Embed Size (px)
Citation preview
Dr. Sunil SookramMAvMed, MD, CCFP, FRCPC
Clinical ProfessorDepartment of Emergency Medicine
University of AlbertaMedical Director: AHS IFS & Dispatch, STARS Grande Prairie
Objectives
To showcase current Civil Aviation Medical Response Resources
To highlight areas of physician involvement in Aeromedical Transport
To explore how Retrieval Medicine has evolved in Canada.
Today’s Educational Journey
3 real clinical vignettes
Case #1 – Airline Role
Case #2 – Member of Transport Team
Case #3 – Quarterback of Patient Care
Case #1
Flying on a Malaysian Airlines flight B737 –Hong Kong to KL
Steward comes over to you about 2 hrs into flight (3.5 hrs)
Have a sick patient in the back and wonder if you can help out and have a look.
Situational Awareness
Flight Manifest contains titles (Dr.)
Most airline flights have someone (Dr., Nurse, Paramedic) that has advanced medical training statistically
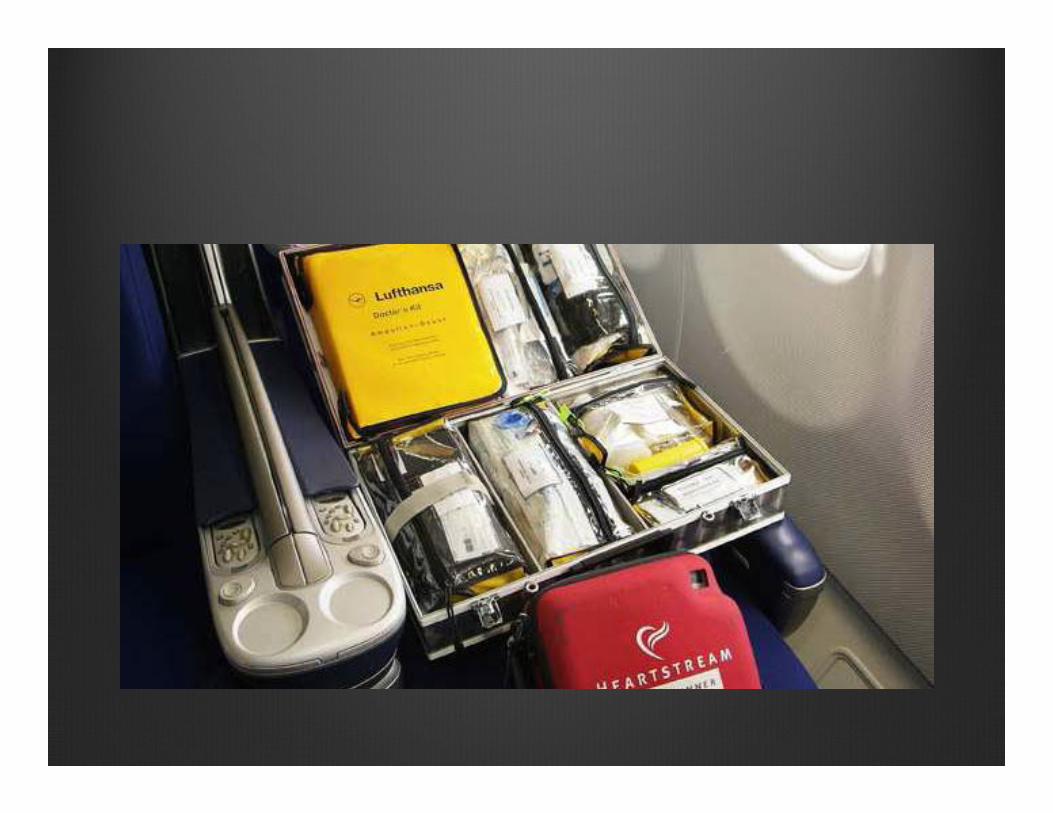
Airlines have a medical kit and most have AED - even discount airlines
North American Airlines and many international airlines subscribe to Medical Assist Companies that provide 24/7 online medical support (i.e. MedLink)
The Sequence of Events
Patient assessed, while navigating medical kit patient starting vomiting and then suddenly arrested
Cardiac arrest run on plane utilizing AED and ACLS drugs within medical kit – help from travelling ICU Nurse and my wife
Kit has limited Epi, bicarbonate, crystalloid fluid because of weight and size
Need to liaise with pilot through flight attendants letting them know progress and medical needs.
The Aircraft Commander (Captain) will make logistical and operational decisions on diversion based upon information provided.
Back to case
Decision to divert was withheld as we were over the sea and 1.5 hrs to destination
Rapid descent process employed to get us on the ground and can hurt ear drums and added vestibular issues of other passengers
Very captive audience watched rescuscitation versus onboard entertainment system
Work with aircrew to meet patient’s immediate needs
Copyright/License ► Request permission to reuse
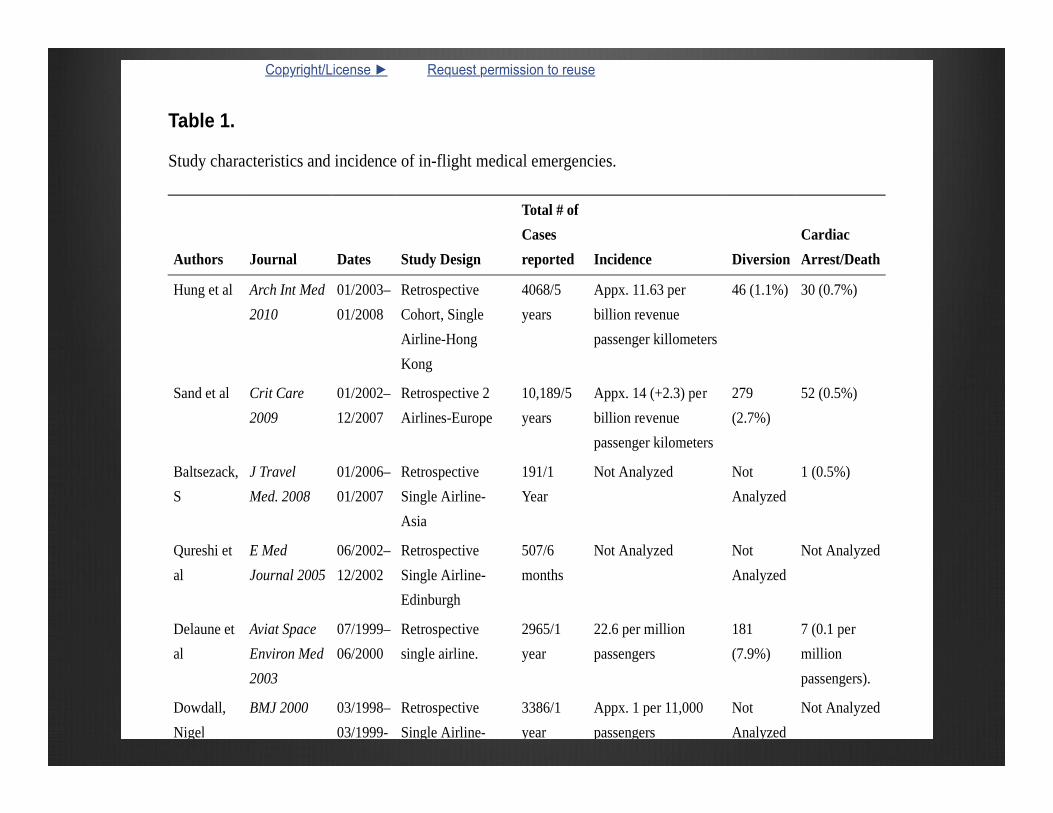
Table 1.
Study characteristics and incidence of in-flight medical emergencies.
Authors Journal Dates Study Design
Total # ofCasesreported Incidence Diversion
CardiacArrest/Death
Hung et al Arch Int Med2010
01/2003–01/2008
RetrospectiveCohort, SingleAirline-HongKong
4068/5years
Appx. 11.63 perbillion revenuepassenger killometers
46 (1.1%) 30 (0.7%)
Sand et al Crit Care2009
01/2002–12/2007
Retrospective 2Airlines-Europe
10,189/5years
Appx. 14 (+2.3) perbillion revenuepassenger kilometers
279(2.7%)
52 (0.5%)
Baltsezack,S
J TravelMed. 2008
01/2006–01/2007
RetrospectiveSingle Airline-Asia
191/1Year
Not Analyzed NotAnalyzed
1 (0.5%)
Qureshi etal
E MedJournal 2005
06/2002–12/2002
RetrospectiveSingle Airline-Edinburgh
507/6months
Not Analyzed NotAnalyzed
Not Analyzed
Delaune etal
Aviat SpaceEnviron Med2003
07/1999–06/2000
Retrospectivesingle airline.
2965/1year
22.6 per millionpassengers
181(7.9%)
7 (0.1 permillionpassengers).
Dowdall,Nigel
BMJ 2000 03/1998–03/1999-
RetrospectiveSingle Airline-
3386/1year
Appx. 1 per 11,000passengers
NotAnalyzed
Not Analyzed
Take Away Lessons for EM Physicians
Be prepared
Utilize the resources at hand (people, equipment, online support)
Work with Aircraft Commander to make informed decisions factoring patient need and operational decisions
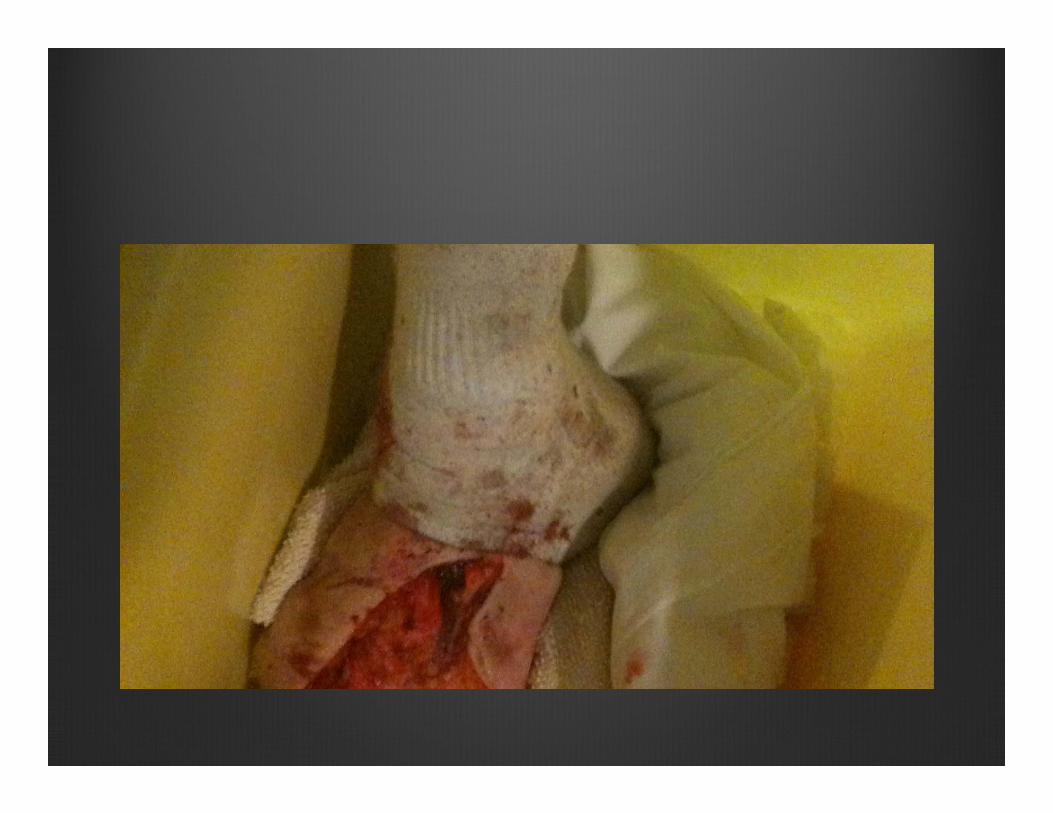
Case #219 yo female drinking and driving. Car stuck lamp pole and drove front end of car posteriorly. Pttrapped in car for prolonged period. 2.5 hrs trying to extricate
“Remove vehicle from patient”
Due to lengthy period of entrapment, primarily 1 very trapped leg under dashboard, consideration of field amputation is made by on scene commander .
Aeromedical crew sent out to transport. Physician accompaniment
The Role of The Physician on Scene
Limited
Aeromedical crews highly trained and get enhanced training and experience compared to their ground based colleagues
Role of Physician on on Mission:Master Triager (Disaster Scene)Advanced skills (USS, Central Line, Chest Tube, RSI)Unique situations (Obstetrics, field amputation)

Strategic Medevac – InterfacilityTransfer
Long Distance (transAtlantic, transPacific), foreign countries
Facilitates transfer of care (heterogenousmedical capabilities around world)
Bringing definitive care to patient on occasion
Medical Diplomacy – building bridges, “field supervision”, teachable moments for rural providers.
Case #3: Patient Quarterback
ORNGE Transport Physician Consultant
STARS Transport Physician
BC – Emergency Physician On line Support
“The Future of Physician On Line Medical Support for a Transport System”
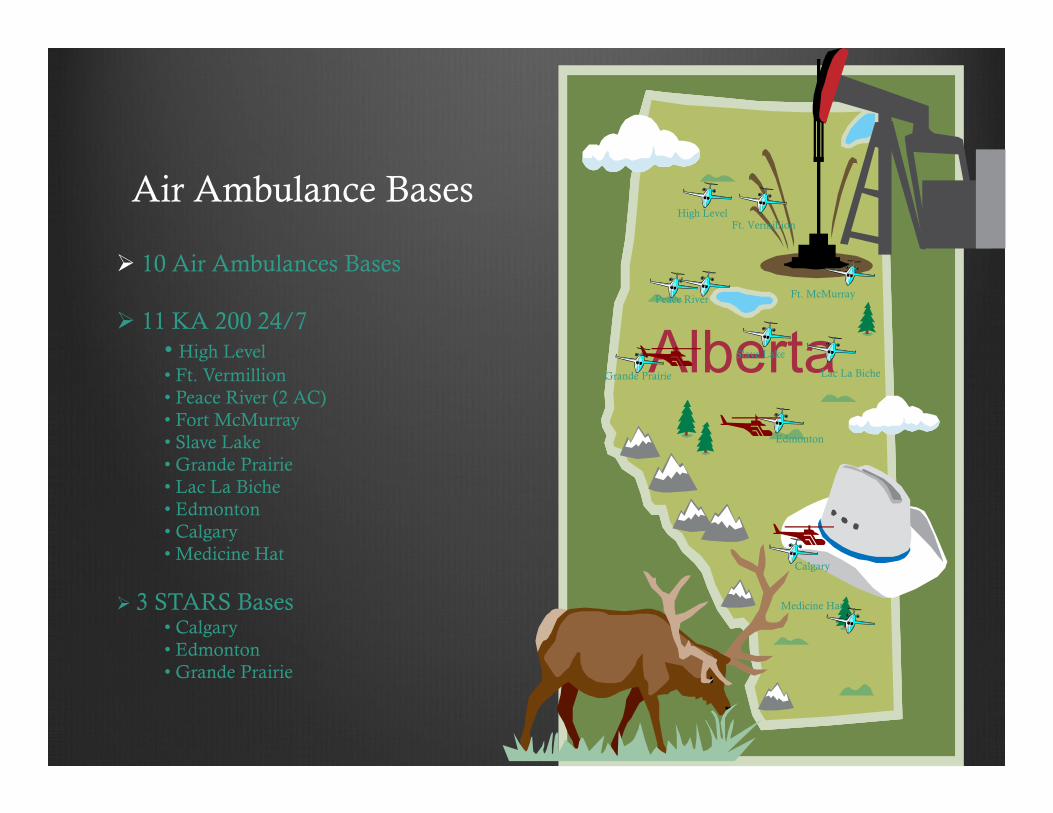
Air Ambulance Bases
Alberta
10 Air Ambulances Bases
11 KA 200 24/7• High Level• Ft. Vermillion• Peace River (2 AC)• Fort McMurray• Slave Lake• Grande Prairie• Lac La Biche• Edmonton• Calgary• Medicine Hat
3 STARS Bases• Calgary• Edmonton• Grande Prairie
High LevelFt. Vermillion
Peace River Ft. McMurray
Slave Lake
Lac La BicheGrande Prairie
Edmonton
Calgary
Medicine Hat
Case #2
Nov 3rd 2 calls occurring simultaneously
Call #1 – hypotensive, shocky 67 yr old female in Mayerthorpe with perforated viscus. Through Red Patient Referral Process. Dispatch STARS-3 and gave rescuscitation advice to local doctor.
NG tube, fluids, Inotropic support, organized receiving surgeon
Helicopter dispatched and call from Wainwright EMS requesting scene RV with STAR-3
Initial Thoughts
Cardiac Arrest – dismal outcome, trauma arrest
CAF member – “full court press”
Similar efforts for RCMP, Fire, EMS, public safety
Then What ?ROSC of CAF mbr.
STARS Helicopter too far north
FW resources unable to land at Wainwright due to weather. Can only land in Lloydminster 1 hr away.
Both patients need Critical Care Transport to Tertiary Care expeditiously
Ground transport from Wainwright to Edmonton – 2 hrs with very inexperienced ground crew.
Physician accompaniment from Wainwright not possible.
What Transpired
Medical Care
TP called Wainwright Hospital, spoke to local physician
Appreciated that local physician needed help
Called local GP Anesthesia, who came in to help manage patient
What Transpired
Transport Medicine – Operational Aspects
No STARS, FW and Ground nonoptimum with current resources
Called CFB Edmonton Base Hospital – spoke to one of Flight Surgeons and he prepared to mobilize AE Team from ad hoc resources
Called RCAF 408 THS Flight Ops – rapid mobilization of Griffon with crew. FE reconfigured helicopter for Medevac
Spoke to Flt Surg to bring appropriate AE kit
Spoke to Wainwright Hospital to borrow ventilator, GP Anesthesia (was former Flt Surgeon)
Dispatched RCAF Helicopter to Wainwright Hospital with Ad Hoc AE team.
Provided ongoing TP OLMC to Flt Surg en route outbound, and at scene to prepare patient, inbound leg via text
Helipad at UAH needed to be secured and team prepared to receive at rooftop
Called UAH ED and prepared team, spoke to Trauma Team to prepare through Charge Nurse


Extreme Example
“massaging” the resources to meet the patient need
Physician role is “quarterbacking” patient journey
Active collaboration with Operational Coordinators to meet patient needs
Active real time support to caregivers in the field with minimal time delay
Summary
Physician as reluctant caregiver on commercial airliner
Physician as active member of aeroretrievalteam
Physician as “quarterback” of patient transport journey