Embed Size (px)
Citation preview
1. Introduction
2. HIV-1 integrase: structure and
function
3. Pharmacokinetics
4. Clinical trials
5. Safety and tolerability
6. Resistance issues
7. Conclusions
8. Expert opinion
Drug Evaluation
Dolutegravir: an exciting new kidon the blockJose Luis Blanco Arevalo† & Gary George Whitlock†University of Barcelona, IDIBAPS, Hospital Clinic, Barcelona, Spain
Introduction: Dolutegravir is the first second-generation integrase inhibitor
approved for the treatment of naıve as well as experienced HIV-infected
individuals.
Areas covered: Data from pharmacokinetics, efficacy, safety, tolerability and
resistance are reviewed from in vitro studies, Phase II and III clinical trials pub-
lished in PubMed (Dolutegravir; S/GSK1349572) or presented in international
meetings.
Expert opinion: Data from studies and clinical trials indicate that dolutegravir
is safe, well tolerated and highly efficacious in the treatment of both
antiretroviral-naıve and treatment-experienced patients and appears to
have a higher genetic barrier to resistance than first-generation integrase
inhibitors.
Keywords: antirtroviral therapy, dolutegravir, HIV, integrase-inhibitors
Expert Opin. Pharmacother. (2014) 15(4):573-582
1. Introduction
Since the approval of raltegravir (RAL) in 2007 and that of elvitegravir (EVG) in anew once-a-day fixed-dose combination pill Stribild� (EVG, cobicistat, emtricita-bine, tenofovir disoproxil fumarate), the challenges for the new drug class of inte-grase inhibitors (INIs) were addressed by improving the weakest points of thefirst-generation drugs in this class: dose administration and genetic barrier. Dolute-gravir (DTG) (Box 1) (Trivicay�) is the first second-generation INI recentlyapproved by the US FDA. The aim of this review is to assess the clinical efficacy,safety, pharmacokinectic profile, drug interactions and resistance profile of thisnew antiretroviral (ART) agent.
2. HIV-1 integrase: structure and function
Following reverse transcription, integrase (IN) cleaves the conserved dinucleotide’sGT from the 3¢-ends of double-stranded HIV-1 DNA leaving two CA overhangs(the 3¢-processing reaction). IN remains bound to each of the 3¢-ends, circularizingthe HIV-1 pre-integration complex (PIC). IN then binds the host protein, lens-epithelial derived growth factor (LEDGF), which translocates the PIC to thenucleus where IN catalyzes a nucleophilic attack of the viral 3¢-hydroxy ends onthe phosphodiester bonds of host genomic DNA (the strand-transfer reaction).Although IN catalyzes both the 3¢-processing and strand-transfer reactions, onlythose compounds that specifically inhibit strand transfer have been effective INIs.Indeed, the development of a high-throughput screening assay for the identificationof strand-transfer inhibitors that bind IN in complex with viral DNA heralded themodern era of INIs development [1].
HIV-1 IN contains 288 amino acids encoded by the 3¢ end of the HIV-1pol gene. It is composed of three functional domains. The catalytic core domain(CCD), which encompasses amino acids 51 -- 212, contains the catalytictriad D64, D116 and E152 and the viral DNA-binding site. D64 and
10.1517/14656566.2014.868883 © 2014 Informa UK, Ltd. ISSN 1465-6566, e-ISSN 1744-7666 573All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.
D116 coordinate the positioning of a metallic cationic cofac-tor (Mg2+ or Mn2+), which is essential for IN function. TheN-terminal domain (NTD), which encompasses amino acids1 -- 50, is characterized by an HHCC zinc-binding motif.Its primary role appears to be to facilitate IN multimerizationthrough its extensive contacts with adjacent CCD monomers.The C-terminal domain (CTD), which encompasses aminoacids 213 -- 288, binds host DNA nonspecifically.There are published crystal structures of the HIV-1 IN
CCD plus CTD domains, the CCD plus NTD domains, theCCD bound to LEDGF and the CCD bound to an active-site inhibitor, the prototype diketo acid inhibitor 5CITEP(reviewed in 2 -- 4). But the relative conformation of theCCD, NTD and CTD domains and the tetrameric state offunctional HIV-1 IN has been inferred primarily from crystal-lographic studies of the homologous IN of the prototypefoamy virus (PFV) [2]. The applicability of the PFV IN struc-ture to HIV-1 IN is validated by the consistency of the PFVIN structure with HIV-1 IN biochemical data and by theability of PFV IN to co-crystallize with RAL and EVG [2,3].HIV-1 INIs are structurally diverse molecules that contain
a motif for binding the essential divalent metal cations Mg2+
or Mn2+ and a hydrophobic region for binding within thecavity formed by IN and the 3¢ HIV-1 DNA ends containingthe terminal CA dinucleotide. RAL, EVG and DTG displaceviral DNA in the active site and contact several active-siteamino acids -- including those in a mobile loop extendingbetween positions 140 -- 149 [4-6].
3. Pharmacokinetics
DTG is readily absorbed with a median time to peak fastingplasma concentration between 0.5 and 1.25 h, after whichits plasma concentration declines biexponentially [7]. Inrepeat-dose studies in healthy subjects, both the area underthe curve (AUC) and the plasma concentration of DTG atthe end of the dosing interval were proportional to the doseadministered over the range 10 -- 50 mg [7,8]. There is littleinter-subject variability (coefficient of variation, range25 -- 50%) observed in single- and repeat-dose pharmacoki-netics (PK) studies [7-9]. After multiple doses, steady-stateDTG concentrations are reached by day 5 in once-dailydosing studies [7]. The trough concentration for the DTG50 mg suspension dose was approximately 25-fold abovethe protein-adjusted 90% inhibitory concentration (IC90)for HIV-1 [9]. The terminal elimination half-life (t1/2) is13 -- 15 h which allows once-daily dosing [7].
In 18 healthy volunteers given DTG 50 mg in the fastingstate or with meals of varying fat content, the mean AUC forDTG concentration increased modestly by 66% for subjectsgiven high-fat-content meals compared with those fasted [10].This increase in plasma concentration is not expected toimpact clinical safety, allowing DTG to be administered withor without food.
DTG has a modest drug interaction profile. Its major and
minor metabolic pathways are uridine diphosphate glucuro-
nosyl transferase (UGT)-1A1 and cytochrome P450 (CYP)-
3A4, respectively [8]. No significant CYP3A induction or
inhibition effects have been noted. It is expected that DTG
will be available as a fixed-dose coformulation with abacavir
and lamivudine. As a class, NRTIs do not undergo hepatic
metabolism by the CYP pathway and, therefore, there is a
low potential for drug interactions between this class and
DTG. An open-label repeat-dose study in 15 healthy volun-
teers demonstrated no clinically significant drug interaction
between DTG 50 mg and tenofovir disoproxil fumarate
300 mg concomitantly given daily [11]. In fact, no dose adjust-
ments are suggested with most ARTs [8]. However, DTG
coadministration with etravirine (ETV) led to significant
reductions in AUC, Cmax and Ctrough to such an extent that
the study authors suggested that DTG and ETV should not
be coadministered [12]. Although, they suggest that the addi-
tion of ritonavir-boosted PI to the regimen would allow their
coadministration with no dose adjustments.In healthy volunteers there are some data on medications
commonly co-prescribed for people living with HIV [8]. Forexample, there is low potential for DTG to interact withoral contraceptive pills. A study of 16 healthy females receiv-ing twice-daily DTG 50 mg and once-daily Ortho-Cyclen, acombined oral contraceptive containing norgestimate andethinyl estradiol, demonstrated no change in the pharmacoki-netic profile of DTG, norgestimate or ethinyl estradiol [13].DTG chelates with products containing metal cations such
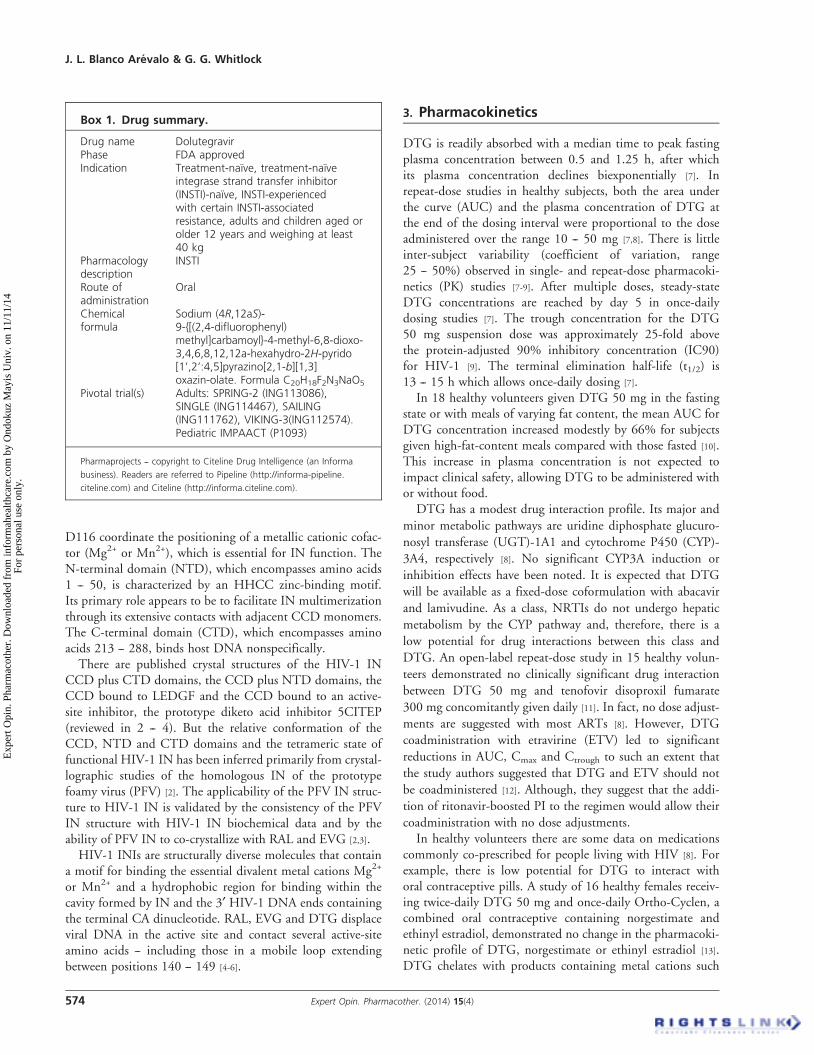
Box 1. Drug summary.
Drug name DolutegravirPhase FDA approvedIndication Treatment-naıve, treatment-naıve
integrase strand transfer inhibitor(INSTI)-naıve, INSTI-experiencedwith certain INSTI-associatedresistance, adults and children aged orolder 12 years and weighing at least40 kg
Pharmacologydescription
INSTI
Route ofadministration
Oral
Chemicalformula
Sodium (4R,12aS)-9-{[(2,4-difluorophenyl)methyl]carbamoyl}-4-methyl-6,8-dioxo-3,4,6,8,12,12a-hexahydro-2H-pyrido[1’,2’:4,5]pyrazino[2,1-b][1,3]oxazin-olate. Formula C20H18F2N3NaO5
Pivotal trial(s) Adults: SPRING-2 (ING113086),SINGLE (ING114467), SAILING(ING111762), VIKING-3(ING112574).Pediatric IMPAACT (P1093)
Pharmaprojects -- copyright to Citeline Drug Intelligence (an Informa
business). Readers are referred to Pipeline (http://informa-pipeline.
citeline.com) and Citeline (http://informa.citeline.com).
J. L. Blanco Arevalo & G. G. Whitlock
574 Expert Opin. Pharmacother. (2014) 15(4)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

as antacids, thus preventing DTG binding to magnesium ionslocated at the catalytic site of the IN enzyme itself. Therefore,although DTG can be taken with antacids with no dose adjust-ment, PK studies suggest that DTG should be administered2 h before or 6 h after antacids [14]. However, the simultaneousadministration of DTG with omeprazole demonstrated a non-significant decrease in DTG exposure and, therefore, may becoadministered at the same time [14].
4. Clinical trials
4.1 Treatment-naıve patientsSPRING-1 is a 96-week, Phase IIb, randomized, partiallyblinded, dose-ranging study in treatment-naıve subjects [15].Two hundred and eight participants were randomized to receiveDTG once daily at one of the three doses, 10, 25 or 50 mg, orefavirenz (EFV) 600 mg once daily plus a co-formulated back-bone: either abacavir/lamivudine or tenofovir/emtricitabine. Ofthe 205 participants who received the study drug, the propor-tion achieving plasma HIV-1 RNA < 50 copies/ml at week96 was 79, 78 and 88% for DTG 10, 25 and 50 mg, respec-tively, compared with 72% for EFV. DTG at all doses led torapid viral load reduction, with 82%of all participants receivingthe study drug achieving viral load < 50 copies/ml. The medianCD4 increase from baseline was 338 cells/µl with DTG (alltreatment groups combined) compared with 301 cells/µl withEFV.
DTG has been compared against existing ARTs in twomultinational 96-week, Phase III, randomized, double-blind,non-inferiority studies in treatment-naıve subjects: EFV(SINGLE) and RAL (SPRING-2 study).
SINGLE enrolled 833 participants to be randomly allo-cated either once-daily tenofovir/emtricitabine/EFV coformu-lated in single tablet regimen (EFV/tenofovir/emtricitabine)or once-daily DTG 50 mg plus coformulated abacavir/lamivudine [16]. Apart from being treatment naıve for entryinto the study, subjects were required to have a viral load ofat least 1000 copies/ml, no primary HIV viral resistance anda negative HLAB*5701. Most participants were men (84%)and two-thirds were white. Median baseline HIV viral loadwas approximately 50,000 copies/ml in each groupand 32% with at least greater than 100,000 copies/ml.The median CD4 count was comparable in both arms(337 cells/µl). The 48-week data were presented at the 52ndAnnual ICAAC meeting in San Francisco in September2012. The results showed that 364 participants (88%) inthe DTG plus abacavir/lamivudine arm achieved the primaryendpoint of viral load < 50 copies/ml at 48 weeks versus338 participants (81%) in the EFV arm (adjusted difference7.4%; 95% confidence interval [CI]: 2.5 -- 12.3). Althoughdesigned to test non-inferiority, the SINGLE data establishedthat DTG plus abacavir/lamivudine achieved superiority toEFV/tenofovir/emtricitabine. The response was similar forpatients with baseline viral loads above and below100,000 copies/ml in both arms. Additionally, significantly
greater CD4 cell-count increases were seen in the DTG arm(267 vs 208 cells/µl, respectively). In each arm there were 4%protocol-defined virological failures. Of note, fewer partici-pants stopped treatment due to side effects in the DTG versusEFV/tenofovir/emtricitabine arm (2 vs 10%). The authorssuggest that the better tolerability of DTG likely explainsits better performance against EFV/tenofovir/emtricitabine inthe SINGLE trial.
SPRING-2 enrolled 822 participants to be randomlyallocated an INI, either RAL given 400 mg twice daily (BID)or DTG 50 mg once daily plus one of two co-formulated back-bones chosen at the investigators’ discretion: abacavir/lamivudine or tenofovir/emtricitabine [17]. Entry criteria weresimilar to those of the SINGLE trial including a viral load ofat least 1000 copies/ml. Baseline characteristics were similarto those of the SINGLE trial: most participants were men(86%) and white (85%). Median baseline HIV viral load wasapproximately 33,000 copies/ml in each group with 28% atleast greater than 100,000 copies/ml. The medianCD4 count was comparable in both arms (360 cells/µl). The48-week data were published in The Lancet in January2013 [17]. This showed that the DTG arm was non-inferiorto the RAL arm for the primary endpoint of viralload < 50 copies/ml at 48 weeks (361; 88% vs 351; 85%.Adjusted difference 2.5%; 95% CI: -2.2 to 7.1). The primaryendpoint was similar for patients with baseline viral loadsabove and below 100,000 copies/ml as well as for choiceof backbone in both arms. Of note, the choice of backbonewas similar in both arms, with 60% receiving tenofovir/emtricitabine and 40% abacavir/lamivudine. CD4 cell countsincreased in both groups by a median 230 cells/µl.
FLAMINGO, a multinational open-label trial, randomized484 ART-naıve patients to receive either DTG 50 mg oncedaily or ritonavir-boosted darunavir (DRV/r) 800/100 mgonce daily plus one of the two investigator-selected backbones:abacavir/lamivudine or tenofovir/emtricitabine. The 48-weekdata were presented at the 52nd Annual ICAAC meeting inDenver in September 2013 [18], and more recently at the14th European AIDS Conference in Brussels, Belgium [19].Although set up as a non-inferiority trial, the data showedthat DTG was superior to DRV/r for the primary endpointof viral load < 50 copies/ml at 48 weeks by snapshot analysis:90 versus 83% (adjusted difference 7.1%; 95% CI: 0.9 --13.2%; p = 0.025). These results were confirmed in per-protocol analysis: 91 versus 84%, respectively (difference:7.4%; 95% CI: 1.4 -- 13.3%), and particularly favored individ-uals with baseline HIV-RNA greater than 100,000 copies/ml(90 vs 70%). However, it is important to highlight that therewere an equal number of virologic failures in both arms.CD4 cell counts increased in both groups to week 48 by amedian 210 cells/µl. Two individuals in each arm (< 1% ineach arm) had protocol-defined virologic failure. The investi-gators suggested that DTG’s superiority reflected both its bet-ter tolerability and also a better response rate for participantswith baseline viral load greater than 100,000 copies/ml in the
Dolutegravir
Expert Opin. Pharmacother. (2014) 15(4) 575
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

DTG arm (proportion with viral load < 50 copies/ml at48 weeks: 93 vs 70%) [18,19].
4.2 Treatment-experienced patients4.2.1 Antiretroviral-experienced
integrase-inhibitor-naıveSAILING is a 48-week, Phase III, randomized, double-blind,active-controlled, non-inferiority study that evaluated safety,efficacy and emergent resistance in ART-experienced, INI-naive adults with HIV-1 with at least two-class drug resis-tance [20]. From Oct 2010 to Jan 2012, 1441 patients werescreened in 156 centers in 5 continents, of whom 724 wererandomly assigned (1:1) to DTG (50 mg once a day) orRAL (400 mg BID) plus up to two additional ARTs, with atleast one of them fully active. Seven hundred and nineteen par-ticipants were included in the intention-to-treat analysis(DTG, 357; RAL, 362). Sixty-eight percent of the study pop-ulations were male with a median age of 43 years and broaddiversity in ethnicity as well as HIV-1 subtypes due to thebroad geographical participation. Median (interquartile range)baseline plasma viral load and CD4+ cell counts were 4.18(3.45 -- 4.84) log10 copies/ml and 200 (95 -- 366) cells/µl,respectively, and around half had HIV advanced disease or ahistory of AIDS and resistance to at least one drug in each ofthree or more ART drug classes. The primary endpoint wasthe proportion of patients with plasma HIV-1 RNA < 50copies/ml at week 48 assessed with the US-FDA-defined snap-shot analysis, and the statistical analysis tested the superiorityof DTG if non-inferiority was established in both primary(all subjects who received at least one drug of study drug)and per-protocol analyses (excluding subjects with prespecifiedprotocol deviations).At week 48, 251 (71%) of 354 patients receiving DTG had
plasma HIV-1 RNA < 50 copies/ml versus 230 (64%) of361 patients receiving RAL, showing DTG non-inferiority(difference in proportions 7.4%, 95% CI: 0.7 -- 14.2). Statis-tical superiority (p = 0.03) was subsequently shown as part ofthe prespecified testing procedure. The increase of CD4+
T-cell count was 162 cells/µl in the DTG arm versus 153cells/µl through week 48. Virological failure was morefrequent in the RAL group 45 (12%) versus 21 (6%) in theDTG group by week 48 and earlier, and 19 of 45 virologicalfailures were nonresponders (plasma HIV-1 RNA decrease< 1 log10 copies per ml unless < 400 copies/ml by week16 or HIV-1 RNA ‡ 400 copies/ml on or after week 24) inthe RAL versus only 2 of 21 in the DTG group. For the sec-ondary endpoint, the proportion of patients harboring viruswith evidence of treatment-emergent genotypic resistancewas significantly lower in the DTG group (see Resistanceissues), 1% (4 of 354) compared with 5% (17/361) in theRAL group (adjusted difference -3.7%, 95% CI: -6.1 to-1.2, p = 0.003). The proportion of patients with resistanceto the background regimen was also greater in the RAL group(27 vs 19%, of the virological failures).
4.2.2 Antiretroviral-experienced RAL resistanceOn the basis of data of limited cross-resistance between DTGand first-generation INIs (RAL and EGV) shown fromin vitro studies [21,22], a Phase IIb study (VIKING study) wasconducted to assess the activity of DTG in HIV-1-infectedindividuals with RAL-resistant viral isolates [23]. Fifty-threeand 54 subjects were screened, of whom 27 and 24 subjectswere enrolled to compose the intention-to-treat of two cohorts:the 50-mg once-daily dose of DTG was first evaluated in a firstcohort (cohort I) of 27 participants who replaced RAL withDTG for 10 days in addition to their background therapy,none of which contained active drugs. However, followingthe assessment of the virological response of cohort I, a proto-col amendment was prompted and a second cohort of 24participants was evaluated, who received DTG 50 mg BID.Most participants were men with a median age of 48 years.According to the in vitro data of previous cross-resistancebetween DTG and RAL, subjects were allocated to two groupsin order to ensure a broad range of DTG sensitivity (unfortu-nately no analysis was done by these two groups): group1 included subjects with the worse DTG resistance profile(Q148H/K/R + ‡ 1 secondary RAL resistance mutations);and group 2 included subjects with a better DTG resistanceprofile (all other mutations, including codon 148 singlemutation).
Eighty-six percent of subjects (44 of 51) achieved the pri-
mary efficacy endpoint (plasma HIV-1 RNA load of
< 400 copies/ml or of ‡ 0.7 log10 copies/ml below the baseline
value on day 11): 78% of subjects (21 of 27) in cohort I and
96% of subjects (23 of 24) in cohort II. Subjects from cohort
II had a significantly larger reduction in HIV-1 RNA level
from baseline on day 11, compared with cohort I (mean
adjusted treatment difference, -0.32 log10 copies/ml;
-1.76 vs -1.45 log10 copies/ml; p = 0.017). At day 11, the start
of the second phase of the study, background therapy could be
optimized according to genotypic and phenotypic tests. That
was encouraged in cohort I but mandated for cohort II, such
that only one subject (4%) from cohort I, compared with
12 (44%), had an optimized background regimen phenotypic
susceptibility score of 0. At week 24, the response (viral
load £ 400 copies/ml) rate was greater in cohort II, 20 subjects
(83%) in contrast to 14 subjects (52%) in cohort I. The
increase of CD4+ T-cell count was similar in both cohorts
through week 24 (54 and 60 cells/µl for cohorts I and II,
respectively).Based on these findings, DTG 50mg twice-daily dosing was
chosen for VIKING-3, a Phase III, single-arm open-label
study, which assessed efficacy and safety of DTG through
24 weeks in treatment-experienced patients with ‡ 3 class resis-tance including INI resistance. One hundred and eighty-three
adults with screening HIV-1 RNA ‡ 500 copies/ml started
DTG 50 mg BID and continued their failing regimen (with-
out RAL/EVG). After 7 days of open-label DTG, background
drugs were optimized and DTG continued. There was a drop
J. L. Blanco Arevalo & G. G. Whitlock
576 Expert Opin. Pharmacother. (2014) 15(4)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

in mean HIV-1 RNA of an average 1.4 log after 7 days.
At week 24, 126 of 183 people (69%) had a viral load
< 50 copies/ml, and after 48 weeks of treatment, 64 of
114 (56%) had viral load < 50 copies/ml. There were 50 viro-
logic nonresponders (27%) at week 24 and 44 (39%) at week
48. DTG 50 mg BID was well tolerated despite advanced dis-
ease. In multivariate analyses of baseline factors on week
24 response rates, the presence of Q148 + ‡ 2 secondary IN
mutations and increasing DTG fold change (FC) were highly
correlated with fewer subjects achieving < 50 copies/ml
(p £ 0.001) but the optimized background regimen activity
score did not impact response [24].
5. Safety and tolerability
In the SINGLE study, insomnia was the only side effectreported more commonly in the DTG arm (15 vs 10%). Oth-erwise the most common side effects seen in the DTG armwere gastrointestinal and were found with comparable fre-quency in both arms (18% diarrhea; 14% nausea) [16]. Ten(2%) participants in the DTG arm stopped treatment before48 weeks due to side effects. This compares with 42 (10%)in the EFV/tenofovir/emtricitabine arm. As one might expect,nervous system and psychiatric disorders accounted for15 (4%) and 13 (3%) withdrawals in the EFV/tenofovir/emtricitabine arm, compared with none and 2 (< 1%), respec-tively, in the DTG arm. Two deaths were seen in the EFV/tenofovir/emtricitabine arm, both unrelated to the studydrugs. No deaths were seen in the DTG arm. In SPRING-2,the rates of side effects were similar in each arm, most com-monly nausea (14%), headache (12%), nasopharyngitis(11%) and diarrhea (11%) [17]. The rates of side effects leadingto discontinuation in each arm were also low (2%). The twodeaths, one in each arm, were unrelated to the study drugs.In the SAILING 48-week analysis, the most common adverseevent was diarrhea, seen in 20% in the DTG group and 18%in the RAL group [20]. Side effects leading to discontinuationwere also infrequent (3% DTG, 4% RAL). In FLAMINGO,there were fewer withdrawals due to adverse events withDTG compared with DRV/r (1 vs 4%). There was a lowerincidence of diarrhea with DTG (17 vs 29%) but greater inci-dence of headache (15 vs 10%). No serious adverse event wasreported in ‡ 1% of patients in any treatment group [19]. TheVIKING 24 week data showed that the proportion of partici-pants with serious adverse events was low (15 and 13%, respec-tively), none of which were considered related to DTG [23]. InVIKING-3, 6 of 183 people (3%) discontinued treatmentbecause of adverse events [24]. There were two serious drug-related adverse events -- hyperbilirubinemia, elevated ALT,and drug eruption in a patient taking DTG with ETV, andgrade 2 syncope in another patient.
In both SINGLE and SPRING-2, there were similar lowrates of renal adverse events (4 -- 5% in each arm) [25]. Increasesin serum creatinine were noted with DTG in SPRING-1,
SPRING-2, FLAMINGO, VIKING and SINGLE, whichoccurred early (by week 2) and were stable by week48 [15-17,23,25,19]. In SPRING-2, the mean change in creatinineclearance from baseline was -16.5 ml/min in the DTG armcompared with -5.4 ml/min in the RAL arm [17]. No changefrom baseline was seen in the urine albumin-to-creatinine ratioin either arm. There were no discontinuations to week 48 ineither group due to renal events. The mechanism is due toDTG-medicated inhibition of the organic cation transporterOCT2 which decreases tubular secretion of creatinine, thusincreasing serum creatinine without changing glomerular fil-tration. Hence, the changes in creatinine for DTG are notregarded as clinically significant although its long-term effectis still unknown.
From the week 96 data from SPRING-1, the mean changesin cholesterol were found to be lower in the DTG arm than inthe EFV arm [15]. In SPRING-2, there were no clinically sig-nificant changes over time in the fasting lipid profiles in eitherthe DTG or RAL arm [17].
In SPRING-2, hepatic adverse events also occurred at lowrates: 11 (1%) participants had increases in alanine amino-transferase greater than five times the upper limit of normaland met criteria to discontinue, 7 on DTG and 4 onRAL [17]. Of these, two patients in each arm had possibledrug-induced liver injury due to the INI prescribed. Ofnote, the entry criteria for the SPRING-2 trial excluded thosewith moderate or severe hepatic impairment.
DTG is a well-tolerated drug. The most common sideeffects are nausea, diarrhea and headaches, all seen at low rates(< 20%). In all studies, there is a low rate of discontinuationsdue to reported side effects. Laboratory-observed adverseevents are also infrequent. Although decreases are seen in cre-atinine clearance in all studies, these are not considered to beclinically significant.
6. Resistance issues
6.1 Resistance in vitro dataWith the exception of one report of transmitted INI resis-tance [26], fewer than 0.1% of INI-naıve individuals harborviruses with primary INI resistance mutations [27,28]. Sixty-five percent of the residues in the In gene, which are involvedin protein stability, multimerization, DNA binding and cata-lytic activity and in binding with the human cellular cofactorLEDGF/p75, are fully conserved [29]. From the most variablesites, the most prevalent polymorphic amino acid change atthese positions did not affect susceptibility to DTG in vitroor in vivo [30].
To date, few data have been generated with regard to themutations of resistance selected by DTG. In in vitro serial pas-sage studies, no highly resistance viruses have been selected;however, different INI mutations have been reported. In thefirst studies reported by Shionog &Co., Ltd, resistance passageassays up to day 112 with DTG showed only four substitutionsor combinations of substitutions (T124A, S153Y, T124A/S153Y
Dolutegravir
Expert Opin. Pharmacother. (2014) 15(4) 577
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

and L101Y/T124A/S153Y) [21,22]. These changes did not causean increase of > 4.1 in the DTG FC. These in vitro studies alsodemonstrated that the selection of resistant mutations from awild-type population was greatly delayed in a DTG-containing medium in contrast with that of first-generationINIs [30,31]. Another serial passage in vitro study reportedR263K as the first mutation most commonly selected, withouthomogeneity in the secondary mutation co-selected (G118R,S153Y, H51Y, E138K, V151I, M50I) [32].In vitro data have demonstrated that DTG retains substan-
tial activity against Y143 and N155H pathway virus withadditional secondary mutations and against virus withQ148 mutations alone [31]. There is a broader range of FCresistance against Q148 pathway virus according to the RALsecondary mutations; resistance generally increases withincreasing number of mutations, particularly when theseinclude G140S and/or E138K [31,32]. The main patterns ofcombined mutations associated with DTG resistance areQ148R or Q148H with additional substitutions includingT97A, E138K, G140S and M154I.
6.2 Resistance in ARV-naıve studiesLow rates of resistance were seen in SPRING-1,SPRING-2 and SINGLE. No IN or reverse transcriptase(RT) resistance was seen in the DTG arm of the SINGLEand FLAMINGO trials [16,19]. Of the virological failures inSPRING-1 and SPRING-2, no patients on DTG had theemergence of a virus with IN resistance mutations, and onlyone patient receiving DTG 10 mg developed virus with themutation M184M/V in RT (SPRING-1). In the RAL armof SPRING-2, one patient, whose baseline HIV viral loadwas greater than 3 million copies per ml, developed both INand nucleos(t)ide RT inhibitor resistance with a FC at viro-logical failure of 2.02 for DTG and 34 for RAL. Two addi-tional patients, one in each arm, at protocol-definedvirological failure but with no emergent genotypic resistancehad increased phenotypic resistance to RAL but not toDTG (SPRING-2).
6.3 Resistance in ARV-experienced studiesAt week 48, the proportion of patients in the SAILING studyharboring virus with evidence of treatment-emergent genotypicor phenotypic INI resistance was 1% (4 of 354) in the DTGgroup versus 5% (17 of 361) in the RAL group (adjusted differ-ence -3.7%, 95% CI: -6.1 to -1.2, p = 0.003). Of thesefour patients from the DTG arm, one had a RAL primary resis-tance mutation at baseline (Q148H/G140S). Two patientsselected IN substitutions at R263 position (R263R/K andV260I/R263K) and one with a polymorphic change at V151(V151V/I), all of themwithDTGor RAL FC of < two, suggest-ing no high-level resistance to both RAL and DTG. Viruseswith R263K and V260I/R263K site-directed mutants retaingood activity against DTG -- with lower than twofold changeIC50 for both RAL and DTG -- and a prolonged binding toIN enzyme (with half of the 3H-DTG retained for about
50 h) [33]. The proportion of patients with resistance to thebackground regimen was also greater for the RAL group(27 vs 19%, of the virological failures). Recently, an interestingpotential explanation for the relationship between the R263Kmutation and the absence of resistance mutations in ARTdrug-naive patients treated with DTG has been postulated inanother in vitro experiment. In that study, the combination ofmutations at positions R263K and H51Y shows a unique resis-tance pathway for DTG, where the secondary mutation H51Y,instead of compensating and restoring both enzymatic functionand viral fitness, the effect of the first substitution (R263K),which occurs most commonly [34], increases the level of resis-tance against DTG with a dramatic cost to both enzymaticactivity and viral replication that could explain the absence ofdetection of resistance mutations by the conventional assaysused for detecting drug resistance in the DTG clinical studiesin INI-naıve patients [35].
In VIKING, the baseline RAL FC was greater than themaximum concentration for all viruses, but, in contrast,DTG FC was higher for virus with mutations Q148 thanfor Y143 and N155H pathway viruses [22]. Seventy patientshad protocol-defined virologic failure through week 24,12 of 27 (44%) and 5 of 24 (21%) subjects in cohorts I andII, respectively. New INI genotypic resistance mutationsemerged after virological failure was observed in 7 subjects,4 of the 12 cohort I subjects and 3 of the 5 cohort II subjects.At virologic failure, all 7 subjects harbored ‡ 4 RALresistance-associated mutations, and 5 of the 7 subjects (2 incohort I; 3 in cohort II) had virus with Q148 + ‡ 1 RALresistance-associated mutation at screening or baseline. It isimportant to point out that in the VIKING study, 5 out of33 subjects (15%) with > 150 copies/ml at day 11 (after theend of the functional monotherapy phase) and with baselineIN mutations (4 of these 5 harbored viruses withQ148H + ‡ 1 secondary RAL resistance mutations) selectedadditional IN resistance mutations over the 10-day studyperiod. This datum suggests that, as with protease inhibitors,the apparent high genetic barrier of DTG in IN-naıvepatients, in which the selection of IN-genotypic resistancemutations after virological failure is very slow and uncom-mon, does not seem to demonstrate the same behavior inpatients with previous virological failure and selected muta-tions to INIs, where the selection of new IN mutations couldoccur at a faster rate.
In the VIKING-3 study, which examined the efficacy andsafety of DTG 50 mg BID in patients with resistance to multi-ple ARTs including INI, baseline IN genotypes and phenotypeswere assessed to identify correlates to virological response. Esti-mated DTG phenotypic cutoffs showed wide confidence inter-vals; however, for those patients with baseline DTG FC < 9.45,87% achieved full response (reduction > 1 log10 HIV RNA) atday 8, and 69% viral load < 50 copies/ml at week 24.No patientwith DTG FC > 9.45 reached < 50 copies/ml at week 24. Threebaseline genotypic resistance groups were identified based ontheir impact on DTG antiviral response i) No Q148
J. L. Blanco Arevalo & G. G. Whitlock
578 Expert Opin. Pharmacother. (2014) 15(4)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

(N155H, Y 143C/H/R, T66A, E92Q or historical IN resis-tance); ii) Q148 + 1 and iii) Q148 + ‡ 2 (secondary mutationsfromG140A/C/S, E138A/K/T, L74I)] and were used to assessresponse at week 24. Median decline in viral load at day 8 inlog10 HIV RNA were -1.65 (no Q148), -1.10 (Q148 + 1)and -0.74 (Q148 + ‡ 2); at week 24 the percentage of patientswith < 50 copies/ml in the three groups were 79% (noQ148), 45% (Q148 + 1), and 11% (Q148 + ‡ 2) [36].
7. Conclusions
DTG has been assessed in various clinical scenarios and com-pared with several ART drugs. In naive subjects, DTG 50 mgonce daily has demonstrated a favorable virological outcomecompared with EFV, driven by its better tolerability, andwith RAL, with lower risk of antiviral resistance to IN orNRTI following virological failure. More recently, DTG haseven shown superiority compared with DRV/r in the FLA-MINGO study, mainly driven by its better response in indi-viduals with baseline viral load greater than 100,000 copies/ml, but with equal number of virological failures in botharms. In treatment-experienced subjects who are INI naive,in combination with up to two other ART drugs, DTG50 mg once daily has shown higher virological efficacy thanRAL 400 mg BID with a lower selection of IN and NRTImutations. In treatment-experienced subjects with at leasttriple-class resistance including resistance to INIs, althoughDTG 50 mg BID with an optimized background therapy isat present being evaluated in an ongoing Phase III trial, exist-ing data show excellent virological response in subjects with agenotypic resistance profile different from Q148 + 2 or moresecondary mutations.
DTG has been generally well tolerated when administeredat either 50 mg once daily or 50 mg BID. The most commonside effects reported include nausea, headache, upper respira-tory tract infections and diarrhea. With regard to resistance,data to date show that DTG possesses a resistance profile dis-tinct from that of the first-generation INIs, retaining substan-tial activity against viruses harboring two of the three mainpathways of resistance selected after virological failure to thefirst-generation INIs, Y143 and N155H, and demonstrates ahigher genetic barrier than them, with uncommon and slowerselection of IN-genotypic resistance mutations after first INI-containing regimen virological failure, which may be due toits longer half-life and its slower dissociation from HIV-INcomplexes [37].
8. Expert opinion
DTG is the first of the second generation of IN strand-transfer inhibitors developed by Shionogi-ViiV Healthcareand Glaxo-SmithKlein. In similarity with the other drugsbelonging to this new class of INIs (RAL and EGV), DTGhas demonstrated potent anti-HIV activity with a similar orhigher decline in HIV-1 RNA after 10 days of monotherapy
compared with other ARTs. Its excellent PK, approximately15 h plasma half-life with low intersubject variability withoutpharmacokinetic boosters, and phamacodynamics, a troughconcentration for the 50 mg once daily dose around 25-foldabove the protein-adjusted IC90 for HIV-1 parameters,make DTG an appealing option in ART-naive patients withseveral advantages over the other INIs. Much like RAL,DTG has a very good tolerance and the same metabolic path-way through the UGT-1A1, as well as being a minor substratefor CYP. This explains its modest drug interaction profile andits small laboratory abnormality of total bilirubin increase.The advantages over RAL are its better pharmacokinetic pro-file and genetic barrier, and over EGV, its better drug--druginteractions profile because EGV is metabolized primarilyby CYP, as well as its genetic barrier.
Because of its favorable PK, pharmacodynamics, safety andtolerability profile, DTG is an extremely good candidate fori) a single-tablet regimen formulation (at present, under evalu-ation combined with abacavir 600 mg and lamivudine300 mg); ii) treatment in organ transplant recipients infectedby HIV-1; iii) post-exposure prophylaxis; iv) the elderly withor without co-morbidities or polypharmacy; and v) acuteHIV seroconversion where, due to very high viral loads, it isimportant that drugs have high ART potency and geneticbarrier.
The potential drawbacks of DTG are the changes in creat-inine levels, which, despite being modest and non-progressiveand without changing the glomerular filtration rate, may bean inconvenience in some subjects particularly when tenofoviris included in the regimen. DTG has a different resistanceprofile to other INIs. In data reported to date when DTG isused as the first INI, the selection of genotypic resistancemutations in IN is really uncommon. These data, alongwith the data in vitro, strongly suggest a high genetic barrierof this compound. However, it is important to highlightthat, to date, few patients with a virological failure to DTGas first INIs and only from clinical trials have so far beenreported and, on the other hand, genotypic resistance testingin those clinical trials were performed per protocol on theinitial viral load that rebounded not on the viral load fromthe virological failure confirmation 4 weeks later. In ART-experienced patients failing on a first-generation INI, fromthe three pathways of resistance more commonly selected(involving N155, Y143 and Q148 residues), the activity ofDTG is markedly diminished through Q148, especiallywhen is accompanied by two or three mutations (G140A/C/S, E138A/K/T, L74/I). With regard to the role of the combi-nation of Q148H + G140S substitutions -- the most frequentpathway associated with RAL failure -- in DTG resistance, it isimportant to highlight that, although this combination is notselected immediately at RAL or EGV virological failure, dueto their replicative advantages, variants harboring this combi-nation of mutations have a high selective advantage whenthere is persistent viral replication under first-generationINIs-containing regimen. That makes extremely important a
Dolutegravir
Expert Opin. Pharmacother. (2014) 15(4) 579
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.
prompt monitoring of genotypic resistance after virologicalfailure to avoid the potential evolution to this combinationof mutations associated with a greater reduction in DTG sus-ceptibility [38,39]. In our opinion, although the data availableto date point out that DTG has a high genetic barrier, perhapseven comparable to PI/r, we are still in the process ofevaluation of this area.DTG has shown to be an excellent option in treatment-
naive patients even in individuals with high baseline viralloads (25% of patients in the FLAMINGO study had baselineviral load greater than 100,000 copies/ml). It demonstrateseither noninferiority or superiority to its comparators (EFV,RAL, DRV/r). It has over one or more advantages in additionto them in terms of pill burden, the need for boosting, drug--drug interactions, side effects, cessations and selection of resis-tances. Because of its potential high genetic barrier, it could beconsidered as the best IN inhibitor for rescue therapy -- unlessthe combinations of changes at residues Q148 + G140 or
E138 are presented -- however, its excellent results in terms ofresistance with no cases of emergent resistance in patients whohad virologic failure do not limit its use in first-line therapyby not losing other ART options.
DTG is an extremely interesting agent with a wide range ofindications as ART therapy, due its high ART potency andfavorable tolerability, safety, drug--drug interactions andresistance profile.
Declaration of interest
JL Blanco Arevalo has received research funding, consultancyfees, travel expenses or lecture sponsorships from Abbott,Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead Sciences,Janssen-Cilag, Merck Sharp and Dohme, and ViiV Health-care. GG Whitlock has received travel expenses from Janssen-Cilag and ViiV Healthcare.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Espeseth AS, Felock P, Wolfe A, et al.
HIV-1 integrase inhibitors that compete
with the target DNA substrate define a
unique strand transfer conformation for
integrase. Proc Natl Acad Sci USA
2000;97:11244-9
2. Hare S, Gupta SS, Valkov E, et al.
Retroviral intasome assembly and
inhibition of DNA strand transfer.
Nature 2010;464:232-6
3. Alian A, Griner SL, Chiang V, et al.
Catalytically-active complex of HIV-1
integrase with a viral DNA substrate
binds anti-integrase drugs. Proc Natl
Acad Sci USA 2009;106:8192-7
4. McColl DJ, Chen X. Strand transfer
inhibitors of HIV-1 integrase: bringing
IN a new era of antiretroviral therapy.
Antiviral Res 2010;85:101-18
5. Mouscadet JF, Delelis O, Marcelin AG,
Tchertanov L. Resistance to HIV-1
integrase inhibitors: a structural
perspective. Drug Resist Updat
2010;13:139-50
6. Metifiot M, Marchand C, Maddali K,
Pommier Y. Resistance to integrase
inhibitors. Viruses 2010;2:1347-66
7. Min S, Song I, Borland J, et al.
Pharmacokinetics and safety of
S/GSK1349572, a next-generation HIV
integrase inhibitor in healthy volunteers.
Antimicrob Agents Chemother
2010;54:254-8
8. Cottrell M, Hadzic T, Kashuba A.
Clinical pharmacokinetic,
pharmacodynamic and drug-interaction
profile of the integrase inhibitor
dolutegravir. Clin Pharmacokinet
2013;52:981-94
. Complete review on pharmacokinetics
and main drug--drug interactions.
9. Min S, Sloan L, DeJesus E, et al.
Antiviral activity, safety, and
pharmacokinetics/pharmacodynamics of
dolutegravir as 10-day monotherapy in
HIV-1-infected adults. AIDS
2011;25:1737-45
10. Song I, Borland J, Shuguang C, et al.
Effect of food on the pharmacokinetics
of the integrase inhibitor dolutegravir.
Antimicrob Agents Chemother
2012;56(3):1627-9
11. Song I, Min SS, Borland J, et al. Lack of
interaction between the HIV integrase
inhibitor S/GSK1349572 and tenofovir
in healthy subjects. J Acquir Immune
Defic Syndr 2010;55:365-7
12. Song I, Borland J, Min S, et al. Effects
of etravirine alone and with ritonavir-
boosted protease inhibitors on the
pharmacokinetics of dolutegravir.
Antimicrob Agents Chemother
2011;55:3517-21
13. Song I, Mark S, Borland J, et al.
Dolutegravir has no effect on the
pharmacokinetics of methadone or oral
contraceptives with norgestimate and
ethinyl estradiol [abstract 535]. 20th
Conference on Retroviruses and
Opportunistic Infections; 3 -- 6 March
2013; Atlanta
14. Patel P, Song I, Borland J, et al.
Pharmacokinetics of the HIV integrase
inhibitor S/GSK1349572
co-administered with acid-reducing
agents and multivitamins in healthy
volunteers. J Antimicrob Chemother
2011;66:1567-72
15. Stellbrink H-J, Reynes J, Lazzarin A,
et al. Dolutegravir in antiretroviral-naive
adults with HIV-1: 96-week results from
a randomized dose-ranging study. AIDS
2013;27:1771-8
16. Walmsley S, Antela A, Clumeck N, et al.
Dolutegravir (DTG; S/GSK1349572) +
abacavir/lamivudine once daily statistically
superior to tenofovir/emtricitabine/
efavirenz: 48-week results -- SINGLE
(ING114467) [abstract H556b]. 52nd
Interscience Conference on Antimicrobial
Agents and Chemotherapy (ICAAC);
9 -- 12 September 2012; San Francisco
. This is an important study in
ARV-naıve patients that compared
ABC/3TC/DGV with Atripla�.
17. Raffi F, Rachlis A, Stellbrink H-J, et al.
Once-daily dolutegravir versus raltegravir in
antiretroviral-naıve adults with HIV-1
infection: 48 week results from the
randomized, double-blind, non-inferiority
SPRING-2 study. Lancet 2013;381:735-43
.. This is an important clinical trial with
a face to face of DTG with RAL in
ARV-naıve patients.
18. Feinberg J Clotet B, Khuong MA, et al.
Once--daily dolutegravir is superior to
J. L. Blanco Arevalo & G. G. Whitlock
580 Expert Opin. Pharmacother. (2014) 15(4)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.
darunavir/ritonavir in antiretroviral naıve
adults: 48 week results from
FLAMINGO (ING114915) [abstract
H-1464a]. 53rd Interscience Conference
on Antimicrobial Agents and
Chemotherapy (ICAAC);
10 -- 13 September 2013; Denver
19. Clotet B, Khuong MA, Antinori A, et al.
Once-daily dolutegravir versus darunavir/
ritonavir in antiretroviral naive adults:
48 week subgroup analyses from
FLAMINGO [abstract LBPS4/6].
Program and abstracts of the 14th
European AIDS Conference;
16 -- 19 October 2013; Brussels, Belgium
.. This is a very important clinical trial
that shows superiority over darunavir/
ritonavir using both NRTIs backbones.
20. Cahn P, Pozniak AL, Mingrone H, et al.
Dolutegravir versus raltegravir in
antiretroviral-experienced,
integrase-inhibitor-naive adults with
HIV: week 48 results from the
randomised, double-blind, non-inferiority
SAILING study. Lancet
2013;282(9893):700-8
.. Clinical trial that compares DTG with
RAL into rescue regimens in a
pretreated population INI-naıves.
21. Sato A, Seki T, Kobayashi M, et al. In
vitro passage of drug resistant HIV- 1
against a next generation integrase
inhibitor (INI), S/GSK1349572 [abstract
H-932]. 49th Annual Interscience
Conference on Antimicrobial Agents and
Chemotherapy Meeting; 12 -- 15
September 2009; San Francisco, CA
22. Seki T, Kobayashi M,
Wakasa-Morimoto C, et al.
S/GSK1349572 is a potent next generation
HIV integrase inhibitor and demonstrates
a superior resistance profile substantiated
with 60 integrase mutant molecular clones
[abstract 555]. 17th Conference on
Retroviruses and Opportunistic Infections;
16 -- 19 February 2010; San Francisco, CA
23. Eron JJ, Clotet B, Durant J, et al. Safety
and efficacy of dolutegravir in treatment-
experienced subjects with raltegravir-
resistant HIV type 1 infection: 24-week
results of the VIKING Study.
J Infect Dis 2013;207:740-8
24. Nichols G, Lazzarin A, Maggiolo F,
et al. Phase 3 assessment of dolutegravir
(DTG) 50 mg twice daily in
HIV-1-infected subjects with raltegravir
(RAL) and/or elvitegravir (EVG)
resistance in VIKING-3: week 24 results
of all 183 patients enrolled [abstract
TULBPE19]. 7th IAS Conference on
HIV Pathogenesis, Treatment and
Prevention; June 30--July 3 2013; Kuala
Lumpur
.. In this study DGV shows its activity in
heavily pre-treated patients with the
different IN resistance pathways.
25. Curtis L, Min S, Nichols G, et al.
Once-daily dolutegravir (DTG;
S/GSK1349572) has a renal safety profile
comparable to raltegravir (RAL) and
efavirenz in antiretroviral (ART)-naıve
adults: 48 week results from SPRING-2
(ING113086) and SINGLE
(ING114467) [abstract TUPE282]. 7th
IAS Conference on HIV Pathogenesis,
Treatment and Prevention; June 30 --
July 3 2013; Kuala Lumpur
26. Fransen S, Young B, Frantzell A, et al.
Control of viral replication following
transmission of HIV-1 exhibiting
resistance to reverse transcriptase,
protease, and integrase inhibitors
[abstract 56]. Antiviral Ther
2010;15(Suppl 2):A67
27. Varghese V, Liu TF, Rhee SY, et al.
HIV-1 integrase sequence variability in
antiretroviral naıve patients and in triple-
class experienced patients subsequently
treated with raltegravir. AIDS Res
Hum Retroviruses 2010;26:1323-6
28. Gutierrez C, Hernandez-Novoa B,
Perez-Elıas MJ, et al. Prevalence of
primary resistance mutations to integrase
inhibitors in treatment-naıve and -
experienced patients infected with B and
non-B HIV-1 variants. HIV Clin Trials
2013;14(1):10-16
29. Ceccherini-Silberstein F, Malet I,
D’Arrigo R, et al. Characterization and
structural analysis of HIV-1 integrase
conservation. AIDS Rev 2009;11:17-29
30. Vavro C, Hasan S, Madsen H, et al.
Prevalent polymorphisms in wild-type
HIV-1 integrase are unlikely to engender
drug resistance to dolutegravir
(S/GSK1349572).
Antimicrob Agents Chemother
2013;57:1379-84
31. Kobayashi M, Yoshinaga T, Seki T, et al.
In vitro antiretroviral properties of
S/GSK1349572, a next-generation HIV
integrase inhibitor.
Antimicrob Agents Chemother
2011;55:813-21
. In vitro study that explores the
pathways of escape to DTG and its
activity against different genotypic
resistance patterns selected by first
generations INIs.
32. Quashie PK, Mesplede T, Han YS, et al.
Characterization of the R263K mutation
in HIV-1 integrase that confers low-level
resistance to the second-generation
integrase strand transfer inhibitor
dolutegravir. J Virol 2012;86:2696-705
. In vitro study that explores the
pathways of escape to DTG.
33. Underwood MR, Dudas K, Horton J,
et al. Analysis and characterization of
treatment-emergent resistance in
ART-experienced, integrase inhibitor-
naive subjects with dolutegravir (DTG)
vs raltegravir (RAL) in SAILING
(ING111762) [abstract 21]. International
Workshop on HIV &hepatitis virus drug
resistance and curative strategies;
4 -- 8 June 2013; Toronto, ON, Canada
34. Quinones-Mateu ME,
Moore-Dudley DM, Jegede O, et al.
Viral drug resistance and fitness.
Adv Pharmacol 2008;56:257-96
35. Mesplede T, Quashie PK, Osman N,
et al. Viral fitness cost prevents HIV-1
from evading dolutegravir drug pressure.
Retrovirology 2013;10:22
. That study suggests an interesting
explanation about the lack of
genotypic resistance mutations after
first DTG virologic failure.
36. Vavro CL, Huang J, Underwood MR,
et al. Integrase genotypic and phenotypic
predictors of antiviral response to
dolutegravir (DTG) in subjects with
resistance to integrase inhibitors (INIs)
[abstract 29]. International Workshop on
HIV & hepatitis virus drug resistance
and curative strategies; 4 -- 8 June 2013;
Toronto, ON, Canada
37. Hightower KE, Wang R, Deanda F,
et al. Dolutegravir (S/GSK1349572)
exhibits significantly slower dissociation
than raltegravir and elvitegravir from
wild-type and integrase inhibitor-resistant
HIV-1 integrase-DNA complexes.
Antimicrob Agents Chemother
2011;55:4552-9
38. Canducci F, Ceresola ER, Boeri E, et al.
Cross-resistance profile of the novel
integrase inhibitor Dolutegravir
(S/GSK1349572) using clonal viral
variants selected in patients failing
raltegravir. J Infect Dis
2011;204:1811-15
Dolutegravir
Expert Opin. Pharmacother. (2014) 15(4) 581
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.

39. Abram ME, Hluhanich RM,
Goodman DD, et al. Impact of primary
elvitegravir resistance-associated
mutations in HIV-1 integrase on drug
susceptibility and viral replication fitness.
Antimicrob Agents Chemother
2013;57:2654-63
AffiliationJose Luis Blanco Arevalo†1 MD &
Gary George Whitlock2 MD†Author for correspondence1University of Barcelona, IDIBAPS,
Hospital Clinic, Barcelona, Spain
E-mail: [email protected] London Hospital,
Barts Health NHS Trust,
London, UK
J. L. Blanco Arevalo & G. G. Whitlock
582 Expert Opin. Pharmacother. (2014) 15(4)
Exp
ert O
pin.
Pha
rmac
othe
r. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y O
ndok
uz M
ayis
Uni
v. o
n 11
/11/
14Fo
r pe
rson
al u
se o
nly.





























