Embed Size (px)
Citation preview

Burns…Burns…Back to Basics 2009Back to Basics 2009
Dr. Jennifer Clow, CCFP (EM)Dr. Jennifer Clow, CCFP (EM)

Case:Case:
45 y. o. male, working in shed45 y. o. male, working in shed Wood-burning stove for heat…Wood-burning stove for heat…
– Thinks stove is cold – adds more wood, Thinks stove is cold – adds more wood, then pours lighter fluid on topthen pours lighter fluid on top
– Stove explodesStove explodes Patient and shed on fire!!!Patient and shed on fire!!! Brought in by paramedics to your Brought in by paramedics to your
ER…ER…

Case, cont’dCase, cont’d
What do you want to do???What do you want to do???– AirwayAirway– BreathingBreathing– CirculationCirculation– DisabilityDisability– ExposureExposure
What other information do you need?What other information do you need?

Case, cont’dCase, cont’d
History…History…– Wood-burning stoveWood-burning stove– Door open at time of exposureDoor open at time of exposure– Flash caught patient’s clothing on fireFlash caught patient’s clothing on fire– Patient ran from burning shed Patient ran from burning shed
immediatelyimmediately– No toxic chemicals in shedNo toxic chemicals in shed
PMHxPMHx Meds/SocialMeds/Social

Case, cont’dCase, cont’d
Physical ExaminationPhysical Examination– Hemodynamic stability?Hemodynamic stability?– Depth and extent of burns – TBSA?Depth and extent of burns – TBSA?– Any facial burns?Any facial burns?– Signs of inhalational injury?Signs of inhalational injury?– Circumferential burns?Circumferential burns?– Any associated traumatic injuries?Any associated traumatic injuries?– Signs of poisoningSigns of poisoning

The info…The info…

Causes of burns…Causes of burns…
Thermal – flame, flash, contact, scaldThermal – flame, flash, contact, scald Electrical – high/low voltage, Electrical – high/low voltage,
lightninglightning Chemical – acid, alkaliChemical – acid, alkali Radiation – UV, therapeuticRadiation – UV, therapeutic

Clinical Evaluation of BurnsClinical Evaluation of Burns

Burn DepthBurn Depth
11stst degree – just epidermis degree – just epidermis 22ndnd degree – dermis degree – dermis
– SuperficialSuperficial– DeepDeep
33rdrd degree – full thickness degree – full thickness 44thth degree – involves muscles, bones, deep degree – involves muscles, bones, deep
organsorgans

Burn depth….Burn depth….
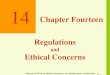
Figure 43-3. Layers of the skin, showing depth of first-, second-, and third-degree burns. (Reproduced, with permission, from Way LW [editor]: Current Surgical Diagnosis & Treatment, 9th ed. Appleton & Lange, 1991.)

First degreeFirst degree
Skin is red, tender, drySkin is red, tender, dry No blister formationNo blister formation e.g. sunburne.g. sunburn Usually heals within 7-10 daysUsually heals within 7-10 days Does not scarDoes not scar

First Degree BurnFirst Degree Burn

Second DegreeSecond Degree
Superficial Partial ThicknessSuperficial Partial Thickness– Blisters, very painfulBlisters, very painful– Dermis exposed – red, moist, good Dermis exposed – red, moist, good
capillary refillcapillary refill– Heals within 2-3 weeksHeals within 2-3 weeks– Minimal scar formationMinimal scar formation

Second Degree BurnSecond Degree Burn

Second Degree BurnSecond Degree Burn

Second Degree, cont’dSecond Degree, cont’d
Deep Partial ThicknessDeep Partial Thickness– Skin is white/yellowSkin is white/yellow– Minimal pain – difficult to differentiate Minimal pain – difficult to differentiate
from third degree by inspectionfrom third degree by inspection– Cap. Refill, pain sensation absentCap. Refill, pain sensation absent– Pressure felt, 2 point discrimination Pressure felt, 2 point discrimination
decreaseddecreased– Healing takes 1-3 monthsHealing takes 1-3 months– Usually scars, may need graftingUsually scars, may need grafting

Third DegreeThird Degree
Full thickness of skin (epidermis, Full thickness of skin (epidermis, dermis and subcutaneous tissue)dermis and subcutaneous tissue)
Skin white or black, may be charredSkin white or black, may be charred No dermal elements remain, No dermal elements remain,
therefore will not heal independently therefore will not heal independently – require surgical intervention and – require surgical intervention and skin graftsskin grafts
Significant scarringSignificant scarring

Third Degree BurnThird Degree Burn

Third Degree BurnThird Degree Burn

Fourth DegreeFourth Degree
Extends through skin and Extends through skin and subcutaneous tissue to involve subcutaneous tissue to involve muscle, bones, tendons or deeper muscle, bones, tendons or deeper tissuestissues
Requires extensive surgical repairRequires extensive surgical repair May necessitate amputationMay necessitate amputation

Fourth Degree BurnFourth Degree Burn

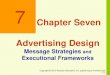
Burn Depth… ComparisonBurn Depth… ComparisonTable 43-5. Characteristics of burns of different depth.
Depth of Burn Appearance Skin Texture Capillary Refill
Sensation Healing
First-degree Superficial epidermis Red Normal Yes Yes 5-10 days; no scar
Second-degree Superficial partial-thickness
Red; may be blistered
Edematous Yes Yes 10-21 days; no or minimal scar
Deep partial-thickness Pink to white Thick Possibly Possibly 25-60 days; dense scar
Third-degree Full-thickness White, black, or brown
Leathery No No No spontaneous healing
Fourth-degree Involves underlying subcutaneous tissue, tendon, or bone
Variable Variable No No No spontaneous healing

TBSA???TBSA???
Total Body Surface AreaTotal Body Surface Area Only applies to area with second and Only applies to area with second and
third degree burnsthird degree burns
““Rule of Nines”Rule of Nines” May use palm of patient’s hand to May use palm of patient’s hand to
signify 1% TBSAsignify 1% TBSA

Rule of Nines…Rule of Nines…

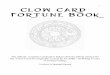
Rule of NinesRule of NinesTable 43-4. Rule of nines (rapid means of estimating body surface area burned in adult patients) and rule of lives (rapid means of estimating body surface area burned in infants and children.)
Percentage
Area Adult Infant Child
Head and neck 9 20 15
Arm
Right 9 10 10
Left 9 10 10
Torso
Front 18 20 20
Back 18 20 20
Leg
Right 18 10 15
Left 18 10 15
Genitalia and perineum 1 . . . . . .
Total 100 100 = 100

Adults vs. ChildrenAdults vs. Children

Inhalational Injury??Inhalational Injury??
Signs of Inhalational InjurySigns of Inhalational Injury– Singed nasal hairs, soot around naresSinged nasal hairs, soot around nares– Carbonaceous sputum, coughCarbonaceous sputum, cough– Hoarse voice, stridor, respiratory distressHoarse voice, stridor, respiratory distress– Carboxyhemoglobin > 10%Carboxyhemoglobin > 10%
Risk FactorsRisk Factors– Burns sustained in a confined spaceBurns sustained in a confined space– Flash burns, burns to faceFlash burns, burns to face

Inhalational Injury…Inhalational Injury…
MechanismMechanism– Injury occurs due to heat exposure, Injury occurs due to heat exposure,
chemical inhalation, particulate matterchemical inhalation, particulate matter InjuryInjury
– Upper airway edemaUpper airway edema– BronchospasmBronchospasm– Pulmonary edemaPulmonary edema

TestsTests
ECGECG CXR, other imaging as indicatedCXR, other imaging as indicated CBC, electrolyes, glucose, renal fcnCBC, electrolyes, glucose, renal fcn ABG, carboxyhemoglobinABG, carboxyhemoglobin
?tetanus status?tetanus status

Management…Management…

Minor Burns…Minor Burns…

TreatmentTreatment
Includes all 1Includes all 1stst degree, and many degree, and many superficial 2superficial 2ndnd degree burns degree burns
Can usually be managed as outpatientsCan usually be managed as outpatients May or may not require specialized May or may not require specialized
follow-up, or GP carefollow-up, or GP care Many patients need significant Many patients need significant
reassurancereassurance Ensure patients have a safe place to stayEnsure patients have a safe place to stay

TreatmentTreatment
CoolingCooling Cleaning – mild antiseptic solution, or Cleaning – mild antiseptic solution, or
soap and water; limit rubbingsoap and water; limit rubbing Debride blisters if large, or over Debride blisters if large, or over
jointsjoints Topical antibioticsTopical antibiotics Sterile dressingsSterile dressings AnalgesiaAnalgesia

Major Burns…Major Burns…

ABC’s!!!ABC’s!!!
AirwayAirway– Intubate if any signs of airway injury, if Intubate if any signs of airway injury, if
significant TBSA burns, if altered LOCsignificant TBSA burns, if altered LOC BreathingBreathing
– 100% O2100% O2– Monitor SpO2, respiratory rate, WOBMonitor SpO2, respiratory rate, WOB– Intubate Early!!!Intubate Early!!!

ABC’s cont’dABC’s cont’d
Circulation…Circulation…– 2 large bore IVs2 large bore IVs– FLUIDS, FLUIDS, FLUIDS…FLUIDS, FLUIDS, FLUIDS…– Parkland FormulaParkland Formula
Disability, ExposureDisability, Exposure– Cut off all clothing; may need soaking Cut off all clothing; may need soaking
offoff– Evaluate other injuriesEvaluate other injuries

Parkland FormulaParkland Formula
Ringers lactateRingers lactate 4 ml/kg/%TBSA over 24 hours4 ml/kg/%TBSA over 24 hours
– Half in 1Half in 1stst 8 hours 8 hours– Half in next 16 hoursHalf in next 16 hours
Titrate to urine output, BP, HRTitrate to urine output, BP, HR May need 40+ liters of fluidMay need 40+ liters of fluid

Other ManagementOther Management
Foley catheterFoley catheter Nasogastric tubeNasogastric tube Tetanus prophylaxisTetanus prophylaxis Remove jewelryRemove jewelry AntibioticsAntibiotics Wound careWound care Control pain – narcotics, amnesticsControl pain – narcotics, amnestics

Special SituationsSpecial Situations
Circumferential BurnsCircumferential Burns– May need escharotomy, especially on May need escharotomy, especially on
neck, trunk, limbsneck, trunk, limbs Inhalational InjuryInhalational Injury
– Require intubation, 100% O2Require intubation, 100% O2– May need hyperbaric oxygenMay need hyperbaric oxygen
Ocular InjuryOcular Injury– Need urgent ophthalmologic evaluationNeed urgent ophthalmologic evaluation

Assessment of SeverityAssessment of Severity
Table 43-2. Determinants of burn severity.
Burn sizeBurn depthBurn sitePresence of circumferential burnsInhalation injuryElectrical injuryAge of patientAssociated injuriesMajor underlying medical problems

Assessment of Severity…Assessment of Severity…Table 43-3. Summary of American Burn Association burn severity categorization.
Major burn injurySecond-degree burn of > 25% body surface area in adultsSecond-degree burn of > 20% body surface area in childrenThird-degree burn of > 10% body surface areaMost burns involving hands, face, eyes, ears, feet, or perineumMost patients with the following:Inhalation injuryElectrical injuryBurn injury complicated by other major traumaPoor-risk patients with burns
Moderate uncomplicated burn injurySecond-degree burn of 15-25% body surface area in adultsSecond-degree burn of 10-20% body surface area in childrenThird-degree burn of < 10% body surface area
Minor burn injurySecond-degree burn of < 15% body surface area in adultsSecond-degree burn of < 10% body surface area in childrenThird-degree burn of < 2% body surface area

Transfer to Burn Center?Transfer to Burn Center?
All “Major” BurnsAll “Major” Burns Any burn patients with associated Any burn patients with associated
major traumamajor trauma Suspected child abuseSuspected child abuse Anyone requiring surgical Anyone requiring surgical
interventionsinterventions

Back to the case…Back to the case…
22ndnd and 3 and 3rdrd degree burns degree burns– Chest and abdomen, full backChest and abdomen, full back– Both arms, handsBoth arms, hands– Anterior legsAnterior legs– Half of faceHalf of face
??TBSA??TBSA

Rule of Nines…Rule of Nines…

Back to the case…Back to the case…
VitalsVitals– BP 170/100BP 170/100– HR 130HR 130– SpO2 – cannot obtain due to burned SpO2 – cannot obtain due to burned
fingersfingers– RR 30RR 30– Temp 36 orallyTemp 36 orally

Back to the case…Back to the case…
Singed nasal hairsSinged nasal hairs Soot in mouthSoot in mouth CoughingCoughing Talking normallyTalking normally Complains of severe pain over entire Complains of severe pain over entire
bodybody

Back to the case…Back to the case…
Now what??????Now what??????
Sedate and intubateSedate and intubate Keep sedatedKeep sedated Foley, NGFoley, NG BIG IVsBIG IVs How much fluid???How much fluid???

Back to the case…Back to the case…
Parkland formulaParkland formula– Approximately 70% TBSAApproximately 70% TBSA– Patient weighs 80 kgPatient weighs 80 kg
– 4 ml/kg/%TBSA = 4 x 80 x 70 = 22400 4 ml/kg/%TBSA = 4 x 80 x 70 = 22400 mlml
– i.e. more than 22 liters of fluid… 11 over i.e. more than 22 liters of fluid… 11 over first 8 hours, then 11 over next 16…first 8 hours, then 11 over next 16…
– Titrate to urine output and vitalsTitrate to urine output and vitals

Back to the case…Back to the case…
Circumferential burns to chest, arms, Circumferential burns to chest, arms, fingersfingers– Requires escharotomy to ensure chest is Requires escharotomy to ensure chest is
able to expand, and to limit chances of able to expand, and to limit chances of losing fingers!losing fingers!
Needs a burn center!!!Needs a burn center!!!

EscharotomyEscharotomy

Severe Burn CaseSevere Burn Case