Embed Size (px)
Citation preview

Hemodynamic Case StudiesEdward G. Hamaty Jr., D.O. FACCP, FACOI

Pattern Recognition


Fluid Replacement Therapy-Goals

Fluid Therapy Protocol

Fluid Challenge Guideline Chart

Depressed Myocardium and Wedge

Pressure-Volume Compliance Relationship

PCWP and SV• Changes in preload are important primarily if they
affect stroke volume.• The next graphic illustrates the importance of
noting the PCWP in conjunction with the SV.• Notice that on the right side of the table no
optimal PCWP appears to exist.• The lack of determining an optimal wedge
pressure is more the rule than the exception.• Be very cautious in using the PCWP as the
primary guide to treating hemodynamics.• PCWP values are only useful when used in
conjunction with other hemodynamic information.
• To use the PCWP as the primary indicator for therapies runs the risk of employing unnecessary or inappropriate therapies.

PCWP and SV

PCWP on EVLW

PCWP on EVLW

Practice Clinical Senarios• Simple and typical clinical senarios
for pattern analysis.

Practice Exercise 1

Practice Exercise 1 Answer

Practice Exercise 2

Practice Exercise 2 Answer

Practice Exercise 3

Practice Exercise 3 Answer

Practice Exercise 4

Practice Exercise 4 Answer

Practice Exercise 5

Practice Exercise 5 Answer

Practice Exercise 6

Practice Exercise 6 Answer

Practice Exercise 7

Practice Exercise 7 Answer

Practice Exercise 8

Practice Exercise 8 Answer

Practice Exercise 9

Practice Exercise 9 Answer

Practice Exercise 10

Practice Exercise 10 Answer

Practice Exercise 11

Practice Exercise 11 Answer

Total Peripheral Resistance

Current Treatment of Shock - General
• The main determinants of tissue perfusion are cardiac output and mean arterial pressure. Although it has its limitations, especially in certain distributive types of shock, the MAP is a simple measure to roughly determine the adequacy of tissue perfusion.
• MAP – CVP is dependent on CO and SVR:• MAP-CVP = CO x SVR• MAP = (CO x SVR) + CVP [CO = SV x HR]• MAP = SV x HR x SVR + CVP [SV = EDV-ESV]
• This brings us back to one of our initial diagrams:

Determinants of Cardiac Output
SVI, LVSWI, RVSWI
SVR (LV)
PVR (RV)
Compliance
RVEDV
RAP, CVP
PAD, PAWP
[MAP = CO x SVR + CVP]

Case 1 Pneumonia vs CHF• PATIENT 1: PNEUMONIA VERSUS• CONGESTIVE HEART FAILURE./Chaim Putterman, Charles L.
Sprung• A 22 year old woman with systemic lupus erythematosus (SLE) was
hospitalized in her 21st week of pregnancy for evaluation of anemia, proteinuria and peripheral edema. She was diagnosed as suffering from SLE two years previously based upon fever, lymphadenopathy, arthalgia, pancytopenia, and a characteristic malar rash, accompanied by a positive anti-nuclear factor and high levels of anti-DNA antibody. An exacerbation of her disease one year previously responded to a course of intravenous hydrocortisone, and she was recently reasonably well controlled with a daily dose of 15 mg of prednisone.
• During the first trimester of her pregnancy, she developed fever and decreasing hemoglobin from 11 to 9 gr/dl. She was hospitalized in the high risk obstetric ward for in-hospital evaluation. Despite an increase in the daily dose of prednisone to 20 mg and subsequently to 60 mg. the hemoglobin decreased to 6.9 gr/dl, the direct Coombs test was positive and the lactic dehydrogenase increased. In addition, hyperkalemla. hypoalbuminemia, severe proteinuria and a de-crease in creatinine clearance developed, and she was transferred to the Internal Medicine ward.

Case 1 Pneumonia vs CHF• On examination, the blood pressure was 105/70 mmHg, pulse
76 beats/min, respirations 20 breaths/min with slight dyspnea, and normal temperature. The only notable physical findings were slight pallor of the skin and conjuctivae, mild peripheral edema, and a II/VI systolic non-radiating flow murmur heard at the left sternal border.
• Laboratory examinations: white blood count 3,200/cu mm with 66% neutrophils, hematocrit 21%, and platelets 115,000/cu mm. Coagulation studies were normal. Abnormalities in the biochemical profile included 'total protein 5.0 gr/dl. albumin 2.7 gr/dl, urea 34 mg/dl and creatinine 1.3 mg/dl. C4 was 14 mg% (normal 20-50). C3 16 mg% (normal 50-120). anti-cardiolipin was negative, anti-SS-A negative, anti-nuclear factor positive +4/+4, anti-DNA 15.2 microgr/ml (normal 0-1.5), and anti-Sm positive. Urinary albumin was 2.0 gr/dl, with a daily urinary output of 800 to 1000 cc, and a creatinine clearance of 88 cc/min. The chest X-ray was normal and the electrocardiogram showed sinus tachycardia. Obstetrical ultrasound showed a viable infant appropriate for gestational age. with no obvious anatomical abnormalities.

Case 1 Pneumonia vs CHF• A diagnosis of pregnancy-induced exacerbation of SLE was
made, based upon the hemolytic anemia, leukopenia, thrombocytopenia and nephrotic syndrome, accompanied by impressive laboratory evidence of disease activity. Intravenous high dose hydrocortisone was begun, together with azathioprine. Fluid therapy included diuretics and intravenous albumin. Over the next month, the patient's nephrologic status gradually stabilized with a decrease in urinary albumin excretion, and serum urea and creatinine. After two months of hospitalization, the patient began to complain of dyspnea, and the temperature rose to 40.5°C.
• On examination, the patient was in moderate to severe respiratory distress. Blood pressure was 160/90 mmHg, pulse regular at 140 beats/min and respirations 50 breaths/min. The jugular veins were not distended and anasarca was present. On auscultation of the lungs, diffuse coarse crepitations were heard throughout inspiration and expiration. A summation gallop was heard on auscultation of the heart. The abdomen was soft, and the uterine fundus was palpated at the level of the umbilicus. Peripheral pulses were normal and Homan's sign was negative.

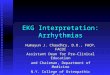
Case 1 Pneumonia vs CHF• The chest X-ray revealed borderline cardiomegaly, with signs of
diffuse bilateral infiltrates (Figure 12.1). • On room air, an arterial blood gas analysis showed pH 7.46, pO2 59 mmHg with
a saturation of 92%. and pCO2 28 mmHg. The patient was transferred to the ICU.
• Despite high concentrations of oxygen by mask and nasalprongs, arterial blood gases improved only slightly. Due to the hypox‑emia, tachypnea, and need for diagnostic bronchoscopy, the patientwas incubated and mechanical ventilation was instituted.
• Because of the inability to determine by clinical means whether the diffusebilateral pulmonary infiltrates were secondary to congestive heartfailure (from lupus myocarditis, toxemia of pregnancy, peripartum cardiomyopathy), volume overload (due to glucocorticoid therapy or low serum protein and colloid osmotic pressure), or progressive pneumonia in an immunocompromised host, a pulmonary artery catheter (PAC) was inserted.
• The central venous pressure (CVP) was 6 mmHg. pulmonary artery pressure 20/12 mmHg. pulmonary artery occlusion pressure (PAOP) 8 mmHg, cardiac output 12.5 liter/ min, and cardiac index 7.2 liter/min/m2.
• Bronchoscopy was performed at the bedside, but was negative for bacterial, viral, fungal or parasitic organisms. A precise microbiological diagnosis was deemed essential in this immunocompromised host, and an open lung biopsy was performed.

Case 1 Pneumonia vs CHF
Figure 12.1. Chest roentgenogram demonstrating borderline cardiomegaly and diffuse bilateral infiltrates. Pulmonary artery catheterization was performed to differentiate between pneumonia and congestive heart failure as an etiology.

Case 1 Pneumonia vs CHF• Discussion• Catheterization of the pulmonary artery at the bedside with the
balloon-tipped PAC is frequently indispensable for an accurate differentiation between cardiac and pulmonary etiologies of respiratory distress and diffuse bilateral pulmonary infiltrates. Heart failure and pulmonary edema are common situations in every-day practice. Most clinicians are confident in their diagnostic ability to accurately identify and reasonably quantify the presence of heart failure. Suprisingly, it has been demonstrated that non-invasive techniques are clearly inadequate for predicting cardiovascular function in the critically ill, and for correctly differentiating between cardiac and non-cardiac pulmonary edema.
• Bayliss et al (1) prospectively studied 55 patients in a cardiac care unit to determine the accuracy of clinical evaluation, relative to "hard" data obtained from invasive hemodynamic monitoring. Physicians correctly predicted cardiac output in 71%, the PAOP in 62%, and the overall hemodynamic status only in 55%. Fein et al (2) examined the ability of physicians to differentiate cardiac from non-cardiac (permeability) edema on the basis of clinical and radiographic criteria in 70 patients admitted to the ICU with pulmonary edema.

Case 1 Pneumonia vs CHF• Clinical assessment of permeability pulmonary edema was correct in 17
of 20 patients (85%). However, of the 50 patients initially suspected of having a cardiogenic cause for the edema, only 31 patients were correctly classified (62%). Even in patients with known chronic heart failure, Stevenson and Perloff)recently documented limited reliability of physical signs for estimating hemodynarnics. Rales, edema and elevated mean jugular venous pressure were absent in 18 of 43 patients with PAOP pressures equal or greater than 22 mmHg. Stevenson and Perloff (3) concluded that reliance on physical signs alone for the diagnosis of elevated ventricular filling pressure may result in inadequate therapy.
• The occurrence of pulmonary disease with diffuse bilateral in-filtrates is a recognized and ominous manifestation of SLE. The differential diagnosis is wide, and includes pulmonary hemorrhage, lupus pneumonitis, uremia, drug reactions and congestive heart failure (4). Heart failure in patients with SLE can also be multifactorial. Many different mechanisms of heart involvement in SLE have been recognized and have recently been summarized by Doherty and Siegel (5). Lupus cardiomyopathy (6), valvular heart disease (7), premature coronary artery disase (8) and myocarditis (9) can all lead to a decrease in myocardial function and produce the clinical syndrome of congestive heart failure.

Case 1 Pneumonia vs CHF• Recently, yet another cause of respiratory failure has been identified in
patients with severe SLE, particularly those treated with high doses of corticosteroids. Andonopolous (10) found that 7 of 46 patients with SLE, all female, died with a clinical, radiological, physiological and pathological picture compatible with ARDS. In fact, the entire mortality of the patient population was represented by the prevalence of ARDS. In most patients with SLE and ARDS, infection was documented as the probable link between these syndromes. However, ARDS also appeared primarily in patients with SLE in whom no infectious process could be identified (10-12).
• What parameters derived from the PAC can assist in the differentiation between a cardiac and pulmonary etiology of lung in-filtrates? The patient with congestive heart failure typically has a decreased cardiac output and an increased CVP and PAOP, whereas the patient with a pulmonary disorder has a normal or increased cardiac output, normal or low PAOP, and a CVP that may be elevated.
• Another helpful parameter derived from the PAC is the gradient between the pulmonary artery diastolic pressure and the PAOP. This gradient is usually normal in patients with cardiac disorders, but may increase in primary pulmonary disorders. Rahimtoola et al (13) examined the relationship of the pulmonary artery diastolic pressure (PADP) to left ventricular diastolic pressures in patients with acute myocardial infarction.

Case 1 Pneumonia vs CHF• In patients without significantly increased pulmonary vascular resistance (PVR),
there were no significant differences between the PADP and mean PAOP. All patients but one with a PADP > 15 mmHg had a PAOP > 12 mmHg and all but one patient with a mean PAOP > 12 mmHg had a PADP > 15 mmHg.
• However, with increased PVR, an average gradient of 6.7 mmHg existed between the PADP and PAOP. Lappas et al (14) found good correlation between left atrial pressure (LAP) and PAOP, and between LAP and PADP, in 161 paired measurements in cardiac-surgical patients. Gabriel et al (15) investigated the difference between PADP and the mean PAOP and its relationship to PVR in 24 patients with chronic lung disease. In patients with normal PVR, there was no significant pressure difference either at rest or during exercise over a wide range of PAOP values (6-27 mmHg), while in patients with increased PVR a significant pressure difference was present.
• A gradient of 4-5 mmHg allowed for differentiation between normal and increased PVR. Several studies have shown that an in-creased gradient also correlated with the presence of pulmonary hypertension, and may be predictive of a higher mortality (16,17).
• Sibbald et al (18) have summarized a practical approach to differentiate cardiac from non-cardiac pulmonary edema in the critically ill. Definitive separation between these two major types of edema necessitates demonstration of increased microvascular permeability, which is characteristic of non-cardiogenic pulmonary edema. However, this can be shown only by cumbersome radiotracer techniques not generally available outside the research setting.
• In most clinical situations, documentation of persistently increased extravascular lung water [by direct measurement (or indirectly from the chest X-ray) and the measurement of microvascular hydrostatic pressures with the PAC will allow accurate diagnosis of the cause of the pulmonary edema.

Case 1 Pneumonia vs CHF• Traditionally, use of invasive hemodynamic monitoring has usually
been in the complicated, medical or surgical patient with multiorgan dysfunction, either due to the current disease process or because of the patient's premorbid health status. However, experience in recent years supports an important role for the PAC for certain indications in obstetrics and gynecology, particularly during complicated pregnancy.
• Major hemodynamics adjustments occur in the pregnant woman, even without cardiovascular disease. Important factors are increased uterine blood flow, the placental circulation, and inferior vena cava obstruction. Cardiac output increases by al-most 40% by the 28 to 32 week of pregnancy, while vascular resistance tends to decrease. Further changes in hemodynamic parameters during labor and delivery increase the need for careful observation in the complicated obstetric patient (19).
• Several specific applications of the PAC in the critically ill obstetric patient have been discussed in recent years (20-23). Pre-eclampsia (toxemia) can be accompanied by significant hemodynamic changes that can predispose to pulmonary edema. However, defining the exact mechanism of the edema is essential for pro-per treatment.
• Cardiogenic pulmonary edema may occur in this setting because of the markedly increased systemic vascular resistance, leading to depressed left ventricular function and congestive heart failure. The primary therapy in this case would be aggressive afterload reduction and rigid control of hypertension.

Case 1 Pneumonia vs CHF• On the other hand, pulmonary edema may also be caused by the decrease in
colloid osmotic pressure present in patients with severe eclampsia, or by an increase in pulmonary capillary permeability.
• Management in non-cardiogenic pulmonary edema consists of lowering the PAOP (with fluid restriction and diuretics) to the lowest level compatible with peripheral perfusion, while treating the responsible insult. The only reliable way to distinguish between the cardiogenic and non-cardiogenic mechanisms of edema in women with pre-eclampsia is by using the PAC.
• Indeed, both aforementioned mechanisms may be operative, and defining their relative contribution to the clinical situation is possible only by invasive monitoring. Clark and Cotton (21) suggest that monitoring with the PAC in pre-eclamptic patients is also indicated in severe, unresponsive hypertension, persistent oliguria unresponsive to fluid challenge, and for safe induction of anesthesia in certain parturients.
• Many indications for catheterization encountered in obstetric and gynecologic patients are common to other areas of medicine, such as radical surgery, septic shock, and acute myocardial infarction (22).
• Unique indications include pre-eclampsia and rheumatic heart disease in pregnancy. Although based on a retrospective summary, Clark et al (22) advocate an important role for the PAC in the critically ill obstetric or gynecological patient to ensure an optimal outcome-both for the mother and fetus.

Case 1 Pneumonia vs CHF• Microvascular disorders involving the pulmonary arterial tree such as
amniotic fluid embolism, fat embolism and lymphangitic carcinomatosis are often a diagnostic challenge to the clinician. The differential diagnosis of respiratory failure and pulmonary infiltrates can be extensive, as it was in our patient, and may necessitate invasive investigation. In some cases, however, a diagnosis cannot be made until autopsy.
• Masson and Ruggieri in 1985 (24) hypothesized that fetal squamous cells, fat globules, and malignant cells would be recognizable in microvascular blood obtained from the pulmonary circulation via the lumen of a PAC in the wedged position. Wedged pulmonary blood was found to almost invariably contain megakaryocytes and megakaryocytic nuclei, which are particulary abundant in the pulmonary capillary bed, indicating the microvascular source of the blood obtained. In preliminary studies (24,25), fetal squamous cells in amniotic fluid embolism and fat globules in fat embolism were easily identified by cytologic study, and provided important confirmatory di-agnostic information.
• This information is available without risk in those patients in whom a PAC is already present for hemodynamic monitoring. Masson et al (26) recently evaluated this technique of cytologic analysis of blood from wedged PAC in 8 patients in whom lymphangitic carcinomatosis was subsequently confirmed by other means. Malignant cells were found in 7 of the 8 patients. Cytologic findings were normal in 16/17 patients with cancer but without pulmonary metastases, and in 22/23 patients with non-malignant pulmonary disorders.

Case 1 Pneumonia vs CHF• Masson et al concluded that pulmonary microvascular cytology may be
especially valuable for the diagnosis of some patients with obscure respiratory failure, when lung biopsy is refused or too dangerous, or when a PAC is otherwise present for other purposes.
• Although prognosis of cancer patients with such extensive spread is generally dismal, a positive pulmonary microvascular cytology result may allow for better planning of the subsequent management.
• The present patient, based upon the above discussion, had several indications for the insertion of the PAC upon the precipitous deterioration in her respiratory status. The etiology of the diffuse pulmonary infiltrates was unclear, and it was thought that further diagnostic delay would only be to the patient's detriment.
• The various-contributions of pregnancy, SLE, or complications of therapy could not be determined, and the primary question of whether the infiltrates resulted from a "cardiac" or "pulmonary" etiology could not be resolved.
• As can be seen from the initial hemodynamic data of a low PAOP, high cardiac index, and low SVR, no cardiac dysfunction was present-whether due to pregnancy or systemic vasculitis. The cardiac output was appropriate for the metabolic demands of the mother and fetus. The main diagnostic considerations at this stage became lupus pneumonitis, an infectious pneumonia due to the immunosuppression, or ARDS.

Case 1 Pneumonia vs CHF• Routine microbiology and bronchoalveolar lavage
failed to provide a definite pathogen and a diagnostic open lung biopsy was performed. On histological examination, severe interstitial inflammation was present. In the alveolar spaces, an amorphic, necrotic infiltrate was the dominant finding, in which small corpuscles could be seen.
• On silver staining, the diagnosis of Pneumocystis carinii pneumonia was confirmed. High dose cotrimoxazole therapy was initiated.
• Two weeks later, there was spontaneous rupture of the amniotic membranes, and the patient gave birth to a 900 gram, healthy female infant. After a pro-longed and stormy hospital course, the patient slowly improved, was weaned from mechanical ventilation, was discharged from the ICU and finally sent home.

Pulmonary Disease-Acute Respiratory Distress

Case 2 Complicated MI• ATIENT 2: COMPLICATED MYOCARDIAL INFARCTION/John M.
Phelan, Joseph E. Parrillo
• A 54 year old man with a history of non-insulin dependent diabetes and hypercholesterolemia presented to the emergency room with 1 hour of left arm discomfort with associated dyspnea, nausea and diaphoresis. He also noted palpitations and lightheadedness. On arrival to the ER he was given oxygen by nasal cannula and attached to a cardiac monitor. His medications included micronase and mevacor.
• Physical examination was remarkable for: marked diaphoresis with a blood pressure of 105/60 mmHg, an irregular pulse of 115 beats/min, and a respiratory rate of 22 breaths/min. Lung exam revealed few bibasilar rales. Examination of the heart showed a focal non-displaced PMI with normal S, and S2 and an S4 gallop. The abdomen was benign and extremity exam unremarkable.
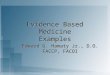
• Laboratory analysis revealed: hemoglobin 13 gm/dl, white blood count 10,000 /cu mm, hematocrit 39%, ABG (on 2L 02) pH 7.46, P02 86 mmHg, PCO2 34 mmHg, BUN 17 mg/dl, creatinine 0.9 mg/dl, and CPK 200. The chest x-ray showed no evidence of congestive heart failure or cardiomegaly. The electrocardiogram revealed 8 mm of ST elevation in leads V2 thru V6 and in AVL and I. (see EKG, Figure 12.2).

Case 2 Complicated MI

Case 2 Complicated MI• Hospital Course• Sublingual nitroglycerin was administered without relief, and eventually
morphine sulfate was given to relieve his symptoms. Thrombolytic therapy was initiated with intravenous t-PA and heparin was begun with a 5000 unit bolus and 1000 u/hr continuous drip. Aspirin 160 mg P.O. was given. Because of frequent episodes of non-sustained ventricular tachycardia. lidocaine therapy was initiated. He had a persistent tachycardia to 115-120 beats/min, and metoprolol 5 mg IV was administered three times.
• Over the next three hours his symptoms were not ameliorated. In addition his blood pressure fell to 75/40 mmHg with a pulse of 100 beats/min. Dopamine therapy was initiated and the patient was transferred to the cardiac catheterization laboratory where a pulmonary artery catheter was inserted and showed the hemodynamic Pro-file 12.1, #1.
• With these results an intraaortic balloon pump was inserted and a dobutamine drip was started (see 12.1, #2). Coronary angiography was quickly performed and revealed a 100% occlusion of the proximal left anterior descending artery.
• On the basis of this man's hemodynamic profile and coronary anatomy the decision was made to proceed with salvage angioplasty. This was successfully performed and the patient was returned to the CCU where follow-up hemodynamic monitoring was employed so that the PAOP and cardiac output were optimized until inotropic support could be weaned after 2 days (Profile 12.1, #3).

Case 2 Complicated MI

Case 2 Complicated MI• Discussion• This patient's clinical course demonstrates the reduced mortality (27) associated
with cardiogenic shock and reflects our belief that incipient cardiogenic shock following acute myocardial infarction (AMI) should be approached with aggressive early efforts at revascularization. Prior efforts (28) to classify patient outcomes based on bedside clinical examination demonstrated a high clinical mortality as shown in the Killip classification (Table 12.1).
• Of note, the incidence of cardiogenic shock in the 1970's was 10% to 20% and the mortality remained high probably because pharmacotherapy alone was only supportive.
• As noted in Table 12.2, Forrester, et al (29) have correlated the clinical findings with hemodynamic data from pulmonary artery catheterization. While these hemodynamic subsets closely follow physical exam, there is enough disparity in about 20-30% of patients to mandate the use of a pulmonary artery catheter (PAC). In fact pulmonary catheterization is needed to optimize fluid and pharmacologic therapy.
• Crexell et al (30) have shown that when a PAOP is less than 14 in the face of LV systolic impairment, patients derive great benefit from volume loading. In this study optimal filling pressures of 14 to 18 mmHg resulted in significant improvements in cardiac out-put and mean arterial pressure. This occurs as the result of reduced left ventricular compliance produced by ischemia. Even higher pressures may be tolerated so long as respiratory compromise is avoided. Usually, filling pressures beyond this level result in further deterioration of cardiac performance.

Case 2 Complicated MI

Case 2 Complicated MI• An intelligent use of the PAC in cardiogenic shock requires a
solid understanding of the underlying pathogenesis of this form of shock (Figure 12.3).
• When total myocardial necrosis exceeds 40% of left ventricular myocardial mass, cardiogenic shock ensues. This may occur as the result of one large infarction, infarct extension or a small infarct in the setting of prior damage. Right ventricular infarction may also be associated with cardiogenic shock, and mechanical complications of MI should be excluded in every patient who develops cardiogenic shock. Thus, the physician should always look for the presence of an acute ventricular septal defect, ruptured (or dysfunctional) papillary muscle, or free wall rupture. When inserting a PAC in the setting of cardiogenic shock, blood should be sampled for percent saturation in the right atrium, right ventricle and pulmonary artery.
• Generally an oxygen saturation step-up of 5% or greater suggests left to right shunting characteristic of a VSD. A large v wave (10 mmHg or greater above the PAOP) suggests mitral regurgitation. Since other entities may yield similar findings, the presence of mitral regurgitation should be confirmed with echocardiography or left ventriculography.

Case 2 Complicated MI

Case 2 Complicated MI• In the era of thrombolytic therapy, the incidence of cardiogenic shock has
fallen dramatically to about 5%. This reduction has probably resulted from emphasis on the urgent need to re-establish myocardial blood flow to salvage myocardium and pre-vent further pump failure. This must be accomplished early, prior to the development of end organ manifestations of pump failure (i.e. acute renal failure, shock liver).
• As noted above, supportive therapy alone (i.e. inotropic, vasopressors, vasodilators, diuretics) has little impact on survival in cardiogenic shock. Use of the intraaortic balloon has improved mortality in patients with cardiogenic shock insofar as it enables stabilization of the patient prior to more invasive therapeutic modalities aimed at restoration of coronary blood flow. However, if the balloon pump is utilized for support without revascularization, prognosis remains poor (31).
• As DeWood et al (32) demonstrated, patients with cardiogenic shock after myocardial infarction have improved survival with surgical revascularization. In the study, two groups of post MI patients with cardiogenic shock were stratified. Those who received intraaortic balloon pumping with pharmacologic therapy had a long-term mortality of 71%.
• By contrast, those who received early surgical revascularization in combination with an intraaortic balloon pump had a much lower mortality. While these data show a significant survival advantage with this approach to cardiogenic shock, not all hospitals are able to provide surgical resources in such a timely fashion.

Case 2 Complicated MI• While thrombolytic therapy may have reduced the incidence of
cardiogenic shock, large clinical trials such as the GISSI (33) trial have not demonstrated a reduction in mortality when thrombolytic therapy is given to patients in cardiogenic shock with an AMI.
• Percutaneous transluminal coronary angioplasty has been reported to improve survival in AMI complicated by cardiogenic shock. This approach has the advantage that it is faster and less invasive than surgery. In addition the rate of reperfusion is greater with direct PTCA compared to thrombolytic therapy and there is a lower rate of residual stenosis.
• In a retrospective trial, Lee et al (34) showed an impressive survivor benefit (50% vs 17%) in those patients undergoing emergent PTCA for cardiogenic shock compared with those who were managed with conventional therapy. This trial was performed retrospectively and the controls were not completely comparable to the angioplasty group; however, it represents the best data presently available.
• Therefore, our approach is to stabilize patients with cardiogenic shock with pharmacological support and the intraaortic balloon pump and then proceed directly to the catheterization laboratory.

Case 2 Complicated MI• Pharmacotherapy in cardiogenic shock is important in order to stabilize patients prior to
definitive coronary flow restoration. Clearly, in this clinical situation the goal is to optimize myocardial oxygen supply and minimize oxygen consumption. In patients who have isolated pulmonary congestion, therapy consists mainly of diuretics and anti-ischemic agents. This group of patients does not require emergent intervention except when post infarction angina occurs. Recent data prove the mortality benefit of ACE inhibitors in patients with chronic heart failure (35), and other information (36) suggests that treatment with captopril following myocardial infarction leads to lower left ventricular filling pressure and a smaller end-diastolic volume at one-year follow-up. In addition, exercise capacity appears to be improved. Whether these latter two effects will translate into improved longevity re-mains to be seen.
• In patients who have peripheral hypoperfusion without pulmonary congestion (Forrester Class III) an effort is made to find the optimal combination of PAOP and cardiac output (i.e. a clinical application of Starling's law). As previously noted this usually occurs at a PAOP between 14-18 mmHg. Beyond this range, further volume loading, usually precipitates hemodynamic and respiratory decompensation. If the patient remains hypotensive in spite of volume loading, inotropic therapy with agents such as dobutamine and dopamine are indicated. Pressor and inotropic support have multiple effects on myocardial oxygen supply and demand. Oxygen demand is increased by virtue of enhanced con-tractility and heart rate, whereas the increase in aortic diastolic pressure leads to improved oxygen supply. The net effect is to cause increase oxygen demand and this may precipitate further episodes of ischemia.
• In some circumstances, patients will respond nicely to inotropic support with dobutamine and with reasonable systolic blood pressure (> 100 mmHg) afterload reduction with sodium nitroprusside may be initiated thereby enhancing peripheral perfusion. For most Class III patients who require pressor support, the prognosis remains poor and the clinical strategy should revolve around early definitive revascularization of jeopardized but viable myocardium. This point is particularly obvious when one remembers the survival benefit from pharmacotherapy alone remains negligible.

Case 2 Complicated MI• In the patient example above incipient cardiogenic shock was
identified when insertion of the PAC revealed a cardiac index of 1.8 L/min/m2 with a PAOP of 18 mmHg, a mean artertial pressure of 65 mmHg and a low mixed venous saturation of 0.51.
• Dobutamine therapy was selected for this patient because of its selective, almost purely inotropic properties. By contrast dopamine, which also may be used, usually produces a significant chronotropic effect which may be deleterious to the balance between myocardial oxygen demand and supply. As shown in this case example our patient responded well to dobutamine and insertion of the intra-aortic balloon pump. This was manifested by the increase in cardiac index to 2.4 L/min/m2, the fall in PAOP to 14 mmHg, the improvement of mean arterial pressure to 75 mmHg and the increase in mixed venous saturation to 0.66.
• During his hospital course his CPK/MB peaked at 4800 IU with 20% MB. While there is no perfect correlation, CPK elevations of this magnitude usually signify extensive myocardial necrosis and a potentially fatal outcome from pump failure.

Cardiac Disease – Acute MI

Cardiac Disease – Acute MI

Cardiac Disease – Acute MI

Case 3 Ruptured Ventricular Septum• PATIENT 3: RUPTURED VENTRICULAR SEPTUM / John M. Phelan, Joseph
E. Parrillo
• A 54 year old woman with hypertension and non-insulin dependent diabetes presented to the emergency room with chest pain. She de-scribed substernal heaviness radiating to her back and left shoulder beginning four hours earlier with associated nausea and diaphoresis. The ECG revealed 3 mm ST segment elevation in V2 through V4 with ST depression in leads II, III, and AVE Examination revealed a pulse of 110 beats/min with a BP of 150/90 mmHg. There were no bruits and the neck veins were not distended. The lungs were clear. Cardiac exam revealed normal S, and S2 with a prominent S4. No murmurs were heard. The distal pulses were intact and the remain-der of the exam was normal. The chest x-ray was normal. Therapy was initiated with chewable aspirin, intravenous metoprolol, nitro-glycerin, heparin and t-PA. The CPK peaked at 3564 with 14% MB.
• During the first 5 days the patient did remarkably well without evidence of heart failure, hypotension, ventricular arrhythmia or further chest pain. On day 6 she complained of dyspnea and weakness. Examination revealed a BP of 90/60 mmHg with a pulse of 95 beats/min. Rales were heard in the lower half of her lung fields. Cardiac examination revealed a new third heart sound with a grade IV murmur heard best along the lower left parasternal border. The chest x-ray showed pulmonary vascular redistribution and the patient was transferred back to the CCU.
• A pulmonary artery catheter was inserted using the right internal jugular vein and the following hemodynamic data were demonstrated:

Case 3 Ruptured Ventricular Septum
•These data demonstrated the presence of a step-up in oxygen saturation between the right atrium (60%) and right ventricle (82%) signifying a left to right shunt from an acute rupture of the inter-ventricular septum.

Case 3 Ruptured Ventricular Septum•This calculation shows that pulmonary flow is 2.5 times
systemic flow. In this patient, the thermodilution cardiac output yielded a CO of 5.5 L/min. Thus, the systemic output is 2.2 L/min (5.5/2.5).•With these hemodynamic data, the patient was managed with sodium nitroprusside and dobutamine. Repeat hemodynamic and oximetry data several hours after initiation of therapy were:

Case 3 Ruptured Ventricular Septum• These hemodynamic data reveal that following therapy with
dobutamine and sodium nitroprusside the new step-up from the right atrium (66%) to right ventricle (74%) was smaller signifying diminution of the left to right shunt.
• This was confirmed by the shunt calculation (Qp/Qs) which shows the Qp/Qs, 1.3:1.0 following therapy compared with the Qp /Qs of 2.5:1.0 prior to the initiation of therapy. Of note, the total cardiac output increased from 5.5 L/min to 6.2 L/min with the effective systemic output rising from 2.2 L/min to 4.1 L/min following therapy.
• Thus the patient remained stable and was brought to the cardiac catheterization lab the following morningwhere coronary angiography revealed a 90% mid LAD obstruction, 70% proximal circumflex stenosis and 60% stenosis of the distal right coronary artery. Left ventriculography demonstrated severe anterolateral and apical hypokinesis with an LVEF of 38%. The LAO projection of the ventriculogram showed evidence of the interventricular septal defect.
• The patient was taken to the operating room where the VSD was closed with a dacron patch and 3 vessel coronary artery bypass was performed. One year later she remains well, has returned to work as a computer operator and is functionally class II (NYHA).

Case 3 Ruptured Ventricular Septum• Discussion
• This case demonstrates many of the features found in the acute rupture of the interventricular septum following myocardial infarction (37). This complication occurs in approximately 2% of all patients with myocardial infarction and is more common with anterior wall infarctions. When the VSD occurs in this setting, the apical septum is more commonly involved. By contrast in the setting of an inferior wall MI, rupture of the basal septum is more likely. Clinically one usually finds a harsh holosystolic murmur along the lower left sternal border with an associated thrill. The patient usually evolves biventricular failure over hours and survival appears to be dependent in part on right ventricular performance. In those patients who have sustained a right ventricular infarction (or have RV failure) outcome is considerably reduced. Medical management clearly is unacceptable because of a mortality that exceeds 90%. Prompt surgical intervention reduces mortality to 50% and should not be delayed.
• Analysis of the preceding case example demonstrates the valuable role of the pulmonary artery catheter in yielding the correct diagnosis. The presence of a significant step-up in oxygenation between the right atrium and right ventricle established the diagnosis of VSD. The large "v" wave (23 mmHg above the mean PAOP) also raised the possibility of acute mitral regurgitation. The specificity and sensitivity of this finding have been shown to be suboptimal. One report showed that large "v" waves were present in only 33% of patients with mitral regurgitation (38). Conversely 18% of patients with large v waves do not have mitral regurgitation. Other causes of prominent v waves are listed in Table 12.3. This patient's v wave clearly was not the result of mitral regurgitation as only a trivial amount of regurgitant flow was seen on left ventriculography. The likely explanation for the v wave in this example is the presence of an acute VSD with a non-compliant left atrium.

Case 3 Ruptured Ventricular SeptumTable 12.3. Differential diagnosis of a large v
wave in the pulmonary artery occulsion pressure tracing
• .Mitral Regurgitation/Stenosis• Aortic Regurgitation• Aortic Stenosis• Multivalvular Disease• Cardiomyopathy (Dilated and Hypertrophic)• Ventricular Septa] Defect• Pulmonary Hypertension• Pericardial Constriction• ASD

Case 4 Cardiac Tamponade• PATIENT 4: CARDIAC TAMPONADE/John M. Phelan,
Joseph E. Parrillo• A 37 year old man had undergone coronary artery bypass
surgery 4 weeks earlier. He returned to see his physician with complaints of lethargy and lightheadedness. His family had noted that the patient was intermittently confused.
• Physical examination revealed a BP of 85/55 mmHg with a pulsus paradoxus of 20 mmHg. The pulse was 125 beats/min and the temperature was 100.5°F. There, was jugular venous distension 8 cm above the clavicle at 45 degrees. The lungs were clear except for diminished breath sounds at the left base and cardiac examination revealed a normal S, and S2 without murmurs. gallops or rubs. The remainder of the exam was normal except for trace pretibial edema.
• The ECG showed sinus tachycardia with non-specific T wave abnormalities and the chest x-ray revealed marked cardiomegaly with a small left pleural effusion.

Case 4 Cardiac Tamponade• The patient was admitted to the hospital through the emergency
room where efforts to raise his blood pressure with fluids were unsuccessful; dopamine was begun. He developed tachypnea and a room air arterial blood gas showed: pH 7.47, PO2 54 mmHg with a saturation of 87% and PC02 28 mmHg. Upon transfer to the MICU, insertion of a pulmonary artery catheter yielded the following information:
• Site Pressure• Right Atrium 22 (mean)• Right Ventricle 42/24• Pulmonary Artery 40/22• Pulmonary Artery• Occlusion Pressure 23 mmHg• Cl = 1.8 L/min/m2• Equalization of diastolic pressures was clearly demonstrated.
Therefore, an echocardiogram was obtained and revealed evidence of a large pericardial effusion with diastolic collapse of the right ventricle. The patient was immediately transferred to the operating room where pericardial drainage was performed. His blood pressure improved and pressor support was weaned.

Case 4 Cardiac Tamponade• Discussion• This case clearly points out the utility of pulmonary catheterization in arriving at the proper
diagnosis. On a clinical basis, the diagnosis of cardiac tamponade is difficult. The most common physical finding is jugular venous distension. One may also observe tachypnea, tachycardia and pulsus paradoxus in about 80% of patients.
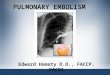
• Hemodynamic monitoring typically shows elevation and equalization of all diastolic pressures. The right atrial pressure tracing demonstrates a characteristic prominent systolic X descent with an absent Y descent. Right ventricular end diastolic pressure is elevated and equal to the right atrial, pulmonary artery diastolic and mean wedge pressures. The dip and plateau pattern characteristic of constrictive pericarditis is not seen. These findings are explained by the fact that the intrapericardial pressure is elevated and equal to the diastolic right atrial pressure so that the net transmural pressure is zero (Figure 12.4, panel A).
• Thus, rapid diastolic emptying of the right atrium (corresponding to the Y descent) is impeded. With compression of the cardiac cycle, the stroke volume falls prompting increased adrenergic tone leading to tachycardia and increased ejection fraction to maintain cardiac output. Systemic vascular resistance also in-creases in order to maintain blood pressure. Initial treatment of cardiac tamponade includes volume expansion with fluids and, if necessary, inotropic agents such as dobutamine. Rapid drainage should be performed. With pericardiocentesis, right atrial and intrapericardial pressures begin to fall (Figure 12.4, panel B) and when a sufficient amount is aspirated (panel C) all pressures re-turn to normal with reappearance of the Y descent. In post-operative cardiac surgical tamponade, pericardiocentesis should be employed only as a temporizing measure in order to stabilize the patient prior to surgical intervention.
• Pericardiocentesis may be used as definitive treatment in patients with a pericardial effusion due to malignancy, collagen vascular disease, or an inflammatory pericarditis.

Restriction Summary TableDiastolic Equilibration
Dip and Plateau Physiology
Constrictive Pericarditis
YES YES
Restrictive Cardiomyopathy
NO YES
Cardiac Tamponade
YES NO


Case 4 Cardiac Tamponade• Finally, the diagnosis of pericardial tamponade is
frequently suggested by the echocardiogram. • By itself, this technique may provide compelling
evidence for emergency pericardial drainage in hypotensive patients refractory to fluids or pressors. However, we believe that in the majority of circumstances the diagnosis of tamponade should be established by a pulmonary artery catheter. These critically ill patients frequently have co-existing problems (e.g. LV dysfunction, sepsis) that may obscure the response to pericardial drainage.
• We believe that baseline hemodynamic variables provide a crucial reference point for the management of these patients in the critical care setting.

Case 5 Vasodilator Therapy•PATIENTS 5a AND 5b: VASODILATOR THERAPY/ Charles M. Carpati, Mark E. Astiz, Eric C. Rackow
•Patient 5a:•A 71 year old man with a history of coronary artery disease was admitted with an anterior wall myocardial infarction. On exam ne was in moderate distress, blood pressure 132/82 mmHg. pulse 116 beats/ min, and respirations 28 breaths/min. Jugular venous distention was present at 45 degrees. Lung examination was remarkable for rales to the apices. The PMI was in the 5th intercostal space in the anterior axillary line. On auscultation both an S3 and an S4 were present, and a grade III/VI blowing holosystolic murmur radiating to the axilla was heard. The liver span was 13 cm, and there was +2 edema of the lower extremities. On laboratory exam sodium was 132 meq/1, BUN was 31 mg/dl and creatinine was 1.0 mg/dl. The electrocardiogram revealed anterior lead S-T elevations and the chest X-ray showed cardiomegaly with pulmonary edema.
•The patient was admitted to the coronary care unit and a pulmonary artery catheter (PAC) was placed for optimization of cardiac status. The initial physiologic profile is seen in Profile 12.2. #1.
• Profile 12.2, #2 shows a repeat hemodynamic study taken after nitroprusside was titrated to decrease the MAP approximately 10 mmHg.

Case 5 Vasodilator Therapy•Patient 5b:•A 42 year old man with a history of essential hypertension and medical noncompliance was admitted to the hospital with progressive shortness of breath, associated with headache and blurred vision. On physical exam he was in severe respiratory distress, blood pressure 244/178 mmHg, pulse 104 beats/min, and respirations 36 breaths/min. Fundoscopic examination revealed papilledema. Jugular venous distention was present to the angle of the jaw at 90 degrees. Lung examination revealed rales at the bases. The PMI was present in the 6th intercostal space in the midclavicular line and there was an S3 gallop. Abdominal exam was remarkable for paradoxical inspiratory movements. Lower extremities had +2 pitting edema.
•An electrocardiogram showed sinus tachycardia with left ventricular hypertrophy. A chest X-ray revealed a markedly enlarged cardiac silhouette and an alveolar pattern consistent with pulmonary edema. The hematocrit was 30.4%. Electrolytes were normal. The BUN was 52 mg/dl and creatinine 4.8 mg/dl. Urinalysis was remarkable for hemoglobin without red cells. Arterial blood gas on 100% FIO2 showed: pH 7.30, P02 57 mmHg and PCO2 51 mmHg.
•The patient was intubated and admitted to the intensive care unit where a PAC was placed. The initial hemodynamic profile is shown in Profile 12.3, #1. •He was started on intravenous nitroprusside, but proved extremely sensitive to this drug as shown in Profile 12.3. #2. Profile 12.3, #3 shows the patient's profile after fluid resuscitation.

Case 5 Vasodilator Therapy• Discussion• The treatment of acute and chronic congestive heart failure (CHF) has
continued to evolve over the past 10 years, coincident with further insight into the physiologic contributions of the endocrine and nervous systems to the syndrome. In addition to a better understanding of the benefits of digitalis and diuretics, vasodilator therapy has moved to the forefront of the treatment of this disease.
• Clinically, syndromes of heart failure are manifested to varying degrees by poor exercise tolerance, dyspnea and edema, as well as signs such as rales, gallops and elevated venous pressures. The hemodynamic hallmarks of congestive heart failure include a low cardiac output state induced by the inability of the ventricle to mount an adequate stroke volume. The decrease in effective circulating blood volume triggers a sympathetic release of catecholamines and activation of the renin-angiotensinaldosterone axis, as well as release of antidiuretic hormone.
• The catecholamines and angiotensin II are potent vasoconstrictors. Although adaptive for the maintenance of blood pressure, this effect results in an increased cardiac afterload and may worsen perfusion of vascular beds, contributing to organ dysfunction. Aldosterone and antidiuretic hormone release result in renal salt and water retention, an effect which may be exacerbated by renal vasoconstriction. These "maladaptive" responses perpetuate a vicious circle. Current therapy rests on manipulating contractility, preload and afterload.

Case 5 Vasodilator Therapy• Although potent intravenous inotropes exist to increase contractility
(dobutamine, amrinone, dopamine), their use is limited by a lack of oral analogues. Of the oral inotropes, only digoxin has proven to be of long-term benefit (39). It has been suggested that digoxin is less efficacious than vasodilator therapy in improving exercise tolerance (40). Vasodilators can act preferentially on the venous bed, the arterial bed or can be balanced in activity (Table 12.4). Agents acting to increase the capacitance of the venous bed may be effective in heart failure by decreasing preload and wall tension. Arterial vasodilation decreases afterload, i.e. the impedance to left ventricular ejection, thereby increasing cardiac output and stroke volume. Vasodilator therapy may result in hypotension and tachycardia either through excessive reduction in venous return or preload, or through excessive decrease in arterial resistance.
• Table 12.4. Mechanisms of action of vasodilators• VENODILATION• Diuretics• Nitrates (Low Dose)• ARTERIAL DILATION• Hydralazine Diazoxide• Minoxidil• Nifedipine• MIXED VENOUS AND ARTERIAL• ACE Inhibitors Nitroprusside Nitrates (High Dose)• Prazosin• Trimethaphan Phentolamine

Case 5 Vasodilator Therapy• Patients in acute heart failure manifest low cardiac outputs, high filling (wedge)
pressures, and high systemic vascular resistances. In the acute setting a parenteral vasodilator with a short half-life that is easily titratable should be utilized. This therapy should only be used in an intensive care setting with continuous blood pressure monitoring. Nitroprusside toxicity usually consists of reflex tachycardia or the toxicity of its breakdown product, thiocyanate. In congestive heart failure with systolic dysfunction, filling pressures will be high and vasodilation will result in decreased afterload and decreased end-diastolic volume as manifested by a decrease in wedge pressure. Goals of therapy should be the reduction of filling pressures and an increase in cardiac index without a deleterious fall in blood pressure. This is seen in Patient 5a, Profile 12.2.
• Note that in accelerated or malignant hypertension, filling pressures may actually be low. Vasodilation may then result in precipitous hypotension which should be treated by lowering the dose of vasodilator; blood pressure lability in this setting may re-quire the infusion of fluid. This is shown in Patient 5b, Profile 12.3. Treatment with nitroprusside resulted in a decrease in the filling pressures, an increase in cardiac output and decrease in systemic resistance but the decrease in blood pressure and after-load was too great and caused severe tachycardia. A decrease in nitroprusside together with fluid therapy led to a more gradual decrease in blood pressure and resistance, a greater cardiac out-put, stroke volume index, stroke work, mixed venous oxygen saturation and oxygen delivery and a lower arteriovenous oxygen content difference and oxygen utilization ratio. As noted, dose optimization in hypertension is achieved by measuring cardiac out-put, stroke volume or stroke work at sequentially titrated blood pressures; other indices of perfusion, such as mixed venous oxygen tension and arterial lactates, may also be followed. Conversion to oral therapy can then accompany tapering of intravenous therapy.

Case 5 Vasodilator Therapy• Other intravenous agents, such as hydralazine (direct arteriolar dilator),
diazoxide (direct arteriolar dilator), trimethaphan (ganglionic blocker), and phentolamine (alpha-blocker) are less ideal than nitroprusside in the acute setting because of longer half-life, lack of titratability or expense. Intravenous nitroglycerin may accomplish similar goals as nitroprusside; however, this agent causes more venodilation at low doses.
• At present, angiotensin converting enzyme (ACE) inhibitors or the combination of isosorbide dinitrate with hydralzine are themost commonly used oral therapy for vasodilation. Studies have demonstrated long-term benefit of these agents in improving survival in chronic CHF (41,42). Both ACE inhibitors and hydralazine/isosorbide dinitrate maintain a long-term increase in cardiac ejection fraction. Captopril has been associated with an increase in long-term exercise tolerance in patients with congestive heart failure (43).
• Hydralazine/isosorbide dinitrate is associated with lowered norepinephrine levels when compared to captopril in chronic CHF (44). ACE inhibitors may affect renal and hepatic function adversely, as well as lower white blood cell counts. Hydralazine is associated with reflex tachycardia and a lupus-like syndrome.
• Other oral vasodilators, such as nifedipine (calcium channel blocker), although possibly useful in the acute setting, have not been shown to improve mortality. Both nifedipine and minoxidil (direct arteriolar dilator) have been associated with no-table renal salt and water retention.
• Although the short-term effects of prazosin (alpha-1 blocker) are similar to those of the other vasodilators, the development of tachyphylaxis, possibly as a result of alpha-1 receptor downregulation, mitigates against its long-term benefit (45).

Case 9 Septic Shock• PATIENT 9: SEPTIC SHOCK/Debora G. Geber, Charles L. Sprung• A 52 year old woman presented with chills, fever, disorientation, re-current
vomiting and oliguria, three days after an uneventful elective extracorporeal shock wave lithotripsy. She had a previous history of nephrolithiasis, non-insulin dependent diabetes mellitus and recurrent urinary tract infections.
• The physical examination revealed a prostrated patient with blood pressure 100/45 mmHg, pulse 120 beats/min, respirations 40 breaths/min and temperature 39°C. The laboratory data showed hemoglobin 8 gm/dl, white blood cell count 13,100/cu mm, platelets133,000/cu mm, sodium 138 meq/1, potassium 5.1 meq/1, BUN 44 mg/dl, glucose 180 mg/dl, and creatinine 2.5 mg/dl. Chest x-ray was normal and EKG showed sinus tachycardia. Cultures were obtained and the patient was started on mezlocillin and gentamicin.
• The day after admission the patient's systolic blood pressure dropped to 70 mmHg and the arterial blood gases on FI02 0.6 were: pH 7.38, PaO2 42 mmHg, PaCO2 49 mmHg, and 02 saturation 75%. Another chest x-ray showed diffuse bilateral infiltrates. The patient was transferred to the intensive care unit, volume resuscitated, intubated and started on intravenous inotropes and vasopressors.
• A pulmonary artery catheter was inserted and the initial hemodynamic profile can be seen in Profile 12.7, #1. Blood cultures taken on admission grew E. coll. The patient also received monoclonal anti-bodies against endotoxin (HA-1A) as part of a clinical research study. The patient remained oliguric, uremic and therefore hemodialysis was started. Mechanical ventilation was maintained with high FI02 and high PEEP values.

Case 9 Septic Shock

Case 9 Septic Shock• The next day's hemodynamic profile measured when the patient
was under treatment with dopamine 12 mcg/ kg/min, dobutamine 10 mcg/kg/min and norepinephrine 3 mcg/min is shown in Profile 12.7, #2.
• Four days after admission to the ICU and aggressive treatment with fluids, dopamine, dobutamine, norepinephrine, antibiotics, TPN, blood components and hemodialysis, her hemodynamic parameters became more stable. The dopamine dose was reduced to 3 mcg/kg/min, the dobutamine dose to 5 mcg/ kg/min, and the norepinephrine was discontinued (Profile 12.7, #3).
• Two days later the patient was successfully weaned from the ventilator. She had no fever and good urinary output, therefore no further hemodialysis was needed. Nine days after admission the patient was discharged from the intensive care unit and subsequently to her home.

Case 9 Septic Shock• Discussion• Septic shock is a severe medical problem that has been increasing in incidence
over the past few years (61). It is now the most common cause of death in intensive care units (61). The high incidence of sepsis today is paradoxically linked to advances in modern medical technology including an increase in patient age, greater number of immunocompromised patients as a consequence of the use of cytotoxic drugs and radiotherapy, the wider use of invasive techniques and devices such as catheters, and the emergence of antibiotic resistant microorganisms (61,62). De-spite all of the medical progress, septic shock still carries an unacceptably high mortality. Therefore it is imperative to elucidate the pathophysiology of sepsis and septic shock in order to provide our patients with better treatment and an improved outcome.
• The most common pathogens that cause sepsis are the gram-negative bacilli but sepsis may also follow gram-positive infections (62). It is believed that many of the profound hemodynamic changes that occur in septic shock are due to endotoxin released by microorganisms, which activate other mediators such as cytokines, tumor necrosis factor, interleukins, myocardial depressant substance and others. The latter appears to exert direct myocardial effects responsible in part for the abnormal myocardial function seen in septic shock (63).
• The action of endotoxins in septic patients results in an impairment of vasomotor control (64). The loss of vasomotor tone decreases systemic vascular resistance (SVR) resulting in hypotension and shock. A baroreceptor reflex increases cardiac output and a hyperdynamic cardiovascular state ensues with an elevated cardiac index (64,65). Ventricular function is abnormal with a decreased right and left ventricular ejection fraction. (61-64,66).

Case 9 Septic Shock• As a consequence, end-systolic and diastolic volumes will increase and
ventricular dilation occurs (63). The cardiac output remains elevated despite the decreased ejection fraction because of the increased heart rate. Failure to achieve an appropriately augmented cardiac output results in hypotension which together with the decreased SVR further aggravates shock. In septic shock there, is an increase in microvasculac permeability which leads to extravasation of albumin and fluid. from the intravascular compartment causing generalized tissue edema. This edema further impairs the micro-circulation aggravating the maldistribution of blood flow (64).
• Patients suffering from septic shock fail to extract oxygen normally and are
highly dependent on oxygen supply (DO2) to maintain oxygen consumption (VO2) and aerobic metabolism (67,68). The maldistribution of blood flow, peripheral arteriovenous shunting, cellular damage and tissue edema have all been implicated as causative factors of the ineffective oxygen utilization (66). The impaired capacity of oxygen metabolism results in a high mixed venous blood oxygen saturation and narrow arteriovenous oxygen difference (avDO2)(66,67). On the other hand, because of the hyperdynamic state, patients have high oxygen requirements. When oxygen delivery, even though augmented, is not sufficient to maintain aerobic metabolism, oxygen extraction by peripheral tissues will be deficient and blood lactate concentrations will in-crease (68). If the relationship between oxygen supply and demand is not restored quickly and the shock state is inadequately treated, irreversible tissue damage occurs in multiple sites. Multiple organ failure is most common in septic patients and worsens the clinical picture and prognosis.

Case 9 Septic Shock• In addition to lactic acidosis other metabolic derangements occur in sepsis
including hypoxemia, hyperglycemia, hyperuricemia, hypocalcemia, hypertriglyceridemia, and respiratory alkalosis (62,66).
• Successful management of septic shock requires an organized strategy and aggressive therapy from the onset. The corner-stone of management is the use of broad spectrum antibiotic agents, until the pathogen it definitely isolated and the sensitivity to antibiotics veriiicd, a.id removal of any possible source of infection such as pus, catheters or prostheses. Correction of hypotension must be made with adequate fluid resuscitation. The use of the pulmonary artery catheter (PAC) may help to ensure an adequate left ventricular preload while avoiding pulmonary edema (68,69). Despite adequate volume infusion, hypotension frequently persists. It is then necessary to add inotropic and vaso-
• pressor agents such as dopamine, dobutamine, norepinephrine and/or epinephrine (61,62,69,70). Maximizing DO2 is also an important part of hemodynamic resuscitation and prevention of multiple organ failure (68,71). To achieve this goal, one can in-crease cardiac output by the use of volume and/or inotropes. In addition, the arterial oxygen saturation should be maintained above 90% by the use of increasing FIO2. mechanical ventilation. PEEP, respiratory physiotherapy and/or pulmonary toilet. When anemia is present, transfusion of packed red blood cells should be considered (71).
• The use of high dose corticosteroids is no longer controversial. In addition to the possibility of superinfection, hyperglycemia and gastrointestinal bleeding in corticosteroid-treated patients, large trials have shown some evidence of increased mortality and no beneficial effect of corticosteroids in preventing or reversing shock in septic patients (72-74).

Case 9 Septic Shock• Recently, trials employing human monoclonal antibodies against endotoxin have
shown improved survival in patients with gram-negative bacteremia (75). The use of continuous arteriovenous hemofiltration associated with plasmapheresis and dialysis may also be of use in patients suffering from sepsis and multiple organ failure (76). The search for new methods to treat patients with sepsis and septic shock continues. Trials are currently under way to assess monoclonal antibodies to tumor necrosis factor and to interleukin-1 receptor antagonists.
• The present patient developed septic shock four days after an extracorporeal shock wave lithotripsy. When analyzing the initial hemodynamic profile (Profile 12.7, #1), one can see that the patient had a rapid heart rate which maintained the high cardiac output despite the low stroke index. The high cardiac output, low systemic vascular resistance and narrow arterio-venous oxygen difference are typical of the hyperdynamic picture found in patients with septic shock.
• Arterial hypoxemia was also present, despite mechanical ventilation with high FIO2 and PEEP, secondary to an increased pulmonary shunt fraction related to the adult respiratory distress syndrome (ARDS), frequently accompanying septic shock. This hypoxemia associated with the low hemoglobin contributed to the relatively low oxygen delivery. In clinical circumstances, oxygen delivery is in excess of what is needed and oxygen consumption is supply independent. As stated before, beyond a critical level, tissues fail to extract oxygen adequately and are unable to sustain aerobic metabolism, switching then to anaerobic metabolism and increasing the lactate production (77).

Case 9 Septic Shock• At this stage oxygen consumption is decreased and so one can say it becomes
supply dependent. In normal individuals this critical level is about 300 ml/min/m2. In septic shock patients it is necessary to have a higher delivery as the critical level is about 600 ml/min/m2 which corresponds to an oxygen consumption of 170 mUmin/m2 (78,79). In Profile #1, it can be seen that oxygen de-livery is far below the amount needed and so is oxygen consumption. The decreased oxygen consumption and low extraction ratios lead to normal or even high mixed venous saturation in septic patients. The low V02 and high venous oxygen saturation associated with the arteriovenous peripheral shunt are responsible for the narrow a-v oxygen difference found.
• A repeated hemodynamic study (Profile 12.7, #2) was taken after the patient was better ventilated and oxygenated with a high FI02 and PEEP and received blood components. She was also receiving inotropic and vasopressors agents. It demonstrated improvement of arterial oxygen saturation and an increase in oxygen delivery and consumption and consequently a better oxygen extraction ratio. The avDO2 was wider, however there was still a hyperdynamic state with high CO and heart rate and low systemic and pulmonary resistances. The next hemodynamic profile (Profile 12.7, #3) shows an increase in systemic vascular resistance and arterial blood pressure and lower heart rate. All of this was probably related to the resolution of the septic shock state, resulting in a decrease in cardiac output. The pulmonary shunt fraction was much lower and the arterio-venous 02 difference wider. The patient had almost normal parameters and was successfully recovering from the severe illness which made it possible to wean the dopamine, dobutamine and norepinephrine. Cardiac index was restored to almost normal values. Two days later the patient had good urinary output and tachypnea disappeared. She was transferred from the intensive care unit four days after this last profile was taken.

Case 9 Septic Shock

Case 10 Post Traumatic Shock and ARDS• PATIENT 10: POST TRAUMATIC SHOCK AND THE ADULT
RESPIRATORY DISTRESS SYNDROME (ARDS)/Loren D. Nelson• A 17 year old woman was ejected from a high speed motor vehicle
crash. She sustained severe multiple trauma and was brought to the Trauma Center with a known closed head injury, multiple facial lacerations, bilateral femur fractures, bilateral pneumothoraces, and multiple rib fractures bilaterally, bilateral pulmonary contusions, and significant hypotension with a distended abdomen. She was taken immediately to the operating room where an exploratory laparotomy was performed.
• She was found to have a grade IV liver laceration and a splenic avulsion at the hilum. A splenectomy was rapidly performed and attention was turned to the liver laceration. Marked bleeding from deep in the parenchyma of the liver could not be controlled by the usual surgical methods. The patient, at this time, had lost more than 15 units of blood and was becoming hypothermic with a core temperature of 33°C. Because of her falling temperature and continued bleeding, the liver injury was packed with laparotomy sponges and the abdomen was closed.
• The patient was taken to the Surgical Intensive Care Unit for hemodynamic monitoring and ventilatory support. A chest x-ray demonstrated diffuse bilateral pulmonary infiltrates consistent with ARDS.

Case 10 Post Traumatic Shock and ARDS• On arrival in the SICU, the patient was on 100% oxygen, 5 cm H2O of PEEP,
and an IMV rate of 14. Initial arterial blood gases showed: pH 7.3, PO2 40 mmHg with a saturation of 75%, PCO2 30 mmHg, and Sv02 of .45, and a cardiopulmonary profile demonstrated in Profile 12.8, # I. The initial CI was low but yet the oxygen utilization coefficient or oxygen extraction ratio (OUC) was greatly elevated implying that oxygen delivery (D02) was inappropriately low for the current (normal or slightly elevated) oxygen consumption (V02). However, Cl was being maintained by a very high heart rate, indicating a low stroke index. The low stroke index with tachycardia and high OUC in the presence of a low PAOP suggested intravascular volume depletion.
• Because of the profound acute respiratory failure (99/9-0.57), the patient was treated with increasing levels of positive end-expiratory pressure in order to improve the functional residual capacity and peripheral oxygen delivery. Using the pulse oximeter and continuous mixed venous oximeter, the end-expiratory pressure was titrated up and the FIO2 was reduced in an attempt to lower the toxic inspired oxygen concentration and improve intrapulmonary shunting. Because the patient had initially low filling pressures (CVP = 10 mmHg, PAOP = 12 mmHg), she received additional intravenous fluid boluses to augment ventricular preload to improve stroke volume and cardiac output. This is especially important in patients on PEEP since some of the increases in airway pressure (de-pending upon the relationship between lung and chest wall compliances) will be transmitted to the pulmonary vasculature and perimyocardial space. The effect of increases in transmitted pressure will be to increase right ventricular afterload and decrease left atrial transmural pressure. Both of these effects may lower left ventricular preload and may account for a reduction of cardiac index sometimes seen during high levels of PEEP.

Case 10 Post Traumatic Shock and ARDS• Fifteen minutes after admission, the patient was on 18 cm H2O
of PEEP and the FIO2 was reduced to 0.6. This produced a 90% arterial saturation and a 62% venous saturation with an estimated oxygen utilization coefficient of 0.31 and intrapulmonary shunt of 0.39.
• The PEEP was further increased and the second arterial blood gas was obtained. At this point, the FI02 was 0.5 and the shunt was reduced to 0.32. Fifteen minutes later following an IMV change andan increase in the PEEP to 22, the FI02 was reduced to 0.4 and the arterial oxygen tension had increased to 80 with a saturation of 96%.
• The mixed venous oxygen saturation, however, had fallen to 0.60 and the OUC had increased to 0.38. The shunt fraction had decreased to 0.17 but because the patient was showing signs of impaired oxygen transport with a worsening of her metabolic acidosis, a fluid bolus was administered and 15 minutes later, another blood gas was obtained.
• At this time, the intrapulmonary shunt fraction was 0.19, the oxygen utilization coefficient was 0.28, and the PaO2 was now 85 on 22 of PEEP, and IMV of 4, and 40% oxygen.

Case 10 Post Traumatic Shock and ARDS• Discussion
• This patient demonstrated the utility of arterial and venous continuous saturation measurements in the titration of high levels of positive end-expiratory pressure (PEEP). The rapid titration ofincreasing levels of PEEP and decreasing FI02 was accomplished over a period of 15 minutes without additional blood gases. Several other alterations in ventilatory support were achieved. Blood gases were obtained for the evaluation of pH and PCO2 following IMV changes.
• A total of 14 ventilator changes were made in a period of less than 60 minutes. The patient's oxygenation support with in-creased levels of PEEP allowed normalization of the intrapulmonary shunt to 0.19 and an improvement in the Pa02/FI02 ratio from 40 to 213 mmHg. It is generally true that diverging values of SaO2 and SvO2 indicate greater peripheral utilization of oxygen or lower central shunting. Converging values, on the other hand, generally indicate lesser peripheral oxygen utilization or greater venous admixture (right-to-left shunting).

Case 10 Post Traumatic Shock and ARDS• If SaO2 decreases, the oxygen utilization coefficient will in-
crease implying a greater consumption of delivered oxygen. OUC = V02/D02 but if the small amount of oxygen dissolved in the plasma is ignored OUC = (SaO2 - SvO2)/SaO2. The diverging SaO2 and SvO2 indicate greater utilization of oxygen.
• If SvO2 is stable and SaO2 decreases, it is most likely that right-to-left intrapulmonary shunting has increased. Normally the magnitude of shunting is estimated by calculating the physiologic shunt fraction (venous admixture):
• Qs/Qt = (Cc'02 - CaO2)/ (Cc'02 - Cv02)• If the small volumes of oxygen dissolved in the plasma are
ignored, an estimate of venous admixture can be calculated as:• 1 - SaO2/ 1 - SvO2• Thus converging values of SaO2 and SvO2 (when SvO2 is
stable) imply worsening venous admixture. Obviously, these hold true only when hemoglobin concentration and FI02 are constant. The combined use of arterial and venous oximetry in this critically ill patient shortened the time to the therapeutic end-point and al-lowed more frequent measurements with fewer expenditures of resources.

SvO2 Decision Tree