Embed Size (px)
Citation preview

1349
Occasional Surveys
DO YOUNG PATIENTS WITH DYSPEPSIANEED INVESTIGATION?
B. WILLIAMS
J. H. M. ELLINGHAMM. LUCKASA. DAIN
A. C. B. WICKS
Leicester General Hospital, Gwendolen Road, Leicester LE5 4PW
Summary During 1986, 1386 patients with simpledyspepsia were referred by general
practitioners for endoscopy (686) or double-contrast bariummeal examination (700) at Leicester General Hospital. 618(45%) were under the age of 45 years. Abnormal findingswere more common in older than younger dyspepticpatients (58% vs 40% at endoscopy, 69% vs 25% by bariummeal). Malignant disorders were diagnosed in 5% at
endoscopy and 3% at barium meal, but in no patient under45 years old. The incidence of malignant disorders at
endoscopy was analysed for the 6 years 1980-86. Of 707cases identified, only 13 (1·8%) occurred in patients under45 years old; all 13 had symptoms suggesting pathologymore serious than simple dyspepsia. It can be concludedthat young patients with simple dyspepsia are
overinvestigated. A majority can be treated safely withantacids and/or histamine receptor type 2 antagonists.
INTRODUCTION
THE symptom of dyspepsia is a common reason forconsultation in general practice and one of the main reasonsfor referral to hospital gastroenterology services.1,2 The
management of dyspepsia has been revolutionised in thepast decade by two major advances-the development offibreoptic upper gastrointestinal endoscopy, now
considered the investigation of choice and the gold standardfor diagnosis of the range of pathologies underlyingdyspeptic symptoms,3.4 and the development of specifichistamine receptor type 2 antagonists (H2RA) to become asafe and effective treatment for most of these pathologies.
Greater availability and awareness of the various
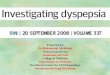
applications of upper gastrointestinal endoscopy have led tomany requests to investigate patients with a wide range ofupper gastrointestinal symptoms. Many of these patientswould have been adequately treated before the advent ofendoscopy without investigation. The escalation in demandfor endoscopy has been dramatic. In 1976, 990 endoscopieswere carried out for the whole Leicester catchment area of850 000 people; by 1986 this total had risen to over 6000.Leicester General Hospital’s endoscopy service hasfunctioned at full capacity for the past 3 years and like manyothers nationwide has reached a saturation point (fig 1). Atthis point, the demand continues to escalate but since thefunctional capacity of the service is restricted, the inevitableconsequence is ever-increasing waiting lists. Within thisframework of open-access endoscopy, patients with earlysinister pathology, who need prompt evaluation and
treatment, will wait as long as those with benign disease orfunctional dyspepsia. A more critical approach is needed tostratify endoscopy waiting lists more appropriately and toreduce the number of unnecessary investigations.
It is our clinical impression that the investigation ofyounger patients with dyspepsia rarely influences their
management and the majority could be adequately treatedsymptomatically in the first instance. Furthermore, few
Fig 1-Number of upper gastrointestinal endoscopic examinationsper year at Leicester General Hospital.
studies have selectively analysed young patients with
dyspepsia and, in those which have, the numbers reviewedhave been small.5,6 We have reviewed the results of allexaminations (double-contrast barium meal and uppergastrointestinal endoscopy) carried out at Leicester GeneralHospital to investigate dyspeptic patients at the request ofgeneral practitioners during 1986. The incidence and natureof pathologies in the younger (under 45 years) and olderdyspeptic patients were compared. To assess whether theempirical symptomatic treatment of young dyspepticpatients may delay the diagnosis of early gastric cancer, anage-stratified review of all gastric malignant disorders
diagnosed endoscopically at the Leicester teaching hospitalsduring the 1980s was carried out.
METHOD
Leicester General Hospital is one of three major hospitalsforming the Leicester teaching group which serve a population ofapproximately 850 000. This study retrospectively analysed theresults of all upper gastrointestinal endoscopic examinations anddouble-contrast barium meal radiological examinations carried outat the hospital in 1986, on dyspeptic patients referred by generalpractitioners.A precise definition of dyspepsia is difficult. For the purposes of
this study it was used to describe symptoms thought likely to beemanating from pathology in the upper gastrointestinal tract,
excluding patients with dysphagia or upper gastrointestinalhaemorrhage.The number of gastric malignant disorders diagnosed in a single
year was likely to have been small and possibly not representative ofprevious years. Therefore, we analysed the age and sex distributionsof all patients with gastric malignant disorders proved by biopsydiagnosed at any of the hospitals in the Leicester teaching groupduring a 6-year period (1980-1986).The endoscopic examinations were carried out by experienced
operators using ’Olympus P2 or Q’ endoscopes. The double-contrast barium meal examinations were reported by a singleexperienced radiologist.
TABLE I-ENDOSCOPIC AND BARIUM MEAL FINDINGS IN PATIENTS
WITH SIMPLE DYSPEPSIA

1350
TABLE II-SYMPTOMS ASSOCIATED WITH PRESENCE OF ABNORMAL
FINDINGS AT ENDOSCOPY
RESULTS
During 1986, 2872 endoscopies were carried out atLeicester General Hospital; of these, 686 were for patientswith symptoms of dyspepsia referred by generalpractitioners. Of the general practitioner referrals, 415(60%) were male and 271 (40%) were younger than 45years. The endoscopic findings are shown in table I.
Oesophageal disease and peptic ulceration were morecommon findings in the older group, gastritis andduodenitis occurred with similar frequency in both agegroups, and oesophageal and gastric carcinoma were
confined to the older age group. Overall, abnormal
endoscopic findings were more common in the older group(58% vs 40%). The most important symptoms associatedwith the presence of pathology in all 686 patients are shownin table II.
During 1986, 700 double-contrast barium meals wererequested by general practitioners to investigate their
dyspeptic patients (table I). There was also a male
predominance in this group (65%) and a majority of thoseinvestigated (57%) were under the age of 45 years. Theresults were similar to those of the endoscopy group, with amuch higher percentage of abnormal fmdings in the olderthan the younger patients (69% vs 25%). Oesophagealdisorders and peptic ulceration were more common findingsin the older patients and no carcinomas were reported in theyounger patients. Interestingly, the numbers of patients inthe endoscopy and barium meal groups were similar.
However, although only 40% of patients in the endoscopygroup were younger than 45 years, 57% of the double-
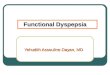
Fig 2-Age stratification of 707 patients with histologically provenneoplasia at Leicester teaching hospitals, 1980-86.
LJ = male patients; S = female patients.
TABLE III-PRESENTING FEATURES OF PATIENTS AGED 45 YEARSWITH ENDOSCOPICALLY PROVEN GASTRIC NEOPLASIA
GIH = gastrointestinal haemorrhage.
contrast barium meal group were under that age. This
finding suggests that the barium meal is favoured by generalpractitioners for investigation of young patients with
dyspepsia. The overall detection of pathology was muchhigher in the older patients whatever the means of
investigation. The detection of malignant disorders by thetotal of 1386 examinations was low (3% barium meal, 5%endoscopy). No malignant disorders were detected in
patients under 45 years. To quantify the incidence moreprecisely, the age and sex distributions of all gastricmalignant disorders diagnosed in the three hospitals of theLeicester teaching group during 1980-86 were analysed (fig2). There was a male predominance, and only 13 of the 707patients (1-8%) were younger than 45 years (11adenocarcinoma, 1 undifferentiated carcinoma, 1 malignantcarcinoid). The presenting symptoms of these patients arelisted in table III.
DISCUSSION
Many practitioners treat simple dyspepsia with variousantacid preparations or H2RAs, particularly in their
younger patients. Standard teaching practice demands afirm pathological diagnosis before a dyspeptic patient isgiven H2RA therapy, partly because of the cost implicationsof "blind" use of expensive drugs but, more importantly,because of the concern that in some patients these drugs willprovide symptomatic relief of an underlying carcinoma,thereby delaying diagnosis. Along with others/,8 we believethat this concern is exaggerated, particularly for youngerpatients.
In this study, the overall incidence of pathology was muchlower in younger than older dyspeptic patients, and during1986 no patient under 45 years was found to have a
malignant disorder to account for his or her symptoms. Inthe retrospective study of gastric malignant disorders in thethree Leicester hospitals, there was a very low incidence inpatients under 45 years (less than 2%). However, 56% ofendoscopic diagnostic services were directed at detectingthese cases, even though the prognosis for gastric malignantdisorders is not strongly dependent on the age of the patientat diagnosis. Furthermore, most gastric malignant disordersdiagnosed endoscopically are advanced and there is littleevidence that endoscopy has either shortened the time todiagnosis or improved the prognosis.9An important small group that would benefit from early
diagnosis is patients with early gastric cancer. To put thisdisorder in perspective, only 4 cases of early gastric cancerhave been diagnosed at Leicester General Hospital after 8years and 16 000 endoscopies. This group assumes

1351
importance, however, because the prognosis for early gastriccancer is very much better than that for advanced disease.
Preliminary reports from the early gastric cancer/dysplasiasurvey conducted by the British Society of
Gastroenterology have emphasised that prompt diagnosisand treatment of early gastric cancer can result in more than85% 5-year survival, compared with almost 100% 1-yearmortality for advanced disease.10 Interestingly, a computeranalysis of dyspeptic symptoms was able to allocate over90% of patients with early gastric cancer to a high prioritygroup for endoscopy.Symptom scoring systems to assess patient priority for
endoscopy have already been adopted by some centres.l1-13The additional use of computerised symptom assessment byDavenport et al was criticised as being too technical andcostly to use; however, they too allocated 87% of patientswith gastric cancer to a high risk group.14 All this proves isthat there is no substitute for a good clinical history. None ofthe 13 patients with gastric cancer under the age of 45 yearsin our study had uncomplicated simple dyspepsia; they allhad more alarming additional features such as dysphagia,weight loss, postprandial vomiting, and haemorrhage.There would have been no difficulty in identifying thesepatients as high priority for endoscopy. There is genuinedifficulty, however, for patients with uncomplicateddyspepsia and it is for such patients that more guidance isneeded.
Accepting that malignant disorders are an unlikely causefor simply dyspepsia in younger patients, what benefitsacrue by investigating such patients in preference to startingappropriate treatment at their first consultation?
Endoscopic and/or radiological assessment of many patientswith dyspepsia does not ultimately change their
treatment,15,16 and open access endoscopy has not modifiedthe complication rate from peptic ulcerationY However,objectivity is helpful and particularly important in thosewith recurrent dyspepsia. Moreover, although thereassurance of a negative examination is difficult to assess,there is good evidence that it can be as effective as activetreatment, and hospital clinicians often underestimate itsvalue.18 Conversely, mild degrees of mucosal abnormalitycan be difficult to translate into symptoms and often confuse
patient management.The value of a double-contrast barium meal as a first line
investigation for patients with dyspepsia is diminishing. It isless sensitive than endoscopy, and in many cases of
suspected abnormality the patient is referred for a
confirmatory endoscopic examination, which delays thediagnostic process further. Nevertheless, it remains a
popular first line investigation with general practitioners,especially for their younger dyspeptic patients.
In conclusion, a reassessment of our thoughts aboutdyspepsia, its investigation, and treatment, is needed, withmore clinical and less technological input.15,19,20 Too manyyoung patients with simple dyspepsia are being investigated.In the first instance, the young dyspeptic patient should bereassured and treated symptomatically with antacids and/orH2RAs. Patients failing to respond to these measures shouldthen be referred for prompt evaluation, preferably byendoscopy. Such an approach would reduce the escalatingdemands on endoscopy units and help hospital clinicianstarget the overburdened service to those likely to reap mostbenefit.
Correspondence should be addressed to A. C. B. V’.
B. WILLIAMS AND OTHERS: REFERENCES
1. OPCS Morbidity statistics for general practice; third national study (1981-82).London: HMSO, 1986
2. Gear MWL, Bames RJ. Endoscopic studies of dyspepsia in a general practice. Br MedJ 1980; 280: 1136-37.
3. Dooley CP, Larson AW, Stace WH, et al. Double contrast barium meal and uppergastrointestinal endoscopy; a comparative study Ann Intern Med 1984; 101:538-45.
4. Cotton PB. Fibre optic endoscopy and the barium meal; results and implications.Br Med J 1973; ii: 161-65.
5. Nyren O, Willson F. Is gastroscopic examination of young patients worthwhile? ScandJ Gastroenterol 1982. suppl 78.27.
6. Forbat LN, Gnbble RJN, Baron JH. Gastrointestinal endoscopy in the young.Br Med J 1987; 295: 365.
7. Clarke ML Upper gastrointestinal endoscopy. Lancet 1985; i: 629.8. Fjosne U, Kleveland H, Waldum H, Halvorsen T, Petersen H. The clinical benefit of
routine upper gastrointestinal endoscopy. Scand J Gastroenterol 1986; 21: 432-39.9. Holdstock G, Bruce S. Endoscopy and gastric cancer Gut 1981; 22: 673-76.10. National survey of gastric dysplasia and early gastric neoplasia. London. British
Society of Gastroenterology, 1988.11. Martin KE, Sox HC, Masson WJ, Duisenbere CE. The clinical value of the upper
gastrointestinal series. Arch Intern Med 1980; 140: 191-95.12. Holdstock G, Harman M, Machin D, et al. Prospective testing of scoring system
designed to improve case selection for upper gastrointestinal endoscopy.Gastroeneterology 1986; 90: 1164-69.
13. Mann J, Holdstock G, Harman M, Machin D, Loehry CA. Screening system toimprove the cost effectiveness of open access endoscopy. Br Med J 1983; 287:937-40.
14. Davenport PM, Morgan AG, Darnborough A, De Dombal FT. Can preliminaryscreening of dyspeptic patients allow more effective use of investigation techniques?Br Med J 1985, 290: 217-20
15 Jones R. Open access endoscopy Br Med J 1985; 291: 424-26.16. Mead GM, Moms A, Webster GK, Langman MJS. Use of barium meal examination
in dyspeptic patients under the age of fifty. Br Med J 1977; i: 1460-61.17. Holdstock G, Colley S. Failure of increased use of endoscopy to influence complication
rate m peptic ulcer disease. Br Med J 1983; 287: 393-94.18. Editorial. Sense and sensibility about the barium meal. Lancet 1980; i: 1171-7219. Grant AK Open access endoscopy. Med J Austr 1986; 144: 58-59.20. Colin-Jones DG. Does every dB speptic patient need endoscopy? Advanced Medicine
23. London: Ballière Tindall, 1987, 112-18.
DEGREE OF MYOPIA IN RELATION TOINTELLIGENCE AND EDUCATIONAL LEVEL
T. W. TEASDALE1 I. FUCHS2E. GOLDSCHMIDT2
Copenhagen University, Institute of Clinical Psychology,Copenhagen,1 and Danish Institute of Myopia Research,
Ophthalmology Department, Centralsygehuset, Hillerød, Denmark2
Summary Intelligence test scores and educationallevels were compared for 5943 myopic and
9891 non-myopic 18-year-old men being drafted for
military service in Denmark. The former were grouped bydegree of myopia, in the range -0·25 diopters (D) to -7·75 D,according to the power of correcting lenses required.Myopes of all degrees had significantly higher test scoresand educational levels than non-myopes. However, therelation of these two variables to degree of myopia was notlinear; for both variables there were no significantdifferences among myopia groups in the range -2·0 to -7·75D. Whereas factors associated with intelligence andeducation seem to be important in triggering the onset ofmyopia, they seem to be much less important in determiningthe degree to which myopia progresses.
INTRODUCTION
IT is a widespread practice to distinguish two forms ofmyopia, a rare pathological form and a less severe simpleform. The pathological form can show several
complications, including chorioretinal degeneration, and italmost always appears in association with a high refractiveerror, usually to some degree above -8-0 diopters (D).The much more common myopias of degrees below
-8-0 D are almost always of the less severe form; it is