Embed Size (px)
Citation preview

Drug Development for Diabetic Foot Infections:
Lessons Learned
Alfred F. Sorbello, DO, FACOIMedical Officer, CDER/DAIDP
Anti-Infective Drug Advisory Committee Meeting
October 28, 2003

Introduction• Defining Diabetic Foot
Infections• Classifying Diabetic Foot
Infections and Foot Ulcers• Characterization of Study
Population• Adjunctive Treatment Measures• Microbiologic Considerations

Definition of a Diabetic Foot Infection
• No generally-accepted definition• Foot infections in diabetics can be
ulcer- or non-ulcer related– ~15% of diabetics develop chronic non-
healing foot ulcers– Not all chronic foot ulcers are infected
• Clinical trials– Broad studies of cSSSIs with
supplemental studies involving diabetic foot infections
– Eligibility criteria • Specific disease entities • Discrete clinical findings • Presence/absence of a foot ulcer

Common Lower Extremity Problems in Diabetics
• Developmental foot deformities•hammer toes, valgus deformities
• Soft tissue changes•chronic lower extremity edema•dependent rubor•stasis dermatitis•chronic ulcers colonized with
bacteria
• Decreased peripheral pulses• Sensory peripheral neuropathy• Charcot (neuropathic) joints

Comparative Prognostic Factors in Diabetics with Osteomyelitis of the Foot
Feature Good Outcome Poor OutcomeAge (years) 61 1 63 2Length of DM(years)
17 1 18 3
Temp >100.4F 22.2% 12.5%Presence of footulcer
96.3% 91.7%
Erythema 88.9% 83.3%Drainage 85.2% 79.2%Warmth 85.2% 62.5%Swelling* 88.9% 58.3%Necrosis* 14.8% 54.2%Neuropathy 96.3% 91.7%
Bamberger et al. Am J Med 1987;83:653-660
* statistically significant

Clinical Trials: Framework for a Definition for a Diabetic Foot Infection• Presence or absence of:– open wound, foot ulcer, break in skin– clinical findings
• Anatomic location of primary site• Depth of infection
(skin/soft tissue vs. bone/joint)• Isolation of pathogenic bacteria from
an appropriate culture specimen

Classification Systems for Diabetic Foot Infections
• Classification systems– Severity of Infection– Foot Ulcer (Wound)
•No generally-accepted classification•Differ in criteria & complexity•Require validation for clinical trials

Classification Systems for Severity of Diabetic Foot
Infections• Limb-threatening vs.
non-limb threatening• Mild, moderate, severe

Classification Systems for Diabetic Foot Ulcers
•Wagner•Univ of Texas•S(AD) SAD•Simple staging

Clinical Trials: Framework to ClassifyDiabetic Foot Infections
• Standardize definitions – clinical disease entities– assessments of ischemia, neuropathy
• Correlate with extent, natural history, and prognosis of the infection
• Distinguish skin/soft tissue from bone/joint infections
• Would need validation

Characterization of Study Population
• Demographics• Co-morbidities• Baseline
Assessments• Clinical Diagnoses

Demographics and Co-morbidities
• Age• Gender• Race• Weight• Country of Origin• Study
Center/Site
• Type 1 vs type 2 DM• Peripheral neuropathy• Peripheral vascular
disease• Renal insufficiency• History of
osteomyelitis• History of lower
extremity surgery– podiatric, orthopedic,
vascular

Baseline Assessments
• Laboratory– hematology– chemistry
– HgbA1C
– C-Reactive Protein
– Wound, tissue, and blood cultures
• Radiologic imaging• Vascular evaluation• Neurologic exam• Pulse oxygenation
measurement (toe)• Wound or ulcer
dimensions

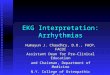
Infected ulcer Cellulitis Deep soft tissue infection Paronychia Septic arthritis Osteomyelitis Other
Cellulitis Infected Ulcer Septic Arthritis Paronychia Other Deep soft tissue Osteomyelitis Infected ulcer, Osteomyelitis Cellulitis, Infected ulcer, Osteomyelitis Cellulitis, Osteomyelitis, Septic Arthritis Cellulitis, Deep soft tissue, Osteomyelitis Deep soft tissue, Infected ulcer, Osteomyelitis Deep soft tissue, Osteomyelitis Cellulitis, Deep soft tissue, Infected ulcer, Osteomyelitis Infected Ulcer, Paronychia Cellulitis, paronychia Cellulitis, Infected Ulcer Deep soft tissue, Infected ulcer Cellulitis, Other Cellulitis, Deep soft tissue, Infected ulcer Cellulitis, Deep soft tissue, Paronychia Cellulitis, Infected ulcer, Other Cellulitis, Infected Ulcer, Deep soft tissue, Paronychia Cellulitis, Deep soft tissue Infected ulcer, Other Cellulitis, Infected ulcer, Paronychia
CRF Tabulation
FDA
Heterogeneity of Baseline Clinical Diagnoses:CRF Tabulation

Adjunctive Treatment Measures
• Adjunctive treatments permitted per protocol to augment wound healing
• Are they utilized equally in all subjects in both treatment groups?
• Could adjunctive treatments make two dissimilar drugs appear indistinguishable?

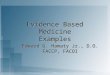
Adjunctive Treatments and Clinical Outcome
# of subjects cured at EOTStudydrug
Comparator Study drug ComparatorNumberof surgicaldebridements N=241 N=120 N, % N, %
0 126 54 84 (67) 43 (63)
1-2 89 52 61 (69) 31 (60)
3 26 14 19 (73) 12 (86)
EOT = end of therapy; N = number of subjects
Trend indicative of improved cure rate associated with increasing number of debridements.

Microbiologic Considerations• Identify pathogens
– among polymicrobial infections
• Standardize culture methodology– swabs, curettage, biopsy
• Microbiological outcome– Presumed pathogen eradications
predominate due to healing of pre-therapy wounds/ulcers
– outcome endpoints are clinically-driven
– follow-up cultures should be performed in treatment failures

Guidance Development for DFIs
• Define and classify diabetic foot infections and foot ulcers
• Characterize study population• Primary focus is on clinical outcome • Standardize microbiologic methodology• Effect of adjunctive treatment(s) on
clinical outcome• Separate clinical trials to assess drug
development for bone and joint infections