Embed Size (px)
Citation preview

Dynamic Daily Surgery Scheduling
Centre for Biomedical & Healthcare Engineering
CNRS UMR 6158 LIMOS
Ecole des Mines de Saint Etienne, France
Centre for Healthcare Engineering
Dept. Industrial Engr. & Management
Shanghai Jiao Tong University, China
Xiaolan XIE

- 2 -
Healthcare engineering lab
At
EMSE & SJTU

- 3 -
People
Xiaolan Xie, professor
Saint Etienne Vincent Augusto, CR, HDR en 2015 Thierry Garaix, MA Ramesky Pham, Engineer (2016) 4-8 Ph.D. students Associate members: Marianne Sarazin, MD, Hopital Firminy Bruno Salgue, IMT
Shanghai Zhibin Jiang, professor Andrea Matta, professor Na Geng, Asso prof. Ran Liu, Assist prof. Feng Chen, asso. Prof. Na Li, asso. Prof. About 10 PhD students and 10 Msc students Zheng Zhang, SJTU-Univ. Michigan Siqiao Li, SJTU-Free Univ. Amsterdam

- 4 -
Eco-system
Campus for Health & Innovation @ Saint Etienne • EMSE-Centre for Biomedical & Healthcare Engineering • Medical school • Teaching hospital CHU-SE • Incubator for spin-offs in med tech PTM
Shanghai Jiao Tong University
• 13 affiliated hospitals including 6 LARGE ones
• Strong incentives for medicine-engineering collaboration

- 5 -
Smoothing demand
Triangle: Quality of service, Quality of Work, Cost
Extra-beds at ED, 2013.07 Outpatient queue, 6h AM,11/15/2011
Matching capacity & demand Improving service quality

- 6 -
Mission statement
Develop quantitative methods for modeling, simulation and
optimization of health care systems & health services
Explore the integration of medical knowledge and patient
health information in operations management of health care
systems
in close collaboration with hospitals
Stochastic modeling and optimization in the face of random events and changing system dynamics

- 7 -
Theme I : Engineering health care systems & services
To develop scientific methods for performance evaluation, capacity planning and process engineering.
Examples of work done : • Patient flow analysis with UML and Petri nets • Simulation & capacity planning of Emergency departments
• Process improvement of hospital supply chains by RFID • Health care logistics with mobile service robots • Permance evaluation of Hospital Information Systems
• Designing home healthcare networks • Design and operations of perinatal care networks • Care pathway for elderly people
• Blood collection optimization

- 8 -
Dynamic perinatal network reconfiguration
Context • 3 types of neonatal cares (OB = obstetrics care,
Neo = basic Neonatal Care, NICU) • 3 types of maternity services (OB, OB+Neo,
OB+Neo+NICU) • Demographic evolution • Immediate admission of random arrivals
Dynamic capacity planning and location of hierarchical service networks under service level constraints, IEEE Transactions on Automation Science and Engineering, 2014.
Perinatal Network of North Hauts-de-Seine
(Type-3) H. Louis Mourier
H. Beaujon
(Type-1)
H. FOCH
(Type-2)
CH Neuilly (Type-2)
H. Franco Britan (Type-2)
H. Nanterre (Type-1)
Challenge: • Determine optimum reconfiguration of perinatal
networks to meet demographic changes with equal service level of care
Solution & results: • Erlang loss-queueing model for admission probability evaluation; • Original hierarchical service network with nested hierarchy of patients and maternity services • Network reconfiguration by opening/closing services, capacity transfers, hiring/firing • Large-scale nonlinear optimization models solved with original linearization techniques • 5% increase of admissions at the 1st choice hospital.

- 9 -
Process mining of cardiovacular patients (funded by HEVA company)
Goal • Extract the process model of
hospitalization events • From what patients actually endured
instead what the « experts » think
“An Optimization Approach for Process Discovery of Complex Event Logs”, on going.
Challenge: • Huge number of hospitalization events • Delicate balance between details and
readability (avoid spaghetti diagrams)
Key treatment: Implantable Cardioverter Defibrillators
Solution & results: • Hierarchical structure of event classes to
capture event relations • Formal mathematical modelling of the process
mining optimization • Application of efficient optimization algorithms

- 10 -
Traceability in biobanks
Research questions
Performance evaluation of traceability technologies
Design supply chains of drugs and medical devices with RFID
New operation management problems (re-warehousing of bio-banks, skill/quality monitoring, ...)
Info errors
Inventory error Current situation
Samples stored in nitrogen tanks (77°K) “Cold Chain” constraints Resistance of the tags?
Hand-made inventories, data-base updates, cryotube numbering or label edition…
Problems: Error probabilities (Hand-copy, inventory, picking, computerization…)
Impacts of Radio-Identification on Cryo-Conservation Centers, TOMACS, 2011.

- 11 -
Theme II: Planning and logistics of health care delivery
To develop optimization methods for operations management of healthcare delivery and its supply chains.
Example of work :
• Planning and scheduling operating theatres subject to uncertainties • Capacity planning control MRI examinations of stroke patients • Stochastic optimization for hospital bed allocation
• Inpatient admission control • Dynamic outpatient appointment scheduling
• Operation management of outpatient chemotherapry • Capacity planning and patient admission for radiotherapy
• Robust home healthcare planning • Home healthcare admission planning&control
• Management of winter epidemics (flu, bronchitis, gastroenteritis) • Long-term care planning & scheduling

- 12 -
Optimization of outpatient chemotherapy
ICL Loire Cancer Institute
Major challenges of further research: • Integration of decisions different levels and different time scales
(medical planning, patient assignment, appointment scheduling) • Modeling treatment protocols with rich medical knowledge • Modeling the dynamics of health conditions based on rich patient data • High uncertainties of patient flow and patient's health care requirement
Large variation in bed capacity requirement in actual planning
20% reduction of peak bed requirement in the optimized planning
bed requirement
Planning oncologists of ambulatory care units. Decision Support Systems. 2013

- 13 -
Capacity planning of diagnostic equipment (MRI)
MRI examination of stroke patients
Expensive (over 1 million $) -> high utilization
Demand uncertainties and demand diversity (both elective and emergency)
Goal: Reduce waiting time for stroke patients without degrading MRI utilization
Actual waiting times of 30-40 days for MRI examination
2 - 10 days with the optimized reservation and control strategy。
Monte Carlo optimization and dynamic programming approach for managing MRI examinations of stroke patients. IEEE Transactions on Automatic Control, 2011

- 14 -
Some funded projects
• Management of winter epidemics (flu, bronchitis, gastroenteritis) (ANR-TECSAN project HOST)
• Engineering home health care logistics (Rhone-alps Region, Labex IMOBS 3, St Etienne metropole)
• Performance modeling & evaluation of HIS (DGOS-PREPS e-SIS)
• CIFRE-Heva : Patient pathway mining with national database
• Care pathway of elderly people (Fondation Caisse d’Epargne)
• Spare care management of family caregivers (Fondation MSD-Avenir)
• CIFRE-Lomaco : Ambubalance network optimization
Past:
• FP6-IST6-IWARD on mobile & reconfigurable robots for hospital logistics.

- 15 -
Planning and optimisation of hospital resources
5-year project funded by Natural Science Foundation of China (2012-2016)
Consortium: IE, B. School, Ruijin hospital all from SJTU
Four major research tasks: Planning / scheduling of key clinical resources (human +
beds) Capacity planning / preventive maintenance of diagnostic &
treatment equipment Coordination / cooperation mechanism design Modelling / simulation of hospital emergency responses

- 16 -
Dynamic Daily Surgery Scheduling
Centre for Biomedical & Healthcare Engineering
Ecole des Mines de Saint Etienne, France
Centre for Healthcare Engineering
Dept. Industrial Engr. & Management
Shanghai Jiao Tong University, China
Xiaolan XIE

- 17 -
Basics of surgery scheduling

- 18 -
Importance of efficient surgery planning/scheduling
• Heart of a hospital involving nearly all medical specialties/units
• Relied on expensive skilled human resources and material resources
• About 10% of hospital budget
• Efficiency in terms of Cost-Quality-Delay is a must
• Mutation from a monospecialty with ad hoc organization to a multi-specialities with better organisation due to budget constraints and more strict safety regulations
• Health system reforms impose efficient management that the health professionals are not prepared and trained to

- 19 -
Overview of surgery patient journey
Patient arrivals Waiting
lists
Transfer
Leave the hospital
Surgery & Recovery

- 20 -
Patient perspective
• Elective patients = regular patients that can be planned
• Non elective patients = patients that arrive unexpectedly and have to be operated urgently
• Emergency patients = patients to be operated as soon as possible
• Urgent patients = patients to be operated in a short period
• Inpatients = patients requiring at least one-night hospitalization
• Outpatients = patients arriving & departing the same day
• Patient classification by DRG (Diagnosis Related Groups)

- 21 -
Health service perspective
• Presurgery: consultation, medical examination, …
• Surgery operations
• Post surgery: recovery and monitoring in wards
T1 T2 T3 T4 T5
Patient preparation Anaesthesia Surgery Bandage Cleaning
Patient arrival in OR
induction incision end of surgery OR available
Patient departure Surgeon time
Medical time
Patient sojourn time in OR
Total OR occupation time = Surgery time

- 22 -
Material resources perspective
Other material resources
Recovery rooms
Induction rooms
Stretchers
Obstetric labor rooms
Interventional radiology ORs
Emergency department
Sterilisations
Wards
Operating room (OR)
Operating theatre = set of ORs of a hospital

- 23 -
Human resources perspective
Surgeon = main operator
Anaesthesist
Surgery team = nurses of various skills assigned to an OR
Stretchers
Hospital attendants
Secretaries
Operating room (OR)

- 24 -
Performance mesure perspective
Resource utilization
• OR occupation
• Overtime
• Hospital revenue
Service quality
• Access time
• Waiting time

- 25 -
Operation decision perspective

- 26 -
Field observations of surgery scheduling

- 27 -
Ruijin Hospital (since 1907 by French missionaries)
Teaching hospital of the medical school of the Shanghai Jiao Tong University
Top 1 hospital in Shanghai
+12000 outpatient visits / day
A 23-floor outpatient consultation building

- 28 -
Field observation of the operating theatre of Ruijin Hospital
An integrated operating theatre of 21 OR and a second one recently constructed
60-70 elective surgery interventions + 10 emergency surgeries / day
No integrated surgery planning but each surgery speciality is given an amount of total OR time
Each speciality decides the surgeries to perform the next day
The operating theatre (OT) is responsible for daily OR assignment and the OR program execution.

- 29 -
Field observation of the operating theatre of Ruijin Hospital
Special features of the Ruijin Hospital
Queue of elective patients never empty
Availability of patients to be operated in short notice
Availability of surgeons to operate each day
Large variety of surgeons : top surgeons, senior surgeons, ordinary surgeons
Strong demand to operate at the OT opening in the morning to avoid endless waiting
Strong concern of OT personal overtime

- 30 -
Field observation of the operating theatre of Ruijin Hospital
Issues to be addressed
Promising surgery starting times to meet surgeon's demand for reliable surgery starting
(Tell me early enough when I start my surgery)
Surgery team overtime management
(How to guarantee the on-time end of duty of surgery teams?)
Outpatient surgery appointment when servers respond to congestion

- 31 -
Managing surgeon appointment times

- 32 -
Why surgeon appointments not used in practice
• Not used in practice to avoid potential OR capacity loss
Research question
How to provide surgeon appointment guarantee while ensuring appropriate OR capacity usage?
Observed Daily OR utilization
• But OR capacity usage is not always high over the day

- 33 -
Related work
Static scheduling for a single OR
Surgeon appointment scheduling (AS):
Two surgeries: AS solved by a newsvendor model (Weiss, 1990)
A fixed sequence of surgeries: stochastic linear program solved by SAA and L-shape algo to determine the allowance of each surgery, or equivalently, the arrival time (Denton 2003).
Others: discrete appointment (Begen et al, 2011), robust appointment (Kong et al, 2011)
Sequence scheduling: The problem is to jointly determine the position and arrival time of each surgery (Denton 2007; Mancilla 2012).

- 34 -
Related work
Dynamic scheduling for a single OR
Arrival scheduling: The demand of surgeries is uncertain, surgeries are processed as FCFS rule. The problem is to dynamically determine the arrival time upon each application(Erdogan 2011).
Sequence scheduling: The demand of surgeries is also uncertain. The problem is to jointly determine the position and arrival time of each surgery upon each application (Erdogan 2012).

- 35 -
Our focus
Multi-OR setting

- 36 -
Our focus
Multi-OR setting
Single-OR
Multi-OR
A1 A2 A3 An
A1/A2 A3 A4 An
No OR assignment
Dynamic OR assignment

- 37 -
Our focus
Two inter-related problems:
• Determining surgeon arrival times by taking into account OR capacities and random surgery durations.
• Dynamic surgeon-to-OR assignment of during the course of a day as surgeries progress by taking into account planned surgeon arrival times.

- 38 -
Assumptions of our work
A1: Emergency surgeries in dedicated ORs and hence neglected.
A2: Identical ORs and surgeries assignable to any OR.
A3: At most one surgery per surgeon each day.
A4: Promised starting or appointment time informed at the end of day D-1 (Surgeon appointment scheduling or proactive problem).
A5: Surgeons not available before the promised times.
A6: Dynamic surgery-to-OR assignment during the course of the day upon the surgery completion events.

- 39 -
Dilemma of promising surgery starting time
Promise too early
Surgery 1
promised start of surgeon 2
Surgery 2
Surgery 1
promised start of surgeon 2
Surgery 2
Promise too late
surgeon waiting
OR idle OR overtime
Easy if known OR time but OR times are uncerain

- 40 -
Data
J set of surgery interventions or surgeons
N number of identical ORs
T length of OR session
pi(ω) random duration of surgery i in scenario ω
bi unit time waiting cost of surgeon i
c1 unit OR idle time cost
c2 unit OR overtime cost
Similar to parallel machine scheduling but with planned job release dates and random service time.

- 41 -
Dynamic Surgery Assignment of Multiple Operating Rooms with Planned Surgeon Arrival Times
Zheng Zhang, Xiaolan Xie, Na Geng
In IEEE Trans. Automation Science and Engineering

- 42 -
Plan
Approximate optimal surgery start promising
Real time OR assignment strategies
Some numerical results
Conclusion and perspective

- 43 -
Decision variables
si promised surgery starting time of surgeon i Approximation assumption: fixed assignment & sequencing xir = 1/0 assignment of surgery i to OR r yij = 1 if surgery i precedes j in the same OR = 0 if not Auxiliary scenario-based random variables Cir(ω) completion time of surgery i on OR r Ir(ω) idle time of OR r Or(ω) overtime of OR r Wi(ω) waiting time of surgeon i

- 44 -
Model for promising surgery starting times
Assign each surgery to an OR ∑r xir = 1
Relation between assignment & sequencing yij + yji ≥ xir + xjr -1
Promised start before the end of the session si ≤ T
Scenario-dependent completion time xir pi(ω) ≤ Cir (ω)
Cir (ω) ≤ M xir
Cjr (ω) ≥ Cir (ω) + pj(ω) - M (1- yij) - M(2- xir - xjr )
Scenario-dependent OR idle time Cir (ω) ≤ Ir (ω) + ∑i∈J xir pi(ω)
Scenario-dependent OR overtime Or (ω) ≥ Cir (ω) - T
Scenario-dependent surgeon waiting time ∑r∈E Cir(ω) = si + Wi(ω) + pi(ω)
OR idle cost OR overtime cost
surgeon waiting cost
min Eω{c1 ∑r Ir(ω) + c2 ∑r Or(ω) + ∑i biIi(ω)}

- 45 -
Proposed solution
1. Convertion into mixed-integer linear programming model by Sample Average Approximation by using a given number of randomly generated samples
2. Heuristic for large size problem based on a) Local search for surgery-to-OR assignment
optimization b) Surgery sequencing rule based on optimal
sequencing of the two-surgery case c) Optimal promised start time by SAA and MIP

- 46 -
Plan
Approximate optimal surgery start promising
Real time OR assignment strategies
Some numerical results
Conclusion and perspective

- 47 -
Dynamic surgery assignment optimization
At time 0, start surgeries planned at time 0
At the completion time t* of a surgery in OR r*, select a surgery i* to be the next surgery in OR r* among all remaining ones J*
Surgery i* starts at time max{ t*, si* } in OR r* after the arrival of the surgeon at time si*
An Event-Based Framework

- 48 -
Dynamic surgery assignment optimization
Surgery i* is selected in order to minimize E[ TC(t*, i*, J*)] where E[ TC(t*, i*, J*)] is the minimal total cost similar to promised time planning model by conditioning on all completed surgeries and ages of
all on-going surgeries by scheduling i* as the next surgery on OR r*

- 49 -
Two-stage stochastic programming approximation
• At k-th surgery completion event at time tk
where J\J(k-1) is the set of remaining surgeries
• The first stage cost is the OR-idle or surgeon waiting cost induced by surgery l
• Θlk is the second stage cost, i.e. the total cost induced by remaining surgeries plus OR overtimes.
( )\ 1mink lk
l J J klkV g
∈ −= + Θ
( ) ( )ˆlk l k l k ls t t sg β+ += − + −

- 50 -
The second stage cost
( ) { }\ 1 \minlk jlk
j J J k lθ
∈ −Θ =
where • θjlk is the expected stage cost induced by surgery j
• if surgery l is selected at event k and surgery j at event k+1 Jensen's inequality is used to speedup the OPLA rule.
One-period look-ahead (OPLA) approximation

- 51 -
The second stage cost (cont'd)
Min. cost of two dynamic assignment rules: • Rule 1 (minimal stage cost first): Remaining surgeries assigned
in the scenario-independent order of minimal expected first stage cost, i.e. the surgery in selected at event n > k minimizes the stage n cost induced by in.
• Rule 2 (FCFS): Remaining surgeries are selected in non-
decreasing order of their surgeon arrival times si Jensen's inequality and another valide inequality are used to speedup the MPLA rule.
Multi-period look-ahead (MPLA) approximation

- 52 -
Lower bound of the dynamic surgery assignment
• Based on perfect information, i.e. all surgery duration realizations pj(ω) are known at the beginning of the day, i.e. randomness known at time 0+
• The lower bound problem is similar to the proactive problem but with
o given promised surgery start times
o scenario-dependent surgery assignment xir(ω) and sequencing yij(ω)

- 53 -
Dynamic surgery assignment policies
Policy Static: No real time rescheduling OR assignment / sequencing decisions of promised time
planning model are followed Policy FIFO: Dynamic surgery assignment in FIFO order of surgeon
arrival times Policy I: Dynamic surgery assignment optimization with OPLA Policy II: Dynamic surgery assignment optimization with MPLA

- 54 -
Plan
Approximate optimal surgery start promising
Real time OR assignment strategies
Some numerical results
Conclusion and perspective

- 55 -
Optimality gap
Observations
• Optimality gap is relatively small
• High surgery duration variation degrades the optimality gap
• High workload reduces the optimality gap
• MPLA better than OPLA
GAP = (costX- LB) / LB
(η,ρ%) GAPI(%) GAPII(%)
Ave. Min. Max. Ave. Min. Max. (0.3,0.75) 7.4 0.1 14.7 6.3 0.1 12.8 (0.7,0.75) 8.5 5.1 14.8 7.7 3.8 18.4 (0.3,1.25) 5.6 1.3 11.2 4.1 1.0 8.3 (0.7,1.25) 7.8 1.9 17.3 6.0 1.6 9.6
(80 3-OR instances)

- 56 -
Value of dynamic scheduling
OR# (η,ρ%) VDS (%)
Ave. Min. Max. 3 (0.3,75) 10.6 2.6 22.9
(0.7,75) 14.8 5.5 26.9 (0.3,125) 7.4 3.9 14.1 (0.7,125) 11.1 5.7 15.5
Ave. 11.0 4.4 19.9 6 (0.3,75) 25.4 18.7 31.6
(0.7,75) 29.2 24.7 39.9 (0.3,125) 11.1 7.1 15.5 (0.7,125) 19.1 12.8 24.1
Ave. 21.2 15.8 27.8 12 (0.3,75) 33.6 30.1 37.9
(0.7,75) 36.0 28.9 42.1 (0.3,125) 18.6 17.2 20.4 (0.7,125) 26.1 23.9 30.1
Ave. 28.6 25.0 32.6
Observations • Dynamic surgery scheduling always
helps.
• The benefit is more important for larger OT.
• Dynamic surgery scheduling is able to cope efficiently with surgery uncertainties.
• VDS decreases as the workload of OT increases.
η : variation parameter of surgery time ρ : workload
VDS = (costStatic - costDyna) / costStatic

- 57 -
Value of dynamic scheduling optimization
Observations • VOS increases as OR# increases.
• VOS increases as η increases, i.e. the variance of surgery durations increases.
• VOS decreases as ρ increases, i.e. the workload of OT increases.
OR# (η,ρ%) VOS (%)
Ave. Min. Max.
3 (0.3,75) 2.8 0.0 14.4
(0.7,75) 5.4 0.0 26.5
(0.3,125) 2.3 0.0 7.0
(0.7,125) 3.1 0.0 10.2
Ave. 3.4 0.0 14.5
6 (0.3,75) 5.4 -0.1 13.6
(0.7,75) 6.0 -0.1 11.3
(0.3,125) 2.9 0.0 5.0
(0.7,125) 5.0 0.6 8.7
Ave. 4.8 0.1 9.6
12 (0.3,75) 7.0 5.8 7.8
(0.7,75) 9.3 6.1 11.8
(0.3,125) 5.0 3.4 6.8
(0.7,125) 6.4 4.7 9.2
Ave. 6.9 5.0 8.9
η : variation parameter of surgery time ρ : workload
VOS = (costFIFO - costDynaOpt) / costFIFO

- 58 -
Value of proactive decisions
Observations • Proactive decision is very important to dynamic assignment scheduling.
• The arrival times that optimize the proactive model may not be adjustable to the dynamic assignment scheduling.
• Joint optimization of promised start times and dynamic assignment policies is an open research issue.
VOS = (costX - costX) / costX
where costX is the average cost of the strategy X but with promised start times determined with deterministic surgery duration.
(η,ρ%) VPSI(%) VPSII(%)
Ave. Min. Max. Ave. Min. Max. (0.3,0.75) 7.2 -15.2 23.3 7.0 -20.9 22.6 (0.7,0.75) 6.8 -11.1 20.4 6.4 -14.4 20.4 (0.3,1.25) 9.8 1.1 23.1 10.0 0.9 21.6 (0.7,1.25) 10.1 1.1 19.2 10.1 3.2 17.9

- 59 -
Plan
Approximate optimal surgery start promising
Real time OR assignment strategies
Some numerical results
Conclusion and perspective

- 60 -
Optimal surgery promised starting times for a given OR assignment / sequencing?
Features of surgeries planned to start at OR opening?
Time slacks in promised times vs surgery OR time and waiting cost?
Design of efficient optimization algorithms for promised time planning and real time rescheduling?
Promising time planning under starting time reliability constraints?
Open issues

- 61 -
Simulation-based Optimization of Surgery Appointment Scheduling
Zheng Zhang, Xiaolan Xie
in IIE Transactions

- 62 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 63 -
Our focus
Example :
1st released OR allocated to surgeon 3,
2nd released OR to surgeon 4, ....
Multi-OR
A1/A2 A3 r1
An
FCFS assignment
r2 A4
Surgeon appointment optimization for a given sequence of surgeries assigned to ORs on a FIFO basis.

- 64 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 65 -
Modeling
Parameters
n surgeries\surgeons
m ORs with regular capacity T for each OR
pi(ξ): surgery duration with known distribution
1 / α /βi: unit OR idling cost / overtime cost / surgeon waiting cost
Decisions
Surgeon arrival time A = [Ai] such that:
A1 = A2 = … Am = 0 ≤ Am+1 ≤ Am+2 ≤ … ≤ An

- 66 -
Modeling
Sample-path cost function
C[i](ω): i-th surgery completion event time.
C[i](ω) depends on A and ω and can be solved using a simple recursion.
[ ] ( )( ) [ ] ( )( ) [ ] ( )( )1
1 0( , )
n m
i i ii m i m n pi m p
f A C A A C C Tω β ω ω α ω−+ + +
− − −= + =
= − + − + − ∑ ∑
Waiting cost Idling cost Overtime cost

- 67 -
Modeling
Expected cost function
Objective
( )( ) ,g A E f Aξ ω=
1
min ( )
0, 1,...,, ,..., 1
A
i
i i
g A
A i mA
A A i m n
∈Θ
+
= = Θ = ≤ = −

- 68 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 69 -
Sample path analysis
LEMMA . The sample path cost function f(A,ω) is
• differentiable with probability 1 and
• Lipschitz-continuous throughout Θ with finite Lipschitz constant
1 2 1 2 1 2( , ) ( , ) , ,f A f A K A A A Aω ω− ≤ − ∀ ∈Θ

- 70 -
Sample path analysis
THEOREM 1 (unbiasednes of sample path gradient). The objective function g(A) is continuously differentiable on Θ, and the gradient of g(A) exists for all A∈Θ with
( ) ( ), ,A AE f A E f Aξ ξω ω∇ = ∇
The noisy sample-path gradient is on average correct!

- 71 -
Sample path analysis : partial derivative at interior point
\{ }
\{ }
\{ }
A:B:
C: 1
D: 1
i
i
i
i
jj BP i
ji j BP i
jj BP i
fA
β
β
β
α β
∈
∈
∈
−∂ = +∂ + +
∑∑
∑
Ai
i BP2(i) j
A.
B.
i
Ai waiting
i BP2(i) BP3(i)C.
Ai
i BP2(i) BP3(i)D.
Ai
waiting
waiting waiting
waiting waiting overtime
[i-m]1 …
[i-m]1 …
[i-m]1 …
[i-m]1 … BP4(i)
waiting
1 = unit OR idling cost
α = overtime cost
βi = surgeon waiting cost
Busy Period approach
A. i does not initiate BP(i)
B. i initiates BP(i) but not the last BP of the OR
C. i initiates the last BP of the OR without overtime
D. i initiates the last BP of the OR with overtime

- 72 -
Sample path analysis : directional derivative at boundary point
Boundary point A with Ak = Ak+1 = … = Al
( ) ( ) ( )
( ) ( ) ( )
( )( )
[ ][ ] [ ] ( ){ }[ ] ( ){ }
0
0
... , ,, lim
... , ,, lim
, if 0
, if 0
1 1 , if
1 0 , if
i
i
lk i
v jj i
ii l
u jj k
i i ii
i i
j j
j
j m j mj
f A e e f Af A
f A e e f Af A
x W
W
C T j n mx
W x j n m
ω ωω γ
ω ωω γ
β ωγ
β ω
β α ω
β ω
− ∆→=
∆→=
+ +
− ∆ − − ∆ −∇ = = −
∆
+ ∆ + + ∆ −∇ = =
∆
− == − > + + > > −=
+ > ⋅ ≤ −
∑
∑
Left-hand directional derivative
Right-hand directional derivative

- 73 -
Sample path analysis : improving direction
At an interior point, i.e. Ai-1 < Ai < Ai+1 At a boundary point A with Ak = Ak+1 = … = Al Select two surgeries i < j such that Determine the improving direction
( ),f A ω= −∇d
( ) ( ), 0, , 0i jv uf A f Aω ω−∇ < ∇ <
,..., ,0,...,0, ,...,i i j jv v u ud f f f f− −
= ∇ ∇ −∇ −∇

- 74 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 75 -
Stochastic approximation
( )1k k k kA A s d+Θ= Π +
( )
( )
where
is an improving direction according to sample-path gradient ,
= is a converging step-size
min is the orthogonal projection into the feasible set
k k
k
d f A
ask
ω
Θ
∇
Π = − Θy
x y x
Hill-climbing with noisy sample-path gradient

- 76 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 77 -
Convergence of stochastic approximation
BAD NEWS: The sample path cost function is not quasiconvex. Counter-example: p(ξ) = {9, 4, 4, 1}; 2 ORs, OR session T=10; idle time cost = 1; no overtime cost; Unit waiting cost β3=1, β4=3. Three arrival time vectors: A1=(0, 0, 4, 7.5) A2=(0, 0, 6, 8.5) A = αA1 + (1-α)A2
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
0 0,2 0,4 0,6 0,8 1
f(A, ω)
α

- 78 -
Convergence of stochastic approximation
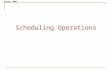
By randomly perturbing p around {9, 4, 4, 1}, we implement the stochastic approximation algorithm.
Evolution of arrival times visited by the stochastic approximation algorithm in Example 1, when applying it over 200 sample paths.

- 79 -
Convergence of stochastic approximation
Hopeful news: The sample path cost fuction f(A,ω) is strongly unimodal.
Properties verified experimentally:
• Unimodality of the expected cost function
• Convergence of the stochastic approximation algorithm.

- 80 -
Convergence of stochastic approximation: numerical evidence
Log normal distribution Uniform distribution
var, wkload 0.3,0.75 0.7,0.75 0.3,1.25 0.7,1.25 0.3,0.75 0.7,0.75 0.3,1.25 0.7,1.25
Initial dispersion
3-OR 5.0 4.9 6.5 7.0 5.4 4.8 6.6 6.8
6-OR 6.5 6.7 8.5 9.5 6.5 6.6 10.3 9.8
9-OR 8.0 7.4 11.2 10.5 7.9 7.7 10.5 10.5
Final dispersion
3-OR 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
6-OR 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
9-OR 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Final grad
3-OR 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
6-OR 0.0 0.0 0.1 0.1 0.0 0.0 0.1 0.1
9-OR 0.0 0.2 0.1 0.3 0.0 0.2 0.2 0.3

- 81 -
Allowances of Multi-OR vs single OR settings
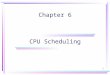
Optimal allowance shape dome shape in 1-OR, zigzag shape in 2-OR 2-OR vs 1-OR smaller allowances, half total allowance, highly uneven Increasing surgery duration variability (o vs o) smoothing 2-OR allowances, increasing 1-OR allowance variability Higher waiting cost (o vs o) larger allowances in both settings but rather insensitive in the 2-OR setting

- 82 -
Allowances vs OR#
Zigzag shape
1 large allowance followed by m-1 small allowances
Total m-OR allowance = 1/m of total-1-OR allowance
Higher OR# and higher duration variation → smoother allowances

- 83 -
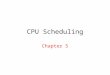
Allowances vs OR#
Two-parameter heuristic
Larger 1st allowance followed by constant allowances

- 84 -
Value of dynamic assignment and proactive solution
Three strategies Strategy I : no dynamic surgery-to-OR assignment Strategy II : same appointment times, FIFO surgery-to-OR assignment Strategy III : same surgeon arrival sequence, FIFO surgery-to-OR assignment, simulation-based optimized appointment times Value of dynamic assignment (VDA) percentage improvement of strategy II over strategy I Value of proactive anticipation and dynamic assignment (VPD) percentage improvement of strategy III over strategy I

- 85 -
Value of dynamic assignment and proactive solution
VDA > 0, VPD > 0 , VPD > VDA : dynamic assignment and the proactive anticipation of dynamic assignments always pay
Higher OR number : increasing VDA and VPD due to scale effect and benefit of well planned arrivals. Higher duration variability: increasing VDA and VPD implying the importance of careful appointment planning and dynamic scheduling. Higher waiting costs: higher VPD but smaller VDA implying the importance of appointment time optimization. Higher workload: smaller VPD and VDA due to unimprovability of overloaded syst Impact of case-mix: • larger VPD when surgeries are identical due to their interchangeability. • smaller VDA when surgeries are identical due to suboptimal appointment times
Value of dynamic assignment (VDA) Value of proactive anticipation and dynamic assignment (VPD)

- 86 -
Outline
• BACKGROUND AND MOTIVATION
• SURGERY APPOINTMENT SCHEDULING PROBLEM
• SAMPLE PATH ANALYSIS
• STOCHASTIC APPROXIMATION
• NUMERICAL EXPERIMENTS
• CONCLUSION AND PERSPECTIVE

- 87 -
Summary
A more realistic model of AS which has m servers; patients are served in a pre-determined order but are flexible to any server.
Our aim is to proactively optimize the arrival times under the FCFS dynamic assignment strategy.
We formulate a simulation-based optimization model to smooth integer
assignments, and derivate a continuous and differentiable cost function. The proposed stochastic approximation algorithm is able to solve
realistic-sized instances and significantly improve the initial solution.

- 88 -
Managing surgery team overtime
“Branch and Price for Chance Constrained Bin Packing”
Zhang, Denton, Xie
submitted

- 89 -
Motivation
ORs: critical resources that require high utilization
Unpredictable overtime causes high nurse turnover rate
Nurses ask for ...
• Some ORs to have low overtime
• Predictable completion times
Challenges: • Fixed number of ORs • Uncertain service time • High cost of overtime

- 90 -
A chance constrained OR scheduling setting
Chance constraint (δr , α) of an OR r
The surgery team of the OR r completes its daily due before time T + δr with probability α
where
Τ = regular OR session time (T)
δr = allowable overtime
Chance constraint = End-of-duty guarantee
Examples: No overtime with proba 90% : δr = 0, α = 0.1
at most 1h overtime with proba 95% : δr = 1, α = 0.05

- 91 -
A chance constrained OR scheduling setting
An informal setting
Decisions: Surgeries-to-ORs assignment Constraints: For each chance constrained OR:
P(OR overtime ≤ δk) ≥ 1 - α
Objective: Minimize the expected overtime
A version of chance constrained extensible bin-packing problem

- 92 -
A stochastic programming formulation
Decision variables:
(1a) = Minimize total expected ovetime
(1b) = Assign each surgery to an OR
(1c) = Determine the overtime
(1d) = Chance constraints
I, R set of surgeries and set of ORs
di(ω) duration of surgery i under scenario ω
T regular OR session time
set of ORs of chance constraint k
xir binary var equal to 1 if surgery i is assigned to OR r
or(ω) overtime of OR r under scenario ω
Defining elements:
CkR

- 93 -
Solving Stoch. Prog. formulation: Branch-and-Price
Master problem
Decision variables
p column containing surgeries to be allocated in the same OR
λp binary var equal to 1 if the column p is selected

- 94 -
Solving Stoch. Prog. formulation
Key ideas of branch-and-price
1. Branch on constraints
• Select a pair: (i, j )
• Left side (in the same bin): yip = yjp
• Right side (in separate bins): yip + yjp ≤ 1
2. Enforcing the antisymmetry constraints due to identical ORs

- 95 -
Solving Stoch. Prog. formulation
Pricing problem
Decision variables
yip binary var equal to 1 if surgery i is in column p
ckp binary var equal to 1 if column p is type-k chance constrained
op(ω) overtime of column p
Stochastic knapsack problem

- 96 -
Solving Stoch. Prog. formulation
Pricing problem solution acceleration
• Tight lower bound by replacing the chance constraint by Cvar (Conditional Value at Risk) reformulation with convex recourse
• Tight upper bound with probabilistic covers and probabilistic packings (Song et al., 2014).
( ) ( ) ( )( )( ) ( ) ( )
( )
Chance constraint
1- inf 1-
1inf
= convex set
k k
k kz
k
P X T VaR X z P X z T
VaR X T CVaR X z E X z T
CVaR X T
δ α α δ
δ δα
δ
+
≤ + ≥ ↔ ≤ ≥ ≤ +
≤ + ← = + − ≤ +
≤ +

- 97 -
Robust optimization formulation
Assumptions:
A1. Given first two-moments (mi, σi) of surgery durations.
A2. Unknown probability distributions of surgery durations.
Chance constraints replaced by worst-case chance constraints:
where D is the set of all distributions matching the first two moments:
inf 1i ir kD i IP d x T δ α
∈∈
≤ + ≥ − ∑d
[ ]{ }2 2 2,i i i i iD E d m E d m σ = = + d

- 98 -
Robust optimization formulation: key result
Theorem: For any random variable X of mean m and standard deviation s, the worst-chance probability CP is reached by a three-point distribution such that
( )( )
( )
22 2
22
2 2
1, if
, if ,
, if ,
k
k kk
k kk
m T
CP m T m m TT m
m m T m m TT
δ
σ δ σ δσ δ
δ σ δδ
> += ≤ + + ≤ +
+ + − ≤ + + > +
+
Under the mild assumption CV≤ (α-1 – 1)0.5,
the robust optimization formulation can be converted into a deterministic mixed-integer-programming model.

- 99 -
Case study
• Experiments are based on real data of 21 surgical days.
• Number of ORs: m = 3 + 3 + 3; OR session time T = 10h; Overtime threshold dk ∈ {0.0; 2.0h; ∞}.
• Number of surgeries: dk ∈ [11; 37].

- 100 -
Performance of Branch-and-Price
Performance of different methods for the stochastic model
• Simple size: 500 • Computation time limit: 15,000 seconds. • Probability guarantee: 1 - α = 0.9.

- 101 -
Value of Robust Optimization
Worst-case probability
Experimental setting: 1- α = 0.9 (stochastic), 1- α = 0.9 (robust), n [21; 25]
• Extensive form of robust optimization can be solved by Cplex • The unachieved probability of stochastic solution could be 0.16 • The average overtime of robust solution could be 2 times higher
Average overtime
90%

- 102 -
Value of Robust Optimization
Worst-case probability
Experimental setting: 1- α = 0.9 (stochastic), 1- α = 0.7 (robust), n [21; 25]
• More robust solution with slighter higher overtime
Average overtime
90%

- 103 -
Conclusions
• The Branch-and-price can effectively solve the real-size problem instances
• The robust optimization problem can be much easier to solve than the stochastic problem
• The robust optimization can provide more robust solution with slightly higher overtime

- 104 -
Accounting for congestion behavior in appointment scheduling
“Appointment Scheduling Problem When the Server Responds to Congestion”
Zhang, Berg, Denton, Xie
Submitted

- 105 -
Evidences from the literature
• Outpatient clinic: physicians tend to speedup when they perceive congestion in the waiting area (Rising et al. 1973; Cayirli et al. 2008);
• Emergency department: triage-ordered testing and task reduction are used to reduce service time (Batt and Terwiesch 2012);
• ICU/ED: delays in receiving intensive care can result in longer lengths of stay in the ICU (Chan et al. 2015).

- 106 -
An outpatient procedure case
• Data for a one year period
• Samples are classified by surgeon and procedure type
• Specific records on patient waiting time, pre-procedure time, procedure time and post-procedure time.
We look at the impact of waiting time on different service times

- 107 -
A case in the context of outpatient procedures
• Negative correlation Between pre-procedure time and waiting time
• No correlation between procedure time, post-procedure time and waiting time

- 108 -
Related work
• Although there is a vast literature on appointment scheduling, none of the existing studies considered endogenous randomness.
• Congestion was incorporated in queuing models by Chan et al (2014), Vericourt and Jennings(2011), …
• However, appointment systems have a little number of customers and they need to determine arrival times.

- 109 -
Research questions
• Can the appointment scheduling problem be solved when the endogenous randomness is incorporated?
• How important is it to anticipate a congestion response from the server when scheduling appointments?
• Why is the dome shaped rule that is claimed "optimal", in practice, not widely implemented?

- 110 -
Problem setting
A1/A2
FCFS assignment
Appointment optimization
for a given sequence of customers
to a single server system with congestion response behaviour
in order to minimize the total cost related to
• Customer waiting (lower service quality)
• Service time reduction (lower quality service)
• Overtime.

- 111 -
Problem setting
A1/A2
FCFS assignment
Decision variables:
xi = customer-i allowance or interarrival time between i-1 and i
( ) ( ) ( )( ) ( )
( ) ( ) ( )( )( ) ( ) ( )( )
( ) ( ) ( )
2 2
1 1
2
min
, ,
, , , ,
,
n nw s oi i i i i
i i
i i i i
i i i i
n
i n ni
E c w c Z d c o
w w Z x i
Z f w d i
o x w Z T
ω ω ω ω
ω ω ω ω
ω ω ω ω ω
ω ω ω ω
= =
+
+ +
+
=
+ − +
= + − ∀
= ∀
= + + − ∀
∑ ∑
∑
( )( )( ) ( )
: waiting cost
: service reduction cost
: overtime cost: normal service time
: actual service time
, ,
wisio
i
i
i i i i
c
c
cd
Z
Z f w d
ω
ω
ω ω=

- 112 -
Problem setting : congestion behavior models
A1/A2
FCFS assignment
Linear response model

- 113 -
Problem setting : congestion behavior models
A1/A2
FCFS assignment
Logic Regression response model
( ) ( ) ( )2
11 i
ii i i w
Z de ω
θω ω θ
−
= + − +

- 114 -
Problem setting : congestion behavior models
A1/A2
FCFS assignment
Linear response model with customer no-show
( ) ( ) ( ) ( )
( )[ ] ( )
0, if no-show
1 , if show and
1 , if show and
ii i i i i
i
i i i i
Z d w w tt
d w t
θω ω ω ω
ω θ ω
= − <
− ≥

- 115 -
Solution approaches
Under mild continuity condition of the server reponse model,
• Stochastic-optimization with unbiased sample path gradients
Under linear response model
• Stochastic linear Mixed Interger Programming

- 116 -
Computational results : Comparison of SimOpt and SMIP
• Identical customers
• 500 samples are used for the SMIP, and 107 samples for the SimOpt.
• Costs are evaluated based on 106 samples.
• The SimOpt is much more efficient than solving the SMIP
• Across all instances, the SimOpt solved the global optimum

- 117 -
Computational results : Solution
• Allowances increase with variability and waiting cost
• Congestion reduces allowances
• Congestion makes allowances more flat

- 118 -
Computational results : comparison with heuristics
• Our method always finds the best solution
• Mean-value solution may outperform the Dome solution when congestion occurs

- 119 -
Computational results : comparison with heuristics
• Our method always finds the best solution
• Mean-value solution may outperform the Dome solution when congestion occurs

- 120 -
Conclusions
• Simulation-based Optimization can efficiently solve the congestion anticipated AS problems
• Variability and waiting coefficient affect the allowance and cost, while congestion behavior helps to lower the cost and smooth the allowances
• Ignoring the congestion is costly; the dome-shaped solution may perform worse than the mean-value solution

- 121 -
General conclusions

- 122 -
What next?
Joint optimization of surgery sequence and surgeon appointment times.
simulation-based discrete optimization + stochastic approximation
Chance constraints of surgery starts
Dynamic control of overtime allocation
Surgeon behavior
Joint scheduling of inpatient and day surgeries

- 123 -
Relevant previous work
Planning operating theatres with both elective and emergency surgeries
M. Lamiri, X.-L. Xie, A. Dolgui and F. Grimaud. "A stochastic model for operating room planning with elective and emergency surgery demands", European Journal of Operational Research, Volume 185, Issue 3, 16 March 2008, Pages 1026-1037
Mehdi Lamiri, Xiaolan Xie and Shuguang Zhang, "Column generation for operating theatre planning with elective and emergency patients," IIE Transactions, 40(9): 838 – 852, 2008
M. Lamiri, F. Grimaud, and X. Xie. “Optimization methods for a stochastic surgery planning problem,” International Journal of Production Economics, 120(2): 400-410, 2009