-
8/18/2019 Ileostomy Guide
1/29
-
8/18/2019 Ileostomy Guide
2/29
A MessageTo You...
Ileostomy surgery is a lifesavingsurgery that enables a
person toenjoy a full rangeof activities, includingtraveling,
sports, family lifeandwork. Thousands of peopleannually undergo
ostomy surgery for various
reasons and return to a healthy, functioninglifestyle.
TheUnited Ostomy Associations of America (UOAA) is a
volunteer organization dedicated to helpingthosewho haveor
will haveostomy or
other diversionary surgery by providingone-on-onesupport, local
support groupmeetings, conferences, and educational material
through its web site,
printed material and ThePhoenix magazine.
You havemany peers in theUOAA who areready to answer
your questions, providesupport and reassureyou that you can
havea full,
productivelifeafter ostomy surgery.Weinviteyou to join us as
wefulfill our mission in helpingothers.
FromtheUnited Ostomy Associations of America
-
8/18/2019 Ileostomy Guide
3/29
ILEOSTOMY GUIDE
Reviewed by:
Nancy Gutman, RN, CWOCN
2011
This guidebook is available for free, in electronic form, from
the United Ostomy Associations of America(UOAA). It was originally
produced, copyrighted and sold by the United Ostomy Association
(UOA), thenational US ostomy organization from 1962 to 2005, which
released its copyrights on this material.
UOAA may be contacted at:www.ostomy.org • [email protected] •
800-826-0826
-
8/18/2019 Ileostomy Guide
4/29
4
CONTENTS
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . 6
FACTS ABOUT ILEOSTOMIES . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . 7
NORMAL DIGESTIVE SYSTEM. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . .8S ma ll intestine. . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . 8
Large intestine . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
TYPES OF SMALL BOWEL DIVERSION . . . . . . . . . . . . . . . . .
. . . . . . . . . . 9Ileoa nal res ervoir (J -Po uch) . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . 9
B rooke ileos tomy . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Co ntinent ileos tomy . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
MANAGEMENT FOR BROOKE ILEOSTOMIES . . . . . . . . . . . . . . .
. . . . . 10Choos ing a pouching s ystem . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
P ouches . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Meas
uring for a p roper fit . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 11
Belts . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11
Cha nging the pouching s ystem . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 12
Fac tors tha t influence pouc hing s ystem se a l . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 12
Emptying the pouc h . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Osto my s upplies . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
HELPFUL HINTS . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . 13P rotecting the s kin
around the s toma . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 13
S pots of blood on the s toma . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . 13
Removing ha ir unde r the pouch . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . 14Flatulence (ga s)
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . 14
Odor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14
Medications/a bs orption . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . 15
ILEOSTOMY COMPLICATIONS . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 15S evere skin prob lems . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . 15
Obs truction/B loc kage . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Diarrhea. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15
Elec trolyte ba lanc e . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
P hantom rectum . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
S hort bow el syndrome . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . 17Medical
emergenc ies . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . 17
Hos pitaliza tion . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
LIVING WITH AN ILEOSTOMY . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 18Telling others . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . 19
Clothing a nd a ppearance . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . 19
Eating a nd d ige stion . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Returning to wo rk . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Intima cy a nd s exuality . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
-
8/18/2019 Ileostomy Guide
5/29
5
CONTENTS Cont.
LIVING WITH AN ILEOSTOMY cont.P a rticipating in sports . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 21
Ba thing a nd s wimming . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Tra vel . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22
FOR PARENTS OF CHILDREN WITH ILEOSTOMIES . . . . . . . . . . . .
. . . . 23P syc hosoc ial iss ues . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23
Manag ement iss ues . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Everyda y living . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
RESOURCES AVAILABLE . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . 26United Ostom y Ass oc ia tions of
America . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . 26
Internationa l Ostomy Ass oc ia tion . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . 26
Wound Os tomy C ontinence Nurse s S oc iety . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . 26
Age ncies . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26
Medicare, Medica id and S oc ia l Sec urity in the United S
tates . . . . . . . . . . . . . . . . . 26
GLOSSARY . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . 27
-
8/18/2019 Ileostomy Guide
6/29
6
INTRODUCTION
An ileostomy is a life-saving surgery that enables individuals
to enjoy a full range
of activities including traveling, sports, family life and work,
even though they have a
stoma a nd w ear a pouching sys tem.
Ileostomy surgery is performed for many different diseases and
conditions. Some
of the indications for ileostomy surgery are ulcerative colitis,
Crohn’s disease, familial
polyposis and complications of cancer.
There is no o ne w a y to ta ke c a re o f an ileos tomy. J ust
a s ileos tomies differ, s o
does how to take ca re of them. This guide boo k gives you s
ugges tions and idea s for
ma na ging your ileos tomy. Disc uss the ide a s w ith a phys
ician or a Wound Os tomy
Continence Nurse (WOCN), hereinafter referred to as ostomy
nurse, and adapt them
to your situation. Give new things a fair trial, but do not
insist on them if they fail to
make you more comfortable. What is good for someone else may not
be good for
you. The s oo ner you lea rn to ta ke c a re o f your ileos
tomy, the b etter you a re likely tofeel about yourself. In time,
you will gain confidence in your self-care.
There a re ma ny w a ys to g a in a greater understa nding of
your life w ith a n ileos tomy.
Your physician a nd os tomy nurse a re important so urce s of
informa tion a nd suppo rt. In
a ddition, muc h information is a va ila ble at va rious Web s
ites (see Re sources ).
Ta king pa rt in a n os tomy s upport group a llow s you to s
hare your feelings a nd a s k
questions as you make progress with your adjustment. It also
allows you to share
your successful adjustment with others who may need the benefit
of your experience.
Most ostomy visitor programs are sponsored by local support
groups of the United
Ostomy Associations of America (UOAA). If you would like a
visitor or to take part in asuppo rt g roup, a sk your physician, o
sto my nurse , or other nurse s to ma ke a referra l.
You or your family may also locate your local UOAA support group
by calling
800-826-0826 or vis iting w w w.os tomy.org.
-
8/18/2019 Ileostomy Guide
7/29
7
FACTS ABOUT ILEOSTOMIES
An ileos tomy is a surgica lly c rea ted ope ning in the abd
ominal wa ll. The end of the
ileum (the lowest portion of the small intestine) is brought
through the abdominal wall
to form a s toma , usua lly on the lowe r right s ide of the a
bd omen. When you loo k a t
your stoma, you are actually looking at the lining (or mucosa)
of the intestine, which is
like the lining of your cheek. Generally, the colon and rectum
are removed and normalco lon a nd recta l functions a re no long er
pres ent.
The s toma w ill a ppea r pink to red a nd w ill be moist a nd
shiny. It w ill red uce in s ize
over a s hort period of time a fter surgery. The s ha pe w ill
be round to ova l a nd ma y
protrude or be flush with the skin.
An ileostomy may be permanent or temporary depending upon the
reason
for surge ry. The entire c olon, rectum, a nd a nus a re removed
or bypa s se d w ith a
permanent ileostomy. With a temporary ileostomy, all or part of
the colon is removed,
but part or all of the rectum is left intact.
The ma jor function of the s ma ll intes tine is to a bs orb the
bod y’s nutrients a nd
w a ter. Enzymes relea s ed into the s ma ll intestine b rea k
food into s ma ll pa rticles s o tha t
vitally needed proteins, carbohydrates, fats, vitamins and
minerals can be absorbed.
Thes e enzyme s w ill a ls o b e pres ent in ileos tomy d isc ha
rge , a nd they c a n ca use s kin
breakdow n. This is w hy the skin a round a n ileos tomy must a
lw a ys be protected (s ee
S kin P rotection).
After removal of the colon and rectum, digestive contents pass
out of the body
through the s toma a nd a re c ollec ted in a n individua lly
fitted d ra ina ble pouch, w hich
is w orn a t a ll times . The c ons is tenc y of the ileos tomy
output w ill be liq uid to pa s ty,
depending on one’s d iet, medica tions and other factors. B eca
use the output isconstant, the pouch will need to be emptied 5-8
times a day.
-
8/18/2019 Ileostomy Guide
8/29
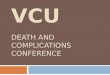
NORMAL DIGESTIVE SYSTEM
Although an ileostomy
crea tes an important c hange for
a patient, the body’s chemistry
a nd d ige stive function a re not
significantly altered by it. A
de sc ription o f the la rge a ndsmall intestine may help
you
understand the chang es to your
body.
Small Intestine• Approxima tely 20 feet long ,
consisting of:
• Duod enum (first pa rt) 10-12
inches long beginning at
the outlet of the stomach.• J ejunum (s ec ond pa rt),
a bo ut 8-9 feet long .
• Ileum (third pa rt), a bo ut 12 feet long c onnec ting to the
la rge intes tine a t the
cecum.
• Food nutrients a re d iges ted a nd a bs orbed in the sma ll
intestine a s food is moved
through by peristalsis.
Large Intestine• Approxima tely 5-7 feet long , c ons isting o
f:
• Ce cum – c onta ins the ileoc ec a l va lve, w hich prevents
reflux into the ileum;
contents are highly acidic liquid• Asc end ing c olon – co
ntents a re a cidic liq uid
• Tra nsverse co lon – co ntents a re less a cidic liq uid
• Des ce nding/sigmoid co lon – co ntents be co me more
formed
• Rectum – formed s tool
• The prima ry functions of the large intestine are a bs orption
o f wa ter and
electrolytes, transport of stool by peristalsis, and storage of
digestive waste until
it is eliminated from the body.
8
-
8/18/2019 Ileostomy Guide
9/29
TYPES OF SMALL BOWEL DIVERSIONS
There a re three ma jor types of s ma ll bo w el diversions (w
hen the entire c olon is
remo ved). The surgeo n and the pa tient should d etermine the
mos t appropria te surgery
for the pa tient. S ome of the s elec tion c riteria for the
type of d iversion a re the d ise a s e
process, age, general health and the preference of the
patient.
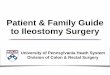
1. Ileoanal Reservoir (J-Pouch)
Indications: Discharge: Management:
• Ulcerative Co litis • S oft, formed stool • Na tura l evac
uation;
• Familia l P olypos is • 6-8 per da y • P eri-ana l skin protec
tion
• Ca ncer co mplica tions
The mo st co mmon surg ica l va ria tion is the ileoa na l
reservoir (pelvic pouch) which is an internal pouch made
of the ileum and pla ced in the pelvis. Other nam es for
pelvic pouc hes include J -pouch a nd S -pouch depend ing
on the s urg ica l proc ed ure. The s phinc ter musc
lesurrounding the a nal opening mus t be intac t to keep the
pouc h from leaking . The cons is tenc y of the output of
the pelvic po uch depends on diet and ma y be a ided by
medications. For additional information on the ileoanal
reservoir or j-pouch, please see the Ileoanal Resvervoir
Guidebook.
2. Brooke Ileostomy
Indications: Discharge: Management:• Ulce ra tive Co litis • Liq
uid or pa ste • S kin protec tion;
• Crohn’s Disea se co nsistency • Open-end, drainab le pouch
• Familia l P olyposis • Unpredictable drainag e
• C anc er complica tions • C ontains residual diges tive
enzymes
The Brooke ileos tomy is the sec ond mo st co mmon
type of ileo s tom y s urgery. The terminal ileum is pulled
through the abdominal wall and a segment is turned
back and sutured to the skin, leaving a smooth, rounded,
everted ileum a s the end of the ileos tomy.
The s toma is usua lly plac ed in the righ t low er
q uad rant w henever poss ible a nd loca ted on a fla t
surface
suffic iently free from irreg ula rities. The feca l output is
not
controlled and will require wearing a collection pouch.
9
Ileoanal reservoir(Pull-through)
Ileoanal Reservoiror Pelvic Pouch
Intestine
Standard or Brooke Ileostomy
-
8/18/2019 Ileostomy Guide
10/29
10
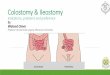
3. Continent Ileostomy (Abdominal Pouch)
Indications: Discharge: Management:
• Ulce ra tive Co litis • Liq uid or pa ste • Dra in period ica
lly
• Familia l P olypos is co nsistenc y w ith intubation tube
• Ca ncer complica tions • Stoma covering
A continent ileostomy is a surgical variation of the
sta nda rd ileos tomy. P atients do not need to wea r a n
externa l pouch. Created w hen a portion o f the ileum
is loo ped ba ck on itself so tha t a res ervoir is formed
inside the a bd omen. A nipple va lve is co nstructed
w ith pa rt of the ileum. The o sto ma te inse rts a ca
theter
a few times e ac h da y to drain contents from the
reservoir. For additional information, please see the
Ileoanal Reservoir Guidebook.
MANAGEMENT FOR BROOKE ILEOSTOMIES
Lea rning to ca re for your ileos tomy ma y s eem ha rd a t
first, b ut with pra ctice a nd
your ow n a da ptations, the e ntire proces s w ill bec ome s ec
ond na ture, just like s ha ving
or ba thing.
A suc ce s sful pouching s ystem sho uld provide the follow
ing:
• S ec urity with a g oo d leakproof s ea l (la sting for 3-7 da
ys )
• Odor resistant pouch
• S kin protec tion• B e incons picuous a nd unnoticea ble
• Easy to a pply and to remove
Choosing a pouching system
Many fa cto rs ca n influence se lec tion. The length of the s
toma , a bd omina l firmnes s
and contours, the loc ation of the stoma , sc ars a nd folds in
the abd ominal area and
your height a nd w eight a ll must b e c ons ide red in de
termining w ha t is bes t for you.
Special adaptations may have to be made for stomas located near
the hipbone,
waistline, groin, scars, etc. Custom-made products to fit
unusual situations can beobta ined from s ome c ompa nies.
The be s t pouc hing s ys tem for you is a very persona l ma
tter. It is important that
you are properly fitted, just as for eyeglasses. When you are
selecting your first
pouching s ystem, it is bes t to co nsult with a n os tomy nurse
or someone w ho ha s
experience in this area.
Continent Ileostomyor Abdominal Pouch
Stoma
-
8/18/2019 Ileostomy Guide
11/29
11
MANAGEMENT FOR BROOKE ILEOSTOMIES cont.
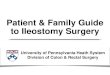
Pouches
A pouching sy stem is used to c ollec t ileos tomy o utput.
There a re tw o m a in types
of systems available: one-piece pouches with attached skin
barrier and two-piece
sys tems c ompo se d o f a s kin ba rrier a nd d eta cha ble
pouch. The ba rrier or bas e of thepouch may require a hole to be
cut for the stoma or may be sized and pre-cut.
Pouches for one- and two-piece systems are drained through an
opening in the
bottom. P ouches a re ma de from od or resistant materials a nd
va ry in cos t. Po uches
a re either tra nspa rent or opa q ue a nd c ome in different
lengths .
Measuring for a proper fit
Pouching systems come with either a pre-cut opening or can be
cut to fit the
stoma size and shape. Immediately after surgery the stoma may be
swollen fora pproxima tely 6 to 8 w eeks. During this pos t
operative period the s toma sho uld
be mea sured a bout once a we ek. A mea suring c ard ma y be
included in boxes of
pouches or you may c rea te your ow n templa te w hich ma tches
your stoma sha pe. The
ope ning on the skin ba rrier or fla nge s hould be no more than
1/8 inch la rger than the
stoma size.
Belts
Wea ring a be lt is a very individua l ma tter. S ome perso ns w
ho
have ileostomies wear a belt because it makes them feel morese
cure or it gives s upport to the po uching s yste m. Others
find
a belt cumberso me. If you choos e to w ea r a belt, a djust it
so
that you ca n get tw o finger widths betw een the belt a nd your
waist in order to avoid a
de ep g roo ve or cut in the s kin a round the sto ma . This co
uld res ult in s erious da ma ge
to the stoma and cause pressure ulcers on the surrounding skin.
Belts should be worn
so they do not ride above or below the level of the belt tabs on
the pouching system.
People who are in a wheelchair may need a special belt.
Manufacturers carry special
belts or you can make one yourself.
One-piece drainablepouch w/skin barrier
Two-piecedrainable pouch
Flange for two-
piece system
Adjustable belt
Drainablepouch clip
-
8/18/2019 Ileostomy Guide
12/29
12
Changing the pouching system
There ma y b e a de creas e in bow el ac tivity a t ce rta in
times in the d a y. During
these times w ill be the ea siest to c ha nge the po uching s
yste m. You ma y find tha t
ea rly morning before you ea t or drink is bes t. Or allow a t
lea st one ho ur a fter a mea l
w hen peris talsis is slowe d. After surge ry ileos tomy o utput
ma y b e thin a nd w a tery. As
the discharge thickens, you will be in a better position to
determine the best time forcha nging your system.
Factors that influence pouching system seal
There a re s everal fac tors tha t ca n influence ho w long the
pouch w ill s tay se a led .
Thes e include w ea ther, s kin c ond ition, s ca rs , w eight c
hang es , d iet, a ctivity, b od y
shape near the stoma and the nature of the ileostomy output.
• P erspira tion d uring the s ummer months in w a rm humid
clima tes w ill sho rten the
number of days you ca n wea r the pouching s ystem. B ody hea t,
in ad dition to
outside temperature, will cause skin barriers to loosen more
quickly than usual.• Moist, o ily s kin ma y reduce w ea ring
time.
• Weight cha nge s w ill also a ffec t your we a ring time.
Weight ga ined a fter ileos tomy
s urge ry cha nges a bd omina l co ntours. You ma y need a n
entirely different s yste m.
Weight los s ma y a ls o ha ve the sa me effect.
• Diet ma y influence your sea l. Foods that ca use w atery disc
harge may prevent a
long lasting seal.
• P hysica l a ctivities ma y have s ome influence o n we a ring
time. S w imming, very
strenuous sports or work that causes perspiration may shorten
wearing time.
Emptying the Pouch
Emptying the pouch w hen it is 1/3 full will prevent bulging a
nd poss ibility o f a lea k.
Also co nsider your co mfort a nd c onvenience .
To empty, follow thes e s teps :
1. S it on the toilet
2. P la ce a sma ll s trip of toilet pa per in the toilet to
minimize s pla s hing
3. Hold the bottom of the pouch up and o pen the pouch at the ta
il
4. S low ly unroll the ta il into the to ilet
5. G ently empty co ntents
6. Clean the outside a nd inside of the pouch ta il w ith toilet
pa per7. Close the pouch at the ta il
8. S ome pouc hing s yste ms ha ve an integrated closure (follow
ma nufa cturer’s
suggestions)
Ostomy Supplies
For the s a ke o f co nvenience , keep a ll your eq uipment tog
ether on a she lf, in a
drawer or in a small box away from hot or cold temperatures.
-
8/18/2019 Ileostomy Guide
13/29
13
MANAGEMENT FOR BROOKE ILEOSTOMIES cont.
It is a good idea to order supplies several weeks before you
expect to run out,
thus allowing enough time for delivery. It is best to avoid
stockpiling of supplies
bec aus e they may be influenced b y cha nges in temperatures. S
upplies do not need to
be s terile. The s toma a nd s urround ing s kin a re no t ste
rile a nd req uire only cleanlines s .
To o rde r a dd itiona l pouches , w a fers a nd o ther os tomy
products , you w ill needthe manufacturer’s name and product
numbers. Supplies may be ordered from
a ma il order compa ny or from a med ica l supply or pha rma cy
in your tow n. For
informa tion a nd help in ordering, yo u may co ntac t a loc a l
os tomy nurse , the prod uct
ma nufa cturer, telephone direc tory busines s pa ge s or the
internet (s ea rch w ords:
ostomy supplies).
HELPFUL HINTS
Protecting the skin around the stoma
Ileos tomy output ca n be irrita ting to the s kin a round the s
toma . This s kin a rea
should a ppear the sa me a s a nywhere else on the ab domen. Us
e the follow ing
techniques to help keep your skin healthy.
• Us e the right s ize a nd type o f pouch a nd s kin ba
rrier opening. An opening tha t
is too sma ll ca n cut or injure the s toma a nd ma y ca use it
to sw ell. An opening
that is too large exposes the skin to possible irritation. In
both cases, change the
pouch or skin ba rrier and repla ce w ith one that is properly
fitted. S ee the s ec tion
in this booklet on measuring for a proper fit.
• Itching or burning a re s igns that the pouching s ystem s
hould be c hang ed.Cha nge the pouc h reg ula rly to a void lea ka
ge a nd s kin irritation. It ma y a lso
indica te tha t you w ould bene fit from a co nvex ba rrier to
prevent stoo l from
lea king underneath
• Remove the pouc h or skin ba rrier by g ently pushing your
skin from the pouch or
ba rrier ra ther than pulling it a w a y from the skin.
• Clean the skin surfac e a round the stoma with wa ter. A
mild soa p ma y be used,
but rinse tho roug hly. Dry w ell be fore a pplying the s kin ba
rrier or pouc h.
• Wa tch for s ens itivities a nd a llergies to a dhes
ive, s kin ba rrier, pa ste, tap e o rpouch ma teria l. They c a n
develop w eeks, months or even years a fter use o f a
prod uct since the bod y ca n bec ome g ra dua lly se nsitized .
You ca n test d ifferent
products to see if your skin will react to them.
Spots of blood on the stoma
S pots of blood are no ca use for alarm. Cleaning a round the
stoma a s you cha nge
the pouc h or skin ba rrier may ca use slight b leed ing. The b
loo d vess els in the tiss ues
-
8/18/2019 Ileostomy Guide
14/29
of the sto ma a re very delica te a t the surfa ce a nd a re ea
sily disturbed . The bleeding
w ill usua lly s top a s ea sily a s it sta rted.
Removing hair under the pouch
Exces s ive ha ir around the s toma a rea ca n interfere w ith
the skin ba rrier and ma ybe pa inful w hen remo ving . Trimming ha
ir with sc iss ors is helpful. A straight ra zor
should not be used to shave this area, if you must use a razor
an electric is the best
choice.
Flatulence (Gas)
Immediately after surgery, it may seem that you have excessive
gas almost all
the time. Most a bd omina l surge ry is follow ed by this
uncomfortab le, emb a rra s sing,
yet harmless symptom. As the tissue swelling goes down, gas will
occur less often.
Certain foods may cause intestinal gas: eggs, cabbage, onions,
fish, baked beans,milk, che es e a nd a lco hol.
Eating reg ula rly w ill help prevent exces sive ga s. S kipping
mea ls to a void ga s or
discharge is unwise because your small intestine will be more
active and more gas
and watery discharge might result. Some people find it best to
eat a lesser amount of
food 4-5 times a day.
Odor
Many things , s uch a s food s, normal ba cteria l a ction in
your intestine, illnes s,different medicines and vitamins can cause
odor. Some people with ileostomies have
more trouble with odors than others. Individual experimentation
is the only solution
to this prob lem. The od or of ilea l co ntents is not the s a
me a s that o f a no rma l s tool
bec a use the ba cteria that c a use food brea kdow n (a nd o
dor) in the co lon a re not
present in the small intestine. Here are some hints for odor
control:
• Use a n odor resistant pouch.
• Chec k to s ee tha t the skin ba rrier is se curely se a led
to the s kin.
• Empty the pouch freq uently.
• P la ce s pec ia l de od orant liq uids a nd/or ta blets in
the pouch.
• Ora l prepa ra tions a re a vaila ble. Chec k w ith your
physicia n or ostom y nurse
ab out the s uitab ility of these products a nd recommended dos
a ge. Amongthos e tha t ma ny ha ve found e ffec tive a re c
hlorophyll ta blets, Devrom® (bismuth
subg a llate), a nd bismuth s ubca rbona te.
• Air deod orizers a re a vaila ble that effectively c ontrol
odo r when emptying the
pouch.
14
-
8/18/2019 Ileostomy Guide
15/29
15
HELPFUL HINTS cont.
Medications/Absorption
Medication in the form of coated tablets or time release
capsules may come out
w hole in the pouc h a nd b e of no bene fit a t a ll. Disc uss
this w ith your hea lthca re
provider or pha rmac is t if this o ccurs. There may b e a
lterna tive med ica tions tha t youca n use to a void this prob
lem. Liq uid or liq uid ge l med ica tions provide fas ter and
more effective a bs orption.
ILEOSTOMY COMPLICATIONS
Severe Skin Problems
La rge a rea s of s kin that a re redde ned, s ore a nd w eeping
(a lw a ys w et) w ill prevent
a go od se a l around the s toma . It is therefore importa nt to
treat minor irritations w henthey first oc cur. If you ha ve a la
rge irrita ted a rea , c onta ct your physician o r ostomy
nurs e. They ma y pres cribe topica l med ica tion s uch a s
Mycos ta tin® pow der or
Kenalog ® s pra y.
For de ep press ure ulce rs ca used by a very tight b elt, loo
se n or remove the belt
a nd ca ll your physician o r ostomy nurs e immedia tely, trea
tment is need ed .
Obstruction/Blockage
There a re o cc a sions w hen the ileos tomy d oes not function
for short period sof time. This is norma l. How ever, if the s toma
is not a ctive for 4 to 6 hours a nd
is a cc ompa nied b y cramps a nd/or nausea , the intestine
could b e ob structed. An
ob struction (or bloc ka ge ) ma y b e pa rtia l; tha t is, so
me liq uid ma y pa ss through. Ca ll
your doctor or ostomy nurse in either case to discuss the
situation.
Wa tch for sw elling o f the stoma a nd a djust the opening of
the pouch a cc ordingly
until the prob lem ha s pa ss ed . Ta ke a w a rm ba th to rela
x the ab do mina l musc les .
S ometimes a cha nge in bod y pos ition, such a s a ss uming a
knee to ches t position,
may encourage movement of the bolus of food. Do not take a
laxative. If unable to
pas s a food b olus, go to the nearest emergenc y room.
Obstruction ca n be c a used b y high-residue food s s uch as
Chinese veg etab les,
pineapple, nuts, co conut and c orn and by internal cha nges
such a s a dhes ions.
DiarrheaWhen d ia rrhea oc curs, the intestina l co ntents p a s
s through the s ma ll intestine
too quickly for the absorption of fluids and electrolytes to
take place and may cause
exces sive los s of fluids a nd elec trolytes . You mus t q
uickly repla ce these elec trolytes
to avoid becoming ill from dehydration and mineral
deficiency.
-
8/18/2019 Ileostomy Guide
16/29
16
However, loose stool can come from eating certain foods and is
usually temporary.
Raw fruits and vegetables, milk, fruit juice, prune juice or
contaminated drinking water
are examples. Loos e stoo l may a lso be c ause d b y emotiona l
stress . So me people
w ith ileos tomies ma y a lw a ys have “ w a tery disc ha rge ”
a nd this is normal for them. The
only w a y to be sure yo u ha ve d ia rrhea is to me a sure yo
ur output. 800-1,000 cc /da y is
normal for an ileostomy.
Diarrhea has these characteristics:• The intestine disc ha rge s
g rea t q uantities of wa tery sto ol.• It comes on s uddenly and
ma y be ac companied by c ramps.
Diarrhea can be caused by:• Intestinal flu which ma y be a cc
ompa nied b y fever a nd vomiting.
• Antibiotics , penicillin a nd o ther pres cription me dica
tions .
• P a rtia l ob struction charac terized by od orous d is cha
rge , cramps , force ful liq uid
output and excess ive noises from the stoma . It ca n be c a
used b y food o r other
fac tors. You s hould s eek medica l a ttention if this oc
curs.
If diarrhea persists , c ons ult your physicia n or os tomy
nurse. Ta ke me dica tions a spres cribed . Then repla ce fluids by
ta king o ne cup o f sw eetened , clear tea o r one g la ss
of orang e juice follow ed the next hour by one cup o f sa lty
broth. Co ntinue a lternating
the drinks until diarrhea subsides.
Electrolyte Balance
Electrolyte balance (especially potassium and sodium) is
important. When the
colon (large intestine) is removed, a greater risk for
electrolyte imbalance can occur.
Diarrhea, excessive perspiration and vomiting can increase this
risk. Your diet should
include fluids a nd foo ds rich in sod ium and pota s sium.
Dehydration is a common concern with symptoms of increased
thirst, dry mouth,
decreased urine output and fatigue. Increase any type of fluids
such as Pedialyte ®
w hich is high in potas s ium and so dium. Avoid high-sug a r
drinks w hich c a n ca use
osmotic diarrhea. Daily intake of fluids should be 8-10 (8 oz.)
glasses. Any liquid
containing water (soda, milk, juice, etc.) helps to meet your
daily requirement. Loss
of appetite, drowsiness and leg cramping may indicate sodium
depletion. Fatigue,
muscle w ea kness a nd s hortness of brea th may indica te potas
sium de pletion.
Additional dietary guidelines may be found in the Diet and
Nutrition Guide
publishe d by the United Osto my Ass oc ia tions of America
.
-
8/18/2019 Ileostomy Guide
17/29
17
ILEOSTOMY COMPLICATIONS cont.
Phantom Rectum
P hanto m rec tum is simila r to the “ pha ntom limb” of a
mputees w ho feel as if their
remo ved limb is s till there. It is norma l for you to feel as
if you need to e va cua te. This
can occur for years after surgery. If the rectum has not been
removed, one may also
have this feeling a nd ma y pa ss mucus w hen sitting o n the
toilet. So me w ho have ha dtheir rectum removed say that the
feeling is relieved somewhat by sitting on the toilet
and ac ting a s if an eva cuation is taking plac e.
Short Bowel Syndrome
This co ndition ha ppens in Crohn’s disea se or dise a se s of
the s ma ll intestine when
surgery is req uired to remove a subs ta ntia l a mount of the s
ma ll bo w el. This c ond ition
merits spe cial attention b ec a use of the loss of the
intestine’s vital ab so rptive function.
P eople w ith this c ond ition mus t rema in under a phys
ician’s s upervis ion. Theyca n live a normal life but must be ca
reful to ma intain ad eq uate nourishme nt, a void
diarrhea a nd to b e w ithin rea ch of med ica l ca re. The s
horter the s ma ll intes tine, the
more liq uid the d isc ha rge w ill be. This ma y reduce the
time a pouch ca n be w orn
bec a use of mo re rapid undermining of the s kin ba rrier. S
pec ia l pouching s ystem s a re
available for high, liquid ileostomy output.
Medical Emergencies
You should call the doctor or ostomy nurse when you have:
• Cramps la sting mo re than 2-3 hours• Co ntinuous na usea a nd
vomiting
• The ileos tomy do es no t have a ny output for 4-6 hours a nd
is a cc ompa nied b y
cramping and nausea
• S evere wa tery disc harge la sting more than 5-6 hours
• S evere od or may indica te infection
• A deep c ut in the stoma
• S evere skin irrita tion o r deep ulcers
• Exces sive bleed ing from the s toma opening (or a mod erate a
mount in the pouch
a t se vera l times of emptying)
• Co ntinuous b leeding a t the junction b etween s toma and
skin
• Unusua l cha nge in sto ma s ize (prolaps e or retra ction) a
nd a ppea ra nce (co lor)
Hospitalization
Ta ke yo ur os tomy s upplies w ith you s ince the hos pital ma
y not ha ve your type.
Prepare to do some expert communicating, especially if you go
into a hospital where
ileos tomy pa tients a re rare or if you g o for a co ndition no
t rela ted to yo ur os tomy.
-
8/18/2019 Ileostomy Guide
18/29
Do not submit to any procedures you think may be harmful such as
taking a
la xative, ta king a n enema through the s toma or rec tum, or
insertion o f a rec tal
thermometer. If you a re in doub t a bo ut a ny proced ure, a s
k to ta lk to your do cto r.
Ask to have the following information listed on your chart: 1)
type of ostomy or
continent diversion 2) whether or not your rectum has been
removed or is intact 3)details of your management routine and
products used 4) procedures to be avoided
(see above).
LIVING WITH AN ILEOSTOMY
Learning to live with an ileostomy may seem like a big
undertaking. It is similar
to o ther major cha nges in your life. B eg inning a new job ,
mo ving to a nother city,
marriage and having children are all examples of adapting to a
new way of life.
Initia lly, yo u ha ve to a djust to the unfamilia r as pec ts
of thes e e xperience s a nd this
may take some time. Having a positive outlook on life, patience
and a sense of humorare keys to adjusting to any new situation. You
can find support through local, UOAA
Affilia ted S upport G roups . To find a g roup in your area ,
vis it w w w.o s tomy.org o r ca ll
800-826-0826.
There a re times a fter surge ry w hen yo u ma y feel disco ura
ge d. You ma y feel alone
and iso lated . Be ca use the whole experience is s o new to
you, you may feel a wkwa rd,
frustrated a nd uncertain. Feeling disc oura ge d is rea l a nd
normal. You might cry, b e
hos tile or angry a nd rea ct in wa ys tha t a re unusua l for
you. Ta lking to a truste d friend ,
nurs e, c lergy a nd c erta inly a nother perso n w ith a n os
tomy ma y help you w ork through
those feelings. You may discover new hope and encouragement.
Your soc ia l life ca n be a s a ctive a s it w a s before surge
ry. You c a n enjoy a ll
activities such as travel, sporting events, eating at
restaurants or whatever you
enjoye d b efore. The firs t time yo u go out of the ho use a
fter surgery, you ma y feel as
if everyone is staring at your pouch even though it is not
visible under your clothing.
You ma y feel your pouch o n your bo dy, but no one c a n se e
it. Keep thes e q uestions
in mind: Did you know wha t a ileos tomy wa s, or where a stoma
wa s loca ted, or wha t
it looked like, before you had surgery?
You ma y a lso w orry a bo ut your pouch filling w ith g a s a
nd bulging under your
clothing. A quick trip to the rest room can take care of this
problem. If you are worried
about your pouch filling up immediately after eating at a social
event, remember,people without ileostomies often need to go to the
rest room after eating and nobody
will think it unusual if you do the same. You will probably find
that you need to empty
your pouch of co ntents a nd g a s less often than you need to
urinate.
18
-
8/18/2019 Ileostomy Guide
19/29
19
LIVING WITH AN ILEOSTOMY cont.
Telling Others About Surgery
You might b e w orried a bo ut how others w ill a cc ept you a
nd ho w your so cial role
may be changed. It is natural to wonder how you will explain
your surgery. Your
friends and relatives may ask questions about your operation.
You can tell them as
much a s you w a nt them to know. You need not feel you ha ve to
explain your surge ryto everyone who asks. A brief explanation
would be that you had abdominal surgery,
or that you ha d a pa rt of or your entire c olon removed.
If you ha ve c hildren, a ns w er their ques tions s imply and
truthfully. A s imple
expla na tion w ill be enoug h for them. Once you ha ve expla
ined w ha t a ileos tomy is,
they may a sk q uestions a bo ut it and w a nt to see yo ur s
toma or the pouch. Ta lking
a bo ut your surge ry in a natural w a y w ill dispel any mis co
nceptions they might ha ve.
They w ill a cc ept your ileos tomy much the s a me w a y you do
.
If you a re c ons ide ring ma rria ge , d isc uss ions w ith
your future s pous e a bo ut life w ith
a n ileos tomy a nd its effect o n s ex, c hildren a nd fa mily
a cc epta nce w ill help to a llevia temisc onc eptions on the pa
rt of the spo use. Attending UOAA suppo rt g roup mee tings
tog ether w ill a ls o b e helpful. Ta lking to o ther couples ,
in w hich one pa rtner has a
ileostomy, will provide an experienced viewpoint.
Clothing and Appearance
One does not need to purchase special clothing after ileostomy
surgery, but some
minor ad justments ma y be nece ss a ry for comfort and
preference . The pres sure of
underga rments w ith ela stic w ill not ha rm the s toma or
prevent function o f the bo w el.
If you were ill before surgery, you may find you can now begin
to eat normally forthe firs t time in yea rs . As your appetite
returns, yo u may ga in weight. This c a n a ffect
the clothes you choose more than the pouching system itself.
Cotton knit or stretch underpants may give the support and
security you need.
P anty hos e a re a lso co mfortab le. A simple pouch c over ad
ds comfort by ab so rbing
perspira tion a nd keeps the pouc h from resting on the skin.
Men ca n w ea r either boxer
or jockey-type shorts.
Eating and Digestion
After healing is complete and the ostomy is functioning
normally, most people with
ileos tomies ca n return to a reg ula r diet. If you ha ve a spe
cial diet be ca use o f hea rt
disease, diabetes or other health problems, you should ask your
doctor about a diet
that will work for you. Here are a few simple guidelines about
your diet:
• Doc tors often ha ve their patients follow a low -res
idue d iet the first w eeks a fter
a ny a bd omina l surge ry. This include s only food s that a re
ea sily d ige sted a nd
excludes ra w fruits a nd vege tables. B e s ure to find out w
hen you ca n sta rt a
reg ula r diet. Ea t a ll food s that you like e xcept thos e
restricted by your physician.
-
8/18/2019 Ileostomy Guide
20/29
20
• Try one food a d a y that you ha ve not ea ten since
surge ry. Eat sma ll portions a t
first, then grad ually increas e the a mount. If a sm a ll s
erving gives yo u cramps or
diarrhea , eliminate that foo d from te mporarily a nd try it a
ga in in a few w eeks.
• Drink plenty o f liq uids . A minimum of 8-10
eight-ounce g la s ses of w a ter per da y
is rec ommend ed . Dehydra tion a nd los s of electrolytes (s a
lts a nd minera ls ) a repossible if not enough fluids are consumed
in a day. Increase your fluid intake if
persp iring or in ho t c lima tes .
Beets will make ileostomy output turn a reddish color rather
like blood, but
there is no ha rm do ne. Toma to juice a nd foo d d yes ma y cha
nge the usua l co lor of
ileos tomy o utput a s w ell.
Additional dietary guidelines may be found in the Diet and
Nutrition Guide
publishe d by the United Osto my Ass oc ia tions of America
.
Returning to Work
As your strength returns, you can go back to your regular
activities. If you return
to w ork, you ma y w is h to c onfide in your employer or a g oo
d friend. B eing o pen
a bo ut your ileos tomy w ill help ed uca te others. Keeping it
a c omplete sec ret ma y
cause practical difficulties.
Persons with ileostomies can do most jobs; however, heavy
lifting may cause a
stoma to herniate or prolapse and should only be resumed under
the guidance of
a physician. A sudden blow in the pouch area could cause the
barrier or pouch to
shift and cut the stoma. Still, persons who have ileostomies do
heavy lifting, such asfiremen, mec ha nics a nd truck drivers.
There a re a thletes w ho ha ve s toma s. Chec k
with your doctor about your type of work. As with all major
surgery, it will take time
for you to regain strength after your operation. A letter from
your doctor to your
employer ma y be helpful sho uld the employer have d oubts a bo
ut your physica l
capabilities.
Employability and insurability are issues for some individuals.
If these issues
de velop, se ek help from hea lthca re profess iona ls a nd/or
talk w ith others w ho ha ve
found solutions to these issues.
Intimacy and Sexuality
Sexual relationships and intimacy are important and fulfilling
aspects of your
life that should continue after ostomy surgery. Your attitude is
a key factor in
re-establishing sexual expression and intimacy. A period of
adjustment after surgery
is to b e e xpected . S exual function in wo men is us ually not
impa ired , w hile s exual
potency of men may sometimes be affected, usually only
temporarily. Discuss any
prob lems w ith your phys ic ia n and/or os tomy nurse .
-
8/18/2019 Ileostomy Guide
21/29
21
LIVING WITH AN ILEOSTOMY cont.
Any sexuality co ncerns you have s hould be disc ussed openly
betw een you a nd
your pa rtner. It is likely tha t yo ur pa rtner w ill ha ve a
nxieties a bo ut s exua l a ctivities due
to lack of information. An intimate relationship is one in which
it matters how well two
people c a n co mmunica te.
The first time yo u bec ome intima te a fter surgery things ma y
not g o perfec tly. Menmay have trouble getting and keeping an
erection and women sometimes have pain
during intercourse. Thes e c onditions w ill usua lly improve w
ith time. Your interes t in
sex will gradually return as your strength is regained and
management issues are
ma s tered . B od y c onta ct d uring s exual ac tivities w ill
usua lly not ha rm the s toma or
loos en the pouch from the a bd omen.
Women ma y co nsider wea ring c rotc hles s p a nties , “ted
dies,” or a s hort slip or
nightie. Men may consider wearing a cummerbund around the
midsection to secure
the pouch. There a re s evera l types of pouch c overs that c a
n be purcha s ed o r you ca n
make your own.
Ostomy surgery may present more concerns for single individuals.
When to tell
“that s omeone s pecia l” depend s upon the relationship. Brief
ca sua l da tes ma y not
need to know. If the relationship grows and leads to intimacy,
the partner needs to be
told a bo ut the os tomy prior to a se xual experience .
P regna ncy in women w ho ha ve had ileos tomy s urgery is not
uncommon. B efore
preg na ncy is c ons ide red , it sho uld b e d isc uss ed w ith
your do cto r. The ileos tomy
itself is not a reason to avoid pregnancy. If you are healthy,
the risk during childbirth
appears to be no greater than for other mothers. Of course,
other health problems
must be taken into consideration and discussed with your
physician.
For more information, the guide book Intimacy, Sexuality and an
Ostomy is
a vaila ble from the United Osto my As so ciations of America
.
Participating in Sports
An os tomy should not limit your pa rticipa tion in sp orts.
There a re a few
preca utions, however. Many physicians do not a llow conta ct s
ports b eca use o f
possible injury to the stoma from a severe blow or because the
pouching system
ma y s lip. How ever, thes e problems ma y b e o verco me w ith
s pec ia l protec tion. Weight
lifting c ould result in a hernia a t the s toma . C heck w ith
your do cto r a bo ut such s ports.Inde ed, people w ith os tomies
a re d ista nce runners, w eight lifters, skiers, s w immers
and participate in most other types of athletics.
Bathing and Swimming
You ma y ba the w ith or without your pouching sy stem in pla ce
. Norma l expos ure to
air or contac t with so a p a nd w a ter will not harm the s
toma a nd w a ter does not enter
the ostomy opening.
-
8/18/2019 Ileostomy Guide
22/29
22
Remember these points;
• You may w a nt to protec t the barrier by ta ping the edge s w
ith wa terproof ta pe
• You ma y wa nt to choo se a sw im suit that ha s a lining for
a s moo ther profile
• Women ma y we a r stretch panties m a de e spe cially for s w
im suits
• Men may w a nt to wea r a support ga rment sold in men’s
underwea r depa rtments
or athletic wear departments
• Men may prefer to w ea r a tank top a nd trunks, if the sto ma
is a bo ve the belt line
• For s w imming, emp ty your pouch b eforeha nd a nd remember
to ea t lightly
Travel
All methods of travel are open to you. Many people with
ileostomies travel
extens ively inc luding c a mping trips , c ruises a nd a ir tra
vel. Travel sug ge s tions :
Ta ke along enoug h supplies to la s t the entire trip plus s
ome extras . Double wha t
you think you may need , bec a use they may not be ea sy to get
w here you are going.
Even if you don’t expect to change your pouch take along
everything you need to do
so. Zip-Lock® bags may be used for pouch disposal. Leave
home fully prepared. Findout if and where supplies are available
before a long trip. A local UOAA support group
may be helpful in locating ostomy supplies and local medical
professionals. Contact
the UOAA office or visit www.ostomy.org to find the nearest
support group.
Seat belts will not harm the stoma when adjusted comfortably.
You may place a
clothes pin near the retraction slot to relieve tension on the
belt. When traveling by
car, keep your supplies in the coolest part. Avoid the trunk or
back window ledge.
When tra veling b y pla ne, rememb er tha t chec ked-in lugg a
ge so metimes ge ts
lost. Carry an extra pouching system and other supplies on the
plane with you. Small
co sme tic ba gs w ith pla stic linings or sha ving kits w ork w
ell. Thes e s hould be pla ce din yo ur ca rry-on lugg a ge .
To a void prob lems w ith cus toms or lugg a ge inspe ction,
have a note from yo ur
doc tor sta ting tha t you need to c arry os tomy supplies and
medica tion by hand.
Further problems might be avoided by having this information
translated into the
la ngua ge or la ngua ge s of the c ountry(s ) you a re
visiting.
B efore traveling a broad , g et a lis t of the current
English-spe a king physicia ns in
various foreign cities that cha rge a sta nda rd fee. The
Interna tiona l As so ciation o f
Med ica l Ass is ta nc e to Travelers (IAMAT) a t 716-754-4883
publishes lis ts of Eng lish
spe a king physicia ns in over 2,500 cities a round the w orld.
w w w.ia ma t.org.
Tra veler’s d ia rrhea is a comm on prob lem in foreign c
ountries , w hether you ha ve
an o stomy o r not. The mos t commo n ca use of d iarrhea is co
ntaminated wa ter and /
or food. It may also be caused by mere changes in water, food or
climate. It is wise to
avoid unpeeled fruits and raw vegetables.
Persons with ileostomies lose water and minerals quickly when
they have diarrhea.
For this rea s on yo u ma y need med ica tion to s top the fluid
a nd e lec trolyte loss . Your
physicia n c a n g ive you a pres cription for med ica tion to
co ntrol dia rrhea . It s hould be
-
8/18/2019 Ileostomy Guide
23/29
23
filled in your home sta te, s ince the presc ription ma y no t
be valid else w here. B e s ure
drinking w a ter is sa fe. If the wa ter is not s a fe, do not
use the ice either. B ottled w a ter
or boiled water is recommended.
FOR PARENTS OF CHILDREN WITH ILEOSTOMIES
If you are a parent of a child with an ileostomy, you probably
have many questionsa nd co ncerns. When the s urge on s a id your
child needed this surge ry, yo ur firs t
reaction may have been, “Is this the only choice?” Your doctor
no doubt assured you
that the ileostomy was necessary to save your child’s life. You
may have felt shock.
You may have asked yourself, “Why did this happen to us?”
Ta lking to a goo d friend , your docto r, clergy, os tomy
nurse, o r the pa rents of a
child w ho ha s a n ileos tomy helps. Your loc a l suppo rt
group of the United Osto my
Assoc ia tions of America ca n refer you to other parents . This
w ill prepa re yo u to he lp
your child adjust to the ileostomy. Deal with your own feelings
first, then you may give
your child the emotional support he or she need s.
If you a re fee ling guilty o r res pons ible for your child’s
illnes s a nd surgery, this is
a normal feeling for parents. You ma y think tha t your drea ms
ha ve be en s hattered
and may wonder if your child will be able to do the things that
others do. Most
parents worry about their child’s life span, ability to work,
adjustment to living with an
ileos tomy a nd in la ter years, ma rria ge a nd family. Thes e
a re no rma l conc erns o f a ll
parents facing major changes in their child’s life.
When your child is in the hos pita l, be there a s often a s pos
sible. B eing in the
hospital and having surgery are frightening at any age. At this
time your child is
especially vulnerable and needs to feel wanted and reassured
about your love. You
be ing there ma kes him/her feel se cure.
B e prepared for how y ou w ill feel se eing a n opening on yo
ur child’s a bd omen w ith
bowel contents running into a pouch. Your first reaction, in
your child’s presence, is
vitally important and must be as positive and casual as
possible.
If your child ha s a fever or other symptoms , don’t pa nic. He
or she w ill ha ve a ll the
a ches a nd pa ins that o ther children have. When in doubt, c a
ll your physician.
Psychosocial Issues
As your child beg ins to recover from ileos tomy s urge ry,
there a re ma ny w a ys you
ca n be a so urce o f strength and support.
Your so n or da ughter may b e a fra id tha t young
friends a nd rela tives w ill not w a nt
to be a round them. Your ac cepta nce is need ed. Encourag e
your son or da ughter to
talk to yo u ab out these feelings . If you a re op en a nd na
tura l a bo ut the ileos tomy, he or
she w ill be, too.
Try to und ersta nd how your child feels. Your child ne ed s to
fee l tha t you
-
8/18/2019 Ileostomy Guide
24/29
24
unders ta nd w ha t it is like to have a n ileos tomy. Too m uch
s ympa thy, how ever, is no t
goo d a nd w ill take a wa y a sens e of independ ence. Listen,
try to understand feelings ,
enco ura ge a nd b e ta ctful. It is difficult not to o
verprotec t a nd pa mper a c hild w ho is
rec overing from ma jor surge ry. B ec a use it is so ea sy to g
ive in to your feelings , be a s
firm a s pos s ible.
If your child is very young, they will probably accept the
ileostomy easier than
you. The c hild w ill g row up with it a nd it w ill be co me a
na tura l pa rt of them. For a
teenag er who is facing a ll the problems a ss ociated w ith
puberty a nd a dolescenc e,
this s urge ry co mes a t an e spe cially difficult time. The c
hang es in bod y ima ge ca used
by the ileos tomy ma y co mpound the stress es of a dolescenc e.
Your teenag er may feel
unattra ctive, rejec ted a nd d ifferent be ca use of the ileos
tomy.
You may notice temporary changes in behavior patterns. Your
acceptance and
suppo rt is es pec ia lly nee de d now. Try to understa nd the
feelings a nd liste n to the
co mpla ints. P rovide enco ura ge ment to find realis tic so
lutions to thes e problems .
Management Issues
Ta ke an interest in your child’s c a re a nd ma na ge ment. If
he or she is o ld enoug h,
you will want to encourage independence in their ostomy care.
Your child may require
so me help and s upport a t firs t, due to inse curity a bo ut
the new s upplies , phys ica l
w ea knes s a nd tiring e a sily. A very young child c a n be ta
ught to emp ty the pouch. An
older child can get supplies together and learn steps of
changing the pouch, until
the whole proces s c a n be do ne alone. You may w ant to use a
teac hing proc ess that
begins with your son or daughter assisting you. Later on you can
help, standing by to
help only when it is need ed .
A very important pe rs on to help with ca re o f your child is
the o s tomy nurse. This is
a person w ho ha s rec eived s pec ia l tra ining in ostomy m a
na ge ment. To find a n os tomy
nurs e, c heck w ith your hospita l or conta ct the United Osto
my Ass oc ia tions of America
a nd its s upport g roups w ho c a n refer you to a n WOCN (ET)
nurs e in your area .
Be prepared for trial and error in managing, or helping to
manage, your child’s
ileos tomy. There are some cha nges tha t will oc cur in the beg
inning tha t w ill not
hap pen later. There ma y b e d iet a djustments , s kin prob
lems , po uching prob lems a nd
others. The importa nt thing to rememb er is that a nything new
needs experimenta tion
a nd a da pta tion. A se nse of humor and a pos itive a ttitude
w ill be helpful.
Everyday Living
B e flexible in d ea ling w ith your child’s a da ptation to s
cho ol and everyda y living
situa tions . If at first, the p ouch s hould hap pen to leak a
t sc hool, your child c a n go
to the s cho ol nurse . You might p ick up your child for a po
uching cha nge a t home,
then he or she c a n return to s cho ol. One young ste r tells
this sto ry: he noticed that his
pouch w as lea king a nd ha d sta ined his trousers. Instea d o
f rushing o ut of the cla ss a s
-
8/18/2019 Ileostomy Guide
25/29
25
everyone else did, he ca lmly w a ited until everyone ha d left
the room. In this w a y, he
very wisely avoided embarrassment and then called home so that
his mother could
pick him up. You may want to visit the principal, the classroom
teacher, the physical
education teacher and the nurse to explain your child’s
needs.
You will find that your child can participate in sports, can go
on overnight trips, to
ca mp a nd do a ll ac tivities enjoye d be fore. At first, it
will be d ifficult to let yo ur child
go a wa y on his o r her ow n. Disc uss w hat c an b e do ne if
any problems come up whileyour child is a w a y from ho me. Trea t
them a s you trea t your other children.
Ta lk with your child a bo ut how they w ill explain the s
urgery to o thers. He or she
ma y w a nt to tell close friends , rela tives a nd a cq uainta
nces . Natura lly, peo ple w ill be
curious. Once the surgery is explained, chances are your child
will be accepted as
before. Your child will likely duplicate your explanation. If
you discuss it in a natural
w a y w ith others, your child w ill a lso . Most peo ple w ill
w a nt to know w ha t to expec t
and how they ca n help. Encourag e o thers to empa thize, not s
ympathize.
Remind yo ur child to be co nsiderate o f others. Cleaning up
the ba throom a fter
ileostomy care is important to maintaining family harmony. You
and your child arefac ing a new situa tion in your lives. If it is
a pproa ched w ith opennes s, p erseverance
a nd a se nse of humor, you w ill find that a n ileos tomy w ill
not s top yo ur so n or
da ughter from enga ging life’s everyda y a ctivities . P a
rents find that a hea lthy child w ith
an ileos tomy ca n once a ga in be a happy c hild.
Eac h s ummer, the United Osto my Ass oc ia tions of America spo
nso rs a Youth
Ra lly for ag es 11 through 17. This is a ca mp for young pe
ople with osto mies ,
alternate procedures and other related conditions. Planned
educational sessions on
self-esteem, b od y imag e, hygiene, os tomy iss ues plus d isc
ussion ses sions, craft
projects, tours and sports are offered. For further information,
contact the Youth Rally
Co mmittee, Inc. a t w w w.ra lly4youth.org.
J oin the loc a l UOAA suppo rt group a nd keep ab rea st of the
new es t prod ucts a nd
med ica l prog res s a nd sha re e xperience s w ith other pa
rents. Add itiona l informa tion for
support of the children and their families can be obtained by
calling 800-826-0826 or
by visiting w w w.os tomy.org.
-
8/18/2019 Ileostomy Guide
26/29
-
8/18/2019 Ileostomy Guide
27/29
27
GLOSSARY OF TERMS
Anastomosis: the surgica l formation of a pas sa gew a y betw
een two normally
dista nt spa ce s o r orga ns. A “ho oking-up” of bo w el,
ureter, a rtery, vein, etc., a fter a
section is removed.
Benign: not cancerous, not malignant.
Carcinoma: cancer, malignant growth.
Colectomy: remo va l of all or pa rt of the co lon.
Colitis: infla mma tion o f the la rge intestine. A pa rticula
rly s evere type is ulcerative
colitis, which may require an ileostomy.
Colon: pa rt of the intestine which s tores d ige stive ma teria
l a nd a bs orbs w a ter. Als o
referred to as the large intestine or the large bowel.
Congenital: pres ent or existing a t the time o f birth, suc h a
s a de formity, disea se , ortendency.
Continent Diversion: any fecal or urinary diversion that avoids
the need to wearan external collecting pouch. Continent fecal
diversions include the J-Pouch(evacuated through the anus) and Kock
Pouch (emptied with a catheter). Continenturinary diversions
include the Indiana Pouch (emptied with a catheter) andNeobladder
(evacuated normally through the urethra).
Continent Ileostomy (or Kock Pouch): the surgical creation of an
ileal pouch inside
the low er ab do men to co llec t w a ste a fter a co lec tomy
for ulce ra tive c olitis. The
pouch is emptied regularly with a small tube inserted through an
opening in theabdomen - no external bag is required.
Crohn’s Disease: ileitis, regional enteritis or granulomatous
disease of the bowel:
inflammatory bowel disease which penetrates the deep lining of
any part of small
or la rge bow el. In se lected ca ses , ileos tomy bec omes
neces sa ry; Crohn’s ca n flare
up after ileostomy surgery, however.
Diverticulitis: inflammation of the diverticula (little sacs on
the colon); can cause
abscess, scarring with stricture or perforation of the colon
with peritonitis in severe
cases .
Diverticulosis: presence of diverticula (little sacs on the
colon).
Electrolytes: sa lts a nd minera ls needed by the b ody for
health.
Enzyme: subs tance formed in a nimal and pla nt cells that s
tart or speed s up
sp ec ific chemica l rea ctions.
-
8/18/2019 Ileostomy Guide
28/29
28
Familial Polyposis (multiple polyps ): rare dise a s e; runs in
fam ilies . The colon
a nd rec tum co nta in ma ny po lyps . This is a different
condition from me rely the
presence of a small number of polyps in the colon. Familial
polyposis requires
reg ula r medica l s upervision of a ll members o f the fa mily
b ec a use of s erious
complica tions and strong tendency to maligna ncy.
Fistula: an a bnorma l pas sa ge betw een two internal orga ns
or from a n internal
orga n to the surface of the bod y.
Gastroenteritis: an inflammation of the stomach and the
intestines.
Hernia: the protrusion (bulging) of a loop or knuckle of an
organ or tissue through
a structure which usually contains it.
Hernia (a bd omina l): the protrusion of a n interna l orga n
throug h the a bd ominal
muscula ture; ca n oc cur a round s tomas .
Ileostomy output: w a s te ma tter from the ileum (sma ll intes
tine). Als o referred to a s
intestinal contents, d isc harge, d raina ge, b ody wa ste, s
tool, feces .
Ileostomy: an “opening of the ileum” in which the end of the
small intestine (ileum)
is brought out s urgica lly through a n ope ning in the a bd
omen. Intes tina l co ntents
a re e xpelled from the b od y through this opening.
Ileum: low es t pa rt or end of the s ma ll intestine.
Inflammatory Bowel Disease (IB D): genera l term for ulcerative
co litis a nd Crohn’s
disease.
J -Pouch: a res ervoir created out of s ma ll isntes tine
a fter remova l of hte co lona nd portions of the rectum. This
interna l pouc h holds feca l ma tter (s too l) be fore
elimination through the anus.
Malignancy: a cancerous growth.
Obstruction: blockage of ileostomy indicated by partial or
complete stoppage of
ileal flow.
Ostomy: surgically created opening through the abdominal wall
for the elimination
of body waste. Refers to ileostomies, colostomies and
urostomies. Also referred to
as s toma.
Ostomy Visitor: person with an ostomy, member of United Ostomy
Associations
of America, with special training to visit people before or
shortly after ostomy
surgery. The vis itor offers support a nd information ra ther
than med ica l a dvice.
Peristalsis: prog res sive wa ves of motion w hich oc cur
without voluntary control to
push w a ste ma teria l through the intestine.
-
8/18/2019 Ileostomy Guide
29/29
Polyp: sma ll projec tion inside of bo w el, often mus hroo m s
ha ped ; ma y b e fla t. It is
usually benign, but can be malignant.
Prolapse: a “falling out” in which the stoma becomes longer.
Prosthesis: an artificial substitute for a missing body part,
such as an arm or leg,
eye, or tooth, used for functional or cosmetic reasons or
both.
Rectum: lowest portion of the large intestine.
Resection: surgical removal or excision.
Retraction: the stoma d raw s b a ck into the bod y.
Revision: construction of a new stoma when the original one does
not function
well.
Skin Barrier: a ny one of severa l subs tance s us ed to c over
skin around the stoma .
Can be pliable sheets, pastes, etc.
Stenosis: narrow ing o r tightness of the stoma which ma y ca
use o bs truction.
Stoma (opening): an end of the ileum or colon which is brought
through the skinas a site for stool or urine to exit the body.
(Note that even urinary stomas are builtfrom a segment of ileum or
colon.) The stoma often protrudes like a nipple andmay be around
3/4” to 1-3/4” in diameter. It is usually pink to red in color.
Stomasdo not include nerves sensitive to pain, so it is possible to
cut or burn a stomawithout feeling anything. Stomas do, however,
include nerves sensitive to otherstimuli such as stretching.
Stricture: an a bnormal narrowing of a body pas sa ge.
Ulcerative Colitis: one form o f infla mma tory bow el dise a se
in w hich ulce rs form in
the intestinal lining of the colon and rectum. Severe, often
bloody, diarrhea is the
primary symptom of the disease, which occurs most often in young
adults.
Wound, Ostomy and Continence Nurse, o r an Ente ros tom a l
Thera py (ET) Nurse.
A person who takes care of and teaches ostomy patients. A
special training course
for registered nurses is required for certification.