Embed Size (px)
Citation preview

1
Interprofessional Geriatrics Training ProgramInterprofessional Geriatrics Training Program
HRSA GERIATRIC WORKFORCE ENHANCEMENT FUNDED PROGRAM Grant #U1QHP2870
Drug Therapy in Older Adults
EngageIL.com
Author: Michael Koronkowski, PharmD, CGP
Contributor: Joseph T. Hanlon, PharmD, MS
Editors: Valerie Gruss, PhD, APN, CNP-BC
Memoona Hasnain, MD, MHPE, PhD
Expert Interviewee: Todd Semla, MS, PharmD, BCPS, FCCP, AGSF
AcknowledgementsAcknowledgements
• Mrs. Roberts is a 77-year-old widow who lives alone
• She has multiple medical problems, which include: chronic obstructive
pulmonary disease (COPD), hypertension (HTN), diabetes (DM), coronary artery
disease (CAD), cerebral vascular accident (CVA), osteoporosis, osteoarthritis,
gastroesophageal reflux disease (GERD), anxiety, insomnia, allergic rhinitis,
glaucoma, multiple falls at home, and currently smokes 4 cigarettes/day
• Though she has prescription insurance (Medicare Part D), she has difficulty
affording her monthly copayments
• She tries to take her medications as prescribed, but she misses doses
Case: Medication Therapy in Older AdultsCase: Medication Therapy in Older Adults

2
• She is currently taking 21 medications, which include:
• Budesonide/formoterol, albuterol, amlodipine, insulin glargine, insulin
aspart, sitagliptin, alendronate, acetaminophen, diclofenac gel,
glucosamine, meclizine, omeprazole, mirtazapine, zolpidem, trazodone,
diphenhydramine, fluticasone, estrogen vaginal cream, triamcinolone
cream, and timolol eye drops
Case: Medication Therapy in Older AdultsCase: Medication Therapy in Older Adults
Upon completion of this module, learners will be able to:
1. Recognize the common consequences of inappropriate medication use and polypharmacy
2. Describe the key principles of pharmacology and the effects of age on medication use
3. Summarize the main approaches to improve medication prescribing and monitoring
4. Describe a stepwise approach to integrating into practice a process for prescribing and monitoring medications
5. Identify provider and patient resources to support drug prescribing and monitoring medications
Learning ObjectivesLearning Objectives
Mrs. Roberts’ Case (Continued)
• In addition to the 21 medications she has been prescribed, Mrs. Roberts has
symptoms that drive many older adults to seek self-care strategies
• This adds to the pill burden, and often the other needs go unrecognized
• Mrs. Roberts’ case exemplifies the challenges of managing clients with
multiple chronic conditions and multiple drug therapies
• Merely using current clinical practice guideline-directed care would result
in 12 medication recommendations and a complex drug regimen
Case: Medication Therapy in Older AdultsCase: Medication Therapy in Older Adults

3
Mrs. Roberts’ Case (Continued)
• Mrs. Roberts may have medication-related problems, given the regimen
complexity, such as:
• Adverse drug events
• Drug duplication
• Nonadherence with possible negative outcomes
• One other aspect of this complex regimen is financial toxicity
• The estimated cost per month is $2,000 for these medications, with
insurance only covering a percent of that total cost
Case: Medication Therapy in Older AdultsCase: Medication Therapy in Older Adults
Mrs. Roberts’ Case (Continued)
• Practice implications:
• What concerns would you have about this older adult with respect to
medication prescribing and medication-taking behavior?
• What is the role of shared decision-making in the medication
management for Mrs. Roberts?
Case: Medication Therapy in Older AdultsCase: Medication Therapy in Older Adults
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults

4
• Medications, including prescription, over-the-counter, and herbal
preparations, are widely used by older adults
• Prescription use of multiple medications has increased between
2005-2006 and 2010-2011
• The number of older adults taking 5 or more prescription medications
has increased from 31% to 36%
• These rates increased from 53% to 67% when over-the-counter
medications and dietary supplements were included
• 15% are potentially at risk for a major drug-drug interaction
Medication Use in Older Adults: OverviewMedication Use in Older Adults: Overview
(Qato et al., 2008, 2016)
• These results are consistent with a large body of research that has documented
a seemingly inexorable rise in medication use among older adults (Greenhalgh et al., 2014)
• However, there are people with multiple chronic conditions who can benefit
from multidrug therapies (Steinman et al., 2011)
• Older adults can be taking more than just what they are prescribed:
• 25% of older adults do not report the herbs and supplements they are
taking to their prescriber (Nahin et al., 2009)
• A complete medication history is essential as a starting point for an
accurate best medication list (Steinman et al., 2011)
Medication Use in Older Adults: OverviewMedication Use in Older Adults: Overview
Practice Implications:
• The presence of polypharmacy and the multiple sources of medications that
contribute to it often go unrecognized
• Perform a medication review annually and each time a new medication is
started or a dosage is changed
• Medication reviews must assess for both:
• Prescription
• Over-the-counter supplements and herbal medications
Medication Use in Older Adults: OverviewMedication Use in Older Adults: Overview

5
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Drug-Drug Interactions
• Taking 5-9 medications has a 50% chance of drug-drug interactions (Doan et al., 2013)
• At 20 more medications, this risk increases to 100% (Doan et al., 2013)
• Medications interact with each other throughout the process of absorption,
distribution, metabolism, and elimination
• This may result in reduced efficacy and therapeutic effects or overdose and
toxicity
• Drug-drug interactions are a frequent cause of medication-related
complications, such as hospitalizations
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Drug-Drug Interactions (Continued)
• Mrs. Roberts screens in for 7 drug-drug interactions: 5 severe, and 2 moderate
• She is at 100% risk of having drug-drug interactions
• Drug effects may be altered by pre-existing disease or health problems
• Diseases may be aggravated by the new drugs prescribed
• For instance, nonsteroidal anti-inflammatory drugs (NSAIDs) and salicylates
can exacerbate peptic ulcer disease
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Drug-Food Interactions
• Often, nutrition and nutritional supplements may interact with the absorption
of drug therapy
• Mrs. Roberts screens in for two drug-food interactions
• Medicine for osteoporosis has to be taken first thing in the morning on an
empty stomach, with no food at all
• Antidepressants interact with certain nutrients, such as grapefruit juice
• Potassium-rich food consumption may increase the risk of hyperkalemia
when potassium-sparing diuretics or angiotensin inhibitors are prescribed
(Schmidt & Dalhoff, 2002)

6
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Practice Implications:
• Screen for drug interactions and reduce polypharmacy
• Refer to the 2015 Beers Criteria to learn more on significant interactions
impacting the older adult
• www.geriatricscareonline.org/toc/american-geriatrics-society-updated-
beers-criteria-for-potentially-inappropriate-medication-use-in-older-
adults/CL001
• Be aware of drug-disease and drug-food interactions
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Prescribing Cascade
• Older adults with dementia are at risk for prescribing cascades
• Like a domino effect, the initial drug is prescribed, then an adverse event
occurs, followed by subsequent drug therapy
(Gill et al., 2005)
Expert Interview: Todd Semla, MS, PharmD, BCPS, FCCP, AGSF
Expert Interview: Todd Semla, MS, PharmD, BCPS, FCCP, AGSF

7
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:
• Do physicians often prescribe medications to treat side effects of other
medications?
• Sometimes it cannot be avoided
• If a patient is taking a diuretic for high blood pressure and it causes
them to lose potassium, the patient then needs to be placed on a
potassium supplement or potassium-sparing diuretic
• That is polypharmacy, but it is acceptable
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:
• Do physicians often prescribe medications to treat side effects of other medications?
• Sometimes it should be avoided:
• A patient may suddenly develop dizziness from a medication, but the provider does not recognize the dizziness as being medication-related, as it is often attributed to older age
• A provider can put the patient on another medication that is supposed to fight the dizziness
• This can compound the patient’s dizziness or increase their risk of falling, which is a negative outcome
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Nonadherence
• Nonadherence is quite common with complex drug regimens (Steinman & Hanlon, 2010)
• Polypharmacy results in potential sources of drug duplication, medication
changes, errors, confusion, shifting doctors, multiple prescribers, and
care transition medication errors (Fried et al., 2014; Lu et al., 2015)
• Almost half of the older population experiences adherence problems (Osterberg & Blaschke, 2005)

8
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:
• Addressing issues of nonadherence:
• The assumption tends to be, “the older you are, the more likely you are to
be nonadherent”
• Older adults have more opportunities for nonadherence, as they tend to
take more medications
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:• Are patients honest about their adherence patterns?
• Probably not:• Patients do not want to disappoint their doctor• Patients are hesitant to ask questions
• Practice implications of nonadherence:• Practitioners should have a list of medications that the patient is
supposed to be taking• Practitioners should have the medications that patients are taking in
front of them, and should ask about the absence of medications• Can find out that patients have stopped taking certain medications
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:• Practice implications of nonadherence (continued):
• Important for patients to understand the importance of adherence for certain medications• For example, with bisphosphonate, one of the drug classes used to
prevent or treat osteoporosis, if a patient does not take 80% of their medication, then it is like they are not taking the medication at all
• Fairly rigorous medication regimen:• Patient must get up 30 minutes before they would normally get up,
take the medication with a full glass of water, not go back to bed or eat anything for at least a half an hour, and cannot lay down in order for the drug to be absorbed

9
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:• Practice implications of nonadherence (continued):
• It is difficult to take the medication, but if the patient does not take it correctly or takes 80% or less of their doses, then it is like not taking the medication at all, so the patient is wasting any effort they put into their regimen
• Adherence:
• Has to be individualized and customized based upon why the patient is not taking their medication
• Adherence problems cannot be solved simply by education, by using a pill box, or by scolding
PolypharmacyPolypharmacy
Practice Implications of Nonadherence:
• Maintain heightened vigilance regarding adverse drug effects
• Be alert to the problem of nonadherence
• Inquire at each and every visit
Expert Interview: Todd SemlaPolypharmacy
Expert Interview: Todd SemlaPolypharmacy
Listen to Our Expert Discuss:
• How do you know when a medication may be the culprit in terms of causing an
adverse effect or complaint the patient has?
• Older adults’ exposure to medication is so great, and medication-induced
problems occur in up to a third to fifty percent of people at any given time
• Have this always in your mind
• Have a current list of their medications
• Determine if this a potential adverse effect of one or more of the medications,
either alone or in combination

10
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Increased Hospitalization Rate
• In the U.S., it is estimated there are ~100,000 emergency hospitalizations due
to medications, with two-thirds of these due to unintentional overdoses in
older adults
• 67% of medication-related hospitalizations are due to insulin, oral
hypoglycemic agents, warfarin, and antiplatelet drug classes
(Budnitz et al., 2011)
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Increased Cognitive Impairment
• Cumulative exposure to medications with anticholinergic burden is associated
with an increased risk of incident dementia or increased cognitive impairment (Gray et al., 2015)
• Common medication classes with anticholinergic activity include:
• Antihistamines, antimuscarinics, antiemetics, antipsychotics, and
tricyclic antidepressants (American Geriatrics Society, 2015)
PolypharmacyPolypharmacy
Practice Implications:
• Reduce polypharmacy and closely monitor higher risk drug classes
• Medication reviews and avoidance of medications with high anticholinergic burden can minimize the risk of increased cognitive impairment
• Compared to more robust peers, frail older people display pronounced changes in response to medications, which affects drug choice, dose and frequency
• Assess kidney function before prescribing renally excreted medicines, and continue to monitor throughout the course of therapy
• Avoiding new medications and stopping unnecessary prescriptions are the only means to reduce polypharmacy

11
PolypharmacyPolypharmacy
Listen to Our Expert Discuss:
• Other actions clinicians should perform on an annual basis:
• Review all of your patient’s medication, particularly before prescribing a new medication
• Ensure people understand what their medications are for, so they are not, for instance, confusing their diabetes medication for their heart medication
• Make sure they understand how to take their medication, what time, and how often to take it
• Determine if the medication is causing an existing harm, or setting the patient up for a future harm, such as a fall, leading to a negative outcome
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Increased Falls and Hip Fractures
• Falls represent a major quality of life issue for the older adult
• Falls can result in a fracture, head trauma, or soft tissue trauma
• They result in tremendous morbidity and mortality
• In addition, the impact can increase anxiety and fear from possible future falls
• Risk of falls in patients taking ≥ 6 medications was 3.0-fold higher (Chiu et al., 2015)
• Polypharmacy is an independent risk factor for hip fractures (Lai et al., 2010; Pan et al., 2014)
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Increased Falls and Hip Fractures (Continued)
• Common medication classes that increase falls include:
• Sedative hypnotics
• Benzodiazepines
• Anxiolytics
• Antidepressants
• Opioids
• Antipsychotics
Practice Implication:
• Caution is required when prescribing medications that increase fall risk
(American Geriatrics Society, 2015)

12
Polypharmacy Consequences in Older AdultsPolypharmacy Consequences in Older Adults
Problem: Palliative Care
• The problem of polypharmacy may be troublesome in patients with limited life expectancy
• Most drugs bear little to no relation to the actual needs of patients in end of life situations
• Medication management should be based on “palliative principles” (Cruz-Jentoft et al., 2012)
• Revise the therapeutic objectives for each condition and adapt treatments(Holmes et al., 2006)
Practice Implication:
• Deprescribe medications based on shared decision-making and comfort care goals
Mrs. Roberts is on a complex daily medication regimen to manage
her multiple chronic conditions. What negative consequence(s) is
she at considerable risk for? (Check all that apply)
a) Nonadherence
b) Decreased hospitalization
c) Increased cognitive impairment
d) Increased falls
Assessment Question 1Assessment Question 1
Mrs. Roberts is on a complex daily medication regimen to manage
her multiple chronic conditions. What negative consequence(s) is
she at considerable risk for? (Check all that apply)
a) Nonadherence (Correct Answer)
b) Decreased hospitalization
c) Increased cognitive impairment (Correct Answer)
d) Increased falls (Correct Answer)
Assessment Question 1: AnswerAssessment Question 1: Answer

13
Mrs. Roberts is currently prescribed 21 medications to manage her
multiple chronic conditions. What is the LIKELIHOOD of a
drug-drug interaction occurring with the use of these medications
concomitantly?
a) 100%
b) 50-75%
c) 25-50%
d) 0%
Assessment Question 2Assessment Question 2
Mrs. Roberts is currently prescribed 21 medications to manage her
multiple chronic conditions. What is the LIKELIHOOD of a
drug-drug interaction occurring with the use of these medications
concomitantly?
a) 100% (Correct Answer)
b) 50-75%
c) 25-50%
d) 0%
Assessment Question 2: AnswerAssessment Question 2: Answer
Impact of MedicationImpact of Medication

14
• Adverse events are quite common in older adults and occur across care settings
• 35% of ambulatory older people and two-thirds of nursing home residents
experience adverse events (Hanlon et al., 1997; Cooper, 1999)
• Taking more medications increases the risk of adverse events 2.3-fold (Ahmed et al., 2014)
Practice Implication:
• Reduce polypharmacy and closely monitor for drug risk [not stated verbatim in film]
• It is important that health providers ask about problems with
medications at each visit, communication, or care transition
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
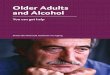
Drug Class Implicated Incidence of Adverse Events (n = 815)
Warfarin 15%
Atypical antipsychotics 11%
Loop diuretics 8%
Opioids 6%
Antiplatelet 6%
Angiotensin inhibitors 6%
Antidepressants 5%
Laxatives 5%
Benzodiazepines 5%
Insulins 5%
(Gurwitz, 2005, p. 255)
• Mrs. Roberts has polypharmacy, which increases her risk for adverse drug events
• In addition, she is on various drug classes, implicated to cause a greater incidence of adverse events, specifically antiplatelet, trazodone, mirtazapine, insulin, and sedative zolpidem, a non-benzodiazepine that works on the GABA receptor
Practice Implication:• Providers should assess for adverse drug events especially in these
particular drug classes and at care transitions (see list of drug classes on the previous slide)
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications

15
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
Prescribing for Older Patients Presents Unique Challenges:
• Pre-marketing drug trials often exclude geriatric patients
• Approved doses may not be appropriate for older adults
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
• Many medications need to be used with special caution because of age-
related changes in pharmacokinetics, such as:
• Absorption
• Distribution
• Metabolism
• Excretion
• Changes in pharmacodynamics, or the physiologic effects of the drug,
can also occur
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
• Physiologic effects are seen as decline in organ function, reserve, and resilience
• Pharmacokinetic changes are commonly manifested as impaired renal function
or altered liver metabolism
• Pharmacodynamic changes create altered receptor and target organ responses
• Particular care must be taken in determining drug dosages when prescribing for
older adults

16
Adverse Drug Events: Impact of MedicationsAdverse Drug Events: Impact of Medications
• Mrs. Roberts is at increased risk for slow drug clearance, drug
accumulation, and drug toxicity based on the common age-related
changes that impact drug therapy
• Most importantly, adjustments based on kidney function are necessary
• Frail older people are more affected by physiologic, pharmacokinetic,
and pharmacodynamic changes
Based upon your understanding of age-related changes that occur in
older adults, which of the following factors is MOST LIKELY to
contribute to an increased risk for slow drug clearance and drug
accumulation for Mrs. Roberts?
a) Age
b) Polypharmacy
c) Kidney function
d) Concurrent disease states
Assessment Question 3Assessment Question 3
Based upon your understanding of age-related changes that occur in
older adults, which of the following factors is MOST LIKELY to
contribute to an increased risk for slow drug clearance and drug
accumulation for Mrs. Roberts?
a) Age
b) Polypharmacy
c) Kidney function (Correct Answer)
d) Concurrent disease states
Assessment Question 3: AnswerAssessment Question 3: Answer

17
Prescribing in Clinical PracticePrescribing in Clinical Practice
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• Research demonstrates improvements in reducing inappropriate prescribing
• However, mixed trial results exist on the overall impact on polypharmacy,
drug utilization, cost, and important long-term health care outcomes
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• Multiple factors contribute to the appropriateness and overall quality of drug prescribing, including:
• Avoidance of inappropriate medications
• Appropriate use of indicated medications
• Adherence
• Monitoring for adverse effects and drug concentrations
• Avoidance of drug-drug interactions
• Involvement of the patient
• Integration of patient values

18
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• Measures of the quality of prescribing often focus on one or some of these factors, but rarely on all
• Furthermore, the predictive value of these measures of quality of prescribing in determining important long-term outcomes of care have not been determined
• Approaches to decrease inappropriate prescribing in older adults include:
• Educational interventions
• Computerized order entry and decision support
• Multidisciplinary team care led by physicians and clinical pharmacists
• Combinations of these approaches
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• Available data for these interventions generally show significant
improvements in reducing inappropriate prescribing, but mixed results for
health outcomes or costs (Alldred et al., 2016; Spinewine et al., 2007)
• Physician order entry with clinical decision support showed a mixed effect on
reduction in adverse drug events (ADEs) (Wolfstadt et al., 2008)
• Five studies showed a statistically significant reduction in ADEs
• Four studies showed a nonsignificant decrease
• One study showed no impact on the rate of ADEs
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• Prescribing for older patients is an extraordinarily complex endeavor
• However, as illustrated by the case of Mrs. Roberts, a thoughtful, systematic
approach to addressing the medication regimen should help to make a
meaningful difference in her outcomes

19
Measuring Quality of Drug TherapyMeasuring Quality of Drug Therapy
• The success of her care is not knowing the right answer for her from the
beginning, but rather from using a careful, stepwise process that merges key
principles of pharmacologic care with the clinical reality, social situation, and
goals of care of the patient (Steinman et al., 2011; Steinman & Hanlon, 2010)
• Efforts to integrate team-based care, involve social supports, and maximize
patient empowerment will enable Mrs. Roberts to remain active and in the
community (Steinman et al., 2011; Coleman et al., 2006)
The Beers CriteriaThe Beers Criteria
• The Beers Criteria are increasingly being used to monitor quality of care for
older adults in the U.S.
• The validity of these consensus-derived criteria in predicting adverse outcomes
is becoming increasingly more important
• Studies of earlier versions of the Beers Criteria did predict adverse outcomes,
but some medications not on the earlier criteria correlated more closely with
adverse outcomes
(American Geriatric Society, 2015)
Expert Interview: Todd Semla, MS, PharmD, BCPS, FCCP, AGSF
Expert Interview: Todd Semla, MS, PharmD, BCPS, FCCP, AGSF

20
Listen to Our Expert Discuss:
• What is the purpose of the Beers Criteria?
• Main purposes:
• To serve as a guidance for clinicians in terms of how to look for or avoid
inappropriate prescribing for older adults, including drugs to avoid and
situations and conditions in which they should be avoided
• Guidelines on medications to use with caution, and dosage adjustments
for some common drugs that have serious consequences if the doses are
not lowered or adjusted based on the patient’s renal function
Expert Interview: Todd Semla Beers Criteria
Expert Interview: Todd Semla Beers Criteria
Listen to Our Expert Discuss (Continued):
• What is the purpose of the Beers Criteria (continued)?
• Main purposes (continued):
• To reduce drug-drug interactions that are common in older adults and
have been shown to have serious consequences when they occur, likely
hospitalization or death
Expert Interview: Todd SemlaBeers Criteria
Expert Interview: Todd SemlaBeers Criteria
Strategies to Guide Prescribing in Clinical PracticeStrategies to Guide Prescribing in Clinical Practice
Practice Implications:
• Become familiar with the 2015 Beers Criteria, which are available free through
the American Geriatrics Society (AGS) website
• Collaborative prescriber-pharmacist-nurse review of drugs (using validated
criteria to identify drugs more likely to be unnecessary or harmful) can help
initiate and guide the prescribing and de-prescribing process
• This process is inherently interdisciplinary (Steinman et al., 2011; Coleman et al., 2006)
• A team approach: Add content listed on page 20 of Ruth’s notes? (film:
Part 3, 4:44)

21
Overprescribed or Inappropriately Prescribed DrugsOverprescribed or Inappropriately Prescribed Drugs
• Anti-infective agents• Anticholinergic agents• Urinary and
gastrointestinal antispasmodics
• Antipsychotics• Benzodiazepines and
non-benzodiazepine sedatives
A Partial Listing of Many Beers Criteria Drugs Considered to Be Overprescribed or Inappropriately Prescribed:
• Digoxin >0.125 mg for heart failure
• Sedating antihistamines• Histamine-2 blockers• Non-steroidal anti-
inflammatory agents• Proton-pump inhibitors• Antidepressants• Vitamins and mineral
supplements
Listen to Our Expert Discuss:
• There are other criteria developed in Great Britain and Ireland called the
STOPP/START Criteria that have a great deal of overlap, but are mostly
complementary in terms of their content
• The Beers Criteria primarily focuses on drugs providers should avoid or use
with caution and make dosage adjustments because of renal function, or
drug-drug interactions that are particularly dangerous in older people
Expert Interview: Todd Semla STOPP/START Criteria
Expert Interview: Todd Semla STOPP/START Criteria
(O'Mahony et al., 2015)
Listen to Our Expert Discuss:
• The STOPP/START Criteria have many of the features of the Beers Criteria,
but focus on drugs that are underprescribed to older people that they should
be receiving
• For example, aspirin should be prescribed as a preventive for
cardiovascular disease
Expert Interview: Todd Semla STOPP/START Criteria
Expert Interview: Todd Semla STOPP/START Criteria

22
Underprescribed DrugsUnderprescribed Drugs
A Partial Listing of Drugs Underprescribed in Older Adults:
• Anticoagulants: in the presence of chronic atrial fibrillation
• Angiotensin inhibitors/blockers: in the presence of diabetes with proteinuria
• Antiplatelet agents: in the presence of documented vascular disease
• Antihypertensive agents: in the presence of uncontrolled hypertension
• Beta-receptor blockers: for heart failure or after myocardial infarction
• Bronchodilators: in the presence of obstructive lung disease
• Statins: in the presence of documented vascular disease unless end of life
• Proton-pump inhibitors or misoprostol: in NSAID-induced gastropathy protection
Listen to Our Expert Discuss:
• One major added category was proton-pump inhibitors
• Added because they are only meant to be taken for a short period of time,
for instance if they are being used to treat a peptic or gastric ulcer or GERD
• Only meant to be used for about eight weeks in total duration, and should
then be discontinued
Expert Interview: Todd SemlaProton-Pump Inhibitors
Expert Interview: Todd SemlaProton-Pump Inhibitors
Listen to Our Expert Discuss:
• However, proton-pump inhibitors are continued while the patient has not
made any lifestyle changes or other interventions that were recommended
to reduce their reflux
• Extended use sets older patients up for some severe effects, as proton-
pump inhibitors cause a decrease in bone mass and an increased risk for
hip and other osteoporotic fractures, and can increase the risk for
Clostridium difficile (C. diff)
Expert Interview: Todd SemlaProton-Pump Inhibitors
Expert Interview: Todd SemlaProton-Pump Inhibitors

23
Listen to Our Expert Discuss:
• Proton-pump inhibitors should be avoided for longer than eight weeks unless
there is justification, such as if a patient is taking a nonsteroidal anti-
inflammatory drug (NSAID), like ibuprofen, and are over 65, the patient
should be on a proton-pump inhibitor to help prevent the development of a
gastric ulcer as a result of being on the NSAID
Expert Interview: Todd SemlaProton-Pump Inhibitors
Expert Interview: Todd SemlaProton-Pump Inhibitors
According to the Beers Criteria for potentially inappropriate
prescribing, which of the following medications on Mrs. Roberts’ list
may be considered potentially inappropriate and/or harmful?
a) Budesonide/formoterol
b) Omeprazole
c) Diphenhydramine
d) b and c
Assessment Question 4Assessment Question 4
According to the Beers Criteria for potentially inappropriate
prescribing, which of the following medications on Mrs. Roberts’ list
may be considered potentially inappropriate and/or harmful?
a) Budesonide/formoterol
b) Omeprazole
c) Diphenhydramine
d) b and c (Correct Answer)
Assessment Question 4: AnswerAssessment Question 4: Answer

24
Appropriate PrescribingAppropriate Prescribing
Logical Approaches to Polypharmacy
• Much has been written and published on the logical approaches to
polypharmacy
• Rational prescribing requires restraint and wisdom in initiating chronic
medications, but also fundamental change in our philosophy of medicinal care
• A complex medication regimen should be challenged routinely, and
simplification welcomed when it can improve health and well-being
ReviewReview
• Doctors, pharmacists, nurses, patients, and their families can work to become
more informed and more adept at addressing the challenges of polypharmacy
with the intent to deprescribe when necessary
• If a practitioner sees a patient on many medications, the practitioner must do
something
ReviewReview

25
When seeing Mrs. Roberts in the clinic, she tells you she is having problems with her medications. Which of the following should MOST
LIKELY be considered as the next step in the context of her overall medication care needs?
a) Discontinue all her over-the-counter medications
b) Perform a complete review and consider stopping at least one medication
c) Consider adding an oral non-steroidal agent for osteoarthritis
d) Decide for her which medications to stop
Assessment Question 5Assessment Question 5
Assessment Question 5: AnswerAssessment Question 5: Answer
When seeing Mrs. Roberts in the clinic, she tells you she is having problems with her medications. Which of the following should MOST
LIKELY be considered as the next step in the context of her overall medication care needs?
a) Discontinue all her over-the-counter medications
b) Perform a complete review and consider stopping at least one medication (Correct Answer)
c) Consider adding an oral non-steroidal agent for osteoarthritis
d) Decide for her which medications to stop
Summary and Take-Home Points Summary and Take-Home Points
• When caring for older adult patients with multiple comorbidities and complex
health needs, the learner should recognize:
• Polypharmacy is common and poses considerable risk for negative health
outcomes
• Age-related changes in drug pharmacology will affect drug treatment
decisions
• Multiple explicit drug therapy tools are emerging to help guide and inform
prescribing practice

26
Summary and Take-Home Points Summary and Take-Home Points
• When caring for older adult patients with multiple comorbidities and complex
health needs, the learner should recognize (continued):
• A stepwise approach to prescribing and ongoing monitoring of medications is
essential
• Shared decision-making and patient engagement is central to quality
medication management
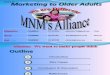
ResourcesGuidelines For Using Medications in Older Adults
ResourcesGuidelines For Using Medications in Older Adults
Guiding Principles (Schiff et al., 2011; Rochon & Gurwitz , 1997)
Additional Comments
1 - Obtain a complete drug history2 - Use non-pharmacological treatments first3 - Know the drugs you plan to use4 - Use no drug beyond its time. 5 - Start low, go slow
1 - Work to achieve a comprehensive, portable, indication-based medication list2 - Medicines should not replace effective psychosocial care3 - Know the pharmacological benefit-to-risk profile of the drugs you prescribe4 - Review patient drug list at each point-of-care visit and update them5 - Always use the minimum dose necessary and adjust based on tolerability
ResourcesGuidelines For Using Medications in Older Adults
ResourcesGuidelines For Using Medications in Older Adults
Guiding Principles (Schiff et al., 2011; Rochon & Gurwitz , 1997)
Additional Comments
6 - Maintain a heightened vigilance regarding adverse effects7 - Encourage treatment adherence8 - Use new drugs with particular caution and skepticism
6 - Be aware of withdrawal syndromes and educate people to anticipate reactions7 - Provide simple verbal and written instructions for every medicine and repeat prescriptions8 - Seek unbiased information, be aware of selective trial reporting
People are Central to Quality Use of Medications

27
ResourcesResources
Where Can You
Go
To Learn More?
Food and Drug Administration – FDA-Approved Drug Products
www.accessdata.fda.gov/scripts/cder/daf/
American Geriatrics Society – Beers Criteriawww.geriatricscareonline.org/toc/american-geriatrics-society-
updated-beers-criteria-for-potentially-inappropriate-medication-use-in-older-adults/CL001
ResourcesResources
Where Can You
Direct Patients,
Families
and
Caregivers
To Learn More?
National Library of Medicine – Medline Pluswww.nlm.nih.gov/medlineplus/
Health in Aging Foundation – Tip Sheetswww.healthinaging.org/
ResourcesResources
www.accessdata.fda.gov/scripts/cder/daf/ Accessed March 10, 2016
www.geriatricscareonline.org/toc/american-geriatrics-society-updated-beers-criteria-for-potentially-inappropriate-medication-use-in-older-
adults/CL001 Accessed March 10, 2016
www.healthinaging.org/ Accessed March 10, 2016
www.nlm.nih.gov/medlineplus/ Accessed March 10, 2016

28
ReferencesReferences
Ahmed B, Nanji K, Mujeeb R, & Patel MJ. (2014). Effects of polypharmacy on adverse drug reactions among geriatric outpatients at a tertiary care hospital in Karachi: a prospective cohort study. PLoS One, 9(11), e112133. doi:10.1371/journal.pone.0112133
Alldred DP, Kennedy MC, Hughes C, Chen TF, & Miller P. (2016). Interventions to optimise prescribing for older people in care homes. Cochrane Database Syst Rev, 2, Cd009095. doi:10.1002/14651858.CD009095.pub3
American Geriatrics Society. (2015). American Geriatrics Society 2015 Updated Beers criteria for potentially inappropriate medication use in older adults. J Am GeriatrSoc, 63(11), 2227-2246. doi:10.1111/jgs.13702
Budnitz DS, Lovegrove MC, Shehab N, & Richards CL. (2011). Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med, 365(21), 2002-2012. doi:10.1056/NEJMsa1103053
Chiu MH, Lee HD, Hwang HF, Wang SC, & Lin MR. (2015). Medication use and fall-risk assessment for falls in an acute care hospital. Geriatr Gerontol Int, 15(7), 856-863. doi:10.1111/ggi.12359
Coleman EA, Parry C, Chalmers S, & Min SJ. (2006). The care transitions intervention: results of a randomized controlled trial. Arch Intern Med, 166(17), 1822-1828. doi:10.1001/archinte.166.17.1822
Cooper JW. (1999). Adverse drug reaction-related hospitalizations of nursing facility patients: a 4-year study. South Med J, 92(5), 485-490.
Cruz-Jentoft AJ, Boland B, & Rexach L. (2012). Drug therapy optimization at the end of life. Drugs Aging, 29(6), 511-521. doi:10.2165/11631740-000000000-00000
Doan J, Zakrzewski-Jakubiak H, Roy J, Turgeon J, & Tannenbaum C. (2013). Prevalence and risk of potential cytochrome P450-mediated drug-drug interactions in older hospitalized patients with polypharmacy. Ann Pharmacother, 47(3), 324-332. doi:10.1345/aph.1R621
Fried TR, O'Leary J, Towle V, Goldstein MK, Trentalange M, & Martin DK. (2014). Health outcomes associated with polypharmacy in community-dwelling older adults: a systematic review. J Am Geriatr Soc, 62(12), 2261-2272. doi:10.1111/jgs.13153
Gill SS, Mamdani M, Naglie G, Streiner DL, Bronskill SE, Kopp A, Shulman KI, Lee PE, & Rochon PA. (2005). A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Arch Intern Med, 165(7), 808-813. doi:10.1001/archinte.165.7.808
Gray SL, Anderson ML, Dublin S, Hanlon JT, Hubbard R, Walker R, Yu O, Crane PK, & Larson EB. (2015). Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med, 175(3), 401-407. doi:10.1001/jamainternmed.2014.7663
Greenhalgh T, Howick J, & Maskrey N. (2014). Evidence based medicine: a movement in crisis? BMJ, 348, g3725. doi:10.1136/bmj.g3725
Gurwitz JH, Field TS, Judge J, Rochon P, Harrold LR, Cadoret C, Lee M, White K, LaPrino J, Erramuspe-Mainard J, DeFlorio M, Gavendo L, Auger J, Bates DW. (2005). The incidence of adverse drug events in two large academic long-term care facilities. American Journal of Medicine. 118, 521-258.
Hanlon JT, Schmader KE, Koronkowski MJ, Weinberger M, Landsman PB, Samsa GP, & Lewis IK. (1997). Adverse drug events in high risk older outpatients. J Am Geriatr Soc, 45(8), 945-948.
Holmes HM, Hayley DC, Alexander GC, & Sachs GA. (2006). Reconsidering medication appropriateness for patients late in life. Arch Intern Med, 166(6), 605-609. doi:10.1001/archinte.166.6.605
Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, & Sung FC. (2010). Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore), 89(5), 295-299. doi:10.1097/MD.0b013e3181f15efc
Lu WH, Wen YW, Chen LK, & Hsiao FY. (2015). Effect of polypharmacy, potentially inappropriate medications and anticholinergic burden on clinical outcomes: a retrospective cohort study. Cmaj, 187(4), E130-137. doi:10.1503/cmaj.141219
Nahin RL, Pecha M, Welmerink DB, Sink K, DeKosky ST, & Fitzpatrick AL. (2009). Concomitant use of prescription drugs and dietary supplements in ambulatory elderly people. J Am Geriatr Soc, 57(7), 1197-1205. doi:10.1111/j.1532-5415.2009.02329.x
O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, & Gallagher P. (2015). STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing, 44(2), 213-218. doi:10.1093/ageing/afu145
Osterberg L, & Blaschke T. (2005). Adherence to medication. N Engl J Med, 353(5), 487-497. doi:10.1056/NEJMra050100
Pan HH, Li CY, Chen TJ, Su TP, & Wang KY. (2014). Association of polypharmacy with fall-related fractures in older Taiwanese people: age- and gender-specific analyses. BMJ Open, 4(3), e004428. doi:10.1136/bmjopen-2013-004428
ReferencesReferences
Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, & Lindau ST. (2008). Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA, 300(24), 2867-2878. doi:10.1001/jama.2008.892
Qato DM, Wilder J, Schumm LP, Gillet V, & Alexander GC. (2016). Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs 2011. JAMA Intern Med, 176(4), 473-482. doi:10.1001/jamainternmed.2015.8581
Rochon PA, & Gurwitz JH. (1997). Optimising drug treatment for elderly people: the prescribing cascade. BMJ, 315(7115), 1096-1099.
Schiff GD, Galanter WL, Duhig J, Lodolce AE, Koronkowski MJ, & Lambert BL. (2011). Principles of conservative prescribing. Arch Intern Med, 171(16), 1433-1440. doi:10.1001/archinternmed.2011.256
Schmidt LE, & Dalhoff K. (2002). Food-drug interactions. Drugs, 62(10), 1481-1502.
Spinewine A, Schmader KE, Barber N, Hughes C, Lapane KL, Swine C, & Hanlon JT. (2007). Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet, 370(9582), 173-184. doi:10.1016/s0140-6736(07)61091-5
Steinman MA, Handler SM, Gurwitz JH, Schiff GD, & Covinsky KE. (2011). Beyond the prescription: medication monitoring and adverse drug events in older adults. J Am Geriatr Soc, 59(8), 1513-1520. doi:10.1111/j.1532-5415.2011.03500.x
Steinman MA, & Hanlon JT. (2010). Managing medications in clinically complex elders: "There's got to be a happy medium". JAMA, 304(14), 1592-1601. doi:10.1001/jama.2010.1482
Wolfstadt JI, Gurwitz JH, Field TS, Lee M, Kalkar S, Wu W, & Rochon PA. (2008). The effect of computerized physician order entry with clinical decision support on the rates of adverse drug events: a systematic review. J Gen Intern Med, 23(4), 451-458. doi:10.1007/s11606-008-0504-5
ReferencesReferences