Embed Size (px)
Citation preview

DIZZINESS, SYNCOPE AND
ATRIAL FIBRILATION IN
THE OLDER ADULT

Slide 2
OBJECTIVES
Know and understand:
• The factors that may lead to dizziness and syncope in older adults
• The elements of evaluation (history, physical examination, testing) of older adults with dizziness and syncope
• The treatment options for dizziness and syncope

Slide 3
TOPICS COVERED
• Dizziness Classification and Causes Prognosis for Older Adults with Dizziness Evaluation and Management
• Syncope Pathophysiology Causative Factors Evaluation and Management

Slide 4
IMPORTANCE AND COMPLEXITY OF DIZZINESS
Dizziness is a common symptom in older adults• Accounts for 7 million clinic visits/year in US• Prevalence = 13%–38%
Challenges for clinicians• Precise classification is difficult• Worry about serious causes• Specific therapy not available for many 50% of cases have multiple causes

Slide 5
DRUG TOXICITY DIZZINESS
• In older adults, prescription drug toxicity is an important contributor to dizziness
• Use of 3 medications = dizziness risk factor
• Certain drugs are more frequently implicated
– Cause orthostasis or CNS effects
– Cardiovascular or antihypertensive drugs
– Psychotropic medications

Slide 6
Oscillopsia• seen in ototoxicity and in patients on
chemotherapy• patients complain of blurred vision• patients on ototoxic medications (eg, 24-hr
gentamicin) should be assessed• testing—ototoxicity possibly developing if
moving head while looking at large printed word produces movement or blurring of word

Slide 7
Ototoxicity
• associated with use of aminoglycosides
• Reassess need for ototoxic medication every week
• inform patients about possible dizziness and imbalance, and document

Slide 8
DIZZINESS: CLASSIFICATION BY SYMPTOMS
• Vertigo — Rotational sensation
• Presyncope — Sensation of impending faint
• Disequilibrium — Loss of balance without head sensation
• Lightheadedness — Ill-defined, not otherwise classifiable

Slide 9
Vestibular system• most patients with peripheral vestibular
dysfunction recover because • 1) central nervous system (CNS) resets incorrect
information received from ears by weighing it against information received from eyes
• 2) proprioceptive areas in feet and ankles maintain balance
• assess eyes• in elderly, check vibration sense, reflexes, and
position sense in toes

Slide 10
Vertigo
• illusion of movement where none exists
• Implies asymmetry between right and left
• does not always imply peripheral vestibular dysfunction
• 60% of patients destined for stroke may complain of dizziness (not necessarily vertigo)
• vertigo often prominent in cardiac dysfunction

Slide 11
CAUSES OF VERTIGO
• Peripheral vestibular disorders Benign positional vertigo Labyrinthitis Ménière’s disease
• Central vestibular disorders (minority of cases) Transient ischemic attack (TIA) Vertebrobasilar ischemia Brain tumors Multiple sclerosis

Slide 12
BENIGN POSITIONAL VERTIGO (BPV)
• Episodic
• Aggravated or brought on by changes in position (eg, turning, rolling over, bending over)
• Spells are often brief (5–15 sec)
• Spells are often milder than in other peripheral vestibular disorders

Slide 13
Benign paroxysmal positional vertigo (BPPV)
• movement in the plane of semicircular canal (eg, lying back, sitting up, or roll-ing over) results in burst of rotary nystagmus
• check for latency (ie, 1-30 sec after patient lies down); when patient lies down, brief burst of nystagmus slows down and stops, but occurs
• (then reverses) when patient sits up again; when patient• in patients who do not have classic rotary nystagmus, alcohol use most
common cause of positional dizziness• lies down again, nystagmus improves or resolves• Epley maneuver— patient sits on side of bed, lies down quickly to one side,
looks over shoulder, then sits up and lies down on other side and looks over shoulder (should be initially performed 5 times per side
• dimenhydrinate [eg, Gravol] 30 min before exercise helpful)• most patients with uncomplicated BPPV improve within days to weeks• difficult for patients with cervicospinal problems (not recommended for
elderly• associated with high recurrence of dizziness)

Slide 14
LABYRINTHITIS
• Also called vestibular neuronitis
• Occurs acutely
• Lasts several days
• Resolves spontaneously

Slide 15
Vestibular neuritis• common; often occurs after upper respiratory
infection (URI), herpes infection, or gastrointestinal viral infection
• patients severely ill, and always have nystagmus• treatment—in emergency department (ED), give
dexamethasone (eg, Decadron)• in office, give prednisone (1 mg/kg per day)• starting steroids early may help patients recover
sooner• (eg, within 2 mo; most patients recover within 1 yr)

Slide 16
Exercise and physiotherapy
• initiate after vomiting resolves
• Cawthorne-Cooksey exercises involve eye and head movements and tilting
• balance exercises with tossing balls
• challenge brain for faster recovery

Slide 17
MÉNIÈRE’S DISEASE
• Repeated episodes of tinnitus
• Fluctuating hearing loss
• Severe vertigo
• Eventual progressive sensorineural hearing loss
• Frequency and severity of vertigo may improve as hearing impairment worsens

Slide 18
Endolymphatic hydrops, Meniere’s disease
• classic episode— plugged ears; roaring tinnitus; severe vertigo• lasts 6 to 8 hr• vomiting; ataxia; hearing decreases with each successive episode• Rare• ask about headache and visual sensitivity• Vertigo and hearing loss in elderly patient more likely ischemic problem than true hydrops• counsel patients about decreasing caffeine, salt, and sugar intake• treatment—sublingual lorazepam (eg, Ativan) for severe episodes (effective in 15-30 min• Transdermal scopolamine patch slower)• rectal dimenhydrinate• Diuretic (eg, acetazolamide [eg, Diamox]) for pressure symptoms (discuss contraindications)• meclizine (eg, Bonine)• flunarizine (Sibelium) helpful when uncertain whether dizziness related to migraine or
peripheral vestibular problem• Meniett device decreases endolymphatic pressure (if ineffective, ablative procedure required)• differential diagnosis—atypical migraine; ischemic disease; autoimmune disease (consider
steroid trial in patients with eg, Crohn’s disease or lupus and fluctuating hearing loss)

Slide 19
BRAIN TUMORS
• Found in <1% of dizzy patients
• Slightly more prevalent (2%–3%) in older patients referred to neurologists
• Acoustic neuroma Most common tumor associated with dizziness
Unilateral cochlear symptoms (tinnitus and hearing loss) predominate, not dizziness
Bilateral cochlear symptoms in older persons usually represent presbycusis, not tumor

Slide 20
PRESYNCOPE
• Sensation of near-fainting
• Sign of decreased cerebral perfusion
• Cardiac causes Electrical: tachy- or bradyarrhythmias Structural, esp. aortic outflow obstruction
• Vascular causes (eg, orthostatic hypotension, vagal stimulation)
• Postural change (with or without orthostatic hypotension)

Slide 21
DISEQUILIBRIUM
• Sensation of being unsteady when standing or, in particular, walking
• Many factors can contribute to imbalance:
Chronic vestibulopathies
Visual problems
Musculoskeletal disorders
Somatosensory or gait deficits

Slide 22
LIGHTHEADEDNESS
• Best reserved as a description for patients who do not experience vertigo, presyncope, or disequilibrium
• Any cause of dizziness may occasionally produce “lightheadedness”
• The 2 most prominent considerations:– Psychiatric causes (depression, anxiety, somatoform
disorders)
– Idiopathic causes

Slide 23
Ophthalmic migraine• may present as visual symptoms and dizziness
without headache• few patients have classic basilar migraine (ie,
migraine associated with dysarthria, visual symptoms, and bilateral hearing loss)
• migraine vestibulopathy diagnosis of exclusion• if dizziness clearly associated with migraine, try
empiric medication (eg, flunarizine or topiramate [Topamax]
• if patient not sleeping well, consider nortriptyline)

Slide 24
PURPORTED CAUSES OF DIZZINESS, ESPECIALLY IN OLDER ADULTS
• Cervical arthritis
• Visual disorders
• Carotid sinus hypersensitivity

Slide 25
Other causes of dizziness
• obstructive sleep apnea (OSA)
• Depression
• rule out nystagmus before attributing hyperventilation dizziness to anxiety
• vestibular physiotherapy may be helpful in anxious patients

Slide 26
Elderly
• rarely present with primary ear problem
• Sudden dizziness may be due to ischemic cause
• perform computed tomography (CT) for patients in ED with risk factors or >60 yr of age

Slide 27
Trauma• short-term memory loss, headache, and loss of sense of smell likely due
to central concussion• slight hearing loss and dizziness with movement of head can be due to
whiplash, or central or vestibular concussion• distinguishing central from peripheral concussion—dizziness with
head movement can be sign of either, but dizziness without head movement more likely vestibular
• BPPV—may present later if head trauma significant• (ask, “is this the same kind of dizziness that you had after your• accident?”)• perilymph fistula—classic history includes dizziness with straining• patient may develop plugged ears and hearing loss, especially after
exertion (eg, weight-lifting) or head trauma• improves in most patients if heavy lifting and straining avoided (fistula
may be repaired if hearing continues to drop)

Slide 28
PROGNOSIS FOR OLDER PERSONS WITH DIZZINESS
• Usually resolves within days to several months
• Chronic or recurrent symptoms Experienced by ~25% of dizzy adults Commonly due to psychiatric disorders,
disequilibrium, or vestibulopathy other than BPV or labyrinthitis
• Not associated with increased mortality, hospitalization, or severe disability
• Associated with ↑ risk of syncope, falls, and depression, and with worse self-rated health

Slide 29
EVALUATION OF DIZZINESS: HISTORY
• Elicit the patient’s own description of the event without prompting
• Learn:
– Whether the dizziness is characterized by any of 3 sensations: spinning, fainting, or falling
– Whether there is a positional effect on symptoms– What other symptoms are associated with dizziness
(specifically ask about focal neurological symptoms)– What medications the patient is taking

Slide 30
EVALUATION OF DIZZINESS: HISTORY
• elderly have difficulty describing symptoms• patients may not mention other symptoms when overwhelmed by
dizziness and vomiting• ask about headache• tingling around mouth• Dysarthria• Imbalance• Severe problems usually present with nausea, vomiting, and
imbalance• assess reduced hearing• clinical signs more recognizable in patients with true disability• ask about bothersome movements• if symptoms worsen only when patient gets up, consider postural
problem

Slide 31
EVALUATION OF DIZZINESS: HISTORY
• true positional—occurs when patients lie down, roll to one side, and rise (or with hyperextension of head)
• movement-induced—occurs with all types of movement• sometimes confused with positional dizziness• Ask whether dizziness occurs only while walking consider cerebellar
problem• peripheral vestibular system stimulated with all movements, even while
driving• exercise-induced— consider cardiac problem, lack of physical
conditioning, or spinocerebellar ataxia type 6 abnormality (associated with familial hemiplegia syndromes)
• if dizziness induced by arm movement (eg, weight-lifting), listen at base of neck for bruit (suggests subclavian steal syndrome)
• visually-induced— common in migraineurs• may present as new symptom in patients developing multiple sclerosis

Slide 32
EVALUATION OF DIZZINESS:PHYSICAL EXAMINATION
• Take blood pressure and pulse while patient is supine and after standing for 1 to 2 min
• Perform a vestibular/nystagmus exam:– Primary position– Gaze-evoked– Head-hanging (Dix-Hallpike) test– Head shaking
• Perform cardiac examination
• Observe for balance and gait difficulties

Slide 33
Physical examination
• ask about initial episode and current symptoms• test rapid alternating movements and corneal reflex• identifying nystagmus• Enlarging patient’s eyes with high-powered reading glasses may be
helpful• dim lights and look at retina for 1 min, then look for• movement in blood vessel in other eye• peripheral vestibular nystagmus may be seen in center gaze (accentuated
by looking in direction of past component• no accentuation in central vestibular nystagmus)• Fukuda stepping test for balance—positive if patient moves to side while
stepping in place with eyes closed• hearing test—distract one ear by rubbing, and speak into other ear, “Suzy
eats tomatoes” (start at low pitch and gradually increase)• test both ears

Slide 34
EVALUATION OF DIZZINESS:DIAGNOSTIC TESTING (1 of 2)
• Audiometry
May help if cochlear symptoms are present (tinnitus, asymmetric hearing loss)
Abnormal results may indicate Ménière’s disease or, rarely, a tumor
• Vestibular testing
Electronystagmography Brain-stem auditory evoked responses Rotatory chair Dynamic posturography

Slide 35
EVALUATION OF DIZZINESS:DIAGNOSTIC TESTING (2 of 2)
• Neuroimaging (CT, MRI) occasionally warranted
• Electroencephalography (EEG) and lumbar puncture typically not useful
• Study the vertebrobasilar system if other neurologic symptoms suggest TIA
• ECG: low yield in patients with normal cardiac exam and no syncope
• Not useful for isolated dizziness: Holter and event monitors, echocardiography, stress testing, tilt-table, electrophysiologic studies

Slide 36
MANAGEMENT OF DIZZINESS (1 of 2)Treatable Cause Treatment
Acute vertigo of peripheral vestibular disorders
Reassurance and behavioral modification; meclizine (overused), plus a benzodiazepine only if absolutely needed, with caution for toxicity
BPV, mild Reassurance
BPV, severe or refractory Home habituation exercises, Epley’s maneuver
Ménière’s disease with frequent attacks
Salt restriction, diuretic, or both; occasionally refer for consideration of surgery

Slide 37
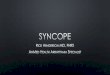
EPLEY’S MANEUVER

Slide 38
MANAGEMENT OF DIZZINESS (2 of 2)
Treatable Cause Treatment
Orthostatic hypotension Correct reversible causes
Disequilibrium Prevent falls with cane or other assistive device
Depression Trial of an SSRI
Chronic vestibulopathy Vestibular rehabilitation, a type of physical therapy

Slide 39
SYNCOPE: INTRODUCTIONSudden, transient loss of postural tone and consciousness
(not due to trauma) with spontaneous full recovery
• Accounts for:– ~3% of emergency department visits– 2% to 6% of hospital admissions
• 80% of those hospitalized for syncope are aged 65+
• Causes– May be benign or life-threatening– In older adults, may be multifactorial– Possible causes are numerous

Slide 40
NORMAL REFLEXES THAT PREVENT SYNCOPE
• 1/3 of blood volume pools in legs while standing
• Reflex pathways facilitate venous return and increase cardiac output– Baroreceptor reflex: ↑ autonomic sympathetic tone
peripheral vasoconstriction and ↑ heart rate
– Renal nerve: ↑ renin release from juxtaglomerular apparatus angiotensin II (causes vasoconstriction) and aldosterone (causes sodium retention)
– Atrial natriuretic factor: reduced upon standing, further facilitating vasoconstriction

Slide 41
PATHOPHYSIOLOGY OF SYNCOPE: EFFECTS OF AGING
• Reflex mechanisms are less responsive – ↓ ability to increase heart rate in response to
sympathetic stimulation– ↑ sensitivity to effects of dehydration and vasodilator
drugs
• Comorbidities that affect postural responses are common (eg, diabetes mellitus)
• Drugs may further impair postural reflexes (eg, -blockers, -blockers, tricyclic antidepressants)

Slide 42
SYNCOPE: NATURAL HISTORY
Altered systemic blood pressure orIncreased cerebral vascular resistance
Reduced cerebral perfusion
Syncope
Causes may be benign or life-threateningCauses may be multiple

Slide 43
COMMON CAUSES OF SYNCOPEIN ELDERLY PERSONS
• Arrhythmia• Aortic stenosis• Carotid sinus hypersensitivity• Hypoglycemia• Myocardial infarction• Orthostatic hypotension• Postprandial hypotension• Psychogenic causes• Pulmonary embolism (large)• Vasovagal faint

Slide 44
SYNCOPE: PROGNOSIS
Type of syncope 1-yr mortality
Cardiac 18%–33%
Noncardiac 6%
Unknown cause (1/3 to 1/2 of patients)
Intermediate, generally favorable

Slide 45
SYNCOPE EVALUATION:HISTORY (1 of 2)
Precipitants? • Eating• Urinating• Coughing• Medication• Emotional stress• Physical exertion• Turning head
Prodromal symptoms?• Chest pain• Palpitations• Dyspnea• Diaphoresis• Presyncope• Nausea• Vomiting

Slide 46
SYNCOPE EVALUATION:HISTORY (2 of 2)
• Medications?– How, when taken, what doses– Relationship to meals and activities– Recent changes
• Any witnesses?– Duration of event– Appearance of patient during event (flaccid tone
and motionless or increased tone and motion?)
• Comorbid conditions?Eg, coronary artery disease, diabetes mellitus

Slide 47
SYNCOPE CAUSED BY ARRHYTHMIA
• Prior to event Occurs in any position, <5 sec warning No precipitant; palpitations rare
• During event Flaccid tone; pulse faint or absent Blue, ashen skin Incontinence (rare)
• Recovery Rapid and complete

Slide 48
VASOVAGAL SYNCOPE
• Prior to event Aborted if person lies flat Seconds to minutes of warning Precipitant present; nausea/diaphoresis common Visual changes
• During event Motionless; relaxed tone; slow, faint pulse Pale color; dilated, reactive pupils
• Recovery Fatigue, nausea and diaphoresis common No retrograde amnesia

Slide 49
SYNCOPE CAUSED BY SEIZURE
• Prior to event Occurs in any position No warning or prodrome
• During event Rigid tone; rapid pulse; elevated BP Tonic eye deviation common Frothing at mouth
• Recovery Slow, incomplete Disorientation; focal neurologic findings

Slide 50
SYNCOPE EVALUATION:PHYSICAL EXAMINATION (1 of 2)
• Pulse in supine and standing positions
• Orthostatic vital signs: Measure BP in both arms, 1 min after standing and again after standing for 3 min
• Carotid pulse examination Delayed upstroke and low volume may identify aortic
stenosis Perform carotid massage only with continuous ECG and
resuscitation equipment availableContraindicated with carotid bruit, CVD, recent MI

Slide 51
SYNCOPE EVALUATION:PHYSICAL EXAMINATION (2 of 2)
• Cardiac examination for murmurs, extra heart sounds
• Stool for occult blood
• Neurologic examination for focal deficits

Slide 52
SYNCOPE EVALUATION: TESTING(1 of 2)
• ECG for all syncopal older adults; assess for: Acute or remote MI Conduction abnormalities and pre-excitation Sinus bradycardia Prolonged QT interval
• Ambulatory ECG
Among patients able and willing to operate loop recorders, diagnostic yield is ~25%
Implantable recorders are cost-effective for patients with ejection fraction >35% and symptoms not consistent with a neural cause of syncope

Slide 53
SYNCOPE EVALUATION: TESTING(2 of 2)
• Echocardiography
• Tilt-table testing
• Electrophysiologic (EP) studies
• Neurologic testing (MRI and CT, plus EEG) if focal neurologic signs or symptoms are present, or if the history suggests seizure

Slide 54
TREATMENT OF SYNCOPE (1 of 3)
• Focus on treating the underlying disorder
• In older patients, treatment of multiple possible causes is often necessary
• Discontinuation of medications that increase the risk of syncope is always an early step

Slide 55
TREATMENT OF SYNCOPE (2 of 3)
Cause Treatment
Myocardial ischemia Revascularization or aggressive medical therapy
Valvular heart disease (esp. aortic stenosis)
Usually surgery, avoid preload reduction
Symptomatic SVT Medical therapy or electrophysiology ablation
Significant ventricular tachyarrhythmia
Implanted defibrillator or medical therapy
Bradyarrhythmia Usually pacemaker

Slide 56
TREATMENT OF SYNCOPE (3 of 3)
Cause Treatment
Orthostatic hypotension
Adjust medications, ensure adequate volume, other conservative measures
Vasovagal syncope Avoidance of triggers; medical therapy is somewhat controversial (-blockers, clonidine, paroxetine, midodrine)
Carotid sinus hypersensitivity
Avoid stimulating factors (tight collars or rapid neck movements); pacemaker
Postprandial hypotension
Avoid alcohol and high-carbohydrate meals; remain recumbent after meals

Slide 57
RECURRENT SYNCOPE WITHOUT IDENTIFIABLE CAUSE
• Help patients avoid harm to themselves or others
• Consider recommending against driving for several months and resuming if patient remains recurrence-free (American Heart Association guidelines)
• Many states have laws against driving with a history of syncope

Slide 58
Complications of A Fib
• Complications associated with permanent atrial fibrillation (AF)
• increased risk for stroke• systemic thromboembolism,• Death• mortality is a function of underlying structural
heart disease or other comorbidities (survival in patients with lone AF same as that in otherwise healthy age-matched controls)

Slide 59
Evaluation
• history—control of hypertension important
• OSA
• look for reversible causes (eg, hyperthyroidism, pneumonia)
• medical history
• 12-lead electrocardiography (ECG) required
• echocardiography recommended

Slide 60
Patterns of AF
• second episode of AF may occur years after first
• important when considering long-term or temporary antiarrhythmic drug therapy
• management of persistent AF
• may differ from that of paroxysmal AF

Slide 61
Rhythm control vs rate control• AFFIRM trial found rhythm control not• superior to rate control for reducing mortality (survival curves similar• in Atrial Fibrillation Follow-up Investigation of• Rhythm Management (AFFIRM) trial, lower survival rates seen in patients
randomized to rhythm control• no difference in incidence of stroke over time between patients randomized
to rate control vs rhythm control• Canadian Cardiovascular Society guidelines—rate or rhythm control
acceptable• Management must be based on symptoms, patient’s preference, and risk
factors• (rhythm control might be favorable in high-risk groups)• factors that may favor rate control include persistent AF, frequent recurrent
AF, less symptomatology, older age, and hypertension• according to Atrial Fibrillation and Congestive Heart Failure (AF-CHF)
study, rhythm control appears more beneficial than rate control in HF

Slide 62
Treatment of newly diagnosed AF
• paroxysmal AF— consider anticoagulation• treat if symptomatic, or if ventricular rate uncontrolled• persistent AF—restore sinus rhythm with electrical or
pharmacologic cardioversion• temporary use of antiarrhythmic drugs (consider
maintenance and long-term use)• permanent AF—anticoagulation and rate control drugs as
required• rhythm control—may need to consider cardioversion• reevaluate therapy over time (as AF evolves,
antiarrhythmic drugs may no longer maintain sinus rhythm)

Slide 63
Infrequent episodes of paroxysmal AF
• “pill in the pocket” approach—give loading dose of propafenone (450 or 600 mg)
• then wait 30 min for conversion
• usually prescribed with rate control drugs
• shown highly effective

Slide 64
Medications• Beta-blockers• calcium channel blockers; dose• based on symptoms• digoxin alone usually not effective in controlling heart
rate during AF, but may be synergistic with other drugs• flecainide, propafenone, sotalol, and amiodarone used in
patients with no underlying structural heart disease• dronedarone—amiodarone analogue with fewer
associated side effects (eg, no corneal deposits, lower frequency
• of hyper- or hypothyroidism, no pulmonary toxicity)• shown superior to placebo

Slide 65
Stroke and systemic thromboembolism
• moderate-risk group—>75 yr of age with hypertension, some left ventricular dysfunction, HF, or diabetes
• high-risk group— history of stroke, transient ischemic attack (TIA), or valvular heart disease
• aspirin shown to slightly reduce risk for stroke in high-risk group, and warfarin significantly reduced risk for stroke (warfarin appears superior to aspirin in all risk groups
• but less beneficial because relative risk for stroke in low-risk group “very low”)

Slide 66
CHADS2 score• 1 point assigned for history of CHF• hypertension• older age• Diabetes• 2 points assigned for history of stroke or TIA• paroxysmal AF, persistent AF, and atrial flutter assigned same number
of points• recommendations—• treat with aspirin (or no medication) with score of 0• Treat with aspirin or warfarin (based on patient’s preference) with
score of 1• treat with warfarin and maintain international normalized ratio (INR)
at 2 to 3 with score 2 or more• CHADS2 score and risk for stroke may vary

Slide 67
Other risk factors for stroke
• Other risk factors• risk for stroke associated with paroxysmal
AF appears lower in recent clinical trials than in earlier studies
• patients who have episodes of AF lasting >24 hr have higher risk for thromboembolism than those with episodes lasting <24 hr

Slide 68
Warfarin use in AFFIRM trial
• Warfarin use in AFFIRM trial• warfarin stopped in patients prescribed
antiarrhythmic drug therapy in mistaken belief patients would remain in sinus rhythm
• risk for ischemic stroke slightly higher in patients treated with rhythm control who discontinued warfarin
• maintain INR of 2 to 3• (>3 increases risk for significant hemorrhage)

Slide 69
Risk for intracranial bleeding in elderly• predictors—
• inadequate education about use of oral anticoagulants• Polypharmacy• INR outside of therapeutic range• study did not see association between cognitive, visual, or
hearing impairment and increased risk of bleeding• careful use of anticoagulation can be successful• warfarin more effective than aspirin at preventing
thromboembolism in elderly patients with AF, but associated with increased risk of bleeding
• substantial risk in first year after initiation of anticoagulation (intense monitoring required)
• risk higher in patients with higher CHADS2 scores

Slide 70
Cardioversion
• associated with increased risk for stroke• Anticoagulation recommended for 3 to 4
wk before initiating and for 1 mo after cardioversion
• if AF has persisted for >48 hr, perform transesophageal echocardiography to rule out clotting in atrium, then proceed with cardioversion

Slide 71
ACTIVE studies• Atrial fibrillation Clopidogrel Trial with Irbesartan for
prevention of Vascular Events (ACTIVE) studies• ACTIVE W—warfarin superior to clopidogrel and aspirin in
preventing stroke (risk of bleeding similar)• patients naïve to warfarin at time of randomization and
treated with either clopidogrel and aspirin had increased risk of bleeding, compared to patients who were not naive to warfarin before randomization (suggests that patients with history of bleeding on warfarin had been weeded out of group)
• ACTIVE result a minor benefit in stroke reduction with aspirin and clopidogrel (compared to aspirin alone)
• but risk of bleeding same as with warfarin

Slide 72
Principles
• Principles of antithrombotic therapy
• individualize therapy
• reassess risk factors over time
• risk stratify when deciding to use aspirin or warfarin

Slide 73
RE-LY trial
• Randomized Evaluation of Long-term anticoagulation therapY (RE-LY) trial
• prevention of stroke or thromboembolism— low-dose dabigatran equivalent to warfarin
• high-dose dabigatran superior to warfarin• risk of bleeding—lower with low-dose
dabigatran than with warfarin• equivalent in high-dose dabigatran and warfarin

Slide 74
Who to refer• most patients with AF• patients <35 yr of age with symptomatic AF
or atrial flutter should be evaluated for supraventricular or atrial tachycardia (can be cured with catheter ablation)
• patients who remain highly symptomatic despite trials of antiarrhythmic drug therapy
• patients intolerant of therapies

Slide 75
Volume 360:668-678 February 12, 2009 Number 7 Effect of Dronedarone on Cardiovascular Events in Atrial
Fibrillation
Stefan H. Hohnloser, M.D., Harry J.G.M. Crijns, M.D., Martin van Eickels, M.D., Christophe Gaudin, M.D., Richard L. Page, M.D., Christian Torp-Pedersen, M.D., Stuart J. Connolly, M.D., for the
ATHENA Investigators• ABSTRACT• Background Dronedarone is a new antiarrhythmic drug that is being developed for the treatment of
patients with atrial fibrillation.• Methods We conducted a multicenter trial to evaluate the use of dronedarone in 4628 patients with atrial
fibrillation who had additional risk factors for death. Patients were randomly assigned to receive dronedarone, 400 mg twice a day, or placebo. The primary outcome was the first hospitalization due to cardiovascular events or death. Secondary outcomes were death from any cause, death from cardiovascular causes, and hospitalization due to cardiovascular events.
• Results The mean follow-up period was 21±5 months, with the study drug discontinued prematurely in 696 of the 2301 patients (30.2%) receiving dronedarone and in 716 of the 2327 patients (30.8%) receiving placebo, mostly because of adverse events. The primary outcome occurred in 734 patients (31.9%) in the dronedarone group and in 917 patients (39.4%) in the placebo group, with a hazard ratio for dronedarone of 0.76 (95% confidenceinterval [CI], 0.69 to 0.84; P<0.001). There were 116 deaths (5.0%) in the dronedarone group and 139 (6.0%) in the placebo group (hazard ratio, 0.84; 95% CI, 0.66 to 1.08; P=0.18). There were 63 deaths from cardiovascular causes (2.7%) in the dronedarone group and 90 (3.9%) in the placebo group (hazard ratio, 0.71; 95% CI, 0.51 to 0.98; P=0.03), largely due to a reduction in the rate of death from arrhythmia with dronedarone. The dronedaronegroup had higher rates of bradycardia, QT-interval prolongation, nausea, diarrhea, rash, and an increased serum creatinine level than the placebo group. Rates of thyroid- and pulmonary-related adverse events were not significantly different between thetwo groups.
• Conclusions Dronedarone reduced the incidence of hospitalization due to cardiovascular events or death in patients with atrial fibrillation. (ClinicalTrials.gov number, NCT00174785 [ClinicalTrials.gov] .)
•

Slide 76
Safely switch from amiodarone to dronedarone in two days, suggests
analysisMARCH 15, 2010 | Steve Stiles• Atlanta, GA - Patients on amiodarone for maintenance of sinus rhythm after cardioversion of atrial fibrillation (AF)
who are looking to switch to dronedarone (Multaq, Sanofi-Aventis) in most cases can safely begin taking the newer antiarrhythmic agent within two days of stopping the older one, according to a post hoc analysis of two randomized trials [1].
• The rate of serious adverse events associated with initiating dronedarone in the combined population of >1200 patients was low and varied little by whether patients had stopped taking amiodarone <48 or >48 hours previously or hadn't been on amiodarone at all.
• The patients were part of the European Trial in Atrial Fibrillation or Flutter Patients Receiving Dronedarone for the Maintenance of Sinus Rhythm (EURIDIS) and American-Australian-African Trial with Dronedarone in Atrial Fibrillation or Flutter Patients for the Maintenance of Sinus Rhythm (ADONIS), which together saw dronedarone reduce the risk of AF recurrence by 25% (p=0.022) over one year compared with placebo [2].
•The most effective and most toxic drug for AF
• The finding that a switch can be made fairly safely and rapidly may help allay concerns over possibly severe increased risk if a patient starts dronedarone too soon after withdrawing from a drug with an unusually long half life and a notorious adverse-effect profile.
• "Amiodarone is the most effective drug we have for atrial fibrillation, and it's also the most toxic drug we have for atrial fibrillation," observed Dr Peter R Kowey (Main Line Health System, Wynnewood, PA) for heartwire. Its multiorgan toxicities are cumulative, he noted, so a transition to the demonstrably safer dronedarone might be wise for younger patients. "With amiodarone, the fear is that if you continue to use it over the long term, then eventually the toxicity will emerge."
• Others on amiodarone who might switch to the newer drug, he said, are those who aren't tolerating it and those who still have AF recurrences despite it.
• Kowey, who cautioned that the post hoc analysis is based on a fairly small population and can be only hypothesis-generating, was to present it here today at the American College of Cardiology 2010 Scientific Sessions/i2 Summit.

Slide 77
Rapid transition preserves efficacy
•Of the 1237 patients with AF or atrial flutter in EURIDIS and ADONIS combined, who were randomized to dronedarone (400 mg twice daily) or placebo after cardioversion to sinus rhythm, 98 had started dronedarone within 48 hours of stopping amiodarone. Their rate of recurrence fell by 36% (p=0.022) compared with 56 placebo recipients with the same amiodarone history. But the two groups' rates of serious adverse events, including bradyarrhythmia, were similar, at 15.3% and 14.3%, respectively.
• For the 35 patients who started dronedarone longer than 48 hours after stopping amiodarone, the rate of serious adverse events was 17.1%, compared with 11.8% for their 17 corresponding placebo recipients.
• In the much-larger group with no history of receiving amiodarone, the rates were 13.7% for the 680 dronedarone patients and 16.2% for the 334 that had been assigned to placebo, Kowey reported.
• The rate of adverse events leading to drug discontinuation—especially bradyarrhythmia—was generally higher for dronedarone compared with placebo regardless of time since amiodarone withdrawal. It was 8.2% vs 3.6% for the group starting the new treatment within 48 hours and 20% vs 11.8% when the wait was longer than 48 hours.
• There were no instances of torsades de pointes, but QT-interval prolongation was more likely with dronedarone regardless of amiodarone status.
• Kowey says there may be some concern about adding dronedarone soon after amiodarone withdrawal in patients with a slow heart rate. In such cases, he said, "it's probably a good idea to wait a bit longer [than 48 hours]."
• And for patients with a long QT interval when taking amiodarone, "it's probably better to wait until the QT comes down."
• Otherwise, he said, "there doesn't seem to be any major liability" involved in starting dronedarone within 48 hours of stopping the older drug.

Slide 78
Brits Not NICE to Dronedarone• Monday January 11, 2010• The British National Institute for Clinical Excellence (NICE) has made a
preliminary determination NOT to cover the new antiarrhythmic drug dronedarone (Multaq, Sanofi-Aventis) for British patients with atrial fibrillation (AF). Instead, NICE implies, patients should continue receiving amiodarone (Cordarone, Pacerone), which is more effective and cheaper.
• Amiodarone is the most effective antiarrhythmic drug (drug that is supposed to stabilize the heart rhythm) available, but it unfortunately produces a bizarre array of side effects that are common, often dangerous or disabling, and difficult to treat. A suitable "replacement" for amiodarone has long been sought.
• Amiodarone: A Uniquely Toxic Drug• Amiodarone's Strange History• For a long time, it was hoped that dronedarone (a compound related to
amiodarone) would be that perfect replacement. It is not. While it appears to have much less toxicity than amiodarone, it is not as effective in treating AF.

Slide 79
Dronedarone Drug Information• And indeed, this was the very logic used by NICE to deny approval for dronedarone -- it is not as
effective as amiodarone, and it is much more expensive. So it will not be made available for British patients.
• DrRich Comments:• The dronedarone/NICE story illustrates how panels of "clinical excellence" (like NICE, or like the
panels apparently being established in the United States under pending healthcare reforms), even when they strictly follow the results of randomized clinical trials, can make decisions that seem reasonable on the surface but ultimately are harmful to patients.
• Consider that while the effectiveness of dronedarone in treating AF (effective in approximately 30% to 40% of patients) is substantially less than for amiodarone (which is effective in approximately 50% to 60%), this still means that a substantial minority of patients could potentially be treated effectively with dronedarone. So, for instance, if patients with AF were given a trial of dronedarone, potentially up to 40% of them could be spared exposure to the extravagant toxicity of amiodarone.
• But because randomized trials tell us that, in a large population of patients, the averageresponse to dronedarone is significantly lower than the average response to amiodarone, no patients (in Britain, at least) will have the opportunity to try dronedarone.
• To my mind, this example succinctly illustrates a key problem with how our bureaucrats propose to use panels of experts. Such panels can be of immense help in providing guidance to clinicians. But when bureaucrats insist on converting such recommendations into strict, "up or down" coverage decisions, individual patients will lose their opportunity to receive the kind of individualized care most of us value -- care given by our chosen doctors, who judiciously apply expert-generated clinical guidelines, while still taking our individual circumstances into account.

Slide 80
Dronedarone• Dronedarone is the latest antiarrhythmic drug to be developed for atrial fibrillation. In their search for a
safe and effective drug for atrial fibrillation, pharmaceutical companies have long imagined their "Holy Grail:" A drug that is as effective as amiodarone, but without its unique toxicity profile. Dronedarone (Multaq) was developed by Sanofi (the makers of amiodarone) specifically in the hopes of creating that holy grail.
• Dronedarone is indeed a derivative of amiodarone -- the most effective, but the most toxic, antiarrhythmic drug yet developed. Unlike amiodarone, dronedarone does not contain idodine atoms, and the iodine within amiodarone has been postulated to produce some of the drug's striking toxic effects, especially the thyroid toxicity seen with the drug, and perhaps the lung toxicity. Encouragingly, during the clinical trials with dronedarone, amiodarone-like toxicity so far has not been seen.
• Several clinical trials with dronedarone have been reported. Two of these trials (the EURIDIS and ADONIS trials) assessed the effectiveness of dronedarone for treating atrial fibrillation. In these trials, 64% of patients treated with dronedarone had recurrent atrial fibrillation during the first year after beginning treatment, as compared with 75% of patients treated with placebo. This improvement is statistically significant, but is by no means striking -- and indeed is little better than the reduction in atrial fibrillation seen with many other antiarrhythmic drugs.
• More recently, however, the ATHENA trial reported that patients treated with dronedarone for atrial fibrillation for 21 months had a signficantly reduced risk of death or cardiac hospitalization, compared to patients treated with placebo. This study is the first clinical study to suggest that treating patients who have atrial fibrillation with any antiarrhythmic drug can improve survival or reduce hospitalizations.
• While the results of the ATHENA trial have caused quite a stir, the mechanism for reduced mortality with dronedarone is unclear. Since dronedarone may not be remarkably effective in reducing recurrences of atrial fibrillation, perhaps the drug may have some other, undefined, benefit aside from actually preventing atrial fibrillation.

Slide 81
Dronedarone• Keep in mind that in 2003, Sanofi had to prematurely halt a clinical trial using dronedarone in patients
with significant heart failure and atrial fibrillation, at the urging of the independent Data Safety and Monitorning Board, because those treated with dronedarone appeared to have an increased risk of death. Notably, patients enrolled in the ATHENA trial were significantly healthier than in that earlier, more alarming, study.
• Side effects with dronedarone so far appear to be relatively benign. The most common reported side effects are diarrhea or nausea, slow heart rate, and rash. The unique side effects seen with amiodarone (such as lung toxicity, thyroid disorders, visual disturbances, or neurological disorders) have not been seen with dronedarone. However, it should be noted that none of the clinical trials with dronedarone have lasted for more than two years -- and some of the unusual toxicities seen with amiodarone may not appear until the drug has been taken for for several years. So, while dronedarone at this point looks reasonably safe, its true safety profile will not be known until it has been in use for a substantial period of time.
• The FDA approved the use of dronedarone for the treatment of atrial fibrillation in the summer of 2009. The FDA specified that dronedarone should be limited to patients who (like those enrolled in the ATHENA trial) do not have significant heart failure.
• Sources:• Hohnloser SH, Crijns HJGM, van Eickels M, et al. Effect of dronedarone on cardiovascular events in
atrial fibrillation. N Engl J Med 2009; 360:668-678.• Singh BN, Connolly SJ, Crijns HJGM, et al. Dronedarone for maintenance of sinus rhythm in atrial
fibrillation or flutter. N Engl J Med 2007; 357:987-99.• Ezekowitz MD. Maintaining sinus rhythm—making treatment better than the disease. N Engl J Med
2007; 357:1039.

Slide 82
Dabigatran• Atrial fibrillation increases the risks of stroke and death. Vitamin K antagonists,
such as warfarin, reduce the risks of stroke and death but increase the risk of hemorrhage as compared with control therapy.1 Therefore, warfarin is recommended for patients who have atrial fibrillation and are at risk for stroke.2Vitamin K antagonists are cumbersome to use, because of their multiple interactions with food and drugs, and they require frequent laboratory monitoring. Therefore, they are often not used, and when they are, rates of discontinuation are high.3,4 Many patients receiving warfarin still have inadequate anticoagulation.5Thus, there is a need for new anticoagulant agents that are effective, safe, and convenient to use.
• Dabigatran etexilate is an oral prodrug that is rapidly converted by a serum esterase to dabigatran, a potent, direct, competitive inhibitor of thrombin. It has an absolute bioavailability of 6.5%, 80% of the given dose is excreted by the kidneys, its serum half-life is 12 to 17 hours, and it does not require regular monitoring.6Dabigatran has been evaluated in a pilot trial involving patients with atrial fibrillation and in a study for the prevention of venous thromboembolism, in which doses of 150 mg twice daily and 220 mg once daily, respectively, were promising.7,8 We performed a large, randomized trial comparing the use of dabigatran, at doses of 110 mg twice daily and 150 mg twice daily, with warfarin.

Slide 83
Volume 361:1139-1151 September 17, 2009 Number 12Dabigatran versus Warfarin in Patients with Atrial Fibrillation
Stuart J. Connolly, M.D., Michael D. Ezekowitz, M.B., Ch.B., D.Phil., Salim Yusuf, F.R.C.P.C., D.Phil., John Eikelboom, M.D., Jonas Oldgren, M.D., Ph.D., Amit Parekh, M.D.,
Janice Pogue, M.Sc., Paul A. Reilly, Ph.D., Ellison Themeles, B.A., Jeanne Varrone, M.D., Susan Wang, Ph.D., Marco Alings, M.D., Ph.D., Denis Xavier, M.D., Jun Zhu, M.D., Rafael
Diaz, M.D., Basil S. Lewis, M.D., Harald Darius, M.D., Hans-Christoph Diener, M.D., Ph.D., Campbell D. Joyner, M.D., Lars Wallentin, M.D., Ph.D., and the RE-LY Steering
Committee and Investigators
• ABSTRACT• Background Warfarin reduces the risk of stroke in patients with atrial fibrillation but increases the
risk of hemorrhage and is difficult to use. Dabigatran is a new oral direct thrombin inhibitor.• Methods In this noninferiority trial, we randomly assigned 18,113 patients who had atrial fibrillation
and a risk of stroke to receive, in a blinded fashion, fixed doses of dabigatran — 110 mg or 150 mg twice daily — or, in an unblinded fashion, adjusted-dose warfarin. The median duration of the follow-up period was 2.0 years. The primary outcome was stroke or systemic embolism.
• Results Rates of the primary outcome were 1.69% per year in the warfarin group, as compared with 1.53% per year in the group that received 110 mg of dabigatran (relative risk with dabigatran, 0.91; 95% confidence interval [CI], 0.74 to 1.11; P<0.001 for noninferiority) and 1.11% per year in the group that received 150 mg of dabigatran (relative risk, 0.66; 95% CI, 0.53 to 0.82; P<0.001 for superiority). The rate of major bleeding was 3.36% per year in the warfarin group, as compared with 2.71% per year in the group receiving 110 mg of dabigatran (P=0.003)and 3.11% per year in the group receiving 150 mg of dabigatran (P=0.31). The rate of hemorrhagic stroke was 0.38% per year in the warfarin group, as compared with 0.12% per year with 110 mg of dabigatran (P<0.001) and 0.10% per year with 150 mg of dabigatran (P<0.001). The mortality rate was 4.13% per year in the warfarin group, as compared with 3.75% per year with 110 mg of dabigatran (P=0.13) and 3.64% per year with 150 mg of dabigatran (P=0.051).
• Conclusions In patients with atrial fibrillation, dabigatran given at a dose of 110 mg was associated with rates of stroke and systemic embolism that were similar to those associated with warfarin, as well as lower rates of major hemorrhage. Dabigatran administered at a dose of 150 mg, as compared with warfarin, was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage. (ClinicalTrials.gov number, NCT00262600 [ClinicalTrials.gov] .)

Slide 84
Dabigatran• We compared two fixed-dose regimens of dabigatran (110 mg twice daily and 150 mg twice daily), administered in a blinded fashion, with adjusted-dose warfarin,
administered in an unblinded fashion, in patients who had atrial fibrillation and were at risk for stroke. Both dabigatran doses were noninferior to warfarin withrespect to the primary efficacy outcome of stroke or systemic embolism. In addition, the 150-mg dose of dabigatran was superior to warfarin with respect to stroke or systemic embolism, and the 110-mg dose was superior to warfarin with respect to major bleeding.
• Previous studies seeking to identify a safe and effective alternative to warfarin for patients with atrial fibrillation have all had specific limitations. The combination of clopidogrel and aspirin was more effective than aspirin alone13 but less effective than warfarin.14 Subcutaneous idraparinux was more effective than warfarin but was associated with a substantially higher risk of bleeding.15 Ximelagatran, an earlier direct thrombin inhibitor, appeared to be similar to warfarin with respect to efficacy and safety but was found to be hepatotoxic.16 In our serial measurement of liver function, we did not find evidence of hepatotoxicity with dabigatran.
• The rate of myocardial infarction was higher with both doses of dabigatran than with warfarin. An explanation might be that warfarin provides better protection against coronary ischemic events than dabigatran, and warfarin is known to reduce the risk of myocardial infarction.17 However, rates of myocardial infarction were similar between patients with atrial fibrillation who were receiving warfarin and those who were receiving ximelagatran, another direct thrombin inhibitor.16The explanation for this finding is therefore uncertain.
• The most devastating complication of warfarin therapy is intracranial hemorrhage, especially hemorrhagic stroke. As compared with aspirin, warfarin doubles the risk of intracranial hemorrhage.1 Thus, our finding that the rate of this complication with both doses of dabigatran was less than one third the rate with warfarin,without a reduction in the efficacy against ischemic stroke, suggests an important advantage of dabigatran. The rate of major bleeding with warfarin was higher in our study than in some previous trials.11,13,14 This is partly explained by the more inclusive definition of major bleeding in our study. There was an increase in the rate of gastrointestinal bleeding with the higher dabigatran dose, despite the overall lower rates of bleeding at other sites. To enhance absorption of dabigatran, a low pH is required. Therefore, dabigatran capsules contain dabigatran-coated pellets with a tartaric acid core. This acidity may partly explain the increased incidence of dyspeptic symptoms with both dabigatran doses and the increased risk of gastrointestinal bleeding with the 150-mg dose.
• The benefit of dabigatran may be explained in part by the twice-daily dosing regimen. Since dabigatran has an elimination half-life of 12 to 17 hours, twice-daily dosing reduces variability in the anticoagulation effect, especially as compared with the anticoagulation effect of warfarin, which is difficult to control. Warfarin broadly inhibits coagulation (inhibiting factors II, VII, IX, and X and proteins C and S). By selectively inhibiting only thrombin, dabigatran may have antithrombotic efficacy while preserving some other hemostatic mechanisms in the coagulation system and thus potentially mitigating the risk of bleeding.
• The use of open-label warfarin could have introduced a bias in the reporting or adjudication of events. This risk was reduced by the implementation of several validated procedures, including blinded evaluation of outcome events. The unexpectedly different rates of myocardial infarction and gastrointestinal bleeding among the three treatment groups support an absence of bias. Control of anticoagulation with warfarin in our study was similar to that in previous international clinical trials, even though half our patients had not previously had extensive treatment with warfarin.10,17
• The net clinical benefit outcome, which is a measure of the overall benefit and risk, was similar between the two doses of dabigatran, owing to the lower risk of ischemia with the 150-mg dose and the lower risk of hemorrhage with the 110-mg dose. These findings suggest that the dose of dabigatran could potentially be tailored to take into consideration the risk characteristics of a specific patient, although this concept was not specifically tested in our trial.
• In conclusion, we compared two doses of dabigatran with warfarin in patients who had atrial fibrillation and who were at risk for stroke. As compared with warfarin, the 110-mg dose of dabigatran was associated with similar rates of stroke and systemic embolism and lower rates of major hemorrhage; the 150-mg dose of dabigatran was associated with lower rates of stroke and systemic embolism but with a similar rate of major hemorrhage.

Slide 85
SUMMARY (1 of 2)
• Precise classification of dizziness into vertigo, presyncope, disequilibrium, and lightheadedness is often difficult, and multiple causes of the same symptoms are common
• Most dizziness resolves within days to several months
• Key physical exam steps include checking for orthostatic hypotension, performing the head-hanging (Dix-Hallpike) test, and observing gait

Slide 86
SUMMARY (2 of 2)
• In older adults the cause of syncope is often multifactorial
• Most diagnostic procedures for syncope are expensive and have a low yield unless findings from the H & P suggest a particular cause
• The absence of cardiac disease strongly suggests that the cause of syncope is not cardiac
• Treatment of dizziness and syncope focuses on treating the underlying disorder

Slide 87
CASE 1 (1 of 3)
• For the past several weeks, a 69-year-old man has had recurrent spells of room-spinning vertigo that last for about 4 minutes.
• The spells occur spontaneously and are unassociated with positional changes. They are accompanied occasionally by double vision and sometimes by weakness on the right side.
• Several times, the patient has had sudden drop attacks, followed by mild weakness of both legs lasting several minutes.
• The patient has a history of diabetes mellitus and CAD.

Slide 88
CASE 1 (2 of 3)
Which of the following is the most likely cause of the vertigo?
(A) Vestibular neuronitis
(B) Vertebrobasilar insufficiency
(C) Labyrinthitis
(D) Migraine-associated vertigo
(E) Ménière’s disease

Slide 89
CASE 1 (3 of 3)
Which of the following is the most likely cause of the vertigo?
(A) Vestibular neuronitis
(B) Vertebrobasilar insufficiency
(C) Labyrinthitis
(D) Migraine-associated vertigo
(E) Ménière’s disease

Slide 90
CASE 2 (1 of 3)
• A 75-year-old woman reports repeated episodes of profound dizziness and near loss of consciousness, along with at least two episodes in which she found herself on the floor but was unaware of how she fell. She denies any confusion after the episode or any significant trauma.
• The patient takes amlodipine 5 mg/day for hypertension.
• BP is 152/84 and pulse is 76 when the patient is supine. In the upright posture, BP is 146/86 and pulse is 86. There is no jugular venous distension or carotid bruit. Lungs are clear. There is a slightly delayed carotid upstroke and a II/VI systolic murmur at the base with an intact S2 but no gallop.

Slide 91
CASE 2 (2 of 3)
Which of the following is the most appropriate next step in the evaluation of this patient to stratify her risk of adverse outcomes?
(A) Blood tests
(B) Electrocardiography
(C) Holter monitoring
(D) Event monitor
(E) Tilt-table test

Slide 92
CASE 2 (3 of 3)
Which of the following is the most appropriate next step in the evaluation of this patient to stratify her risk of adverse outcomes?
(A) Blood tests
(B) Electrocardiography
(C) Holter monitoring
(D) Event monitor
(E) Tilt-table test

Slide 93
CASE 3 (1 of 2)
Of the following features that may be available from a patient history, which best distinguishes syncope from an unexplained fall?
(A) Tonic-clonic movements
(B) Urinary incontinence
(C) Postictal state
(D) Loss of consciousness
(E) Loss of postural tone

Slide 94
CASE 3 (2 of 2)
Of the following features that may be available from a patient history, which best distinguishes syncope from an unexplained fall?
(A) Tonic-clonic movements
(B) Urinary incontinence
(C) Postictal state
(D) Loss of consciousness
(E) Loss of postural tone

Slide 95
Vertigo
• (A) Illusion of movement where none exists• (B) Often occurs after upper respiratory infection;• patients present with nystagmus• (C) Characterized as dizziness without hearing
loss;• treated with topiramate• (D) Seen in ototoxicity and in patients on
chemotherapy;• patients complain of blurred vision

Slide 96
Answer
• (A) Illusion of movement where none exists

Slide 97
Oscillopsia
• (A) Illusion of movement where none exists• (B) Often occurs after upper respiratory infection;• patients present with nystagmus• (C) Characterized as dizziness without hearing
loss;• treated with topiramate• (D) Seen in ototoxicity and in patients on
chemotherapy;• patients complain of blurred vision

Slide 98
Answer
• (D) Seen in ototoxicity and in patients on chemotherapy; patients complain of blurred vision

Slide 99
Vestibular neuritis
• (A) Illusion of movement where none exists• (B) Often occurs after upper respiratory infection;• patients present with nystagmus• (C) Characterized as dizziness without hearing
loss;• treated with topiramate• (D) Seen in ototoxicity and in patients on
chemotherapy;• patients complain of blurred vision

Slide 100
Answer
• (B) Often occurs after upper respiratory infection; patients present with nystagmus

Slide 101
Choose the correct statement about benign paroxysmal positional vertigo
(BPPV).(A) Rotary nystagmus occurs
immediately after movement (eg, to lying down position)
(B) Uncomplicated BPPV improves within days to weeks
(C) Epley maneuver recommended for elderly patients
(D) Most commonly caused by alcohol and drug use

Slide 102
Answer
• (B) Uncomplicated BPPV improves within days to weeks

Slide 103
Which of the following medications is recommended for severe endolymphatic hydrops?
(A) Dimenhydrinate (B) Prednisone
(C) Sublingual lorazepam (D) Nortriptyline

Slide 104
Answer
• (C) Sublingual lorazepam

Slide 105
If a patient is found to have short-term memory loss, headaches, and loss of sense of smell after head
trauma, themost likely cause is:
(A) A central concussion (B) A cervical injury
(C) A perilymph fistula (D) Whiplash

Slide 106
Answer
• (A) A central concussion

Slide 107
In the Atrial Fibrillation Follow-up Investigation of Rhythm
Management (AFFIRM) trial, patients randomized to
rate control therapy had a significantly higher incidence of stroke than those who received
rhythm control therapy.(A) True (B)False

Slide 108
Answer
• (B)False

Slide 109
When considering therapy for patients with atrial fibrillation (AF), which of the following factors might
favor ratecontrol over rhythm control therapy?
(A) Persistent AF (B) Older age
(C) Hypertension (D) All the above

Slide 110
Answer
• (D) All the above

Slide 111
Which of the following therapies is recommended for a patient with AF
and CHADS2 score of 0?(A) Warfarin with maintenance of
international normalized ratio at 2 to 3
(B) Aspirin or warfarin(C) Aspirin or no medication(D) Aspirin and clopidogrel

Slide 112
Answer
• (C) Aspirin or no medication

Slide 113
In elderly patients, warfarin appears to be more effective than aspirin at
preventing thromboembolism, but isassociated with increased risk of
bleeding.(A) True (B) False

Slide 114
Answer
• (A) True

Slide 115
ACKNOWLEDGMENTS
Co-Editors: Karen Blackstone, MD
Elizabeth L. Cobbs, MD
GRS6 Chapter Authors: David Bush, MD
Kurt Kroenke, MD
GRS6 Question Writers: Gail Ishiyama, MD Mathew Maurer, MD
Medical Writer: Barbara B. Reitt, PhD, ELS(D)
Reviewer: Colleen Christmas, MD
Managing Editor: Andrea N. Sherman, MS
© American Geriatrics Society