PowerPoint Presentation
Poisoning in children
Dr M A Maleque Molla, FRCP, FRCPCHConultant Pediatric
Intensivist1September 14, 2015 PoisoningDefinition: Poisoning
refers to an injury that results from being exposed to an exogenous
substance that causes cellular injury or death*. Poisons can be
inhaled, ingested, injected or absorbed. 2* WHOEpiodemiologyGlobal
rate of poisoning 282.4 / 100,000 population WHO The global death
rate from poisonings 1.8/ 100,000 population Non-fatal poisoning,
more common among children aged 1 to 4 yearsHighest rates of fatal
poisoning occurs among Children under the age of one year.Most
poisoning occurs at home and common rout of poisoning is oral
3Most common agents involved Over-the-counter preparations:
paracetamol, cough/cold remedies, vitamins and iron tablets,
antihistamines and anti-inflammatory drugs.Prescription
medications: Antidepressants, narcotics, analgesics and illicit
drugs.Household products: Bleach, disinfectants, detergents,
cleaning agents, cosmetics, vinegar.Paraffin/Kerosene.Pesticides:
insecticides (Organophosphorus compound).Poisonous plants.Animal or
insect bites: Scorpion sting, snake bite, Dog.
World report on child injury prevention, WHO 200444Evaluation of
poisoned patientPriority: Stabilization of the Airway,
Breathing,& CirculationDiagnosisHistoryPatient age and sex,
wt.The type of substance involved, Method of exposure (i.e., skin
contact, inhalation, or ingestion).Assessment of the severity of
the exposurePhysical examinationInvestigationsNote: concomitant
trauma or illness must be recognized and addressed prior to
initiation of decontamination5HistoryWhat poison has been taken?How
much has been taken?When the poison has been taken?What are the
advarse effect of the poison?Reliability- Whether any poison has
been taken?6History (cont..) What poison has been taken ?: can be
identified from;Container Illustrated chart How much poison has
been taken ?Calculating the missing amount from the container. In
doubt, always calculate maximum amount of poison that has been
consumed. When the poison has been taken?: Approximate time elapsed
since ingestion or exposure.
7
History (cont..) What are the adverse effects of the poison?
Information can get from;From books, internet, pharmacyPoison
Information centers: Tel no. Riyadh # 011 4355555/1999,2003, Jeddah
# 021 6720711, Makkah # 021 5575065, Madinah# 041 8462564
8History(cont..) Whether any poison have been ingested?Any
doubt, take that the child has ingested the poison. A history of
medication used by the family members. Poisoning should be
considered for any child, who present with acute onset of; Altered
mental status. Multi organ system dysfunction of unexplained
cause.Respiratory or cardiac compromise. Unexplained metabolic
acidosis. Seizures, or a puzzling clinical picture. 9Physical
examinationThorough physical examination from head to toe
Evaluation of mental status and vital signs, should be repeated
frequently The diagnosis may be assisted by; Temperature
alterationsBlood pressure and heart rate alterationsRespiratory
disturbancesPupillary findingsSkin findingsNeuromuscular
abnormalities Mental status alterationsCharacteristic odors e.g.
acetone, bitter almond, Garlic In case of unknown poison ingestion,
physical findings should be sought to define a particular toxic
syndrome (toxidrome).10ToxidromesAnticholinergics: Atropine,
scopolamine, TCAs, phenothiazines, antihistamines, antipsychotic
mushrooms, Hot as a hare, Blind as bat, dry as a bone, red as a
beet, mad as a hatterCV: tachycardia, hypotension, hypertension,
arrhythmiaGI/GU: decreased bowel sounds, urinary retentionNeuro:
agitation, hallucinations, coma, extrapyramidal movements,
mydriasis, hyperthermia11ToxidromesMascarinic effectNicotinic
effectDiaphoresis/diarrheaUrinationMiosisBrdycardia/bronchospasmEmesisLacrimation
excessSalivation excess
Muscle fasciculationCrampingWeakness (extreme is diaphragmatic
failure)Autonomic hypertension, tachycardia, pupillary dilation,
and pallor
Cholinergics: Organophosphates and
carbamates1212ToxidromesSympathomimetic: Salbutamol, Amphetamine,
Cocain, Ephedrine.Anxiety, Delusion, Diaphoresis, hyperreflexia,
mydriasis, paranoia, seizure Tachycardia, hypertension, mydriasis,
agitation, seizures, diaphoresis, psychosis, hyperthermia
OPIOID; Morphine, hydrocodone, methadoneHypoventilation,
Hypotension, Miosis, Sedation, Hypothermia, Ileus.
13InvestigationsBlood glucose, urea & ElectrolytesBlood gas
& Acid base statusSerum osmolality & osmolal gap, anion
gapQuantitative serum concentration of drugs- paracetamol
salicylate, IronUrine analysis; RabdomyolysisECG.Toxicology
screens: indicated in children in whom the diagnosis of poisoning
is uncertain.Samples of blood, first voided urine , vomitus, and
gastric contents should be save for subsequent analysis. Plain
radiographs of the chest & abdomen when indicated.14Management
Management of the poisoned child depends uponSpecific poison(s)
involved, Presenting and severity of illness,Elapsed time between
exposure and presentation.
Remember the mainstay of therapy is supportive 15ManagementA.
General ManagementABCDDecontamination: Techniques used to prevent
the absorption of the toxic substance Enhanced elimination:
techniques which accelerate removal of a toxins from the body
B. Specific ManagementAntidote: a substance which can counteract
a form of poisoning16Surface decontamination e.g. Organophosphate
poisoning; Removal of the cloths and wash with soap &
waterIrrigation of eyes if affectedGI Decontamination:Gastric
lavage: Not used routinely, use only selected casesActivated
charcoalWhole bowel irrigationPurgation using
catharticsDecontamination is notalways warranted and may be
contraindicated.172. Decontamination
Activated charcoal(AC)It is an insoluble, non absorbable, fine
carbon powder Maximum benefit, if administered within 1 hour of
ingestion Dose: 0.5- 1g/kg (maximum 50 to 60 gm), can be repeated
at 0.5g/kg Q4-6 hourMultiple-dose: in case of ingested
life-threatening amounts of;Carbamazepine, Dapsone, Phenoberbital,
Quinine, TheophylineCare must be taken to protect the airway,
assess for the presence of bowel sounds.
18Activated charcoal(cont..)Contraindication:Absolute
contraindication: Bowel obstruction or perforationDepressed level
of consciousness Ingested non absorbable acidic or alkaline
corrosives e.g. sodium or potassium hydroxide, or hydrochloric or
sulfuric acid.Ingestion of hydrocarbons e.g., gasoline, kerosene,
liquid furniture polish The poisons which are not bound by AC e.g.
Iron, lead, arsenic.19Agents for which activated charcoal is not
recommended
Heavy metalsArsenicLeadMercuryIronZincCadmiumInorganic
ionsLithiumSodiumCalciumPotassiumMagnesiumFluorideIodideBoric
acidCorrosivesAcidsAlkaliHydrocarbonsAlkanesAlkenesAlkyl
halidesAromatic hydrocarbonsAlcoholsAcetoneEthanolEthylene
glycolIsopropanolMethanolEssential oils20Whole bowel irrigation
(WBI)It refers to the administration of polyethylene glycol
electrolyte solution (PEG-ES) to induce liquid stool and
mechanically flush pills, tablets, or drug packets from the GI
tract. WBI significantly decreased absorption of toxic
materials
21Whole bowel irrigation (WBI)Indication: Ingestion of large
amounts of poisons that are not well bound to AC, sustained-release
medications.Contraindications: Intestinal obstruction, perforation,
ileus, or significant GI bleeding , Persistent vomitingTechnique:
Administration polyethylene glycol electrolyte solution (PEG-ES)
via nasogastric tubeDose: 20 to 40mL/kgper hour until the rectal
effluent is clear, which takes 4-6 hours.
PEG-ES (GoLYTELY)2222Cathartics accelerate the evacuation by
fluid load in the intestine and stimulating bowel motility. They
shouldneverbe used as the sole method of GI
decontamination.Recommended agent:0.5g/kg(1 to 2mL/kg)of 7 percent
Sorbitol(0.9g/mL)4mL/kgor 250 mL of Magnesium citratein a 6 percent
suspensionSorbitol is not recommended for use in children younger
than one year of ageIf a cathartic is used, it should be limited to
a single dose in order to minimize adverse effects23Use of
CatharticsEnhance elimination of PoisonsUrinary alkalinization and
forced diuresis: eg, salicylates and Phenobarbital.Hemodialysis:
significant ingestion of alcohols, theophylline, Lithium,
Salicylates.Hemoperfusion: Theophylline, Carbamazepine, valproic
acid, procainamide.Exchange transfusion: arsine or sodium chlorate
poisoningPeritoneal dialysis, Hemofiltration 24Specific
treatmentAntidotesVery few poisons have antidotes.Information can
be found in books or from Poison Information Center25Table.
Antidotes for some common
toxicantPOISONANTIDOTEParacetamolN-AcetylcysteineAnticholinergicsPhysiostigmine
Lead/Heavy MetalsBAL in oil
(dimercaprol)AnticholinergicsPhysiostigmineBeta BlockersGlucagon,
CateholaminesCarbon MonoxideOxygenCyanideAmyl nitrate, Sodium
Nitrate, Sodium ThiosulfateEthylene GlycolDialysis, Fomepizole,
EthanolIronDesferoxamineIsonazidPyridoxineLead/Heavy MetalsDMSA,
BAL, EDTAMethemoglobin Producing agentsMethylene
blueNarcoticsNarcanOrganophosphatesAtropine,
PralodiximePhenothiazinesBenadryl26DispositionPatient can send home
after 4-6 hour of observation if poison is less toxic. Always admit
if Symptomatic. Ingestion of iron, tricyclic antidepressant,
digoxin and aspirin.Unconscious child should be admitted in
pediatric intensive care unit.
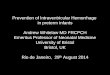
27SPECIFIC POISONING28ParacetamolMost common ingestion in
toddlers, preschoolers and adolescentsToxic dose: > 150
mg/kgKinetics dictate that a serum level to be checked 4 hours
after ingestion4 hour toxic blood level 150ug/dlApply the level to
the management nomogram
29Rumack-Matthew nomogram for single acute paracetamol
ingestions30
30Paracetamol PoisoningStage I(1/2 - 24 hours)Malaise, nausea,
vomiting, pallor, diaphoresisStage II (24 - 72 hours)Asymptomatic,
right upper quadrant pain, increasing LFTs, PT, PTT & INRStage
III (72 - 96 hours)Liver failure, in severe cases renal failure
& multi organ failureStage IV (4 - 14 days)Resolution of liver
injury & Recovery
31ManagementActivated charcoal 1 gm/kgPlasma paracetamol level
at 4 hours and plot on nomogramN-Acetylcysteine(NAC), orally:If
serum level above the line of possible hepatotoxicityIngested >
150 mg/kg & no facilities to do serum level of paracetamol,
Patients with an unknown time of ingestion beyond 24 hours and a
serumconcentration >10mg/L(66mol/L)Dose of NAC: Loading Dose:
140mg/kg. Maintenance Dose: 70mg/kg, 4 hourly for 17 dosesIV :
Indicated if patient is unable to take orally and present within
8-16 hours of ingestionDose: (Acetadote) 150 mg/kg over 1hr,
followed by 50 mg/kg over 4 hr, followed by 100 mg/kg over 16
hr
32NAC therapyIs most effective when initiated within 8 hr of
ingestion, Shown to have benefit even in patients who present in
fulminant hepatic failureThere is no benefit before 4 hr post
ingestion. 33Iron34Available preperationFerrous sulfate -20%
elemental ironFerrous gluconate- 12% elemental ironFerrous fumerate
-33% elemental iron
Toxic Dose: Elemental Iron60 mg/kg potentially life
threatening
Clinical featuresPhase I (Gastrointestinal): 30 min 6
hoursNausea, Vomiting correlate with high toxicity, Diarrhea;
abdominal painGI haemorrhage bloody diarrhea, hematemesisSevere
hypotensionPhase II (Latent): 6-24 hours post ingestionPatient
appears better apparent improvementIn severe poising, this stage
may be absent.In this stage, iron accumulates in mitochondria and
various organs
355 Phases5 stagesPhase III (Shock): 6-72 hours post ingestion;
Hypoglycemia, Metabolic acidosis, Circulatory Failure-ShockPhase IV
(Hepatotoxic): 22-96 days post ingestionSigns of hepatic necrosis
raised AST, ALT and direct bilirubin, prolonged PTRenal Failure,
Metabolic Acidosis, Bleeding diathesis, Adult Respiratory Distress
SyndromeComa DeathPhase V: 2-8 weeks after ingestionSigns of
intestinal obstruction due to scarring and pyloric stenosis
36Clinical features(cont..)InvestigationSerum Iron 2-6 hours
post ingestion, TIBCSerum Iron >350gm/dl- mild to moderate
toxicitySerum Iron >500gm/dl- severe toxicity needs urgent
interventionGreater than 1000mcg/dL Significant morbidity and
mortalityBlood glucose; Blood glucose >150 mg/dl moderate to
severe toxicityCBC, U&Es LFT, WBC > 15000 /cmm- associated
with moderate to severe toxicityPlain x-ray
abdomenABG/VBG37ManagementSupportive careABCD Correct dehydration
Removal of IronWhole bowel irrigation with colonic solution
(colyte, golytely) if large number of tablets are ingested.No
activated charcoal to be given because it does not bind iron.Repeat
x-ray on abdomen after decontamination.If clumps of tablets can be
seen in x-ray and fail to remove with usual procedures, surgical
removal is indicated in rare cases.Desferoxamine orally promote
iron absorption, so should not be given
orally38ManagementDefinitive treatment: Desferoxamine intravenous
infusion.Indications:Serum Iron at 4-8 hours >500g/dl regardless
of symptoms orSerum Iron >350g/dl + moderate to severe
symptomModerate to severe symptom regardless of serum
ironSignificant no. of pills on abdominal x-RayDose:By IV infusion
15mg/kg/hour maximum 6 g/24 hoursBy intramuscular 90mg/kg/dose 8
hourly maximum 6g/24 hours
3939SALICYLATE POISONINGToxic Dose: >150 mg/kgClinical
Manifestation:Early: nausea vomiting tachypnea, deep sighing
respiration, tinnitus, high temperature, lethargy, and
dehydration.Late: Bleeding tendency, coma.
40Clinical featuresImportant signs and laboratory findings:Phase
I: First 12 hoursTachypneaAlkalosisPhase II - 12-24 hoursTachypnea
persist HypokalemiaParadoxical aciduriaPhase III - 4 to 6 in an
infant, or 24 hours in an adolescent or adultDehydration
5-10%Worsening acidosisHypokalemia;
hyperglycemia/hypoglycemiaPulmonary edema, pulmonary
hemorrhageCerebral edema
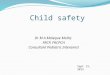
41InvestigationsPlasma Salicylate level no sooner than 6 hours
and plot on the nomogramUrine pH hourlyBlood gasGlucose, serum urea
electrolytes and creatinine 6 hourlyPTLFT.
42Nomogram for Salicylate43
ManagementPlasma salicylate levels 45-65 mg/dl (moderate
poisoning), treat and admit the patient.Plasma salicylate level
>65 mg/dl (severe poisoning), treat and admit in the
ICUDecontamination:Activated charcoal 1 gm/kg.Multiple dose of AC
may be needed in severe poisoningVolume resuscitation:Rehydrate the
child and correct electrolyte specially potassium;Enhance
eliminationUrine alkalinization by IV bicarbonateThe goal is to
achieve a urine pH >7.5 while maintaining a serum pH
7.55.Hemodialysis44Organophosphate poisoning1. Mascarinic
effectDiaphoresis/diarrheaUrinationMiosisBrdycardia/bronchospasmEmesisLacrimation
excessSalivation excess
2. Nicotinic effectMuscle fasciculationCrampingWeakness (extreme
is diaphragmatic failure)Autonomic : hypertension, tachycardia,
pupillary dilation, and pallor
Agents: Malathion, Parathion, Diazenon, Chlorothion45Clinical
features3. CNS manifestations: Anxiety, restlessness, tremor,
confusion, coma, convulsion45ManagementABCRemove cloths and wash
the skin with soap and waterAtropine (vagal block)IV 0.02-0.05
mg/kg every 15 minute until complete atropinization ( dilated
pupil, dry mouth tachycardia, fever) then 1-4 hourly for 24
hourPralidoxime (Protopam, 2-PAM)Regenerates acetylcholinesterase20
- 50 mg/kg/dose (IM or IV)Repeat in 1-2 hour if muscle weakness
does not relieve
46
47Thanks for attention