Embed Size (px)
Citation preview

Distribution of ABO Blood Types among Fertileand Infertile Women
GEORGE I. SOLISH1 AND HENRY GERSHOWITZ2
The factors responsible for the maintenance of the ABO polymorphism in manhave been the object of intensive but inconclusive investigation. Three principal butnot mutually exclusive mechanisms can be visualized, namely, differential mortalityof the ABO genotypes; distortions of the proportions of ABO blood groups, as frommeiotic drive; and differential fertility of the ABO genotypes. This paper is con-cerned with the last possibility, first suggested in a paper by Hirszfeld and Zborowski(1925), who called attention to the possibility of a serological incompatibility of thegametes as a cause for infertility. Later studies of Hirszfeld (1934, 1938) failed tosupport this hypothesis, and the idea was abandoned. Since then, however, severalreports have claimed detection of an association between ABO blood groups of theparents and the mean number of children produced in each family. Among thesereports are the often quoted publications of Waterhouse and Hogben (1947); Allan(1953); Bryce et al. (1950); Kirk et al. (1953); Kirk et al. (1955); and Matsunaga andItoh (1953, 1958). Other studies (Johnstone, 1954; Haga, 1959; Hiraizumi, 1964;Reed et al., 1964) have not revealed any such fertility differences related to the ABOblood groups of the parents.
Infertile couples represent an extreme in normal fertility variation and wouldappear to be especially favorable material in which to search for a possible relation-ship between ABO groups and fertility. The only study thus far directed at couplesknown to be sterile is that of Behrman et al. (1960), who investigated 102 sterilecouples selected by their failure to conceive after five years and for whom "no reasonfor their infertility problem could be determined by the most exhaustive gyneco-logical and urological examinations possible."
Eighty-nine of these couples, or 87.3%, were found to be ABO-incompatiblymated, compared with a control population of 171 fertile couples of whom 66, or38.6%, were incompatibly mated. As a consequence of this finding, Behrman et al.(1960) proposed that otherwise-unexplained infertility might be due to incompat-ibility in the ABO blood-group system.
Received April 9, 1968.This and a companion paper were submitted in partial fulfilment of the requirements for the
degree of doctor of philosophy at the University of Michigan.I Department of Obstetrics and Gynecology, State University of New York Downstate and the
Department of Human Genetics, University of Michigan. Career scientist, Health Research Councilof the City of New York. Present address: Department of Obstetrics and Gynecology, State Uni-versity of New York, Downstate Medical Center, 450 Clarkson Avenue, Brooklyn, New York 11203.
2 Department of Human Genetics, University of Michigan, Ann Arbor 48104.
23

24 SOLISH AND GERSHOWITZ
The present study was undertaken in an effort to confirm and extend the findingsof Behrman et al. (1960), utilizing infertile couples registered in a large metropolitaninfertility clinic because of complete or relative inability of the wife to conceive.
MATERIALS AND METHODS
Description of Study Population
A population of 6,553 married couples who had registered for treatment of infer-tility at the Infertility Clinic of the Margaret Sanger Research Bureau between 1947and 1963 was chosen for study. These patients were particularly suited for this in-vestigation because of their large numbers and the high follow-up rate, and because,
3000
2800
2600
2400 - WIVES
2I0Ih HUS20NDS JZ 2000-
1-1800-(L 1600 m
Li.. 1400.0
120-0LL 000.
800-DZ600.400-
200.
10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-60
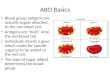
AGE IN YEARSFIG. 1.-Age at time of marriage of husbands and wives registered at Margaret Sanger Clinic
among other data, the ABO blood groups of both marital partners were availablefor over 80% of the registrants.
The Fertility Service of the Margaret Sanger Research Bureau operates as a non-profit outpatient clinic, located in New York City, and serves chiefly the metropoli-tan area. A nominal over-all fee is charged for a complete fertility investigation,which, of course, limits the clientele to those who can afford the fee.
For the most part, these patients had married within their own religious groups,so that less than 3% of the total were "mixed marriages." The ages of the patientsat the time of marriage are shown in Figure 1.
Socioeconomically, these patients fit in the middle income class of New Yorkdwellers. Ethnically, 91.4% were Caucasian, 7,42% were Negro, 0.37% were Ori-

ABO TYPES AND FERTILITY
ental and for 0.371%, ethnic origin was not recorded. Although the exact incomelevels are not available, the occupations of 12,566 individuals shown in Table 1 areindicative of the social standing of this population. One-third of the husbands wereemployed in a professional or technical capacity an additional 20% as craftsmenor foremen. Among the women, 25% were employed as clerical workers, and about50% were housewives.
After registration, a complete history was obtained, and physical examinationsof both the husband and the wife were performed. Certain basic laboratory datawere obtained in accordance with the suggestions of the American Fertility Society.The need for additional laboratory examinations was determined as the work-upprogressed. In the Sanger clinic, ABO and Rh blood typing was included as part
TABLE 1
OCCUPATIONS OF INFERTILITY CLINIC PATIENTS
Occupation Husband MWife
Professional, technical, or kindred worker 2,012 (32.2(" ) 931 (14.9Zc)Manager, official, proprietor ........... 648 (10.4(') ...................Clerical, kindred worker......540 (8.9() 1552 (24. 9 c)Sales worker ......................... 929 (14.8d,,) 108 (I.7c!)Craftsman, foreman, kindred worker.. 1,277 (20.46( ) 110 (1.8c,Operative, kindred worker ............. 290 (4.5c() 289 (4.6d( )Private household worker, laborer ....... 32 (0. Sc) 27 (0. 4( j)Service worker, except private household* 278 (4.66(") 95 (1. 5( c)Othert..230 (3. 7( 3,135 (50.2(--)UnknownT ........................... 317 306
Total ............................. 6,553 6,553
* Includes: guard, policeman, fireman, bartender, barber, elevator operator, etc.t Includes those not in the labor force: housewife, student, member of the armed forces, etc.+ Unknown are excluded in computing percentages.
of the basic work-up. All blood ty-ping was performed by the Bureau of Laboratoriesof the Department of Health of the Citv of New York. Accuracy of blood typingwas tested in the authors' laboratory by re-tx-ping a sample of 300 specimens. Nodiscrepancies were found.
Blood-group data were missing from the records of either husband or wife (orboth) in 1,497 of the 6,553 couples registered at the Sanger clinic during the studyinterval. These were excluded from this study. Organic causes for infertility, suchas infections or tumors of the reproductive organs, anatomical defects of the geni-talia, or sex-hormone derangements, were found in one or both marital partners inan additional 1,962 couples. These, too, were eliminated from the analxyses that follow.Thtus a total of 3,094 married couples with no assigned cause for their infertility wereavailable for this studx.
A nalyses
Two types of analxyses were performed on these data. First, the blood groups of"infertile" husbands were compared with those of their "infertile" wives, on thethesis that, if ABO incompatibility is responsible for the infertility, then there should
25

SOLISH AND GERSHOWITZ
be a relative excess of group A, group B, and/or group AB individuals among thehusbands and of group 0 individuals among the wives. These expectations are basedon reported observations in which clinical A-B hemolytic disease was found to berestricted almost entirely to infants of families in which the mother was blood group 0and the father group A or B (Zuelzer and Kaplan, 1954; Rosenfield, 1955).
Second, the blood groups of women of the largest ethnic segment in the sample,Jewish women, who comprised almost 60% of the population studied, were com-pared with the blood groups of a suitable control population. For the latter, a totalsample of 12,566 Jewish mothers, who proved their fertility by giving birth to achild at one of four New York hospitals during 1962 or 1963, was collected for com-parison. These four hospitals care for a high proportion of Jewish patients fromapproximately the same geographical area as that of Jewish women registered atthe Sanger clinic.The subsequent reproductive performance of individuals consulting the bureau
is updated periodically by the bureau. Accordingly, follow-up data extending onthe average five years after the initial visit were available for over 80% of patients.
RESULTS
ABO Blood Types of Infertile Married Couples
After completion of the gynecological and urological examinations and testingprocedures employed in the Margaret Sanger Infertility Clinic, infertility was un-explained in about 60% of the 6,553 couples studied. Many of these couples with noobserved cause for their infertility were barren prior to clinic registration and re-mained so after treatment. These couples designated "sterile" in Tables 2, 3, 4, 5,and 8 were unable to conceive for at least five years after clinic registration. A largerproportion of couples, for whom a cause for their reduced fertility could not bedetermined, had children or had achieved a pregnancy, at one time or another,either prior to clinic registration or after treatment. These are referred to as "sub-fertile."
For each of the ethnic groups represented and designated by their religious affili-ation, the blood-group distribution of the wives is not significantly different fromthat of their husbands, regardless of whether they fall into the "subfertile" or "ster-ile" groups (Table 2). If the ABO mating types observed among the "subfertile"couples are compared with those of the "sterile" group or if both the "sterile" and"subfertile" groups are combined and compared with the expected frequency ofmating types, no significant differences are seen (Table 3). The expected frequenciesof mating types in Table 3 were calculated from the gene frequencies. The latterwere obtained from the total number of ABO phenotypes, males and females, ineach religious group by the method of Stevens (1938).
Since clinical ABO incompatibility is almost always restricted to families in whichthe mother is blood group 0 and the father is group A, B, or AB, these mating com-binations among sterile couples shown in Table 3 were compared to their reciprocalcompatible mating types. Although there are significantly more incompatible A X 0matings than the reciprocal (X2 = 4.54, 1 df) among all sterile couples, a breakdown
26

ABO TYPES AND FERTILI-I'Y
by religion of couples indicates that a significant difference exists only among theJews (x2 = 4.64, 1 df). Although the trend is in the same direction for Catholiccouples, it is reversed among Protestant couples. Comparisons of B X 0 and AB X 0matings with their reciprocals were not rewarding.
As a further step in the analysis, the reproductive performance of each ABOmating type of the clinic population was analyzed (Table 4). Negro couples havebeen omitted from Table 4 because of the possibility of a bias due to higher rates offetal loss reported for Negroes (U.S. Bureau of the Census, 1966), hence the different
TABLE 2
ABO BLOOD TYPES OF INFERTILITY CLINIC PATIENTS
SUBFERTILE COUPLES STERILE COUPLES
RELIGION Blood Type x2 Blood Type X2
A B AB 0 Total (3 (if) A B AB 0 Total (3 df)
Protestant:Husbandt 127 37 10 116 290 f3.79 66 23 6 92 187 f2.51Wife . 105 43 14 128 290 l.3>P>.2 68 24 12 83 187 l.5>P>.4
Catholic:Husband 109 31 14 136 290 f 1 .56 115 41 10 124 290 3. 01Wife . 112 39 11 128 290 l.7>P>.6 95 47 11 137 290 l.4>P>.3
Jewish:Husband 458 185 78 404 1,125 f2.22 315 114 46 233 708 )13.61Wife ........470 198 85 372 1,125 1.6>P>.5 283 114 52 259 708 Q.4>P>.3
Other and un-known:
Husband 44 16 13 45 118 f3.89 41 16 3 26 86 f3.69Wife . 44 13 6 55 118 .3>P>.2 32 14 2 38 86 1.3>P>.2
Total:Husband.. 738 269 115 701 1,823 f1.30 537 194 65 475 1,271 f6.29Wife. 731 293 116 683 1,823 l.8>P>.7 478 199 77 517 1,271 l.1>P>.05
totals in Tables 3 and 4. The actual number of Negro couples is small and confinedto Protestant and Catholic groups, with no Negroes among the Jewish populationin this clinic.
At the termination of the period of observation, 59% of the women of the totalpopulation had conceived at least once. This includes those couples with pregnanciesterminated prior to clinic registration, with or without pregnancies following treat-ment, and those with no pregnancies prior to clinic registration who were successfulonly after treatment. Because of the failure to demonstrate significant differencesamong these subgroups, they were combined for these analyses. The 41%o of mat-ings remaining barren throughout the period of observation are proportionately dis-tributed among the ABO mating types (see Table 4) (x2 = 3.61, 13 df, P > 0.99).
Thirty-seven per cent of pregnancies terminated in abortion or stillbirth. Thesefetal losses were equally frequent among compatible and incompatible matings, asshown in Table 4 (X2 = 0.87, 1 df, 0.4 > P > 0.3). However, when (A + B + AB)
27

00000000w ON 00 It.6
-0
t d0 ON NO 000
0 Cm
x00n0O00t-(-40000m cN' C14
1-00 C.0 tf)
c4- 000m000 00m t-CN C- CN oo, d° 00
00
OmmNC04 tN NINC\ M (1 \0 'I m It_4 -q
rr ~c In rq x Cer rn
It ON ON en00 '00-' Lfn00 CO rn -"-
1-
NO N
-ON,-00'le)--NO'C00ONCOC) trC,-K'ON --I 00- c-Ci t- tn- n 'O
,' NO cc00000 CO4 mCN Ur
t Un In,-- re)0C-4 N
000cO ON 0 C4 0 NO 000)000 0 c-i - ON ON ON 00
Nc r-- c- ON
C040N e00 e) U-- - Ut-t- - cq-iON
00 c-i c-i 0 c- 00 ON 00'-C-i 00 I~
U-- NO --0 NONCc.11 M--0 00
C).xxxxm xxxx
00L'ot-OC-4o,
I--,0CNOtI- 11
C) mI-,/
t-s~
U-I"C
0C04f)
00000 ON 00m Lf
t c- m- - trc 'Cs C4Cso ) clq ItNO4 -0-
ON - m ONC, 0NO 000O'
00 ON ON NOc ON NO 0et -q en -4 -..
CN 't Xo so r - C14
I00 It 0 NO c- 00
00 00 00 en 0eCiN(, 100n
00 NOc-i NO 00 Ci enCNci C0 -
tn 0 ON 000 t-,-q l 1-4-
c-i c-l cI 0 0 ON NONC ON 00 c-i ONC-1i U- c-I c"i
0 en O'I It 000000 c-i c-i
0 U-- NOc-i - C-i 0-c- -
0 NO 00 dt 0 Ci 00ci U.) -4 -
-1s
r -.t 0
-0
r- >~'1-1
1-
0ir)
-
CO tn 00Cu-i0 00II.-,,
oogc000 00'-00
-4Lrn
Ln
0-
l-q
wri)
0
0Hu
zX)cn
0P4
cn
0
(-)
Hu4
t
0
u-4~4
-
00
0¢
0::
H
04
¢
le0H-
-o
V)
Id0
0
-oDn
CLx
Cd0H
Q)
0
cjn
wP,-
wE, .4
1.0.Nxw
<X;4.4
C)<m
0
0
0
0
0
.0o
00
.e-
Cd
0
0
E
cr
Ur.
0
-e
a0
Cd
0
W
bC
_W.E
Cd
In
*X W
Cd
C-01. 0
.0rQ
NOg-00
-4
1-
-
0)
00
c-i
II
r-i0d
I
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
I I I I I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
axW
.n
*~
X

ABO TYPES AND FERTILITY 29
male X 0 female matings are compared with 0 male X (A + B + AB) female mat-ings, the fetal loss is significantly higher among the compatible couples (x2 = 4.07,1 df, 0.05 > P > 0.025).
ABO Blood Types of Jewish WomenAs seen in Table 2, the blood-group frequencies differ markedly between the
Jewish and non-Jewish patients, but not between Jewish wives and their husbands.Furthermore, no distortion of blood-group distribution among Jewish women was
TABLE 4
DISTRIBUTION OF PREGNANCIES AMONG ABO MATING TYPES WITHNo APPARENT CAUSE FOR REDUCED FERTILITY
ins|. of Sterile eoTotal Mean Total FetalMatings No. of No.ilof ateiles No. of No. of No. of Loss
(M ale XFerale) MatingsM atingsProportion Preg- Preg- Fetal per Preg-nancies nancies Losses nancy
Compatible:AXA .............. 441 179 .4059 370 .8390 123 .3324AXAB............. 67 28 .4179 62 .9254 24 .3871BXBB.............. 59 31 .5254 34 .5763 11 .3235BXAB ............. 24 11 .4583 14 .5833 3 .2143ABXAB............ 13 5 .3846 14 1.0769 8 .5714OXA .............. 394 152 .3858 357 .9061 134 .3754OXB .............. 165 66 .4000 157 .9515 55 .3503OXAB ............. 67 23 .3433 69 1.0299 38 .5507OXO .............. 422 182 .4313 348 .8246 144 .4138
'Subtotal .......... 1,652 677 .4098 1,425 .8626 540 .3790
Incompatible:AXB .............. 184 70 .3804 176 .9565 67 .3807AXO .............. 422 176 .4171 336 .7962 116 .3452BXA .............. 172 66 .3837 164 .9535 65 .3963BXO .............. 164 70 .4268 151 .9207 61 .4040ABXA............. 65 24 .3862 51 .7846 13 .2549ABXB............. 25 9 .3600 25 1.0000 9 .3600ABXO............. 56 24 .4286 41 .7321 9 .2195
Sub total......... 1,088 439 .4035 944 .8676 340 .3602
Grand total. 2,740 1,116 .4073 2,369 .8646 880 .3715
x2 (I3df) . . ......... 3.61 . . 12.76 . ......... 30.12 .........
NOTE-Heterogeneity chi-square values are for columns under which they appear compared with the first column,"Matings."
noted when comparisons were made among fertile, subfertile, and sterile Jewishwomen (Table 5). Similar data for fertile Jewish husbands were not available forcomparison. However, the ABO blood-group distribution among these infertile menand women was quite consistent with those of published reports among Jewish pop-ulations, as shown in Table 6.The remarkable consistency in ABO blood-group distribution among populations
of fertile Jewish women who comprised the comparison group is shown in Table 7.

TABLE 5
ABO BLOOD TYPES OF FERTILE, SUBFERTILE, AND STERILE JEWISH WOMEN
BLOOD TYPE
A B AB 0
Total
No. % No. % No. % No. %
Fertile women .......... 5,273 41.1 2,040 15.9 895 7.0 4,620 36.0 12,828Subfertile women ....... 470 41.8 198 17.6 85 7.5 372 33.1 1,125Sterilewomen.......... 283 40.0 114 16.1 52 7.3 259 36.6 708
Fertile vs. subfertile women: X2(3df) = 4.36.Fertile vs. sterile women: X2(3df) = 0.42.Subfertile vs. sterile women: X2(3df) = 2.50.
TABLE 6
PUBLISHED REPORTS OF ABO BLOOD-GROUP DISTRIBUTION AMONG JEWS
Geographical A Total No. of No. of No. of No. of x2*Location Author No. A B AB 0 (3 df)
U.S.A ............ StarkandHenner, 349 135 53 17 144 7.451953 (38.68%/o) (15.19%) (4.87%) (41.26%)
Brooklyn, N.Y..... Wiener el al., 1930 500 200 84 29 187 2.38(40.00%) (16.80%) (5.80%) (37.40%)
Ohio ............. Rife, 1957 523 216 77 28 202 5.26(41.30%) (14.72%) (5.30%) (38.62%)
New York City.... Schiff, 1940 117 48 20 6 43 0.81(41.03%) (17.09%) (5.13%) (36.75%)
Brooklyn, N.Y..... MacMahonand 375 165 46 22 142 6.32Folusiak, 1958 (44.00%7) (12.3%) (5.9%) (37.9%)
New York City.... This study 3,666 1,526 611 261 1,268(41.6%) (16.7%) (7.1%/10) (34.6%)
* Comparisons are with the total Margaret Sanger Infertility Clinic population, both men and women, given in thelast line.
TABLE 7
ABO BLOOD-GROUP FREQUENCIES OF SAMPLE OF FERTILEJEWISH WOMEN IN NEW YORK CITY
BLOOD TYPE
HOSPITAL A B AB 0Total ._.
No. % No. % No. % No. %
Maimonides ................. 3,752 1,544 41.15 601 16.02 251 6.69 1,356 36.14Brookdale ................... 3,344 1,405 42.02 529 15.82 227 6.79 1,183 35.38Mt. Sinai .................... 1,875 765 40.80 284 15.15 134 7.15 692 36.91Brooklyn Jewish ............. 3,857 1,559 40.23 626 16.23 283 7.34 1,389 36.01
Total ................... 12,828 5,273 41.11 2,040 15.90 895 6.98 4,620 36.01

ABO TYPES AND FERTILITY
Rh Blood Groups
The Rh blood types, defined by testing with anti-Rh, serum, of patients registeredat the Sanger clinic are shown in Table 8. Distortions in frequency distribution arenot seen between spouses or between subfertile and sterile groups, nor are inter-action effects between ABO and Rh incompatibility seen in this population. Rhfrequencies among the Jewish women of this clinic population are consistent withthose of the fertile women of the comparison group. However, difference in Rhblood-group frequencies between Jewish and non-Jewish patients are quite marked(X2 = 24.52, 1 df, P < .0005).
DISCUSSION
The results of this investigation have failed to demonstrate any relationship be-tween ABO blood-group incompatibility and infertility. The basis for this conclu-sion comes from the following: (1) lack of difference of blood-group frequencies be-tween husbands and wives among couples with fertility problems, (2) absence of
TABLE 8
ABO AND RH INCOMPATIBILITY AMONG COUPLES WITHNo APPARENT CAUSE FOR INFERTILITY
SUBFERTILE STERILE
RELIGIONRh Rh Ttl
Rh Rh TotalComp. Incomp. Total Comp. Incomp.
Protestant:ABO Compatible 150 24 174 109 18 127ABO Incompatible 94 22 116 56 4 60
Total ............... 244 46 290 165 22 187
x2(1df) 1.40 2.21(0.3>P>0.2) (0.2>P>0.1)
Catholic:ABO Compatible 172 22 194 161 20 181ABO Incompatible . . . . . .....91596 94 15 109
Total .............. 263 27 290 255 35 290
x2(1df) ............. 2.86 0.47(0.1>P>0.05) (0.6>P>0.5)
Jewish:ABO Compatible 611 60 671 384 30 414ABO Incompatible 411 43 454 265 29 294
Total ............... 1,022 103 1,125 649 59 708
X'(1df) 0.09 1.54(0.8>P>0.7) (0.3>P>0.2)
31

SOLISH AND GERSHOWITZ
deviation of the various ABO mating-type frequencies from a random distribution,and (3) consistency in distribution of ABO blood type among sterile, subfertile, andfertile women drawn from presumably the same parent population (Jewish).
Of the 2,890 Protestant, Catholic, and Jewish subfertile couples in this study,1,723, or 60%, had achieved at least one pregnancy. When conceptions did occur,either before or after treatment, they were no more frequent in one ABO matingtype than another. Fetal losses, however, varied widely among the different matingtypes but were unrelated to ABO blood-group incompatibility of the parents (Table4). The rate of fetal loss per pregnancy is decidedly high in this population and prob-ably reflects not only the tendency for more accurate reporting of pregnancies bysubfertile patients who are keenly aware of basal body temperature changes anddelayed menstrual periods but also the tendency for relatively infertile women whohave had several abortions to seek treatment in an infertility clinic.
The relative proportions of compatible and incompatible matings are virtuallyunchanged from expectation in the subpopulations of this study. Among Catholicsand Jews, a slight nonsignificant increase in incompatible over compatible matingsis seen among the totally sterile couples, but a reverse trend is noted among Protes-tants (Table 3). These inconsistencies, in addition to those noted above for A X 0,B X 0, and AB X 0 matings and their reciprocals, further reduce the possibility ofa relationship, either prezygotically or postzygotically, between decreased fertilityand ABO blood-group incompatibility of the spouses. It is therefore unlikely thatsterility is one of the major selective forces involved in the maintenance of the ABOpolymorphism.
These results do not reveal an increase in frequency of ABO-incompatible matingsand therefore do not confirm the findings of Behrman et al. (1960). The differencesbetween these two studies may relate to, among other factors, the different popula-tions studied, the number of marital pairs involved in each study, and the choice ofcontrols. Although the ethnic composition of the population studied by Behrmanet al. is not stated, the blood-group frequencies of the control group of women, aswell as those of the infertile women presented, are unusual, leading to intrinsic diffi-culties in the analysis of these data. In that study, two groups of fertile controlwomen were presented. The difference in ABO blood-group distribution betweenthese two control groups of fertile women is highly significant (x2 = 14.17, 3 df,.005 > P > .001) and, in fact, is greater than the relatively small difference betweenthe infertile (Group I) and fertile (Group II) women selected from "the same generalgeographical, professional, income, ethnic, and racial groups" (x2 = 9.44, 3 df, .025 >P > .010). The method of selection of controls is therefore suspect, since no infor-mation is presented to preclude the possibility of ethnic stratification.By and large, published studies of the effect of ABO phenotypes of the mates on
fertility have examined differences in family size, irregularities in distribution ofblood groups among children in certain mother-child pairs, differences in rates offetal loss, or other data involving sources of difficulty referred to by Edwards (1957).By selecting for study a population that is not only at the lower end of the fertilityscale but that is also actively seeking help to overcome and correct this deficiency,a number of the problems encountered in other studies have been either eliminated
32

ABO TYPES AND FERTILITY
or greatly reduced. Errors in blood typing of infants, underreporting of abortionsand other prenatal losses, illegitimacy, contraceptive practices, and faulty copulatingtechniques are some of the difficulties which have been virtually eliminated in thisstudy of infertile couples who are under treatment. Furthermore, by defining indi-vidual religious groups for internal as well as external comparisons, heterogeneityof data due to differences inherent in religious practices is minimized. As an example,the customs of Orthodox Jewish couples regarding restrictive periods of the menstrualcycle for intercourse might be cited as a case in point. The choice of the Sanger clinicJewish population for study provided a group which from this point of view canbe considered homogeneous for most practical purposes.
Some possible limitations of these data should be mentioned. Only a small fractionof the total number of women in this study had reached the end of their childbearingperiod. Accordingly, the completed reproductive performance of these couples wasnot available. Lack of information relative to ABO genotypes rather than pheno-types and absence of subgroup data of A antigens may be responsible for some errors,the magnitude of which is difficult to assess. However, these errors are assumed tobe small. Blood-typing errors are believed to be negligible, since retyping in thislaboratory of more than 300 specimens originally typed by the New York HealthDepartment laboratories revealed no discrepancies. Effects due to missing blood-group data in 20% of couples are considered to be random and hence of little conse-quence in the final analysis.
The absence of positive evidence for ABO selection infertility in these data isnot necessarily negative evidence. Fisher (1930), Haldane (1942), and Boyd (1955)have called attention to the fact that selective advantages of the order of 0.1% to1% are sufficient to bring about regular and progressive evolutionary changes inlarge populations. Haldane (1942) estimated the selective advantage in the case ofblood-group genes to be less than 0.9%. The difficulties involved in measuring selec-tion of this order of magnitude are discussed by Boyd (1955). He calculated that108,530 individuals would be required to detect a heterozygote advantage of 2%.More recently, Neel and Schull (1968) have assessed the magnitude of sample sizesrequired to elicit differences in selective genetic advantage and in this context haveconcluded that "to date none of the so-called 'negative' studies on selection andgenetic traits has been adequate to detect (or exclude) even relatively large selectiveadvantages which might be associated with certain specific genotypes."
SUMMARY
The effect of ABO blood groups on fertility was studied in a population of 6,553subfertile married couples registered at the Infertility Clinic of the Margaret SangerResearch Bureau from 1947 to 1963. Among the 3,094 couples with no assigned causefor their infertility who were available for this study, there were no differences inABO blood-group distribution between husbands and wives. Three religious groups-Catholics, Protestants, and Jews-were represented in this population and wereanalyzed separately. The frequency of the different ABO mating types did not differsignificantly from expectation, and pregnancies or fetal losses, when they did occuramong these couples, were proportionately distributed between ABO-compatible and
33

SOLISH AND GERSHOWITZ
incompatible mating types. The frequencies of ABO blood groups among the Jewishwomen of this clinic population did not differ from a control sample of Jewish women,known to be fertile, nor from published frequency distributions of Jewish populationsin general. The Rh blood-group frequencies were also examined in this population.No distortion in Rh frequency distribution was observed between spouses nor be-tween fertile and subfertile groups of women, nor were interaction effects betweenABO and Rh incompatibility seen. From these results it is concluded that sterility,as such, does not seem to be one of the major selective factors concerned with main-tenance of the ABO polymorphism.
REFERENCES
ALLAN, T. M. 1953. ABO blood groups and human fertility. Brit. J. Prev. Soc. Med. 7:220-226.
BEHRMAN, S. J., BUETTNER-JANUSCH, J., HEGLAR, R., GERSHOWITZ, H., and TEW, W. L.1960. ABO(H) incompatibility as a cause of infertility: a new concept. Amer. J. Obstet.Gynec. 79:847-855.
BOYD, W. C. 1955. Detection of selective advantages of the heterozygotes in man. Amer. J.Phys. Anthrop. 13:37-52.
BRYCE, L. M., JAKOBowIcz, R., McARTHUR, N., and PENROSE, L. S. 1950. Blood groupfrequencies in a mother and infant sample of the Australian population. Ann. Eugen.15:271.
EDWARDS, J. H. 1957. A critical examination of the reported primary influence of ABOphenotype on fertility and sex ratio. Brit. J. Prev. Soc. Med. 11:79-89.
FISHER, R. A. 1930. The genetical theory of natural selection. Oxford Univ. Press, New York.HAGA, H. 1959. Studies on natural selection in ABO blood groups with special reference
to the influence of environmental changes upon the selective pressure due to maternal-fetal incompatibility. Jap. J. Hum. Genet. 4:1-20.
HALDANE, J. B. S. 1942. Selection against heterozygosis in man. Ann. Eugen. 11:333-342.HIRAIZUMI, Y. 1964. Prezygotic selection as a factor in the maintenance of variability.
Cold Spring Harbor Symp. Quant. Biol. 29:51-60.HIRSZFELD, L. 1934. Hauptprobleme der Blutgruppenforschung in den Jahren 1927-1933.
Ergebn. Hyg. Bakteriol. Immunitdtsforsch. exp. Ther. 15:54-218.HIRSZFELD, L. 1938. Les groupes sanguins a la lumiere de la science contemporaine. Sang
12: 465-483.HIRSZFELD, L., and ZBOROWSKI, H. 1925. Gruppenspezifische Beziehungen zwischen Mutter
und Frucht und elektive Durchlassigkeit der Placenta. Klin. Wschr. 4:1152-1157.JOHNSTONE, J. N. 1954. Heterospecific pregnancy. Brit. J. Prev. Soc. Med. 8:117-123.KIRK, R. L., KIRK, M., and STENHOUSE, N. S. 1953. Differential fertility between women
of blood groups 0 and A. Brit. J. Prev. Soc. Med. 7:1-8.KIRK, R. L., SHIELD, J. W., STENHOUSE, N. S., BRYCE, L. M., and JAKOBOWICZ, R. 1955.A further study of ABO blood groups and differential fertility among women in twoAustralian maternity hospitals. Brit. J. Prev. Soc. Med. 9:194-111.
MAcMAHON, B., and FOLUSIAK, J. C. 1958. Leukemia and ABO blood group. Amer. J.Hum. Genet. 10:287-293.
MATSUNAGA, E., and ITOH, S. 1953. Intrauterine selection by the ABO incompatibility ofmother and foetus. Proc. Jap. Acad. 29:399-403.
MATSUNAGA, E., and ITOH, S. 1958. Blood groups and fertility in a Japanese population,with special reference to intrauterine selection due to maternal-foetal incompatibility.Ann. Hum. Genet. 22:111-131.
MOURANT, A. E., KOPEC, A. C., and DOMANIEWSKA-SOBCZAK, K. 1958. The ABO bloodgroups. Blackwell, Oxford.
34

ABO TYPES AND FERTILITY 35
NEEL, J. V., and SCHULL, W. J. 1968. On some trends in understanding the genetics of man.Perspect. Biol. Med. 11:565-602.
REED, T. E., GERSHOWITZ, H., SONI, A., and NAPIER, J. 1964. A search for natural selec-tion in six blood group systems and ABH secretion. Amer. J. Hum. Genet. 16:161-179.
RIFE, D. C. 1957. Personal communication to Mourant et al. (1958).ROSENFIELD, R. E. 1955. A-B hemolytic disease of the newborn. An analysis of 1,480 cord
blood specimens with special reference to the direct antiglobulin test and to the group0 mother. Blood 10: 17.
SCHIFF, F. 1940. Racial differences in frequency of the "secretion factor." Amer. J. Phys.Anthropol. 27:255-262. Cited in Mourant et al. (1958).
STARK, G. J., and HENNER, J. 1953. Hematologic values in blood donors and the ABOblood group distribution in Tel Aviv. Harefuah 45:175-176. Cited in Mourant et al.(1958).
STEVENS, W. L. 1938. Estimation of blood-group frequencies. Ann. Eugen. 8:362-375.U.S. BUREAU OF THE CENSUS. 1966. Statistical abstract of the United States. 87th ed. U.S.
Government Printing Office, Washington.WATERHOUSE, J. A. H., and HOGBEN, L. 1947. Incompatibility of mother and foetus with
respect to iso-agglutinogen A and its antibody. Brit. J. Soc. Med. 1: 1-17.WIENER, A. S., LEDERER, M., and POLAYES, S. H. 1930. Studies in isohemagglutination. III.
On the heredity of the Landsteiner blood groups. J. Immunol. 18:201. Cited in Mourantet al. (1958).
ZUELZER, W. W., and KAPLAN, E. 1954. ABO heterospecific pregnancy and hemolyticdisease. A study of normal and pathologic variants. IV. Pathologic variants. Amer. J.Dis. Child. 88:319.