Embed Size (px)
Citation preview


“Il carcinoma della mammella nel 2010: Il Chirurgo Generale tra demolizione,
ricostruzione e radioterapia”
Partial Breast Irradiation
TARGITIl punto di vista
del radioterapistaUdine, 23 ottobre 2010

CENTRO DI RIFERIMENTO ONCOLOGICOISTITUTO NAZIONALE TUMORI – AVIANO
SOC Oncologia Radioterapica
Dr. M. Roncadin

Target for Breast Cancer in the 2000s
Less aggressive treatment
to obtain a better quality of life
and fewer side effects

Previous traditional approach:“Maximum tolerated dose”
Current approach: “Minimum effective treatment”

Breast CancerAt diagnosis Year Year
1970 2000
- T1 17% 65%
- Not palpable 1% 31%

Local treatment of breast cancer
Have the principles really changed?
Halsted’s Radical Mastectomy
Limited Surgery plus Radical Radiotherapy

Randomized Trials comparing Surgery Alone vs Surgery Plus RT
Impact of Radiation% pts with % reductionrecurrence recurrence
Trial CS CS+RT CS vs CS+RT
NSABP B-06* 36 12 67Ontario 35 11 69Milan 24 6 75Scottish 25 6 76English 35 13 63Uppsala-Orebro 24 9 63
*Recently updatedVicini/Harris, ASTRO 2002

Mesi
Cumulative hazard
0 12 24 36 48 60 72 84 96 108 120
0.0
0.1
0.2
0.3
0.4
0.5
Quadrantectomia
Quadrantectomia + RT
Recidiva Locale

Are there any problems with current approach?
RT typically takes 6 weeks to deliverPatients don’t like these 30 daily visitsGeography prevents many women from
receiving conservative breast surgery
Breast cancer = 1/3rd of RT work-loadLong waiting-lists in many Centres

Newer/Alternative Treatment Approaches
Efforts to reduce treatment time of RT after breast conserving surgery:are more rapid fractionation
schedules using increased daily fraction sizes “acceptable”?
Vicini/Harris ASTRO 2002

Newer/Alternative Treatment Approaches
Treat only the index quadrant of the breast

The RationaleWhole organ analysis ofmastectomy specimens*
3-D analysis• 63% harbouroccult cancer
• 80% of theseare in otherquadrants

The RationaleIn trials of conservative surgery: >90% recurrences occur in the index
quadrant whether radiotherapy is given or not
Radiation to the index quadrant alone might be sufficient

Site of Local Recurrence after BCT
Author N. %in index q.
Clark RM, 1982 680 96%Schnidt SJ, 1984 231 83%Boyages J, 1990 783 81%Kurtz JM, 1990 1593 86%Fisher B, 1992 1843 100%Veronesi U, 1993 570 90%TOTAL 5770 91%

The Christie Hospital TrialGG Ribeiro, B Magee, R Swindell, M Harris and SS Banerjee Clin Oncol (R Coll Radiol) 1993; 5: 278-283
708 patients randomised
a) Limited Field (LF):4 Gy (10 days) 8x6 cm area10 MeV to a depth of 2.5 cm
b) Wide Field (WF):4 Gy (21 days) whole breast,axilla & scf

The Christie Hospital Trial8 year Results
Breast Recurrence: LF WFDuct Carcinoma (n=534) 15% 11%
IEC (>25% invasive) (n=45) 21% 14%Lobular Carcinoma (n=95) 34% 8%

Partial Breast Irradiation (PBI)
MetodologiaRiduzione del volume trattato, usando alte dosi equivalenti e risparmiando il tessuto normale
“Irradiazione della sede di
escissione e del solo del tessuto
adiacente”Workshop on PBI, J Natl Cancer Inst, 2004

Da Radioterapia esterna frazionata a
Radioterapia Intraoperatoria - dose esclusiva

Partial Breast Irradiation (PBI)
TechniquesInterstitial brachytherapyMammoSiteAccelerated three-dimensional
conformal radiotherapy
EliotTargit
Accelerated PBI
IORT
Accelerated Partial Breast Irradiation- Definition -
Delivery of large dose/fraction of RT to the lumpectomy cavity (plus 1-2 cm margin) after breast conserving surgery using brachytherapy or external beam RT techniques
Complete RT in <4-5 days after lumpectomy instead of 6-7 weeks
Vicini/Harris ASTRO 2002

Rationale for Accelerated Partial Breast Irradiation
Improve documented under-utilization of Breast Conserving Therapy (BCT)
time, cost and inconvenience of BCTPotentially reduce acute and chronic toxicityImprove quality of life of patientsEliminate scheduling problems with systemic
CTPotentially improve outcome? (Reduce delays
to local therapy)Vicini/Harris ASTRO 2002

Risk of local recurrenceaccording to the waiting time for radiotherapy.1.1% increase of absolute risk per month of delay
No decrease in survival
(Chen Z et al, Radiat Oncol 2008)

Partial Breast Irradiation (PBI)
TechniquesInterstitial brachytherapyMammoSiteAccelerated three-dimensional
conformal radiotherapy
EliotTargit
Accelerated PBI
IORT

TARGIT
TARGeted IntraoperativeRadioTherapy

Device: mobile, flexible, extremely reliable platform for any operating room

Miniature X-ray source of Low Energy (max) 50 KV.



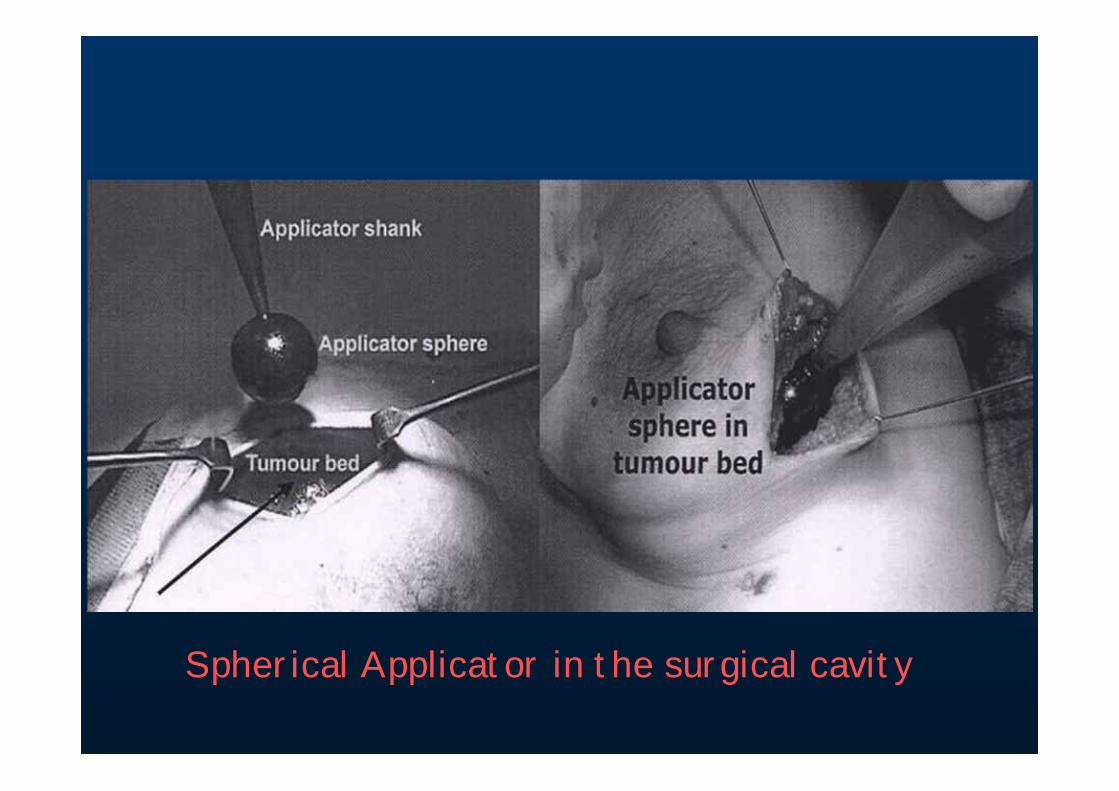
Spherical Applicator in the surgical cavity

Rather than the complicatedconformation of the source
to the target...
The target - the pliablebreast tissue -
is conformed to the source

Spherical Applicators Set (ranging from 1.5 – 5 cm in Ø)to fit different sizes of surgical cavities

Disposable plastic “bag” to ensure sterility

IORT with TARGIT System for PBI
Pilot Study Targit – A Targit – B Translational Research Project

Pilot Study Patients undergoing breast-
conserving surgery were offered boost radiotherapy with targeted intra-operative radiotherapy (TARGIT) using the IntraBeam system(*) to test the feasibility, safety and efficacy of the new approach.
(*) as a substitute for conventional external beam RT boost

Radiation therapy with TARGIT System in
early stage breast cancer
Results at 6 years of follow-up
Pilot Study

PBI Intrabeam System
Period: September 2002 December 2004
N° evaluable pts: 112
Median age : 53 years (range 28-76)

Inclusion CriteriaIn the pilot study, we have no special requirements for inclusion criteria (except for unifocal, invasive, and
<5cm in Ø tumor) because our priority was to test the feasibility of the
treatment, in other words, our focus was on safety and efficacy.

Pathology Tumor size: 1.3 cm in Ø (range 0,6-3,8)
Histology: • Ductal invasive 90 (80%)
• Lobular 5 (4,5%)
• Other 17 (15,5%)
DCIS 70 (62,5%)
Lymphovascular invasion: 47 (42%)

Pathology
Status of surgical margins
Neg. 105 (94%)Ductal invasive ca 2
Pos.(microscopic)
7 (6%)DCIS 3
Lymphovascular invasion 2

Status of estrogen receptor Positive 93 (83%) Negative 19 (17%)
Grading: G1 9 (8%) G2 59 (53%) G3 44 (39%)

Sentinel node (S.N.): 112
Positive S.N.: 48 (43%)
Pathology

Adjuvant TherapySystemic treatment: - No 7 (6%)
- CT 26 (23%)- OT 40 (36%)- CT + OT 44 (39%)
External Radiation Therapy: 111 (*)(50Gy/25 fr./ 5 wks / 2 tang. fields – 6MV Linac)
PBI Spherical applicator: 4 cm (range 3,0-5,0)
*1 pt refused ext. RT

Results (1)
Median F-up: 6 yearsN. Evaluable pts 112Recurrence 2 (1,6%) (at 38 e 68 mos)
Metastases– No 110– Yes 2 (liver; lung-brain)

Results (2)
Toxicity:
• Acute (infections, edema, delayed scar healing, ulcer, skin necrosis): 0
• Chronic (fibrosis, skin retraction/atrophy, teleangectasia):
–Grade 3 (RTOG): 4
–Grade 4 (RTOG): 0


We treated 302 cancers (112 from the Aviano Center)
This was not a low-risk group.The treatment was well tolerated.

164 and 90 patients completed 2 and 3 year follow-up respectively.
The Kaplan-Meier estimated local recurrence is 2.6% at 5 years.
This compares favorably with the 4.3% recurrence rate in boosted patients from the EORTC boost study.

IORT with TARGIT System for PBI
Pilot Study Targit – A Targit – B Translational Research Project

Targit BoostTARGIT can be used as a tumor bed boost as a standard treatmentIt is already in the National Guidelines of many European Countries (e.g. Germany)
We believe that it could yield superior local control. Hence, the TARGIT-B trial

Targit – B (Boost)
International randomized controlled trial to compare targeted intra-operative radiotherapy boost with conventional external beam radiotherapy boost after BCS.

Targit-B: Inclusion CriteriaAt least one of these criteria must be satisfied:1. Less than 46 years of age
2. More than 45 years of age, but with 1 of the following poor prognostic factors:
a. More than minimum lymphovascular invasionb. Gross nodal involvement (not micrometastasis)c. More than 1 tumour in the breast but still suitable for breast conserving
surgery
3. More than 45 years of age, but with at least 2 of the following poor prognostic factors:
a. ER negative and HER-2 positiveb. Grade 3 histologyc. Positive margins at first excision
4. Those patients with large tumours which have responded to neo-adjuvant chemo- or hormone therapy in an attempt to shrink the tumour and are suitable for breast conserving surgery as a result.
5. Lobular carcinoma or Extensive Intraductal Component (EIC)
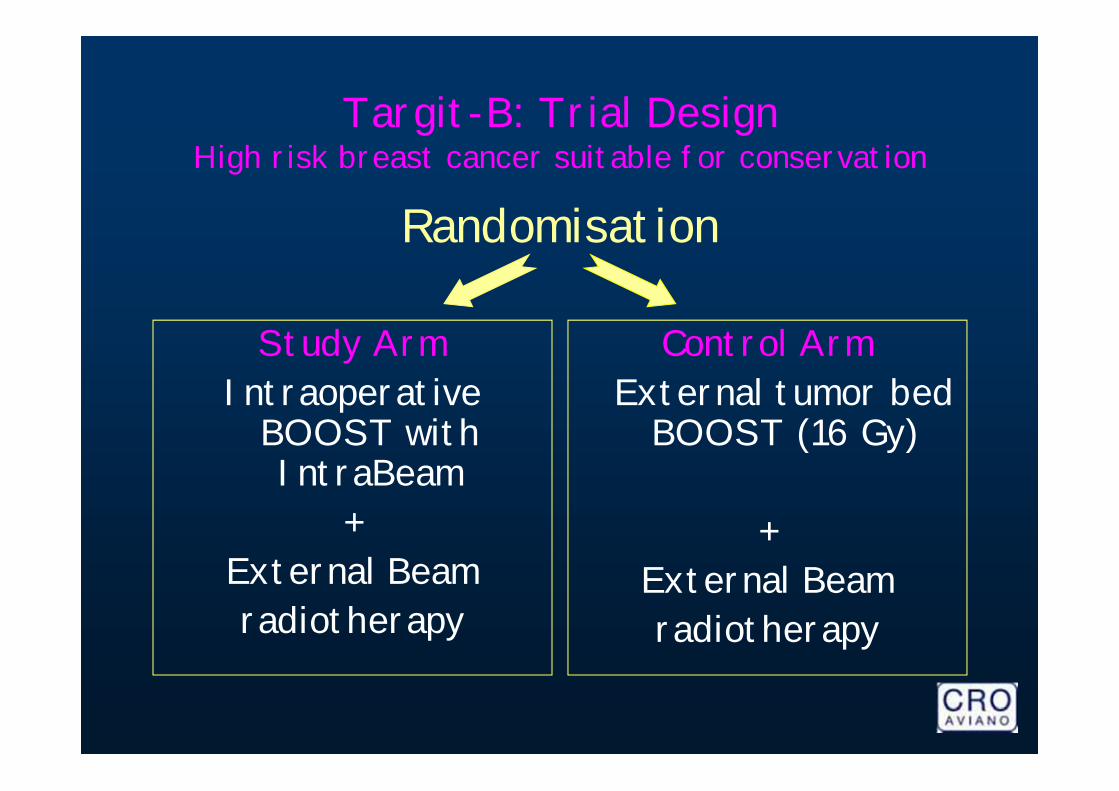
Targit-B: Trial DesignHigh risk breast cancer suitable for conservation
Study ArmIntraoperative
BOOST with IntraBeam
+ External Beamradiotherapy
Control ArmExternal tumor bed
BOOST (16 Gy)
+ External Beamradiotherapy
Randomisation

Targit – B (Boost)
To be activated: end of 2010
SUPERIORITY trial: TARGIT-B
Total accrual goal: 1900 patients
Central Trial Office: UCL (U.K.)

IORT with TARGIT System for PBI
Pilot Study Targit – A Targit – B Translational Research Project

Targit – A (Alone) Activated: November 2004
(International protocol: April 2000)
Age 45 years
Early breast cancer (max Ø 2.5 cm)
Unifocal
Total accrual goal: 2232 pts

TARGIT-ACriteri di eleggibilità
1. Età: 45 anni2. Diametro tumorale 2,5 cm3. Tumore unifocale4. Assenza di componente intraduttale
estesa (>25%)5. Istotipo diverso dal carcinoma lobulare6. Assenza di metastasi linfonodali all’esame
clinico-ecografico7. Assenza di linfangiosi neoplastica a
distanza dal tumore primitivo.8. Margini chirurgici in tessuto sano


Breast cancer - breast conserving therapyRandomisation
Study ArmWide local excision of
primary tumour + SNB/ axillary
dissection+
Targeted Intraoperative Radiotherapy
(if histopathology is Lobular or EIC, add 5wks of
postoperative radiotherapy)
Control ArmWide local excision of
primary tumour + SNB/ axillary
dissection+
6 wks of Postoperative Radiotherapy

TARGIT - A Trial accrualData current on 28 March 2010. 28 Centers
Accrual goal: 2232 patients
Centre Country Total
Perth Australia 227Aviano Italy 176London UCL UK 170Dundee UK 169Munich DRK Germany 146Copenhagen Denmark 134Mannheim Germany 122UCSF USA 76USC USA 56Munich LMU Germany 47Berlin Germany 35London RFH UK 24Frankfurt Germany 23Lublin Poland 23Homburg Germany 21Empoli Italy 18Winchester UK 16Zurich BZS Switzerland 9Melbourne Australia 8Virginia USA 6Indiana USA 4Toronto Canada 4Trondheim Norway 2
1516
238
2209
292
286
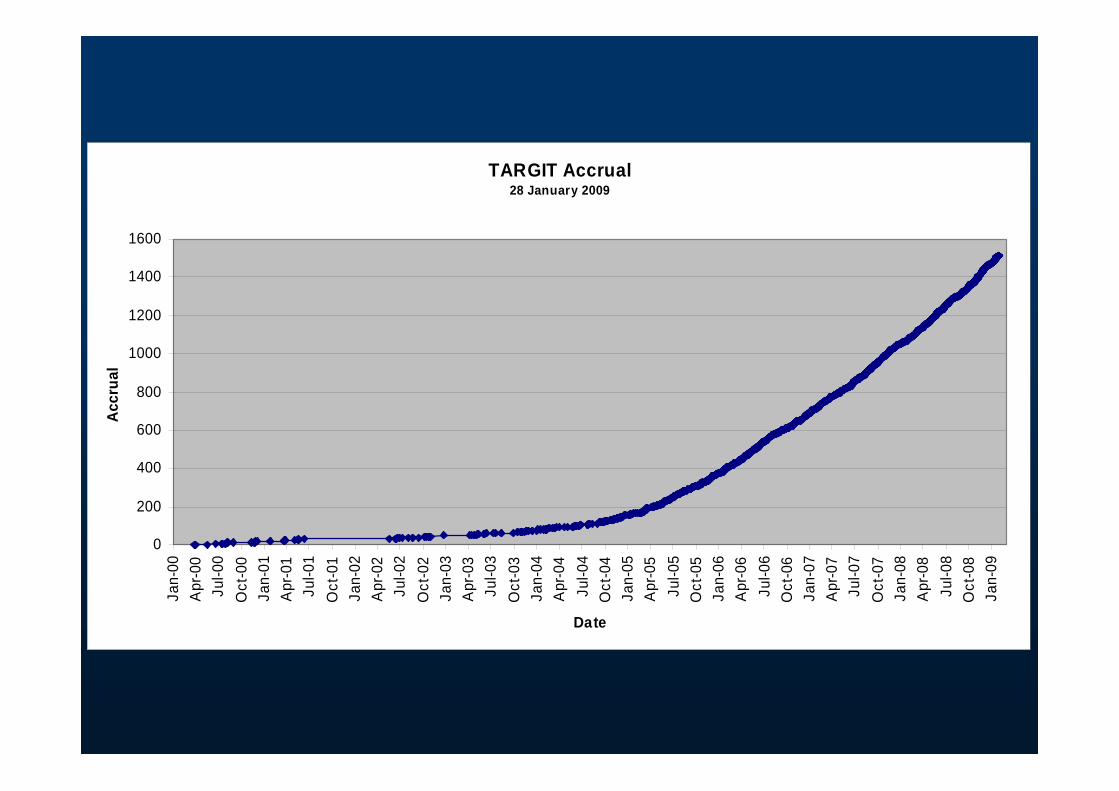
TARGIT Accrual28 January 2009
0
200
400
600
800
1000
1200
1400
1600
Jan-
00A
pr-0
0Ju
l-00
Oct
-00
Jan-
01A
pr-0
1Ju
l-01
Oct
-01
Jan-
02A
pr-0
2Ju
l-02
Oct
-02
Jan-
03A
pr-0
3Ju
l-03
Oct
-03
Jan-
04A
pr-0
4Ju
l-04
Oct
-04
Jan-
05A
pr-0
5Ju
l-05
Oct
-05
Jan-
06A
pr-0
6Ju
l-06
Oct
-06
Jan-
07A
pr-0
7Ju
l-07
Oct
-07
Jan-
08A
pr-0
8Ju
l-08
Oct
-08
Jan-
09
Date
Accr
ual

The Lancet

Partial Breast Irradiation (PBI)
Radioterapia Intraoperatoria:
il punto di vista del
Radioterapista

Trial RandomizzatiTRIAL N pz Controllo PBI
1 ELIOT IEO-MI2000-2007
1306 WBI 50 Gy+b 21 Gy/1 fr
2 GEC-ESTRO APBI TRIAL ‘04
1170 WBI 50 Gy+b 32.0 Gy/8 fr/1w30.3 Gy/7 fr/1w
3 NSABP Protocol B-39. RTOG Protocol 0413 ‘05 3000
WBI 50 Gy+b 34 Gy in 3.4 Gy MammoSite.® 34 Gy in 3.4 Gy M.C.-BRT3.85 Gy *10 fr 3Drt
4 RAPID (OCOG).‘06 2128 WBI 50 Gy+b 3.85 Gy *10 fr 3Drt
5 Irma (AIRO-IT)‘07 3302 WBI 50 Gy+b 3.85 Gy *10 fr 3Drt
6 TARGIT 2000University College London Hospitals
2232 WBI per center + boost
20 Gy*1fr (=5Gy(§) at 10 mm)
7 IMPORT LOW ‘06
2100 WBI 50 Gy/25 or 42.5/16fr +/- b
PB 40Gy/15 IMRTWB 40 Gy/15 IMRTWB 40 Gy/15 IMRT

Partial Breast Irradiation (PBI)
applicabile solo su casistica selezionata nell’ambito di studi controllati
le diverse metodiche di PBI non sono equivalenti
notevoli diversità del volume irradiato
Workshop Bethesda 8-10/12/2002 - J Natl Cancer Inst 2004, 96: 175-84

The cost of delivering Targit is about half that of a 6 week course of radiotherapyAssuming that 60% of patients
have conservative therapy, it could save £15,500,000 pa in the UKWorldwide, it could save thousands
of women from losing their breasts!
Conclusions on Partial Breast Irradiation Studies exploring Reductions in Overall
Treatment Time5-year results are very encouraging
Randomized trials will be useful in documenting long-term local control, survival and overall cosmetic results
Reproducibility and QA techniques will need to be adopted to ensure consistency in dose delivery
Vicini/Harris ASTRO 2002

IORT with TARGIT System for PBI
Pilot Study
Targit – A
Targit – B
Translational Research Project

IORTIntraOperative Radiation Therapy
IntraBeam nel Tumore della Mammella
Progetto di Ricerca Translazionale(Fluidi di drenaggio)
Volto a trasferire nella clinica le conoscenze molecolari relative alle modalità di insorgenza e di progressione tumorale, in modo da ottenere validi approcci terapeutici.
In particolare, se la RT IntraOperatoria riduce le recidive locali, capire i meccanismi molecolari, attivati nelle cellule di carcinoma mammario, partendo dallo studio dei fluidi di drenaggio delle pazienti trattate o meno con la IORT.


Partial Breast Irradiation (PBI)IORT con elettroni (ELIOT)
Trattamento intraoperatorio a ferita aperta dopo verifica margini
Irradiazione omogenea di tutti i tessuti fino al piano della parete

Partial Breast Irradiation (PBI)IORT con raggi X (Targit)
Source and applicator placed inside tumor cavity
360° irradiation of the entiresurgical cavity

Fase 1:Conservazione
del seno
La strategia conservativa(1970-2010)
Fase 2:Conservazione dei linfonodi
Fase 3:Radioterapia
“mirata” Intraoperatoria
Partial Breast Irradiation (PBI)
TechniquesInterstitial brachytherapyMammoSiteAccelerated three-dimensional
conformal radiotherapy
EliotTargit
Accelerated PBI
IORT

Carcinoma Mammario
Altre Metodologie
in corso di valutazione

RadioImmunoTerapia (IART) La tecnica AVIDINA-BIOTINA sfrutta
l’attrazione naturale tra le 2 molecole. Fase I: vengono iniettati gli anticorpi monoclonali
legati alla Biotina, che si localizzano sul loro bersaglio (il tumore).
Fase II: si inietta l’Avidina che si lega alla Biotina, già presente nel tumore.
Fase III: il 3° giorno il paziente riceve l’ultima iniezione di Biotina, marcata con un isotopo radioattivo, che verrà “calamitata” dall’Avidina presente nel tumore.

HIFUUltrasuoni focalizzati ad alta intensità
(High Focused Ultrasound - HIFU) La metodica utilizza ultrasuoni
estremamente focalizzati in grado di scaldare i tessuti ad una temperatura superiore a 65°C, provocando necrosi coagulativa in circa 20 minuti di trattamento.

IORTPBI (Partial Breast Irradiation)
Surgeons Radiation OncologistsE. Candiani M. RoncadinS. Massarut M. G. TrovòM. Mileto M. TrovòPhysicists RT TechnologistsE. Capra G. FedatoG. Sartor R. BertoliM. Avanzo A. De CarisPathologists Experimental Oncol.T. Perin G. BaldassarreA. Carbone A. Colombatti

Grazie per l’ attenzione !





























