Embed Size (px)
Citation preview

DOSE DIALITICA E OUTCOME: UN PROBLEMA ANCORA APERTO
Angelo F. Perego Nefrologia e Dialisi Ospedale Vittorio Emanuele III Monselice (PD) ULSS 17 Veneto
GDS SIN
“TRATTAMENTI DEPURATIVI IN AREA CRITICA”

Status of issues concerning RRT use in the ICU Continuous renal replacement therapy: recent advances and future research John R. Prowle & Rinaldo Bellomo Nature Reviews Nephrology 6, 521-529 (September 2010)
CRRT dose A resolved issue in favor of conventional dosing (target effluent
flow rate 20–25 ml/kg per h) ????!!!!! = 42 L/die ??? CRRT versus IHD Consensus in favor of CRRT in hemodynamically unstable critically ill patients, but without formal evidence Timing of CRRT Unresolved issue that requires further research CRRT outcomes Unresolved issue; studies to date may have been too focused on mortality over renal recovery and other patient-centered outcomes CRRT modality Unresolved issue—CRRT modalities might be equivalent


GFR = 130-180 L/die

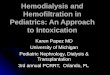
Figure 1 Relationship between delivered RRT intensity and survival in critically ill patients with acute kidney injury (AKI)
John A. Kellum & Claudio Ronco (2010) Results of RENAL—what is the optimal CRRT target dose?Nat. Rev. Nephrol. doi:10.1038/nrneph.2010.15

CRRT cosa?
• SCUF • CVVH • CVVHD • CVVHDF
• EDD; SLED • SLEDD • SLEDD-f • CPFA
• NO REINFUSIONE • POST-DILUIZIONE • PRE-DILUIZIONE • PRE+POST-
DILUIZIONE

Effluente…COSA?
• Ultrafiltrato puro di plasma ( post-dil)? • Ultrafiltrato da pre-diluizione? • Ultrafiltrato da pre+post-diluizione? • Bagno di dialisi?

Effluent Volume in Continuous Renal Replacement Therapy Overestimates the Delivered Dose of Dialysis R. Claure-Del Granado*,Etienne Macedo*,Glenn M. Chertow†,Sharon Soroko*,Jonathan Himmelfarb‡,T. Alp Ikizler§, Emil P. Paganini‖,Ravindra L. Mehta*
Conclusions:
Effluent volume significantly overestimates delivered dose of small solutes in CRRT. To assess adequacy of CRRT, solute clearance should be measured rather than estimated by the effluent volume.
CJASN March 2011 vol. 6 no. 3 467-475

9
Percent Decrease in Solute Clearance During High-Dose Pre-Dilution CVVH#,*
Troyanov et al, Nephrol Dial Transplant 2003
Filter (m2) Urea Creatinine Phosphate β2M M-100 (0.9)a
33.8 ± 2.6 38.2 ± 2.2 38.8 ± 1.6 39.0 ± 3.1
HF1000 (1.1)b
34.4 ± 2.3 39.4 ± 1.5 41.4 ± 4.0 44.0 ± 2.4
#: Results expressed as % decrease relative to post-dilution
*: QB = 125-150 mL/min; QF = 4.5 L/hr a: mean Hct = 0.26 ± 0.04 b: mean Hct = 0.30 ± 0.05


Table 1 Randomized trials comparing CRRT with IHD in the ICU
Prowle, J. R. & Bellomo, R. (2010) Continuous renal replacement therapy: recent advances and future research
Nat. Rev. Nephrol. doi:10.1038/nrneph.2010.100

CRRT-Associated Mortality in Major RCT’s
Clinical Trial Comparison APACHE II Endpoint Mortality Ronco et al (2000) CRRT Dose 22 15-day
2 59%
3
Mehta et al (2001) IHD vs CRRT 25.5 Hospital 66%
Augustine et al (2004) IHD vs CRRT - Hospital 68%
Saudan et al (2006) CRRT Dose 25 90-day 66%3
Vinsonneau et al (2006) IHD vs CRRT 25 60-day 68%
Lins et al (2008) IHD vs CRR 27 Hospital 58%
Tolwani et al (2008) CRRT Dose 26 Hospital 60%3
ATN Trial (2008) Dialysis Dose 26.3 60-day 52.3 4
RENAL Trial (2009) CRRT Dose ~261 90-day 45%
1: APACHE III score 102-103 2: After CRRT cessation 3: Mortality in low-dose group 4: Overall (CRRT + IHD) mortality

Table 2 Randomized controlled trials comparing CRRT dose in the ICU
Prowle, J. R. & Bellomo, R. (2010) Continuous renal replacement therapy: recent advances and future research
Nat. Rev. Nephrol. doi:10.1038/nrneph.2010.100

Comparison of Major CRRT Dose Trials
Ronco Saudan Tolwani ATN Number of patients 425 206 200 1124
Multi-center RCT No No No Yes
CKD (%) NA 33 42 Exclusion
Predominant AKI cause Surgical Sepsis Sepsis Ischemia
APACHE II ~23 25 26 ~29
Initiation BUN (mg/dL) 53 83 75 65
Modality post CVVH pre CVVHDF pre CVVHDF pre CVVHDF
% Convective 100 ~60 43-44 50
Prescribed dose (mL/kg/h) 20/35/45 25/42 20/35 20/35
Effective dose (mL/kg/h) 20/35/45 ~20/37 ~17/29 ~17/27
ICU wait (days) NA NA 8 6.9

ATN Study



18
• The National Cooperative Dialysis Study (NCDS) should give pause to
those who favor an immediate reduction in CRRT dose • NCDS was performed in US chronic HD patients during the late
1970‘s • First large-scale trial to study the relationship between dose and
survival • A flawed analysis of the data resulted in a misinterpretation of the
results and a downward trend in dose prescription for 15 years in the US
• The results were disastrous, with residual effects still influencing clinical practice in the US
• The NCDS debacle argues strongly against a “rush to judgment” with regard to the ATN Trial results
Interpretation of ATN Results: A Cautionary Note for Physicians

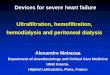
Molecular Transport Mechanisms
Ultrafiltration
Diffusion
Convection
Adsorption
Fluid Transport
Solute Transport }


Sieving Characteristics
MWCOMWCO
0.00.0
20.020.0
40.040.0
60.060.0
80.080.0
100.0100.0
11 1010 100100 10001000
Molecular Weight (Molecular Weight (kDakDa))
Perc
ent P
erm
eate
dPe
rcen
t Per
mea
ted
Feed
permeate
CC
=S
MWCO = Molecular Weight Cut-Off
caratteristiche di SETACCIO che identificano il CUT-OFF point



CONSIDERAZIONE FINALE
Tutta la letteratura, ad oggi, non mostra
differenze, in termini di sopravvivenza, tra
trattamenti intermittenti; continui; diffusivi,
convettivi o combinati; ad alta o bassa dose…
QUALE IPOTESI UNIFICANTE PER SPIEGARE
QUESTA ANGOSCIANTE ASSENZA DI
RISULTATI?

BERNARDINO DI BETTO detto il PINTURICCHIO 1495 Perugia, Galleria Naz.Umbra

RIFLESSIONI INTORNO ALLA DOSE • MODALITA’ • SPETTRO RIMOZIONE • QB • QF • QD • PRE , POST, PRE+POST • FILTRO: TIPO di MEMBRANA, CUT-OFF, SUPERFICIE • ANTICOAGULAZIONE • TIPI DI ACCESSO VASCOLARE

Vol. 1, No. 3, 1983
Original Paper Long-Term Clinical Results with High-Efficiency Hemofiltration
G. Civati, C. Guastoni, A. Perego, U. Teatini, M. Giachetti, F. Zoppi, L. Minetti Renal Unit and
Department of Biochemistry, Niguarda Ca' Granda Hospital, Milano, Italy Uremic toxicity is widely thought to be caused by the retention of a large spectrum of solutes, ranging from small to large molecular weight. Hemodialysis (HD), although achievinga high clearance of small molecules, does not permit a satisfactory removal of middleand large molecules. Conventional hemofiltration (CHF) improves the removal of middleand large molecules, but removes less small molecules compared to HD. A really satisfactory removal of small, middle and larger solutes can only be achieved by post-dilution high-efficiency hemofiltration (HEHF), surpassing the performances of both HD and CHF. On this basis the authors formulate a prescription about hemofiltration dose (2 L/KG/week). The artificial GFR given to each patient must be comparable to that of a symptom-free patient with a residual GFR of 8-10 ml/min.