM1.(iiillierist NiR.] Bacterial overcrowth in the jejunumn ot1;ti.'lts sit h il.al pouches. (Abstract. ) Goairo-i'nirolog 1'(0I9) 78: 1 193.
23 (jianineilla RA. Rout WR. loskes PP. Jelunal brushborder ilnjury ind impaired sugar and arnino aciduptake in blind loop syndrome. ((i.siroetiterologv 1974:67: 965-74.
4 l3loeh R. Menge H. Lorenz-Meseer H. Stockert H(.Riecken EO. Functional. biochemical and morpho-lowical alterations in the intestines of rats with experi-mental blind-loop svndrome. Re.s Exp Me(l 1975: 166:67-78.
25 Bonello JC. Thow GB. Manson RR. Mucosail enteritis:a complication of the continent ileostomy. Dis ColnRecutlatn 1981; 24: 37-41.
26 Nilsson LO. Kock NG. Lindgren 1. Myrvold [HG.Philipson BM. Ahren C. Morphological aind histo-chemical changes in the mucosa of the continentileostomy reservoir 6-1( vears after its construction.S'cand J Gastroeniterol 1980(: 15: 737-47.
27 Drake AA. Huizenga KA. Van Scoy RE. Campvlo-bacter fetus s.s. jejuni: a caIuse of' diarrhea in a patientwith a continent ileostomr. Dig Dis Sci 1982: 27:1(037-8.
on July 11, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.24.3.193 on 1 March 1983. D
ownloaded from