Embed Size (px)
Citation preview

Journal of Electrocardiology Vol. 30 No. 1 1997
Do Repolarization Abnormalities in Hypertrophic Cardiomyopathy Represent
Impaired Fatty Acid Utilization?
An Observation With QRST Isointegral Maps
Y o s h i h i d e K a w a k a m i , M D , * S a t o s h i S h i m a d a , M D , *
Yasu lh iko Saka i , M D , * M i c h i h i r o S u w a , M D , * H i k a r u N a g a o , M D , *
Y u z o H i r o t a , M D , * K e i s h i r o K a w a m u r a , M D , * I t a r u A d a c h i , M D , t a n d
I s a m u N a r a b a y a s h i , M D t
Abstract: To identify the clinical significance of the isointegral body surface map of the QRST interval (QRST map) and the occurrence of repolarization abnormalities in patients with hypertrophic cardiomyopathy (HCM), the QRST map and signal-averaged electrocardiogram were evaluated in 50 patients with HCM, in 33 of whom the results were compared with nuclear images both for radioiodine-labeled fatty acid metabolism and for radiothal- lium perfusion. The QRST departure map was used to determine two parame- ters of difference between patient and control recordings: the subnormal area (the number of lead points at which the departure index values were negative and lay more than 2 SDs from the mean of the normal control group) and the subnormal minimum (the absolute value of the minimum in the departure map). Late potentials were detected in 6 (12%) of the 50 patients; they were observed in 3 of the 5 patients with dilated-phase HCM but in only 3 (7%) of the other 45 patients. The subnormal area and minimum values were lower in nonobstructive HCM than in dilated-phase HCM. Of the 33 patients exam- ined by myocardial imaging, 28 (33%) had a filling defect or decreased uptake, as shown on fatty acid metabolic images, and 10 of the 28 also showed abnormal myocardial perfusion images, while the 18 others showed normal perfusion images. These 28 patients showed significantly larger values of the subnormal area and minimum than patients with normal results in both image tests, regardless of whether or not myocardial perfusion imaging abnormalities were present. The localization of filling defects or of decreased uptake presented in fatty acid metabolic images corresponded to the position of the minimum on the QRST departure map. These results suggest that the QRST map is useful for detection of repolarization abnormalities in HCM and that these abnormalities are highly related to impaired fatty acid utilization of the myocardium. Key words: QRST isointegral map, hypertrophic cardiomy- opathy, radioiodine-labeled fatty acid metabolic imaging, late potentials.
From the *Third Division, Department of Internal Medicine and ~-Department of Radiology, Osaka Medical College, Osaka, Japan Reprint requests: Yoshihide Kawakami, MD, Third Division, Department of Internal Medicine, Osaka Medical College, 2-7 Daigaku-
cho, Takatsuki, Osaka 569, Japan.
21

22 Journal of Electrocardiology Vol. 30 No. 1 January 1997
The ventricular gradient reflecting the isointe- gral value of the QRST interval, reported by Wil- son et al. (1), is theoretically independent of the ventricular activation sequence and useful in identifying whether the T wave change is primary or secondary to QRS deflection. On the basis of this concept, Abildskov et al. (2,3) introduced a method of clinically applying the isointegral body surface map of the QRST interval (QRST map) by using the body surface mapping technique. The QRST map has been employed for the evaluation of the localization and size of lesions of myocar- dial ischemia and infarction (4-6) repolarization abnormalities of essential hypertension and/or left ventricular hypertrophy (7,8), the presence of right ventricular overload (9,10), and susceptibil- ity to malignant arrhythmia in patients with long QT syndrome (11). It is well known that repolar- ization abnormalities, presenting as ST-segment depression and T wave inversion on the standard 12-lead electrocardiogram (ECG), are almost always present in hypertrophic cardiomyopathy (HCM) (12). Using the QRST map technique, Hirai et al. (8) found that repolarization abnor- malities were present in patients with HCM even when left ventricular hypertrophy was assessed as mild by echocardiography.
Recently, nuclear imaging with iodine-i23-beta- methyl-iodophenyl-pentadecanoic acid has been introduced to investigate myocardial fatty acid utilization. Although the main energy source of the normal myocardium is free fatty acids, impaired fatty acid uptake has been frequently observed in patients with HCM while the myocar- dial perfusion imaging with thallium-201 remains normal (13,14). We hypothesized that primary repolarization abnormalities detected by the QRST map might be related not only to impaired myocardial perfusion but also to impaired free fatty acid utilization.
The signal-averaged electrocardiogram (SAECG) has been used for identification of late potentials, which stratify the risk of sudden death and sus- tained ventricular arrhythmias (15). Although the incidence of late potentials in HCM is low (16), their presence indicates a slow conduction area of malignant reentrant tachyarrhythmias, and it is interpreted as the result of extensive tissue dam- age. This may also be related to the impairment of myocardial fatty acid utilization.
The purposes of this study in patients with HCM were to compare the findings of the SAECG, the QRST map, and fatty acid metabolic and myocar- dial perfusion images and to evaluate the possible association between repolarization abnormalities
and late potentials, impaired fatty acid utilization, and impaired myocardial perfusion.
Materials and Methods
The study population consisted of 38 men and 12 women with HCM of (mean age, 54.5 years; range, 20-74 years) whose diagnosis had been con- firmed by two-dimensional and Doppler echocar- diography, cardiac catheterization, and endomy- ocardial biopsy. Patients who also had concomitant preexcitation syndrome, complete bundle branch block, or prominent intraventricular conduction delay were excluded.
The 50 subjects were divided into the following four groups according to localization of hypertrophy and physiologic status: apical hypertrophy (apical HCM, n=20); hypertrophic obstructive cardiomyopa- thy (obstructive HCM, n=12); hypertrophic nonob- structive cardiomyopathy (nonobstructive HCM, n= 13); and dilated-phase hypertrophic cardiomyopa- thy (dilated phase HCM, n=5). Apical localization of hypertrophy on the echocardiogram, giant negative T wave on the ECG, and a characteristic "spade-like" appearance on the left ventriculogram (17) were present in all patients with apical HCM. In patients with dilated-phase HCM, the diagnosis of HCM had been established previously, and these patients were followed until they developed heart failure with hypokinetic and dilated left ventricles (18).
The control subjects were 40 normal individu- als (20 men and 20 women; mean age, 31.6 years; range, i8-43 years) without a history of cardiac disorder or systemic hypertension, whose ECGs, chest radiographs, and physical examinations were normal.
Body surface maps were recorded to construct the QRST map with use of the VCM-3000 system (Fukuda Denshi Co., Tokyo, Japan). This involved placing 87 unipolar electrodes on the chest surface according to the method described by Yamada (19) (59 leads on the anterior chest and 28 leads on the back) with reference to Wilson's central terminal. A standard 12-lead ECG and a Frank (X,Y,Z), lead ECG were recorded simultaneously. These ECG data were scanned by multiplexers, digitized by A/D converters at a rate of 1,000 samples per sec- ond throughout the QRST waves, and stored on floppy disks. After two-point baseline adjustment at the flat portion of the TP-segment before the P and after the T deflection of the selected PQRST complex, the QRST map was constructed. The QRST time integrals represent the sums of all potentials from the QRS onset to the T offset for

each lead. All time integral values were calculated by multiplying millivolts by milliseconds and expressed as mV • ms. The isointegral lines were displayed ,on the QRST map by means of the VCM- 3000 system. The isointegral departure index body surface map of the QRST interval (QRST departure map) was also constructed by the deviation of the patient's data from the normal QRST isointegral values at each lead, calculated as the mean of the recordings from the 40 normal subjects.
The deviation was; expressed as departure index, defined as (QRST isointegral value - mean QRST isointegral value)/SD (5). When a departure index value was negative and lay more than 2SD from the mean on the QRST departure map, the reduc- tion was considered statistically significant, and the reduction area was ,designated as a -2SD area. The following parameters were then derived: the num- ber of lead points within each -2SD area (sub- normal area, reflecting the extent of statistically abnormal negative area) and the absolute value of departure index at the minimum (subnormal mini- mum, reflecting the magnitude of deviation from normal) in each QRST departure map.
We simultaneously recorded the SAECGs from a modified X (standard lead I), Y (lead aVF), and Z (precordial lead V2) lead system using the Multi- cardiner VCM-3000 and VL 303 according to Sire- son's method (15). Ectopic and grossly noisy beats were rejected by a template algorithm, and 200 beats were averaged. Each lead was filtered with a bidirectional, high-.pass digital filter, which was designed to eliminate filter ringing (20). The sig- nal from each lead was recorded at a bandwidth of 40-300 Hz and was then converted from ana- log to digital data with 12-bit accuracy at a sam- pling rate of 1 kHz. The filtered signals from the three leads were combined into a vector magni- tude, ~X2+Y2+Z 2 (21). The end of the filtered vec- tor magnitude QRS complex (filtered QRS) was designated as the point at which the amplitude of the filtered QRS became less than three times the noise level. Late potentials, shown as low-ampli- tude, high-frequency signals at the end of the fil- tered QRS, were defined as being present when any two of the following three criteria were met: the root mean square voltage in the last 40 ms of the filtered QRS was less than 15 gV; the filtered QRS duration was greater than 130 ms; and the filtered QRS duration after the voltage decreased to less than 40 gV was more than 40 ms (22).
Nuclear imagings for both radioiodine-labeled fatty acid metabolism and radiothallium perfusion were performed within 1 month of the body sur- face mapping and SAECG studies in 33 of the 50
QRST Isointegral Map in HCM • Kawakami et al. 23
patients. In fatty acid metabolic imaging, the patient was kept in the fasting condition until the end of the procedure. Each patient at rest received 111 MBq of iodine-123-beta-methyl-iodophenyl- pentadecanoic acid (Nippon Medi-Physics Co., Chiba, Japan) intravenously, and 30 minutes after the injection images were obtained with a gamma camera (Toshiba GCA-9300A/HG) equipped with a low-energy, high-resolution collimator centered on the 160-keV photopeak with 24% window (13, 23). In myocardial perfusion imaging, which was performed on another day, 74 MBq of thallium- 201 was injected intravenously, and images were obtained 15 minutes after the injection with a gamma camera (Siemens ZLC-7500) equipped with a low-energy, high-resolution collimator cen- tered on the 70-keV photopeak with a 20% win- dow. In both imagings, single-photon emission computed tomographic images at slices in the ver- tical long-axis, short-axis, and horizontal long-axis planes were reconstructed by using a Shepp-Logan filtered back projection algorithm. The uptake was classified into normal, increased, decreased, and defect categories by visual analysis, and we evalu- ated impaired regional fatty acid metabolism and impaired myocardial perfusion.
The subnormal area and minimum in the four I-ICM groups are expressed as mean ±SD, and in the three groups classified according to the scinti- graphic findings, the data are expressed as the median, range, and mean _+SD because of the abnormality of the distribution. The Tukey-Kramer method was used for the pairwise comparisons and P values < .05 (two-sided) were considered to be statistically significant for differences between two groups of subjects.
Results
Late Potential
Late potentials were detected by the SAECG in 6 (12%) of the 50 patients with EICM, and they were most frequently observed in the dilated- phase HCM group (3 of the 5 patients). Late potentials were present in only 3 (7%) of the other 45 patients. Both fatty acid metabolic and myocardial perfusion images showed defect or decreased uptake in all patients with late potentials. Figure 1 demonstrates a representative SAECG of a 47-year-old man with dilated-phase HCM. Of note, the terminal portion of the filtered QRS shows fragmented signals of low amplitude and long duration.

2 4 J o u r n a l o f E l e c t r o c a r d i o l o g y Vol . 3 0 No. 1 J a n u a r y 1 9 9 7
: . . . . . i i J i : i i i : t i i i i i ¸ i : • : i ! ; " i : . . . . . i t - ? - . 1 : • : . . . . . . i
J ~ F " i ' 1 ' ~ " i "
i : : :i ~ i{i ~ ' .... ~ ~ ........ . . . . ' ' 1 . . . . . . . . . . . . . . . i
i :. ~:: ' i r . . . . . . . , F " " F F F ~ ~ F~ --- ~ 'F~ - y ~
i~ ! i i!:°~ .. . . ... ~ ~ . . . . i s : , ; : . : . L : ' : . , i , . : : - : i . . . .
. . . . . . i i : " | : - " : . . . . : :
: :!: i i i ! i ! : i i ~ ' : :~ . . . . . . . . . . . . . . . . ' : ~ { ' : I . L L ~ : L ¢ ; " : . . . . . . :
2 [ ' ..... ' . . . . . . . . . . . . . . i : : ' : ' i : ' : : ~ i : ' : : : ~': : : : " i . . . . . . . .
• . . . . : [ " " [ ' [ . . . . . t ~ . . . . . . . . ~ . . . . . . . { "" : :
: . iiiiiil;iiii i::5 V: . . . . . I " ! I f ' - : - : i '
" : t i ~ i . . . . . . ! • •
• . f: :: ; i , : : i : : : ! {
• $ Fig. 1. A representative signal-averaged ECG (magni- tude lead) in a patient with dilated-phase hypertrophic cardiomyopathy. Arrowhead indicates late potentials (root-mean-square voltage in the last 40 ms [RMS 40]; 3.3 g V; filtered QRS duration, 131 ms). S, start point for measurement of RMS 40; E, endpoint of filtered QRS.
ORST Map
As shown in Figure 2, the m e a n QRST map obtained f rom the data for the 40 normal individu- als demons t ra ted smooth bipolar surface distribu- tion, wi th a m a x i m u m at the site of G4 (V4 of the
ECG) and a m i n i m u m at the site of D7 (right upper quadran t of the chest).
The extent (subnormal area) and intensi ty (sub- normal m i n i m u m ) of repolarization abnormali t ies in the four groups of HCM patients are shown in Table 1. The subnormal area value was lower (P < .01) in the nonobst ruct ive HCM group than in the dilated-phase HCM group, and as compared with each of the other three groups of HCM patients, the nonobst ruct ive HCM group showed the small- est subnormal m i n i m u m value (P < .01 or .05). Conversely, the subnormal area and m i n i m u m val- ues were larger in the dilated-phase HCM group than in the nonobst ruct ive HCM group. The inten- sity of repolarization abnormali t ies was least severe in the nonobst ruct ive HCM group, and the extent and intensi ty of repolarizat ion abnormali t ies were more severe in the di lated-phase HCM group than in the nonobst ruct ive HCM group.
Scintigraphic Findings
Among the 33 patients w h o unde rwen t fatty acid metabol ic and myocardia l perfusion imagings, no rmal or increased uptake was detected on bo th imaging studies in only five patients (group 1, 15 %). In 18 patients (group 2), the fatty acid meta- bolic images showed defect or decreased uptake, while the myocardia l perfusion images were nor- real or showed increased uptake. The remaining 10 patients (group 3) showed defect or decreased uptake on bo th images. Table 2 demonst ra tes the compar ison of the subnormal area and m i n i m u m values on the QRST depar ture map in the groups wi th the three different pat terns of up take on fatty acid metabol ic and myocardia l perfusion images. The subnormal area and m i n i m u m values were clearly larger in groups 2 and 3, but no difference was observed be tween these two groups. Thus, the extent and intensi ty of repolarizat ion abnormali t ies
Fig. 2. Normal mean QRST isointegral map. Isointegral contours are separated by 40 mV • ms, and shading indi- cates negative areas. Maxi- mum and minimum are indi- cated by plus and minus signs. Open circles (O) show the six precordial lead points of the ECG.
A B C D E F G H I J K L MA

QRST Isointegral Map in HCM • Kawakami et al. 25
Table 1. Subnormal Area and Minimum in the Four Hypertrophic Cardiomyopathy Groups
Group S u b n o r m a l Area* S u b n o r m a l M i n i m u m *
Apical EICM (n = 20) 18.6 + 8.1 4.8 + 2.0 Obstructive HCM (n = 12) 1 9 . 1 + 9 . 4 4.4_+ 1.2 t ~ ] t Nonobst ruct ive HCM (n = 13) 10.9 + 8.9 I t 2.6 ± 1.2 Dilated-phase HCM (n = 5) 27.4 + 7.7 5.1 + 1.6
*Data are expressed as m e a n ± SD. -{P < .01; SP < .05. There are no significant differences be t ween two groups whe re none are indicated. Subnormal area, n u m - ber of lead points whe re the depar ture index values are negat ive and lie more t h a n 2SD on the QRST depar ture map; subno rma l m i n i m u m , absolute value of depar ture index at the m i n i m u m on the QRST depar ture map; EICM, hyper t rophic cardiomyopathy.
were more severe in the patients with abnormali- ties in fatty acid metabolic images than in the patients with normal scintigraphic findings, regard- less of the presence or absence of myocardial per- fusion imaging abnormalities.
Correlation of the Localization of Abnormalities between Scintigraphy and the QRST Departure Maps
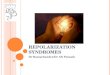
Figure 3 shows the fatty acid metabolic images and QRST departure map of a 47-year-old man with dilated-phase HCM. Scintigraphic defect and decreased uptake were detected in the inferior and apical segments, associated with a dilated left ventricle and disproportionately thickened septal and lateral segments. The QRST departure map showed an extensive -2SD area on the lower part of the left anterior chest and back (subnormal area 39 points and subnormal minimum 4.7 SD), which indicated the regional repolarization abnor- malities in the inferior and apical segments and corresponded with the findings of fatty acid meta- bolic images.
Figure 4 shows the myocardial perfusion and fatty acid metabolic images, QRST departure map,
and ECG of a 64-year-old man with apical HCM. While myocardial perfusion was increased in the apical segment, fatty acid uptake was decreased in the same segment. Extensive repolarization abnor- malities were evident on the QRST departure map (subnormal area 29 points and subnormal mini- mum 5.8 SD), as well as on the ECG (giant nega- tive T waves, mainly in the left precordial leads). These electrical abnormalities corresponded not with the findings of myocardial perfusion images but rather with the findings of fatty acid meta- bolic images.
Twenty-eight patients who showed defect or decreased uptake in fatty acid metabolic images were classified into three groups according to the affected segments, namely, the anteroseptal, apical, and inferior regions. The correlation of the local- ization of the minimum on the QRST departure map with the filling defect in the fatty acid meta- bolic images was displayed on the body surface map (Fig. 5). The positions of the minima (mean ±SD) for the anteroseptal, apical, and inferior defect groups were distributed on the left upper parasternal (F-G 4-5), high left lateral (G-H 4-5), and left lower parasternal (F-G 2-4) areas, respec- tively. Thus, each group showed different distribu-
Table 2. Subnormal Area and Minimum in Three Different Patterns of Uptake of Fatty Acid Metabolic and Myocardial Perfusion Images
S u b n o r m a l Area S u b n o r m a l M i n i m u m
Group* M e d i a n R a n g e M e a n + SD M e d i a n R a n g e M e a n +_ SD
1 ( n = 5) 0 0-12 3.8 + 5.51f ~ 1.5 1.2-3.0 1.9 + 0.71+. 2 ( n = 18) 21 0-30 20.4 + 6.9 J |J- 4.7 1.7-6.8 4.7 + 1.5~-[J - 3 ( n = 10) 24 8-39 2 4 . 4 + 8 . 4 J 4.5 3.1-11.1 5 . 2 + 2 . 4 J
*Group 1 is' comprised of pat ients w i thou t filling defect or decreased uptake on bo th fatty acid meta- bolic and myocardia l per fus ion images, group 2 of those wi th defect or decreased uptake only on fatty acid metabolic images and no t on myocardia l per fus ion images, and group 3 of those wi th defect or decreased uptake on bo th types of images, t P < .01; there are no significant differences be tween two groups whe re n o n e are indicated.

26 Journal of Eiectrocardiology Vol. 30 No. 1 January 1997
A Fatty Acid Metabolic Images
Short Axis Horizontal Long Axis
B
4- " ~ 3 - .2.0
2-
1 , I I I I I I I I I I I
A B C D E F G FI I J K L M A
Fig. 3. (A) Fatty acid metabolic images at short axis (left) and horizontal long axis (right) and (B) QRST isointegral departure map of a 47-year-old man with dilated phase hypertrophic cardiomyopathy. Shading indicates -2SD area.
t ion of the m i n i m u m on the QRST depar ture map, which might indicate the correspondence be tween the localization of fatty acid metabol ic abnormal i - ties and the posit ion of the m i n i m u m on the QRST depar ture map.
.
4- o
3-
2-
1
Fig. 5. The distribution of the minima is displayed on the body surface map according to the fatty acid meta- bolic imaging abnormalities. In patients with filling defects localized in the anteroseptal (O), apical (A), and inferior (11) areas by fatty acid metabolic imaging, the positions of the minima are at F-G 4--5, G-H 4-5, and F- G 2-4 areas, respectively. Open circles (O) show the six precordial lead points of the ECG.
Discussion
It has been emphasized that the QRST map, which is independen t of activation sequence and dependen t on repolarizat ion properties, is a useful and convenient m e t h o d of data reduction. The usefulness of the QRST m a p as a noninvas ive indi- cator has been conf i rmed in its application to detect abnormal repolarizat ion propert ies (4-11) and to assess the vulnerabil i ty to ventr icular a r rhy thmia (24,25) of patients wi th various hear t diseases. However, the clinical usefulness of the
Myocard ia l Fa t ty Acid /-~ A Per fus ion Image Metabolic Image
B r 6 -
5- 4-
Hor izon ta l Long Axis
2- 0,0
1 ! ' "~'~ . . . . , , , - " , , Ai bE .l J K L M A
Fig. 4. (A) Myocardial perfusion (left) and fatty acid metabolic (right) images at horizontal long axis; (B) QRST isointe- gral departure map; and (C) ECG of a 64-year-old man with apical hypertrophy. Shading indicates -2SD area.

QRST Isointegral Map in HCM • Kawakami et al. 27
QRST map in patients with HCM has not been well studied. In this study, we compared the findings of the QRST map, the SAECG, and fatty acid meta- bolic and myocardial perfusion images.
For the assessnctent of the electrophysiologic instability and the extent of repolarization abnor- malities in HCM, tile presence of late potentials in the SAECG and the subnormal area and minimum calculated from the QRST departure map were examined in four groups with different types of HCM. Late potentials were detected in 6 (12%) of the 50 patients, being most frequently observed in patients with dilated-phase HCM, who were known to have impaired systolic function as the end stage of HCM (26). Excluding the patients with dilated-phase HCM, late potentials were found in only 3 (7%) of the other 45 patients. The incidence of late potentials in HCM has been reported to range from 12.5% to 20% (16,27). This low inci- dence in the time.-domain method SAECG might be due to the concealment of fragmented ventricu- lar activation by high-amplitude QRS deflection in HCM. In addition, the high incidence in the dilated-phase HCM group (three of five patients) suggests the presence of delayed electrical activa- tion with myocardial injury such as myocardial fibrosis. All patients with late potentials had a defect or decreased uptake on both the fatty acid metabolic and the myocardial perfusion images. This finding suggests that HCM patients with late potentials have more extensive myocardial damage than patients without them.
In the nonobstructive HCM group, the subnor- mal minimum value was small. This finding sug- gests that the repolarization abnormalities in this group are not severe, which may be due both to diffuse left ventricular hypertrophy, which cancels regional repolarization abnormalities, and to inclu- sion of early-stage HCM patients in this group. Con- versely, the subnormal area and minimum values in the dilated-phase HCM group were larger than in the nonobstructiw, • HCM group. Hayashi et al. (4), and Tonooka et al. (5) have reported the accuracy of the QRST map in estimating the localization and size of myocardial[ infarction. They demonstrated, moreover, a close ,correlation between the extent of the -2SD area and the myocardial perfusion defect score in patients with myocardial infarction. In our study, the subnormal area and minimum values were significantly greater in the dilated-phase HCM group than in the nonobstructive HCM group. However, there were only five patients in the dilated-phase HCM group. Therefore, we should extend our investigation to a larger study popula- tion to determine whether the subnormal area and
minimum values are useful for evaluating the severity of pathologic changes in HCM as well as those in myocardial infarction (4, 5).
The myocardium uses mainly free fatty acids for its energy source, but alternatively uses glucose when it is exposed to hypoxic conditions. Yone- kura et al. (28) have demonstrated that in the hypertrophied left ventricle while the epicardial half of the myocardium uses free fatty acid, the endocardial half uses glucose predominantly. Con- genital defects of free fatty acid uptake at the myocardial cell membrane in patients with ICCM were recently demonstrated by Tanaka and Kawa- mura (29) and Tanaka et al. (30). They also showed that inhibition of free fatty acid uptake to the myocardium would cause myocardial hyper- trophy (31). Nuclear imaging of radioiodine- labeled fatty acid metabolism was recently intro- duced to evaluate this impaired fatty acid utilization. Myocardial perfusion imaging is a reli- able method of evaluating the impairment of the myocardium. The region of perfusion defect depicted by this imaging technique is considered to be the ischemic or fibrotic area in patients with myocardial infarction and dilated cardiomyopathy (32,33). We previously reported that the distribu- tion of the minima and the -2SD areas on the QRST departure map reflected the injured area in patients with dilated cardiomyopathy as assessed by comparison with myocardial perfusion images (34). Fatty acid metabolic imaging, however, is independent of myocardial perfusion imaging. A filling defect or decreased uptake is frequently seen in HCM even in the absence of abnormalities on myocardial perfusion images (35). Furthermore, it has been reported that fatty acid metabolic imaging may play an important role in the diagnosis of early-stage HCM when myocardial perfusion or function is still normal ( 13,36).
In this investigation, the group with a filling defect or decreased uptake apparent in fatty acid metabolic images (groups 2 and 3) had signifi- cantly larger subnormal area and minimum values as compared with the normal uptake group (group 1), but there was no significant difference for sub- normal area or for subnormal minimum between the groups with (group 3) and without (group 2) defects visualized in myocardial perfusion images. These results suggest that both subnormal area and subnormal minimum are closely associated with the findings of fatty acid metabolic images regard- less of the findings of myocardial perfusion images. If so, the repolarization abnormalities assessed by using the QRST map are related to the impaired fatty acid utilization. In addition, this investigation

28 Journal of Electrocardiology Vol. 30 No. 1 January 1997
reveals that the localization of the defect or decreased uptake in fatty acid metabol ic images corresponds to the posit ion of the m i n i m u m on the QRST depar ture map. Overall, it is suggested that the repolarization abnormali t ies in HCM are highly related to impaired fatty acid utilization.
Study Limitations
Our investigation has several limitations. First, we could not assess fatty acid metabol ic images by quanti tat ive analysis employing such paramete rs as up take index in each segment . A correlation coeffi- cient of ei ther subnormal area or subnormal mini- m u m with a decreased uptake index should be obtained to evaluate whe t he r the QRST depar ture map index correlates wi th the severity depicted on the images and wh e t he r it reveals the extent of the injured area. Second, the localization of filling defect or decreased uptake shown on tat ty acid metabol ic images was classified into only three regions. Strict compar ison be tween the posit ion of the m i n i m u m on the QRST depar ture map and abnormal area in fatty acid metabol ic images was impossible because there were several patients wi th two or more decreased uptake segments, especially in the dilated-phase I-ICM group. Finally, the distribution of the m i n i m a on the QRST depar- ture map over lapped with each other. Accordingly, fur ther study with larger pat ient populat ions is needed to confirm the precise localization of the injured area as derived f rom the QRST depar ture map findings.
Conclusion
This investigation demonst ra tes the practical usefulness and clinical significance of the QRST map in identifying the extent and localization of repolarization abnormali t ies in patients wi th HCM. The QRST m a p m a y also provide valuable informa- tion in the evaluat ion of HCM. This investigation also suggests that the occurrence of repolarizat ion abnormali t ies in HCM might be due to impaired myocardia l free fatty acid metabol ism. These results require fur ther validation by prospect ively applying the QRST map to a large n u m b e r of patients wi th HCM.
References
1. Wilson FN, Macleod AG, Barker PS et al: The deter- mination and the significance of the areas of the ventricular deflections of the electrocardiogram. Am Heart J 10:46, 1934
2. Abildskov JA, Urie PM, Lux RL et al: Body surface distribution of QRST area. Adv Cardiol 21:59, 1978
3. Abildskov JA, Burgess M J, Millar K, Wyatt R: New data and concepts concerning the ventricular gradi- ent. Chest 58:244, 1970
4. Hayashi H, Watabe S, Yabe Set al: Diagnostic value of QRST isointegral maps in detecting myocardial infarction complicated by bundle branch block. Cir- culation 80:542, 1989
5. Tonooka I, Kubota I, Watanabe Yet al: Isointegral analysis of body surface maps for the assessment of location and size of myocardial infarction. Am J Car- diol 52:1174, 1983
6. Adachi M, Hayashi H, Hirai M et al: Usefulness of QRST time-integral values of 12-lead electrocardio- grams in diagnosing healed myocardial infarction complicated by left bundle branch block. Am J Car- diol 68:i417, 1991
7. Igarashi H, Kubota I, Ikeda K et al: Body surface mapping for the assessment of left ventricular hypertrophy in patients with essential hypertension. Jpn Heart J 28:165, 1987
8. Hirai M, Hayashi H, Ichihara Y et al: Body surface distribution of abnormally low QRST areas in patients with left ventricular hypertrophy: an index of repolarization abnormalities. Circulation 84:1505, 1991
9. Asano Y, Izumida N, Kiyohara K et al: Diagnosis of right ventricular overload by body surface QRST isointegral maps in children with postoperative right bundle branch block. J Electrocardiol 28:209, 1995
10. Izumida N, Asano Y, Kiyohara K et al: QRST isointe- gral map reflects the sudden reduction of right ven- tricular pressure after balloon pulmonary valvulo- plasty. J Electrocardiol 28:223, 1995
11. De Ambroggi L, Bertoni T, Locati E et al: Mapping of body surface potentials in patients with the idio- pathic long QT syndrome. Circulation 74:1334, 1986
12. Devereux RB, Reichek N: Repolarization abnormali- ties of left ventricular hypertrophy: clinical echocar- diographic and hemodynamic correlates. J Electro- cardiol 15:47, 1982
13. Kurata C, Tawarahama K, Taguchi T et al: Myocar- dial emission computed tomography with iodine- 123-labelled beta-methyl-branched fatty acid in patients with hypertrophic cardiomyopathy. J Nucl Med 33:6, 1992
14. Knapp FF Jr, Ambrose KR, Goodman MM: New radioiodinated methyl-branched fatty acids for car- diac studies. Eur J Nucl Med 12:$39, 1986
15. Simson MB: Use of signals in the terminal QRS com- plex to identify patients with ventricular tachycardia after myocardial infarction. Circulation 64:235, 1981
J.6. Cripps TR,,Cotmihan PJ, Frenneaux MP et,al: Signal averaged electrocardiography in hypertrophic car- diomyopathy. J Am Coll Cardiol 15:956, 1990
17. Maron B J, Bonow RO, Seshagiri TN et al: Hyper- trophic cardiomyopathy with ventricular septal hypertrophy localized to the apical region of the left ventricle (apical hypertrophic cardiomyopathy). Am J Cardiol 49:1838, 1982

18. Fighali S, Krajcer Z, Edelman S, Leachman RD: Progression of hypertrophic cardiomyopathy into a hypokinetic left ventricle: higher incidence in patients with midventricular obstruction. J Am Coll Cardiol 9:288, 1987
19. Yamada K: Body surface iso-potential map: past, present, and future. Jpn Circ J 45:1, 1981
20. Kuchar DL, Thorburn CW, Sammel NL: Late poten- tials detected after myocardial infarction: natural history and prognostic significance. Circulation 74: i280, 1986
21. Simson MB, Untereker WJ, Spielman SR et al: Rela- tion between late potentials on the body surface and directly recorded fragmented electrograms in patients with ventricular tachycardia. Am J Cardiol 51:105, 1983
22. Ozawa Y, Yakubo S, Hatano M: Prospective study of late potentials to predict cardiac sudden death and ventAcular tachycardias in patients with myocardial infarction surviving over 4 weeks. Jpn Circ J 54: 1304, I990
23. Chouraqui P, Maddahi J, Henkin R et al: Compari- son of myocardial imaging with iodine-123- iodophenyl-9-methyl pentadecanoic acid and thal- l ium-201-chloride for assessment of patients with exercise-induced myocardial ischemia. J Nucl Med 32:447, 1991
24. Gardner MJ, Montague TJ, Armstrong SC et al: Vul- nerability to ventricular arrhythmia: assessment by mapping of body surface potential. Circulation 73: 684, 1986
25. Tsunakawa H, Nishiyama G, Kusahana Y, Harumi K: Identification of susceptibility to ventricular tachy- cardia after myocardial infarction by nondipolari ty of QRST area maps. J Am Coll Cardiol 14:1530, 1989
26. Wigle ED, Rakowski H, Kimball BP, Williams WG: Hypertrophic cardiomyopathy: clinical spectrum and treatment. Circulation 92:1680, 1995
QRST Isointegral Map in HCM • Kawakami et al. 29
27. Ozawa Y, Yakubo S, Tanigawa N et al: The clinical evaluation of the late potentials in patients with ventricular arrhythmias. Jpn Circ J 51:230, 1987
28. Yonekura Y, Brill AB, Som P e t al: Regional myocar- dial substrate uptake in hypertensive rats: a quanti- tative autoradiographic measurement . Science 227: 1494, 1985
29. Tanaka T, Kawamura K: Isolation of myocardial membrane long-chain fatty acid-binding protein: homology with a rat membrane protein implicated in the binding or transport of long-chain fatty acids. J Mol Cell Cardiol 27:1613, 1995
30. Tanaka T, Sohmiya K, Kawamura K: Is CD36 defi- ciency an etiology of hereditary hypertrophic car- diomyopathy? J Mol Cell Cardiol (in press)
31. Kusaka Y, Tanaka T, Okamoto F et al: Effect of sulfo- N-succinimidyl palmitate on the rat heart: myocar- dial long-chain fatty acid uptake and cardiac hyper- trophy. J Mol Cell Cardiol 27:1605, 1995
32. Dunn RE Uren RF, Sadick N e t al: Comparison of thallium-201 scanning in idiopathic dilated car- d iomyopathy and severe coronary artery disease. Circulation 66:804, 1982
33. Bulkley BH, Hutchins GM, Bailey I e t al: Thallium- 20I imaging and gated cardiac blood pool scan in patients with ischemic and idiopathic congestive car- diomyopathy: a clinical and pathologic study. Circu- lation 55:753, 1977
34. Kawakami Y, Sakai Y, Kawamura K: QRST isointe- gral map in dilated cardiomyopathy. Nippon Rinsho 53:219, 1995
35. Schelbert HR, Phelps ME, Shine KI: Imaging metab- olism and biochemistry: a new look at the heart. Am Heart J I05:522, 1983
36. Kurata C, Kobayashi A, Yamazaki N: Dual tracer autoradiographic study with thal l ium-20l and radioiodinated fatty acid in cardiomyopathic ham- sters. J Nucl Med 30:80, 1989