Embed Size (px)
Citation preview

PLUTO First report
The PLUTO is a registry developed by aninternational collaboration of the Liver TumorsStrategy Group (SIOPEL) of the SIOP. Thisregistry establishes a multicenter, multi-institu-tional cooperative database with prospectiveregistration of pediatric patients (<18 yr) whoreceive a liver transplant for treatment of aprimary malignant liver tumor. Liver tumors ofchildhood that require liver transplant whenunresectable by conventional surgical resectioninclude HB, HCC, HEHE, and other rare tumorsincluding undifferentiated, embryonal andrhabdoid sarcomas, and angiosarcoma. Accessto the registry is with a remote data entry system,accessible online and worldwide (http://pluto.cineca.org) (Fig. 1).The existing single institution and multicenter
reviews of transplant for liver tumors in childrenhave shown improving results over the pastdecade. The published studies are almost uni-formly limited by small numbers of patientsand selection and reporting bias because of their
retrospective nature and lack of strict inclusionand exclusion criteria (1). If our pediatric oncol-ogy and transplantation community is ever goingto establish standard recommendations, we needto base them upon solid class outcome data. Thiswill require that we prospectively and collectivelyexamine a large number of patients over adefined time period and rigourously examinetreatment variations and outcomes. The Obser-vatory aims to achieve this goal by fully defining(i) the role of liver transplantation performedeither primarily or as a rescue for relapse afterincomplete resection, (ii) the optimal timing ofliver transplantation, (iii) the potential role ofneoadjuvant and adjuvant chemotherapy, and(iv) the best strategy for post-transplant immu-nosuppression. The PRETEXT of disease is asystem that objectively defines the extent ofthe tumor within the liver (2). PRETEXT hasbeen used for many years as a risk stratificationsystem by SIOPEL (3). It has also more recentlybeen used as a tool to define surgical resectabilityby both SIOPEL and COG. In this manner,PRETEXT can be used to identify, at diagnosis,which tumors might most benefit from a livertransplant as a surgical resection strategy(4). The PLUTO registry carefully recordsthe PRETEXT grouping at diagnosis and attransplantation of all patients entered into the
Otte J-B, Meyers R. PLUTO First report.Pediatr Transplantation 2010. � 2010 JohnWiley & Sons A/S.
Abstract: The PLUTO is a registry developed by an international col-laboration of the Liver Tumors Strategy Group (SIOPEL) of the SIOP.Although the number of patients collected in PLUTO to date is toosmall to add any analytic power to the existing literature, this newregistry has great promise. It has been created to clarify issues regardingthe role of liver transplantation in the treatment of children withunresectable liver tumors. By reviewing the results to date, we hope wecan motivate more centers to participate, enroll patients, complete dataentry, and boost the potential impact of the collaborative effort. Toachieve this goal, a large number of patients are needed, which requiresan intensified international collaboration. Pediatric oncologists,pediatric surgical oncologists, and pediatric liver transplant surgeonsare all encouraged to participate and contribute. This is a preliminaryglimpse of what we hope to be a series of interim reports over thenext decade from the steering committee to help guide therapy in thisvery challenging group of children.
Jean-Bernard Otte1 and RebeckaMeyers2
1Universit� Catholique de Louvain, CliniquesSaint-Luc, Brussels, Belgium, 2University of Utah,Salt Lake City, UT, USA
Key words: liver tumors – transplantation – children– international registry
Jean-Bernard Otte, Transplanation Surgery, Universit�Catholique de Louvain, Cliniques Saint-Luc, avehippocrate 10, Brussels 1200, BelgiumTel.: 0032478785328Fax: 003227820866E-mail: [email protected] behalf of the steering committee: P. Chapchap,L. d�Antiga, J. de Ville de Goyet, F. Gennari, Y. Inomata,P. Kalicinsli, M. Kasahara, S. McDiarmid, R. Meyers, G.Perilongo, D. Roebuck, D. von Schweinitz, A.Zimmerman.
Accepted for publication 30 June 2010
Abbreviations: COG, Children�s Oncology Group; HB,hepatoblastoma; HCC, hepatocellular carcinoma; HEHE,hepatic epithelioid hemangioendothelioma; IRB, institu-tional review board; PLUTO, Pediatric Liver UnresectableTumor Observatory; PRETEXT, PREtreatment EXTent;SIOP, Societe Internationale d�Oncologie Pediatrique.
Pediatr Transplantation 2010 � 2010 John Wiley & Sons A/S.
Pediatric TransplantationDOI: 10.1111/j.1399-3046.2010.01395.x
1

registry. Specific data regarding chemotherapyand immunosuppression are collected in anattempt to define best practices and possibleundesired interactions. Additional variables spe-cifically examined include histologic subtype,vascular invasion (including either gross ormicroscopic invasion), metastases, and the mul-tifocality, size, and number of nodules of thetumor. This last examination of size and numberof nodules will help us determine if the MilanCriteria originally developed for adults withHCC are applicable or appropriate for use inchildren. Recent data suggest that these Milancriteria require modification for use in children,and the PLUTO outcome data will help usdetermine an outcome based on an appropriateset of criteria for children (5).Published results for the most rare tumor types
like hemangioendothelioma, embryonal sar-coma, undifferentiated sarcoma, and angiosarco-ma are anecdotal at best. A collective registry ofoutcomes for the most rare tumor types will helpset best practice transplant criteria and defineoutcomes.
Methods
During a meeting in 2004, the SIOPEL group ascertainedthat the role of liver transplantation in the treatment ofprimary, malignant liver tumors could not be clarified onthe basis of retrospective studies and publications. Thecreation of an international registry was suggested for theprospective collection of pediatric patients. The first authorwas entrusted with the task of developing a web site with thetechnical assistance of CINECA, which is a non-profitNational Institute of Oceanography and ExperimentalGeophysics, the National Research Council, and the Min-istry of Education, University and Research. Cineca islocated in Bologna, Italy and operates in the technologicaltransfer sector through high-performance scientific com-puting, the management and development of networksand web-based services, and the development of complexinformation systems for treating large amounts of data.It offers support to the research activities of the scientificcommunity through supercomputing and its applications.Several work sessions in Bologna, during 2005 and early2006, were devoted to identification of relevant items,setting up of the datasheets and data entry system at Cineca,and design of the web site (http://pluto.cineca.org).An international steering committee was set up, includingrepresentatives of SIOPEL, the COG Liver TumorSubcommittee, The German Cooperative Pediatric LiverTumor Study Group, the SPLIT registry, the ItalianAssociation of Pediatric Hematology and Oncology andrepresentatives of Easter Europe, South America, and Asia;consultants were included from radiology and pathology.The design and the content of the web site were discussedand approved by the steering committee. Great attentionwas paid to the ethical aspects. The project was approvedby the Bio-Medical Ethics Committee of the UniversiteCatholique de Louvain, Belgium (home university of thefirst author). Centers and colleagues willing to contribute
were suggested to request an ID and password. The chal-lenge of obtaining approval by the local ethics committee orIRB was the task of individual contributors. PLUTO waslaunched in 2006 for children <18 yr transplanted fromJanuary first onward.
Results
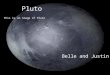
This first interim analysis of the PLUTO dataincludes patients entered between January 2006and April 2009. The dataset to date includesregistration of 36 centers in 17 countries. Not allregistered centers have completed patient dataentry because of several reasons including chal-lenges meeting institutional ethics and IRB reviewprocesses. Seventeen of the 36 registered centershave enrolled 70 patients. Of the 70 patients, dataentry is complete in 52 cases (Table 1). The largestnumbers of patients have been enrolled by BuenosAires (n = 13) and Pittsburgh (n = 11). In thisinterim analysis, the results are expressed inpercentage of available data for each variable asnot all patients had a complete dataset. The mostcompelling observations are as follows: indicationfor transplant was HB in 70% (n:49), HCC in23% (n:16), and rare tumor in 7% (hemangioen-dothelioma = 2; HEHE = 1; embryonal sar-coma = 1; and rhabdoid sarcoma = 1). Age attransplant was £ 10 yr in 90%. Age at transplantwas 1–10 yr (Fig. 2), with 93% and 7% primaryand rescue transplants, respectively. Neoadjuvantchemotherapy was received by 83% of patientsand adjuvant chemotherapy by 40%. PRETEXTat diagnosis was downstaged by one group afterneoadjuvant chemotherapy in 20% of PRETEXTIII tumors (downstaged from a diagnosis PRE-TEXT III to a post-chemotherapy and pretrans-plant POST-TEXT II) and 50% of PRETEXT IVtumors (downstaged from a diagnosis PRETEXTIV to a post-chemotherapy and pretransplantPOST-TEXT III). Arterial, portal, and biliarycomplications were reported in 12%, 7%, and26%, respectively. Kaplan–Meier overall survivalestimate at three yr after diagnosis was 87% forHB and 85% for HCC (Figs. 3 and 4). Of fourpatients who received a rescue transplant for HB,
Table 1. Countries contributing to PLUTO as of April 2009
Countriesparticipating
Registeredcenters/havingenrolled patients
Enrolledpatients
Patients withfilled forms
Europe 10 16/9 33 20N. America 2 9/2 13 11S. America 3 3/2 14 13Asia 2 4/4 10 8Australia 2/0 – –Total 17 34/17 70 52
Otte and Meyers
2

one is alive and well, one is alive with relapse, onedied from relapse, and the outcome of the lastpatient is unknown. One child who received arescue transplant for HCC is alive and well.Extrahepatic recurrence occurred in six patientswith HB (12.2%); three died and three were aliveat last follow-up. Recurrence occurred in fourpatients withHCC (25%); one died from infectionand three were alive at last follow-up. Recurrenceoccurred in one patient with hemangioendotheli-oma, alive at last follow-up. In total, five of 49patients with HB (10%) died (three from recur-rence, one from chronic rejection, and one fromportal thrombosis). One of 16 patients with HCCdied (6%) from infection. Six patients with HBpresented with lung metastases (1 PRETEXT IIIand 5 PRETEXT IV). All cleared their lungs withpretransplant chemotherapy and underwent a
successful transplant. One relapsed three monthsafter transplant and died seven months later.The remaining five were alive five, eight, 23, 24,and 25 months post-transplant, at last follow-up.No registered patients have had a pretransplantthoracotomy to resect metastatic tumor.
Discussion
This manuscript presents a preliminary interimanalysis of 70 patients enrolled over the firstthree yr of the registry between January 2006 andApril 2009.This cohort was recruited through interna-
tional collaboration and remains limited by theinability of more than half of the registeredcenters to fill all sheets due, partly, to difficultiesof completing the necessary approvals for patient
Patients distribution by age
35
20
25
30
ses
10
15
20
N. o
f ca
0
5
<1 year 1.1 — 3 3.1 — 10 >10.1
Years
Fig. 2. Age distribution.
Fig. 1. PLUTO home page.
Registry Report
3

entry and registration. The limited number ofpatients with completed forms and follow-uprestricts the impact of this preliminary study.Epidemiology data, prevalence of HB and HCC,survival rates, and surgical complications aresimilar to previously published single or multi-center studies. Only five children transplantedfor a rare tumor were enrolled; this type ofindication, including HEHE (6), remains verycontroversial; a prospective, international regis-
try will be particularly helpful in this area.Although downstaging after pretransplant che-motherapy was observed in 20% of PRETEXTIII and 50% of PRETEXT IV, we may assumethat liver transplantation remained indicatedbecause invasion of major venous tributariesprecluded a radical resection with conventionalsurgery. Although follow-up is still short, dis-ease-free survival was observed in five of sixpatients with HB and lung metastases at presen-
1.00
Kaplan—Meier survival estimate from diagnosis-HB
.75 0.87
0.0.
500.
250.
00
0 1000 2000 3000 4000
Days
Fig. 3. Kaplan–Meier estimate survival from diagnosis of patients with HB.
1.00
Kaplan–Meier survival estimate from diagnosis-HCC
75
0.888
00.
500.
250.
00
0 500 1000
..
1500
Days
Fig. 4. Kaplan-Meier estimate survival from diagnosis of patients with HCC.
Otte and Meyers
4

tation, which had cleared after chemotherapy;this is in line with previous observations (7).Recurrence rate was high in HCC (25%)
although three patients remained alive at lastfollow-up, while one died because of infection;we may expect 100% mortality with furtherfollow-up. Three patients with recurrent HBdied, while three more were alive at last follow-up; survival may be expected in some of them ifthe recurrence responds to chemotherapy. Sur-prisingly, 17% of patients did not receive neo-adjuvant chemotherapy before transplantation,while 60% did not receive chemotherapy post-transplant. This observation underlines thenecessity to standardize the chemotherapy inpatients needing a transplant, which shouldfollow the same protocols as in children treatedby conventional surgery, with the same amountof courses before and after surgery.The items collected in the PLUTO database
will eventually enable us to make a number ofspecific treatment recommendations once we haveachieved a larger recruitment and the databaseoutcome matures. We continue to solicit andencourage collaboration of all pediatric livertransplant centers worldwide. Although partici-pation to date is encouraging, it can and shouldgrow substantially over the next several years. Ascenters who have volunteered a casual willingnessto collaborate begin to see the benefits of such alarge collaborative database, these early interimresults should help to drive increasing participa-tion. Particularly in the United States, the ethicsand IRB process necessary to begin enrollingpatients have been a significant roadblock. Thischallenge is partially addressed as we move intothe future by inclusion of the PLUTO IRBprocess as an integral part of the new COG studyof HB. We regret the deficit of collaboration inAsian countries and in some of the largestEuropean countries; this will be a goal for futurecollaboration and enrollment.Despite the user-friendly construction of the
PLUTO web site, enrolling patients requiresmotivation based on a common concern aboutthe need to improve the care of children withunresectable primary liver malignancies; theprocess may appear as time consuming butexperience shows that it becomes expeditiouswhen data from a single patient are put together.The PLUTO data are the asset of centers
contributing patients; therefore, they are avail-able to collaborating centers for performingscientific studies that should preferably lead toa publication in a peer-reviewed journal. Regu-lations for scientific studies and publicationshave been established (Appendix).
Conclusion
Although the number of patients collected inPLUTO to date is too small to add any analyticpower to the existing literature, this new registryhas great promise. It has been created to clarifyissues regarding the role of liver transplantationin the treatment of children with unresectableliver tumors. By reviewing the results to date, wehope we can motivate more centers to participate,enroll patients, complete data entry, and boostthe potential impact of the collaborative effort.To achieve this goal, a large number of patientsare needed, which requires an intensified inter-national collaboration. Pediatric oncologists,pediatric surgical oncologists, and pediatric livertransplant surgeons are all encouraged to partic-ipate and contribute. This is a preliminaryglimpse of what we hope to be a series of interimreports over the next decade from the steeringcommittee to help guide therapy in this verychallenging group of children.
Acknowledgments
The professionalism and the efficient collaboration ofCINECA (A. Covezzoli, who extracted the data, and M.Derosa) are acknowledged. We are grateful to SIOPEL,IPTA, and Astellas for their support.
Appendix
Regulations for PLUTO-based studies and publications
The PLUTO data are available to scientists/clinicians whosecenters regularly contribute to PLUTO. Data can be used toperform scientific studies, which should preferably lead to apublication in a peer-reviewed journal.
Access to the data
To obtain access to the data, a written request should beaddressed to the chairperson of the PLUTO SteeringCommittee serving as custodian of the registry with copy tothe chairperson of the SIOPEL group. Decision to releasethe data should be agreed by both.The request should contain:
1 Title, objectives, and description of the study2 Name and affiliation of the investigator(s)3 Supporting letter by the program director4 The list of data to be extracted from the PLUTO database5 A disclosure statement regarding potential conflicts of
interest (such as financial affiliations with pharmaceuticalcompanies)
The data will be extracted from the PLUTO database by acollaborator from CINECA.The statistical analysis will be performed by the investi-
gator and his team; however, it needs to be checked by theSIOPEL group biostatistician.In case the requested data are not completely available
through the PLUTO database, it is allowed to approach
Registry Report
5

centers contributing patients to PLUTO for additional data.A request to the centers should be cosigned by theinvestigator and the chairperson of the PLUTO steeringcommittee.
Publications
The results of the study should be submitted to the chair-person of the PLUTO steering committee who will consultwith other members of the steering committee, dependingon specific issue(s) of the study (e.g., surgical aspects oftransplantation, immunosuppression, chemotherapy…).The investigator will receive the green light for pursuing the
writing of the intended oral presentation (and abstract) and/or the publication. The content will be submitted for finalapproval to the chairperson of the PLUTO steering com-mittee and the other members involved. Full publicationsonly (this rule does not apply to abstracts and oral/postercommunications) should be submitted to the SIOPELPublication Committee before their final release. All centersthat have participated in the study will be listed in a footnoteor an appendix, mentioning the program director. Thecontribution of CINECA will be acknowledged. The choiceof the journal is made in agreement with the chairperson ofthe SIOPEL group and the chairperson of the PLUTOsteering committee.
Authorship
Authorship of any publication based on PLUTO data(abstract or full paper) is regulated as follows: First and lastauthorship for those performing the study.Second and third authorship for the members of the
steering committee who have supervised the study. As manyauthors as possible (this means as allowed by the journal), ingeneral, one per center, according to the number of patients
included in the study. After the last author, the statement‘‘for the PLUTO steering committee’’ should be included,and ‘‘for the SIOPEL group,’’ as well, if appropriate. Allcenters that have participated with patients in the study willbe listed in a footnote or an appendix, mentioning theprogram director.
References
1. Otte JB, Aronson DC, Brown J Liver transplantation for he-
patoblastoma: Results from the International Society of Pediatric
Oncology (SIOP) Study SIOPEL-1 and review of the world
experience. Pediatr Blood Cancer 2004: 42: 74–83.
2. Roebuck DJ, Aronson D, Clapuyt P, et al. 2005 PRETEXT: A
revised staging system for primary malignant liver tumors of
childhood. Pediatr Radiol 2007: 37: 123–132.
3. Aronson DC, Schnater JM, Staalman CR, et al. The predictive
value of the PREtreatment EXTent of disease (PRETEXT) system
inhepatoblastoma-Results of the International Society of Pediatric
Oncology Tumor StudyGroup (SIOPEL-1). J ClinOncol 2005: 23:
1245–1252.
4. Otte JB, Meyers R. Correspondance regarding PLUTO.
J Pediatr Surg 2006: 41: 607–608.
5. Otte JB. Should the selection of children with hepatocellular
carcinoma be based on Milan criteria? Pediatr Transplant 2008:
12: 1–3.
6. Otte JB, Zimmerman A. The role of liver transplantation for the
treatment of pediatric epithelioid hemangioendothelioma. Pediatr
Transplant 2010: 14: 295–297.
7. Perilongo G, Brown J, Shafford E, et al. Hepatoblastoma
presenting with lung metastases: Treatment results of the first
cooperative, prospective study of the International Society of
Paediatric Oncology on childhood liver tumours. Cancer 2000:
89: 1845–1853.
Otte and Meyers
6