Embed Size (px)
Citation preview

Dr. Robert Riehle Jr.
Wofford College 2/24/10

Wofford Healthcare SymposiumOur current system and its need to
change
Financing of the delivery system
Components of an ideal delivery system
What change is possible

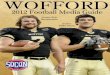
Healthcare Reform- Is now the time?
58%54% 54%
39%41%
36%
41%39%
53% 55%57%56%59% 61%62% 62%61%
42%39%
35%37%37%34% 34%
0%
20%
40%
60%
80%
Oct08 Dec08 Feb09 Apr09 Jun09 Jul09 Aug09 Sep09 Oct09 Nov09 Dec09 Jan10
It is more importantthan ever to take onhealth care reform now
We cannot afford totake on health carereform right now

Healthcare Comments Healthcare system is broken.
We don’t want a government run healthcare system.
I want to choose my doctor!
We don’t put enough resources into prevention
Insurance companies are villains. They get between me and my doctor.
80% of Medicare costs are in the last 6 months of life.
I’m satisfied with the quality of care. It just costs too much.
We have a sickness, not a wellness system.

Issues and Challenges 2010Wants:
1. Excellent care (acute and chronic)
2. Availability – access (convenient, timely)
3. Insurance coverage
4. Affordable
Complaints:
1. Cost of care and coverage
2. Uninsured and underinsured
3. Inefficiencies of process – care delivery

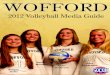
Distribution of National Health Expenditures, by Type of Service, 2008
Note: Other Personal Health Care includes, for example, dental and other professional health services, durable medical equipment, etc. Other Health Spending includes, for example, administration and net cost of private health insurance, public health activity, research, and structures and equipment, etc.
Source: Kaiser Family Foundation calculations using NHE data from Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group, at http://www.cms.hhs.gov/NationalHealthExpendData/ (see Historical; National Health Expenditures by type of service and source of funds, CY 1960-2008; file nhe2008.zip).
Physician/
Clinical
Services
21.2%
Hospital Care
30.7%Other Personal
Health Care
12.9%
Nursing Home
Care, 5.9%
Prescription
Drugs
10.0%
Home Health
Care, 2.8%
Other Health
Spending
16.5%

Healthcare ArenaDelivery SystemsHealthcare provider, facility, vendor = delivery system
Hospitals and Medical Centers FP, NFP
Faith based
Municipal
Governmental
Integrated Healthcare Systems Hospitals
Physicians (office based)
Rehab, ASC, Primary Care Centers, Diagnostic Centers, Home Health, Hospice
Levels of care (continuum)

Healthcare Arena: Reform Plan- insurance coverage
Insurance-employer, group, individual
Finance
Delivery system- IDS, providers
Information
Regulation
Certification, Accreditation
Government role: financed, managed, regulated, sponsored, coordinated, run, owned
Comprehensive Reform- Change all components

Health Versus Healthcare Health: shaped by genetics, lifestyle, diet, social
factors, chance , and sometimes healthcare
Healthcare: Episodic vs. longitudinal
• Restores health vs. promotes health
• Basic vs. specialty
• Preventive vs. reactive

Ideal Delivery System ConceptsHigh quality; effective care and service
Standardized, measurable, improving
Accessible (acute and chronic)
Efficient- cost controlled, technology, innovative
Universal for all; basic, prevention
Managed across continuum (levels of care)
Accountable, monitored

Ideal Delivery System Components Integrated Delivery Systems (IDS)
Engaged physicians
Evidence based medicine
Information sharing via EMR, telemedicine, RHIN
Consolidation versus competition
Transparency of operations (cost, quality, continuum)
Primary care focus
Chronic disease focus
End of life: planned
Tort Reform

Integrated Delivery System Organized, managed, owned across the continuum
Employed staff, new role for extenders
Accountable care organizations
Efficient
Measurable by metrics
Incentives
Vendor bidding
Pay for performance
Prevention pays
Clinical effectiveness research rules –evidence based medicine
Hub and spoke- rural + tertiary

Engaged PhysiciansEmployed and managed
Accountable by metrics
Use of extenders-patient centered team
Incentive based on productivity, process and outcomes… performance based pay
Evolution of manpower: training, financing, continued learning, certification, patient/physician relationship

Are doctors following the guidelines?
Retrospective review, cancer care delivered
1300 oncologists
Non-compliance with NCCN guidelines:17%,61%, 31%, 24%, 31%
Optimal compliance (NCCN) 85%!
Clinical variation?
United Healthcare 2010

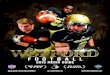
Non-Federal Physicians per 100,000 Civilian Population, 1970-2008
146165
193
220234
262 266 268 273 277 280
312 316 319 322
0
50
100
150
200
250
300
350
1970 1975 1980 1985 1990 1995 2000 2001 2002 2003 2004 2005 2006 2007 2008

Evidence Based Medicine
National guidelines
Algorithms
Risk predicting software
CER (Clinical Effectiveness Research)
Patient education= interactive

Information Sharing-Informatics EMR (EHR, multimedia, patient health records,
interactive)
Telemedicine Teleradiology, pathology
Teleconsultation
Telesurgery
Telerounding
Tele-ICU (e-ICU)
RHIN (regional health info network)
Important for rural, community and public health

Consolidation versus CompetitionMergers at regional/national levels
Devolution of For Profit Hospitals
Certification of Centers of Excellence
More IDS, hub and spoke, geographic mergers
Physician multi-specialty groups, employed networks
More regional/ national networks

Medical Liability: Tort Reform Relocate from tort system to alternative, administrative
Civil court replaced by health court
Less adversarial, more efficient form of justice
No fault concepts
Administrative medical injury compensation
Poor result versus malpractice (negligence)
Current examples: no-fault, government administered National Vaccine Injury Compensation Program
NLRB, Tax, worker’s compensation board
State initiatives: birth injury funds
Risk management
Consent to independent structured arbitration process
www.commongood.org

Transparency of OperationsPerformance metrics (clinical and services)
Pricing/changes – how much will it cost me?
Report card: value, quality of care
Regulation- certification, accreditation
Conflict of interests- ownership, research, industry “expert”

Primary Care Focus Patient centered: new model
Group visits
Medical home, PCP coordination
Electronic visits
Alternative Hours, case managers
Multidisciplinary, coordinated visits
Prevention via EMR
Patient education; responsibility
Specialist advice without visit – video and audio

Chronic Disease Focus Increasing prevalence (emphysema, heart failure,
arthritis, cancer, multiple sclerosis)
Standardized around guidelines
Drugs to slow progression
Extenders as providers; medical home
Acute on chronic: efficient management “back to baseline”
Transition to symptom management (palliative)

End of Life- Planned Advanced directives: What I want done if I can’t decide
myself
Family involvement
Quality of life – metrics
Individualized decision/autonomy/patient rights
PCP/ geriatrics
What can we do vs. what you want done…

Ideal Delivery System Components Integrated Delivery Systems (IDS)
Engaged physicians
Evidence based medicine
Information sharing via EMR, telemedicine, +RHIN
Consolidation versus competition
Transparency of operations (cost, quality, continuum)
Primary care focus
Chronic disease focus
End of life: planned
Tort Reform

Healthcare System Reform: Summary
Less segmented, more integrated
Less independent, more monitored
More standardized, effective, efficient
More electronic, interactive , coordinated
More transparent
More socially responsive
More personal responsibility
Less liability for poor outcomes

WebsitesHospital Patient Info
www. Hospitalcompare.org
www.myschospital.org
www.ncqualitycenter.org
www.abouthealthquality.org
Physician
www.healthgrades.com($12.95)
www.NCQA.org
recognition program
www.JAMA.com Patient page
www.myhealthcareoptions.org
Facility
www.medicare.gov/dialysiscompare/SNF compare

Healthcare Reform : tenets Reduce # of uninsured
Reduce cost of care , premiums
Reduce clinical care variance re practice
Reduce encounter based payments
Reduce administrative costs
Reduce role of government

White House : Healthcare Reform Proposal 2/22/10
Medicaid Expansion – fully funded by Washington
-eligibility 133% of FPL
Tax high cost healthplans (2018)
Medicaire payroll tax – increase .9% on earnings
Medical Device tax (2013)

WH HC Reform 2/22/10 Individual Mandate (2014)
Employer mandate ( ??)
Insurance companies: assessments
Insurers – no exclusions (2014)
Insurers – premium increases – Fed Rate Auth Review
Pharma - assessment

WH HC Reform 2/22/2019 Assume Close to universal coverage
Commission to manage Medicaire (not congress)
CER – clinical effectiveness research
More community health centers (CHC)
Decreased funding to hospitals
Technology Assessment (clinical)
Different payment methodology
Incentive to use EMR