Embed Size (px)
Citation preview

1
PAEDIATRICS
Paediatric EndocrinologyCommon problems
Dr Craig Jefferies
Teaching Content
1. Diabetes 1. Diabetes
2. Vitamin D2. Vitamin D
3. Thyroid3. Thyroid
4. Puberty and Growth 4. Puberty and Growth
Diabetes definition
Before Insulin After Insulin
PAEDIATRICSCase-1
12 yr old Caucasian girl Mild weight loss, polyuria, polydipsia. Random glucose 20 mmol/l, Trace ketonuria.Father diabetic
From 24 yrs age & Rx insulin, no complications as yet.
BMI SDS +1, No acanthosis nigricansHbA1c always around 6.5% (N= 4-6%)Remains with HbA1c <7% for next 2 years
2
PAEDIATRICSCase-1
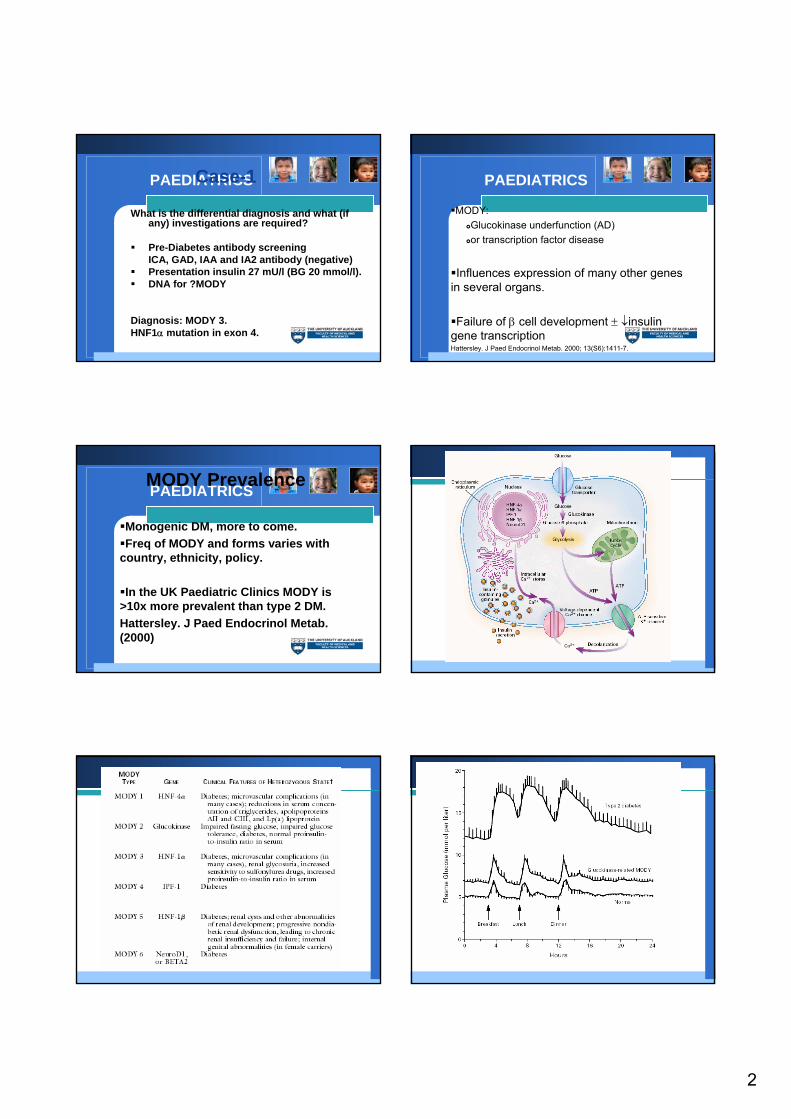
What is the differential diagnosis and what (if any) investigations are required?
Pre-Diabetes antibody screeningICA, GAD, IAA and IA2 antibody (negative)Presentation insulin 27 mU/l (BG 20 mmol/l).DNA for ?MODY
Diagnosis: MODY 3.HNF1α mutation in exon 4.
PAEDIATRICS
MODY: Glucokinase underfunction (AD) or transcription factor disease
Influences expression of many other genes in several organs.
Failure of β cell development ± ↓insulin gene transcriptionHattersley. J Paed Endocrinol Metab. 2000; 13(S6):1411-7.
PAEDIATRICSMODY Prevalence
Monogenic DM, more to come.Freq of MODY and forms varies with
country, ethnicity, policy.
In the UK Paediatric Clinics MODY is >10x more prevalent than type 2 DM.Hattersley. J Paed Endocrinol Metab. (2000)

3
PAEDIATRICSMODY 3
Reputedly commonest form of MODY (65%).
Progressive β cell failure, usually presents with symptomatic hyperglycaemia in 20’s sometimes in adolescence.
Those at risk of developing MODY 3 have normal insulin secretion however fail to increase insulin secretion with increased plasma glucose.
PAEDIATRICSCase-2
A 110 kg 13 yr old Pacific Island female presents with polyuria and polydipsia. Mother has type 2 DM. BG = 30 mmol/lKetonuria =TraceWeight loss 20 KG
PAEDIATRICSCase-2
Cervical and axillary acanthosis nigricans.Tanner 5 breast/pubic hair.BP=140/85 Renal function normalInvestigations:
ICA, GAD negativeDyslipidaemicMicroalbuminuria
PAEDIATRICSCase-2
What sort of Diabetes does she have?Symptomatic Type 2 Diabetes Mellitus
1) Ketonuria Can be present2) “diabetes” autoantibodies negative3) Family history First degree relative4) Pubertal5) Acanthosis nigricans

4
Obesity Trends* Among U.S. AdultsBRFSS, 1985
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 1989
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 1991
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 1995
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)

5
Obesity Trends* Among U.S. AdultsBRFSS, 1997
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 1999
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 2001
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity* Trends Among U.S. AdultsBRFSS, 2003
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
T2DM and obesityGuidelines for type 2 diabetes (Starship)
Who should be tested for diabetes?ANY young person with SYMPTOMS of diabetes
ANDObese* children (normally BMI SDS >3-4 SDS)
WITH acanthosis nigricansAND one of the following additional risks for type 2 diabetes
>10 years of ageHigh risk diabetes ethnic group: Maori, Pacific Island or AsianFirst degree relative with type 2 diabetes Their mother had gestational diabetesPresence of polycystic ovarian syndrome (PCOS)Being known to be hypertensive or dyslipidaemic
Test: Preferably the formal OGTT
Vitamin D

6
Bowed legs Somalian Boy, 18 months old presents with delayed motor milestones, weakness and bowed legs.
Breast fed till 16/12sMother pregnant, wears strict religious coveringsNormal diet, hates milk and drinks ribena
Examination reveals flared epiphyses, hypotonia, and frontal bossing. Rickets confirmed on X-ray
Case: Lab investigations
FBC Mild anaemiaALP 1000 U/LCalcium 2.10 mmol/lPhosphate 0.9 mmol/lAlbumin 40Normal renal function PTH 20 pmol/l (1-5) 25 OH25 OH Vitamin D Low (<25)
Cholecalciferol (D3)
Skin
7 dehydrocholesterol Diet VitD3
UV light
1:25 (OH)2 VitD3 (calcitriol)
25(OH) VitD3 (calcidiol)25α Hydroxlyase
1α Hydroxylase
LIVER
Kidney
Vitamin D intake
“man” received most Vitamin D by sunlight
Diet has only become more important since sunlight exposure and skin area reduced (~5%).Recommended intake
in infants of 10µg/day (400 IU)in the elderly 15µg/day (600 IU) is conservative.
Total body sun exposure provides ~ 250 µg/day (10,000 IU) – consider this the ‘physiological limit’Hypervitaminosis D all caused with doses > 1000 µg/day (40,000 IU)
CausesVitamin D deficiency/ resistance
Nutritional↓ 1α hydroxylase functionVit D receptor mutation
Calcium DeficiencyDietary (no milk, allergies etc)Preterm TPN
Phosphate DeficiencyRenal disease (cystinosis, Fanconi’s etc)Renal loss (X-linked, Autosomal dominant, tumour induced).Preterm TPN

7
Clinical ManifestationsOsseous
CraniotabesFrontal Bossing in early infancyLarge fontanelle with delayed closureHypotonia and delayed walkingRickety rosary, big wristsSkeletal deformities (bow legs, narrowed pelvic outlet, scoliosis)Limb painSeizures
PAEDIATRICS
Thyroid
Thyroid Physiology -1 Thyroid physiology-2
Thyroid Physiology -3PAEDIATRICS
Thyroid
5 day old neonate has an elevated TSH on neonatal screening >100 mIU/LFT4 2.1pmol/l (15-35)FT3 1.2pmol/l (3.9-9.0)TSH 145 mIU/L (0.5-6.0)
Mildly jaundiced quiet baby. No dysmorphicfeatures.

8
PAEDIATRICS
Thyroid scintiscanIncreased unptake into a normal sized, appropriately sited gland.
Dyshormogenesis
Initial treatment with L-thyroxine 10 mcg/kg
Normalization of FT4 and FT3 by day 14
Trial off thyroxine at 3 years of age
PAEDIATRICSCase
6 day old neonate has an elevated TSH on neonatal screening >100 mIU/LFT4 3.8pmol/l (15-35)TSH 135 mIU/L (0.5-6.0)
No features of hypothyroidism or hx or examination.
PAEDIATRICSCase
Thyroid scintiscan – athyreosis
Treated with L-Thyroxine 15mcg/day
TFTs over the first 12 months were normal and minimal increase in her L-Thyroxine was required.
At 13 months of age the mother ran out of L-thyroxine and failed to fill further prescriptions!
PAEDIATRICSCase
But she continued with monthly TFTs.
4 months after stopping L thyroxineFT4 18 pmol/l (15-35)FT3 6 pmol/l (3.9-9.0)TSH 2.5 mIU/l (0.5-6.0)
PAEDIATRICSCase
What is the likely cause for this presentation?A normally formed gland can be missed on thyroid scintiscan in the presence of blocking antibodies. TSH receptor needed for I/technecium uptakeTransient hypothyroidism secondary to TSH blocking antibodies.
A normally formed gland can be missed on thyroid scintiscan in the presence of blocking antibodies. TSH receptor needed for I/technecium uptake

9
PAEDIATRICSGROWTH PAEDIATRICSGrowth regulated by:
Adequate NUTRITIONCaring ENVIRONMENTNormal CHROMOSOMESGood HEALTHAppropriate functioning HORMONES
PAEDIATRICSGrowth Hormone secretion:
Pulsatile with low baseline.Primarily at night (stages III - IV sleep).Increased by: sleep, exercise stress hypoglycaemia, amino acids, malnutrition, sex steroids.Decreased by: obesity, psychosocial deprivation.

10
PAEDIATRICSGH actions PAEDIATRICSSex steroids
Greatest effect on skeleton maturation.Estrogen or TestosteroneESTROGEN
Responsible for epiphyseal maturation/closure in both sexes.
ESTROGEN
PAEDIATRICSThyroid hormones
Facilitatory role in growth.Necessary for normal GH secretion and growth plate development (and body proportions).
PAEDIATRICSInsulin
Facilitatory role in growth.Provides substrate for growth (amino acid uptake, glycogenesis and lipogenesis).
Normal GrowthThe infant/child/puberty model of growth: (Karlberg)•Infant - Birth to 2 years. Rapid growth at birth declining rapidly over the first 2 years of life – less growth hormone dependent.
•Childhood - 2 years until puberty. Relatively constant annual growth - growth hormone
•Puberty - growth primarily dependent on sex steroids and increased growth hormone release.
Sex steroids cause fusion of skeletal epiphyses and growth arrest.
PAEDIATRICSHeight velocity (HV)
HV differentiates normal variant short stature from pathologicalshort stature.
HV calculated over 6-12 month interval because of errors in measurement .Normal height velocity 25-75 PC.
Note HV curve for children with delayed puberty.

11
PAEDIATRICS
Short Stature
PAEDIATRICS
A common clinical problem.A symptom and not a disease.May represent a variant of normal growth.May indicate pathology.One of the commonest manifestations of
chronic illness; recognised or unrecognised.
PAEDIATRICSShort Stature History
Mother and fathers heights.MPH = M (cm) + F (cm) ±13 cm /2.MPH range ±8 cm.FH short stature: males <165 cm
females <152 cmFH delayed puberty: menarche >14 yrs in females and continued
growth after high school in males.
Look at other sibs child development records.

12
PAEDIATRICSGrowth Disorders
Normal height velocity:Familial short statureConstitutional delay in growth and
development
Poor height velocity:Usually pathologicalDisproportionate
Bone Age
Greulich and Pyle standards.Imprecise picture matching.1 yr intervals.Tables of Bayley & Pinneau for final Ht prediction.
PAEDIATRICSNormal Variant Short Stature
Familial short stature.Constitutional delay of growth and development.Account for >95% of children who present with
short stature.HALLMARK IS NORMAL HEIGHT VELOCITY.
PAEDIATRICS
PAEDIATRICSIUGR/SGA
Intrauterine growth retardation or small for gestational age: very common.Birth weight <10th PC for gestation.Catch-up growth above 3rd PC usually occurs by 6/12 but
may drag on to 2 yrs.Short stature by 2 yrs usually associated with short final
height.Approx 10% become short adults.
PAEDIATRICSTurner Syndrome
Consider in ALL girls with unexplained short stature or Ht below MPH range.Commonest feature is short for MPH (100%).50% will only have short stature as clinical feature.Present with short stature, poor HV or delayed puberty.

13
Precocious Puberty
The three puberties of lifeDefinitions- Normal Puberty
Normal Puberty (All in tempo)Central activation of the H-P-Gonadal axis Progressive sequential changesAppropriate rate (over 3-4 years)
Girls (First Sign)Breast development before Growth Spurt
Boys (First Sign)Increased testicular enlargement>4ml (orchidometer)Growth spurt later

14
Precocious Puberty -Definition
Pathological processToo earlyToo fastPathological hormonal milieu
ArbitraryFemales <8 years (menarche <9 years)
This will be 2% of healthy girlsMales <9 years
Clinical confirmationClinical signs (and USS in females)Hormonal evaluationBone age advancementRate of acceleration
Clinical signs of sustained sex steroids exposure
Growth height velocityheight compared to mid parental height
Breasts progressive developmentAndrogen Pimples/acne/body odour
Introitus pink-red epithelium pre oestrogenwhite-pink with sustained oestrogen exposure(cornification of epithelium)
Investigation (First line)Bone Age (X-ray L hand and wrist)
USS pelvis Uterine size, sometimes useful info on ovaries.+/- TFT
Unhelpful/ Useless/ Un-interpretable testsFSH and LHTestosteroneOestradiol
Differential Diagnosis
Endogenous Exogenous
CentralGnRH dependent
PeripheralGnRH independent
O/CHRTE2 creamsSoy?‘Natural remedies’
GnRH (LHRH) stimulation testPubertal response LH dominantPrepubertal FSH dominant
Aetiology of Central PPIdiopathic
Structural AbnormalityHypothalamic HamartomaMeningomyleocoeleHydrocephalusNF-1
CNS insultNeonatal EncephalopathyCranial IrradiationTrauma/Surgery

15
Aetiology of peripheral PP
OvariesCyst (benign/malignant)McCune-Albright
TestesTumourLH receptor+
Liver (beta HCG)Adrenal
TumourEnzyme defect
OtherExogenous (dad’s Androgel®)
CPP treatment
GnRH analoguesDepot GnRH analogues first line
Monitoring and FollowupRegular bone age (yearly)Some advocate regular USSGnRH stim tests
Treatment cessation
PAEDIATRICS
Paediatric EndocrinologyCommon problems