Dr. Rebecca Ewing, OB/GYN Joyce Jorgenson, NOFAS NH
Slide 2
Define Fetal Alcohol Spectrum Disorders Recognize physical,
neuro-developmental and functional outcomes associated with
prenatal alcohol exposure Discuss recent research interventions for
children with FASDs Address intervention approaches to prevent or
lesson fetal alcohol exposure
Slide 3
Fetal Alcohol Spectrum Disorders is an umbrella term describing
the range of effects that can occur in an individual whose mother
drank during pregnancy. These effects may include physical, mental,
behavioral, and /or learning disabilities with possible lifelong
implications. The term FASD is not intended for use as a clinical
diagnosis. CDC July 2004
Slide 4
Estimated Prevalence Data.2011 8-31 Babies born with FAS 23-92
Babies born with FASD Public Health Block Grant Application 2011
Estimated Cost Data Lifetime Cost of Care per Individual NIAAA 2
million SAMHSA 3 million
Growth Restriction: Babies are born smaller than anticipated
for the gestational age at birth, and usually remain so throughout
life. Central Nervous System: Any or all of the following
conditions may be present intellectual disabilities, developmental
delays, short attention span, impulsivity, perceptual problems,
hyperactivity, poor coordination & learning disabilities.
Facial Anomalies: Babies have the following distinctive facial
features-- small widely spaced eyes; a short, upturned nose; a
smooth philtrum (no notch between the nose and lips); abnormally
thin upper lip; and small flat cheeks. (CDC, 2005)
Slide 9
( Reprinted with permission, Streissguth A.P., & Little,
R.E. 1994)
Slide 10
First trimester Cell damage Brain damage Substantial structural
changes Second trimester Poor nutrition can retard the growth of
tissue and organs Risk of miscarriage Third trimester Lower birth
weight/overall amount of growth Increase likelihood of early labor
and delivery Intellectual Disability ( March of Dimes, 2000)
Slide 11
Slide 12
Alcohol passes freely from the mother to the fetus The fetal
liver cannot metabolize alcohol efficiently Blood alcohol levels
are equivalent between the woman and fetus by 1 hr. (Cohen-Kareem,
2002) Alcohol levels in amniotic fluid are lower but persist for
longer (Burd, L. 2007)
Slide 13
Slide 14
Slide 15
The best predictor of adolescent alcohol abuse is prior fetal
exposure or mothers who drank alcohol during pregnancy, Animals
learn to like the smell of what their mothers eat during pregnancy.
It could be alcohol odor, or it could be the odor of apple. Dr.
Youngentob.
Slide 16
No consequences Cravings for alcohol as an adolescent and adult
FASD Neurobehavioral Development Abnormalities FAS Structural and
Functional Abnormalities Genetic changes impact on future
generations Demise
Slide 17
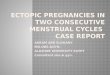
Photo courtesy of Sterling Clarren, MD Brain of baby with no
alcohol exposure Brain of baby with heavy alcohol exposure
Slide 18
Of all the substances of abuse (including cocaine, heroin and
marijuana), alcohol produces by far the most serious
neurobehavioral effects in the fetus. Institute of Medicine,
1996
Slide 19
Slide 20
Cognition/Intellectual Functioning Activity and Attention
Hyperactivity Focusing, encoding, shifting Learning and Memory
Auditory, spatial, design, and narrative memory Working memory
Intrusion, perseveration, false-positive errors Comprehension, math
reasoning
Slide 21
Slide 22
Last serny, Fingledobe and Pribin were in the nerd-link
trepping gloopy caples and cleaming burly greps. Suddenly, a ditty
strezzle boofed into Fingledobes tresk. Pribin glaped and glaped.
Oh, Fingledobe! He chifed. That ditty strezzle is tuning in your
grep!
Slide 23
Other Neuropsychological Abilities/Executive Functioning
Behavioral and emotional regulation-impulsivity, lability
Planning/organization Sensorimotor Integration Social Skills and
Adaptive behavior Mental Health Issues
Language Social communication Word comprehension, naming
ability, articulation Expressive and receptive language skills
Motor Abilities Fine and gross motor dysfunction Delayed motor
development Speed/precision, grip strength Processing Abilities
Spatial memory, processing of visual and auditory information
Difficulties in motor control and functioning
Slide 27
Slide 28
PinkBlackRed BlackYellowBlue Red YellowBlackYellow
RedGreenBlack Yellow Orange Quickly read the words
Slide 29
PinkBlackRed BlackYellowBlue Red YellowBlackYellow
RedGreenBlack Yellow Orange Quickly state the colors
Slide 30
Many individuals with FASD are: Caring, kind, loyal, nurturing
and compassionate Trusting, loving, determined, committed and
persistent Curious, involved, fair and cooperative Energetic, hard
working and athletic Artistic, musical and creatively
intelligent
Slide 31
Early diagnosis Stable and nurturing home environment Early
intervention services No violence/victimization DDD services
Streissguth,2004
Slide 32
Poor sleep-wake cycles/irritability Failure to thrive (poor
weight gain) Chronic ear infections Difficulty nursing Difficulty
bonding with caregiver Developmental Delays Speech delays; low
muscle tone
Slide 33
Delay in potty training Speech delays or difficulties Continued
motor skill delays Easily distracted Colds, infections, other
illness Eating (small appetites or sensitivity to food texture)
Fidgeting (meal time or other structured event) Sleep problems
Slide 34
Delayed speech development Altered motor skills Attention
deficits Learning deficits Caregiver concerns
Slide 35
Bedtime problems Making and keeping friends Difficulties
determining body language and expressions Boundary issues Attention
problems and impulsivity Easily frustrated/tantrums Difficulty
understanding cause and effect
Slide 36
Still need limits and protection due to deficits in reasoning,
judgment and memory High risk of being drawn into antisocial
behavior, eg. stealing, lying, drugs: thrill seekers Unable to
distinguish between friends/enemies; impaired judgment for
decisions Struggle to accept their own disability while trying to
prove ability to be independent Often obsessed by primal impulses
such as sex and firesetting Lacks remorse Negligent of normal
hygiene Extremely vulnerable to suggestions in movies, TV High risk
for school dropout Unable/unwilling to take responsibility for
actions
Slide 37
Moral chameleons Often exhausted and irritable due to poor
sleep patterns Vulnerable to anti-social behavior. The criminal
justice system provides structure and supervision they experienced
in school or in their home Unable to follow safety rules: fire
hazards, vehicles, basic life needs May lack ability to manage
money Incapable of taking daily medications Vulnerable to panic,
depression, suicide, psychosis May need sheltered environment
Slide 38
Professionals, family members, and caretakers need to
reconceptualize how we view the behavior of a individual with
FAS/FASD From seeing: To understanding: WontCant LazyTries hard
LiesFills in Doesnt tryExhausted or cant start Doesnt careCant show
feelings Refuses to sit stillOver stimulated Fussy,
demandingOversensitive ResistingDoesnt get it
Slide 39
One prevention model contains seven basic components, form the
acronym SCREAMS Structure: a regular routine with simple rules and
concrete, one step instruction, paired with examples Cues: verbal,
visual, or symbolic reminders can counter the memory deficits Role
models: family, friends, TV shows, movies that show healthy
behavior and life styles Environment: minimized chaos, low sensory
stimulation, modified to meet individual needs. Attitude:
understanding that behavior problems are primarily due to brain
dysfunction Medications: most often the right combination of meds
can increase control over behavior Supervision: 24/7 monitoring may
be needed for life due to poor judgment, impulse control.
Slide 40
CDC provided funding to develop, implement, and evaluate
interventions appropriate for children with fetal alcohol spectrum
disorders (FASDs) and their families. Each intervention was
designed to improve the developmental outcomes of individuals with
FASDs, reduce secondary conditions, and improve the lives of
families affected by FASDs.
Slide 41
Think: Stretched Toddler. Remember: Individuals with FASD will
always need an external brain. Acknowledge: Interventions must be
useful to, and usable by the individual in order to be an
intervention. Foster: Inter-dependence. Reflect: Respect. Promote:
Self-worth.
Slide 42
Concentrate on their strengths and talents Teach memory
strategies for daily living skills Accept individuals limitation Be
consistent with everything (discipline, school, behaviors) Use
positive reinforcement often (praise, incentives) REPEAT, REPEAT
Honor their feelings
Slide 43
Team approach Multi-discipline assessment Psychosocial history
Physician Disciplines (Mental health, speech, OT/PT, LD)
Parents/caregivers Social service agencies (DDD, SS, Child
protective, drug treatment centers) Case management Diagnosis Early
intervention and tracking Stable home environment Medication Case
manager/mentor in school/home/communities Support services-family
community, educational, vocational Supervised housing/residential
facility Special education and vocational rehabilitation
Slide 44
Drinking alcohol during pregnancy is the leading preventable
cause of birth defects and developmental disabilities in children,
says the Centers for Disease Control and Prevention. But That's not
stopping pregnant women from drinking. RYAN JASLOW / CBS NEWS/ July
19, 2012, 5:24 PM1 in 13 pregnant women drink alcohol, Institute of
Medicine, 1996
Slide 45
Women Age 18 -44 who were not pregnant and do not have children
living in the household 63% Women in first trimester of pregnancy
19.0% Women in second trimester of pregnancy 7.8% Women in third
trimester of pregnancy 6.2%
Slide 46
.no known safe amount of alcohol to drink while pregnant. There
is also no safe time during pregnancy to drink and no safe kind of
alcohol. CDC urges pregnant women not to drink alcohol any time
during pregnancy. CDC There is no known amount of alcohol that is
safe to drink while pregnant. There is also no safe time to drink
during pregnancy and no safe kind of alcohol to drink while
pregnant. SAMHSA No safe level of alcohol consumption during
pregnancy has been identified, and no period during pregnancy
appears to be safe for alcohol consumption. ACOG TOOLKIT
Slide 47
INTERVENTION POINT: PRE-PREGNANCY Policies and practices that
address the substance exposed infant (SEI) problem Health warnings;
Provision of educational materials; Public education and awareness
media campaigns.
Slide 48
INTERVENTION POINT: PRENATAL PERIOD AND BIRTH It proceeds
through the prenatal period and birth, when the interventions
include screening of pregnant women for substance use testing of
infants for substance exposure.
Slide 49
Screening Identification of risk Brief intervention Referral to
treatment Treatment provided to identified patient
Slide 50
Robust prevalence study Universal survey screening A dedicated
FAS/FASD diagnostic and treatment center A clear message to the
public