Embed Size (px)
Citation preview
Page 1/22
Mass Spectrometry Detection of Inhaled Drug inDistal Fibrotic LungTheresia Mikolasch ( [email protected] )
University College London https://orcid.org/0000-0002-9417-1286Eunice Obella
GSK: GlaxoSmithKline PlcMitra Vahdati-Bolouri
GSK: GlaxoSmithKline PlcJosie Morrell
GSK: GlaxoSmithKline PlcEmily Jarvis
GSK: GlaxoSmithKline PlcYi Cui
GSK: GlaxoSmithKline PlcAnthony Cahn
GSK: GlaxoSmithKline PlcRebecca Terry
GSK: GlaxoSmithKline PlcJagdeep Sahota
UCL: University College LondonRicky Thakrar
UCLH: University College London Hospitals NHS Foundation TrustPeter Marshall
GSK: GlaxoSmithKline PlcJoanna PORTER
UCL: University College London
Research
Keywords: MALDI-MS imaging, Transbronchial cryobiopsy, drug distribution, interstitial �brosis.
Posted Date: May 20th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-515610/v1
Page 2/22
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 3/22
AbstractBackground
Currently the only available therapies for �brotic Interstitial Lung Disease are administered systemically,often causing signi�cant side effects. Inhaled therapy could avoid these but to date there is no evidencethat drug can be effectively delivered to distal, �brosed lung. We set out to combine mass spectrometryand histopathology with rapid sample acquisition using transbronchial cryobiopsy to determine whetheran inhaled drug can be delivered to �brotic, distal lung parenchyma in participants with Interstitial LungDisease.
Methods
Patients with radiologically and multidisciplinary team con�rmed �brotic Interstitial Lung Disease wereeligible for this study. Transbronchial cryobiopsies and endobronchial biopsies were taken from �veparticipants, with Interstitial Lung Disease, within 70 minutes of administration of a single dose ofnebulised ipratropium bromide. Thin tissue cryosections were analysed by Matrix Assisted LaserDesorption/Ionization-Mass Spectrometry imaging and correlated with histopathology. The remainder ofthe cryobiopsies were homogenised and analysed by Liquid Chromatography – tandem MassSpectrometry.
Results
Drug was detected in proximal and distal lung samples from all participants. Fibrotic regions wereidenti�ed in research samples of four of the �ve participants. Matrix Assisted LaserDesorption/Ionization-Mass Spectrometry imaging showed co-location of ipratropium with �broticregions in samples from three participants.
Conclusions
In this proof of concept study, using mass spectrometry, we demonstrate for the �rst-time that an inhaleddrug can deposit in distal �brotic lung parenchyma in patients with Interstitial Lung Disease. Thissuggests that drugs to treat pulmonary �brosis could potentially be administered by the inhaled route.
Trial Registration
A prospective clinical study approved by London Camden and Kings Cross Research Ethics Committeeand registered on clinicaltrials.gov (NCT03136120)
BackgroundThe interstitial lung diseases (ILDs) are a group of over 200 lung disorders that are characterised byinterstitial �brosis, and lead to declining lung function, respiratory failure and ultimately death. The most
Page 4/22
severe �brotic (f)ILD is Idiopathic Pulmonary Fibrosis (IPF).
Two oral drugs, pirfenidone and nintedanib, are licensed for the treatment of IPF and have now beenshown to have bene�ts in other fILDs (1) but both have limiting adverse effects. Inhaled therapy for ILDoffers the advantage of drug delivery direct to the lung, thereby minimising systemic exposure andassociated side effects. However, lung deposition, absorption and local therapeutic response may bealtered in the �brotic lung (2).
Assessment of lung drug levels using bronchoscopic lavage has become a critical component of inhaleddrug development but lacks spatial information of the site or region of deposition. The advent oftransbronchial cryobiopsy (TBC) to sample the lung parenchyma for diagnosis of ILD allows importanthistological information of inhaled drug distribution using a minimally invasive bronchoscopic technique(3). TBC potentially also allows more rapid lung tissue sampling following drug inhalation, compared totraditional surgical lung biopsies therefore shortening the time during which the inhaled drug can becleared from the lung before analysis. Furthermore, participants are not subject to mechanical ventilationwhich could theoretically alter inhaled drug distribution in surgical participants.
Liquid Chromatography - tandem Mass Spectrometry (LC-MS/MS) is traditionally used for the analysis ofhomogenised tissue samples and therefore any spatial information regarding drug distribution within thetissue is lost. In contrast, Matrix Assisted Laser Desorption Ionisation – Mass Spectrometry (MALDI-MS)imaging allows detection and characterisation of molecules from tissue (4-15) and supports the spatialvisualisation of drug distribution in tissue samples. Analysing the same TBC biopsy with a combinationof LC-MS/MS, MALDI-MS imaging and histopathology can therefore allow minimally invasiveassessment of drug distribution within the diseased �brotic lung.
Fehniger et al (15) have previously demonstrated inhaled drug distribution using MALDI-MS imaging inthe proximal airways of patients with suspected airway obstruction or tumours. Ipratropium readilyionises and the MS/MS fragmentation pattern produces two major fragment ions (at m/z 166.0 and123.9, (Online Data Supplement Figure E1).
In this clinical study, having carried out a single pre-clinical enabling study, we combined, for the �rst time,rapid distal sample acquisition using TBC with the mass spectrometry modalities of LC-MS/MS andMALDI-MS imaging, together with histopathology to demonstrate inhaled drug delivery to �brotic, distalhuman lung parenchyma in participants with diagnosed ILDs. Whilst this study was designed as a proofof concept, with a low participant number (n=5), we are able to present con�rmation that inhaled drugtherapy is a feasible route of administration for �brotic ILD, which could avoid the signi�cant systemicside effects of current oral therapy. To our knowledge this is also the �rst time that TBC has been used intranslational research.
MethodsPre-Clinical Support Study in Wistar Han rats
Page 5/22
All animal studies were ethically reviewed and carried out in accordance with UK Animals (Scienti�cProcedures) Act 1986, European Directive 2010/63/EU and the GSK Policy on the Care, Welfare andTreatment of Laboratory Animals.
A scaled dose of ipratropium bromide, equivalent to the clinical dose, was nebulised to male Wistar ratsfor 5 minutes. Terminal lung samples were taken at varying time points up to 65 minutes post-dose and 5mm ex-vivo biopsies were embedded into material suitable for MALDI-MS imaging.
For further details of the pre-clinical animal work please see Online dataSupplement.
Clinical Study
We conducted a prospective clinical study approved by London Camden and Kings Cross Research EthicsCommittee and registered on clinicaltrials.gov (NCT03136120) at University College London Hospital(UCLH), London, United Kingdom and sponsored by GlaxoSmithKline. Participants over the age of 18 withsuspected ILD and requiring TBC for further diagnostic assessment, as determined by the ILDmultidisciplinary team, were eligible to participate (see Online Data Supplement for fullexclusion/inclusion criteria). Seven participants were enrolled between November 2017 and November2018.
All participants received a single dose of 500 mcg nebulised ipratropium bromide (Ivax Pharmaceuticals,London, UK) 1 hr prior to bronchoscopy. TBCs for diagnosis were taken ahead of the additional (one ortwo) TBC research samples. Up to three endobronchial forceps biopsy samples were also taken aspositive controls to con�rm drug inhalation by the participant (see Online Data Supplement for fullprocedural and biopsy collection details).
Liquid Chromatography – Tandem Mass Spectrometry (LC-MS/MS) analysis
Following sectioning of biopsy samples for MALDI-MS imaging, the remainder of the biopsy sampleswere analyzed by LC-MS/MS for con�rmation of drug presence. For more details see Online DataSupplement.
MALDI MSI analysis
For experimental conditions and more details see Online Data Supplement.
In the MALDI-MS imaging experiments the ipratropium cation was detected and will be referred to asipratropium or drug. Predetermined speci�c mass transitions for ipratropium (m/z 332.2-166.0 and 332.2-123.9) were utilised. Following smoothing and baseline correction, a signal to noise threshold ratio of 3:1was applied to both fragment ions (166.0 and 123.9) for detection of ipratropium. A spatial resolution ofeither 30, 100 or 200 µm was utilised and the signal for ipratropium was displayed using a colour codedion density map.
Histopathology
Page 6/22
Biopsy sections were stained with haematoxylin and eosin (H&E) following standard histologicalprocedures [16]. Images were captured digitally and scanned at either 20× or 40× magni�cation (AperioScanscope CS, Leica Microsystems, Milton Keynes, UK).
ResultsClinical Study
Seven participants were enrolled of whom �ve completed the trial providing six TBC samples rangingfrom 4 to 6 mm2 in size and fourteen endobronchial biopsy samples ranging from 0.75 to 3 mm2 in size.TBC samples were taken within 70 minutes of the end of ipratropium nebulisation.
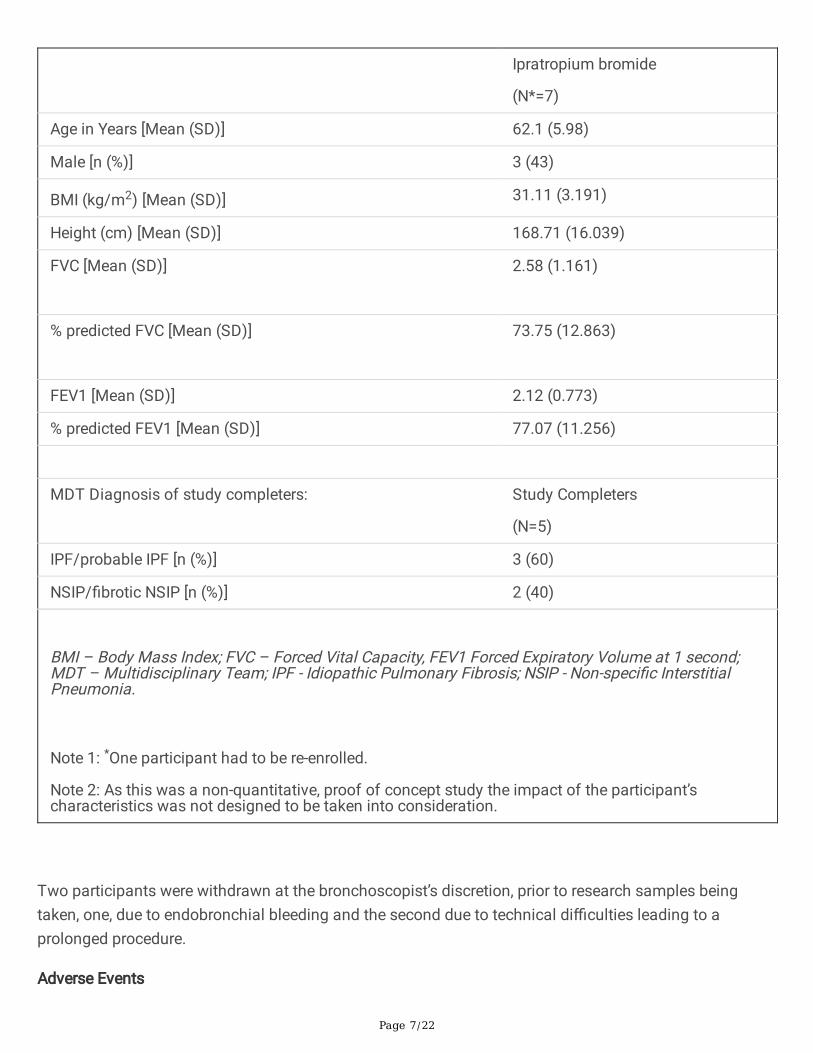
Participants’ characteristics are summarized in Table 1.
Page 7/22
Ipratropium bromide
(N*=7)
Age in Years [Mean (SD)] 62.1 (5.98)
Male [n (%)] 3 (43)
BMI (kg/m2) [Mean (SD)] 31.11 (3.191)
Height (cm) [Mean (SD)] 168.71 (16.039)
FVC [Mean (SD)]
2.58 (1.161)
% predicted FVC [Mean (SD)]
73.75 (12.863)
FEV1 [Mean (SD)] 2.12 (0.773)
% predicted FEV1 [Mean (SD)] 77.07 (11.256)
MDT Diagnosis of study completers: Study Completers
(N=5)
IPF/probable IPF [n (%)] 3 (60)
NSIP/�brotic NSIP [n (%)] 2 (40)
BMI – Body Mass Index; FVC – Forced Vital Capacity, FEV1 Forced Expiratory Volume at 1 second;MDT – Multidisciplinary Team; IPF - Idiopathic Pulmonary Fibrosis; NSIP - Non-speci�c InterstitialPneumonia.
Note 1: *One participant had to be re-enrolled.
Note 2: As this was a non-quantitative, proof of concept study the impact of the participant’scharacteristics was not designed to be taken into consideration.
Two participants were withdrawn at the bronchoscopist’s discretion, prior to research samples beingtaken, one, due to endobronchial bleeding and the second due to technical di�culties leading to aprolonged procedure.
Adverse Events

Page 8/22
The adverse events (AE) reported for the study are presented in Table 2.
Three participants in this study had serious AEs reported namely pneumothorax (n=2) and malaise (n=1).
Table 2: Summary of Adverse Events.
Preferred Term Ipratropium Bromide
(N=7)
Any event, n (%) 7 (100)
Procedural haemorrhage1 5 (71)
Procedural pneumothorax 2 (29)
Cough 1 (14)
Dry throat 1 (14)
Constipation 1 (14)
Malaise 1 (14)
Musculoskeletal chest pain 1 (14)
1Bleeding (procedural haemorrhage) is an expected adverse event associated with biopsy procedures.In this study, for one participant the procedure was stopped before biopsies due to bleeding. For allother participants, bleeding was mild and managed as per UCLH routine procedure.
Drug Detection by LC-MS/MS
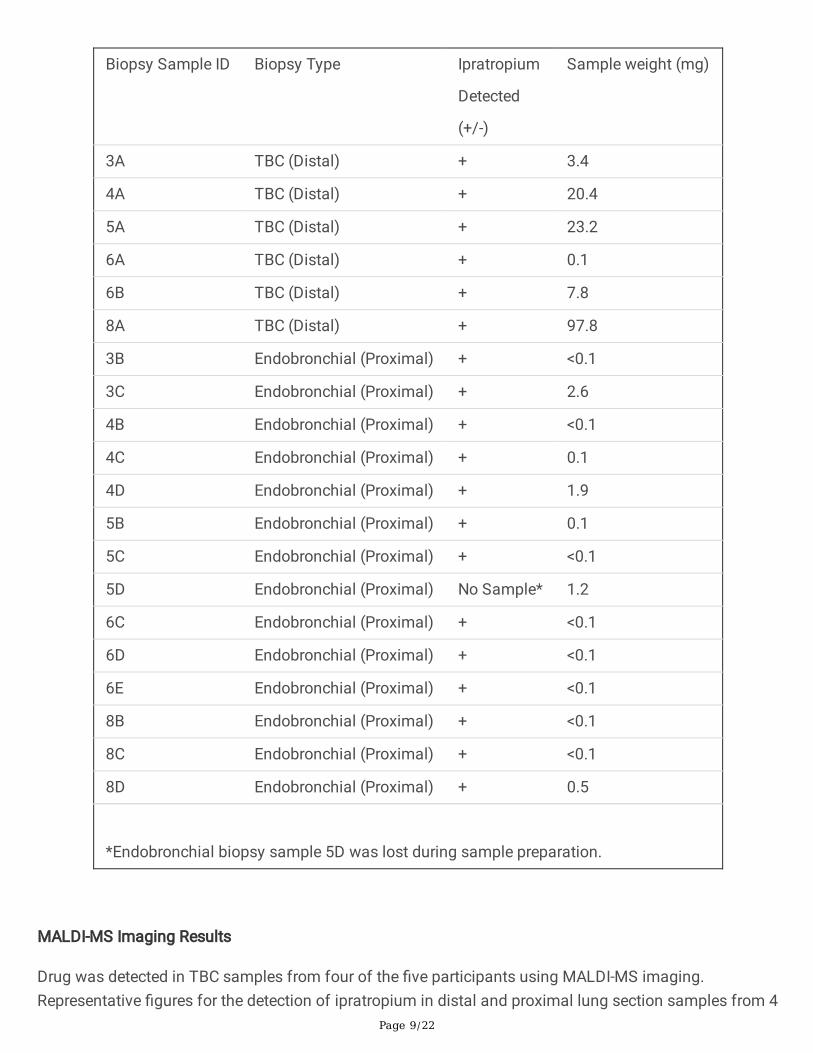
LC-MS/MS was carried out. Ipratropium was detected in all six TBC samples tested (Table 3). Noquanti�cation data is available due to insu�cient TBC or endobronchial control material being availableto prepare calibration standards. In addition, an identical liquid volume was used to produce homogenatefor each sample irrespective of their differing weights (to aid detection).
Drug was detected by LC-MS/MS in thirteen endobronchial biopsy samples tested.
Table 3 – Summary of ipratropium detection by LC-MS/MS
Page 9/22
Biopsy Sample ID Biopsy Type Ipratropium
Detected
(+/-)
Sample weight (mg)
3A TBC (Distal) + 3.4
4A TBC (Distal) + 20.4
5A TBC (Distal) + 23.2
6A TBC (Distal) + 0.1
6B TBC (Distal) + 7.8
8A TBC (Distal) + 97.8
3B Endobronchial (Proximal) + <0.1
3C Endobronchial (Proximal) + 2.6
4B Endobronchial (Proximal) + <0.1
4C Endobronchial (Proximal) + 0.1
4D Endobronchial (Proximal) + 1.9
5B Endobronchial (Proximal) + 0.1
5C Endobronchial (Proximal) + <0.1
5D Endobronchial (Proximal) No Sample* 1.2
6C Endobronchial (Proximal) + <0.1
6D Endobronchial (Proximal) + <0.1
6E Endobronchial (Proximal) + <0.1
8B Endobronchial (Proximal) + <0.1
8C Endobronchial (Proximal) + <0.1
8D Endobronchial (Proximal) + 0.5
*Endobronchial biopsy sample 5D was lost during sample preparation.
MALDI-MS Imaging Results
Drug was detected in TBC samples from four of the �ve participants using MALDI-MS imaging.Representative �gures for the detection of ipratropium in distal and proximal lung section samples from 4
Page 10/22
participants are shown in Figures 2 and 3 respectively. The circled regions in Figure 2 (and all regions inFigure 3) represent the drug foci regions meeting the selection criteria (see Online Data Supplement) forthe positive identi�cation and detection of ipratropium.
TBC (Distal Lung) MALDI-MS Imaging
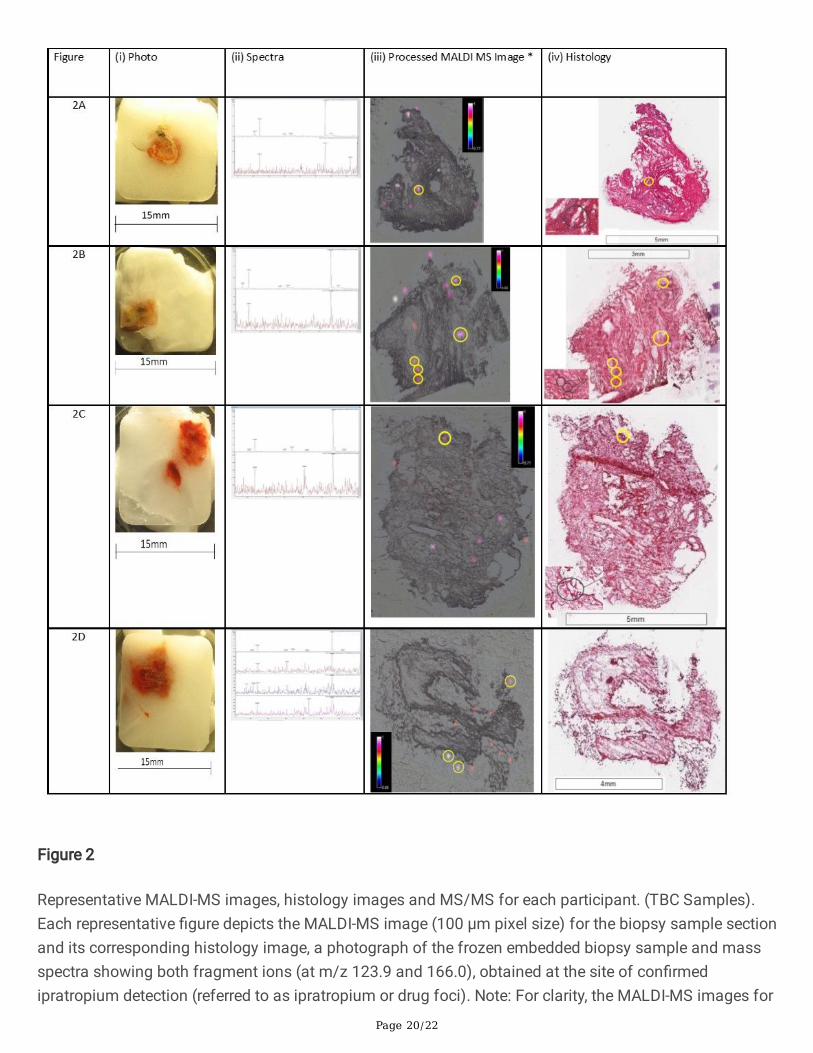
Ipratropium was detected in TBC sections as either a single foci or multiple foci using MALDI-MS imaging(Figure 2). The sample shown in Figure 2B (iii) contains �ve ipratropium foci. Three of these foci areadjacent to each other and appear to be co-located with an airway.
Ipratropium loci were observed to localise in the same region in consecutive biopsy sections (Figure 4iand 4ii) suggesting an alignment through the z-plane.
Co-location of MALDI-MS Imaging and Histology in TBC
Fibrotic regions were identi�ed in biopsies of four of the �ve participants as indicated by coalescingareas of poorly cellular eosinophilic �brillar material (interpreted as collagen). Combining the MALDI-MSimages and histology demonstrated co-location of ipratropium with �brotic regions in the TBCs of threeof the four participants with �brosis.
Whilst the number of drug foci within the TBC sections was low, there were examples from threeparticipants, Figures 2A (iv), 2B (iv) and 2C (iv) where the drug foci were shown to co-locate with areas of�brosis. This indicates that for these three participants, ipratropium bromide could be deposited inregions of the distal lung where �brosis was also con�rmed.
In TBC sections from two participants, drug foci were present within abnormal �brotic areas (Figure 4A-D), possibly co-located with small airway, however, low resolution of the image does not allow a fullhistological interpretation.
One participant (diagnosed with non-speci�c interstitial pneumonia) did not have abnormal �brotic areasobserved in the research sample, although ipratropium was successfully detected in the TBC samplefrom their distal lung.
MALDI-MS Imaging Results for the endobronchial biopsy (proximal lung)
Endobronchial biopsy samples were taken as a control to con�rm drug inhalation by the participant. Thelevels of ipratropium were expected to be higher in the proximal airways than in the distal lung.
Ipratropium was detected in at least one endobronchial biopsy sample for each of the participants, seeFigure 3 and Table 4. The highest signal intensity and greatest number of drug foci were observed inendobronchial samples Figure 3A (iii) and 3C (iii).

Page 11/22
Table 4 - Summary of average drug detection rates per study sample.
Biopsy
Sample
ID
Biopsy Type Number ofSectionsAnalysed
Number of Sectionswith Drug Observed
%Success
Average %
Success forendobronchialsamples
4A Transbronchial 25 5 20
4B Endobronchial 26 5 19
4C Endobronchial 12 8 67
4D Endobronchial 8 3 38 34.8
5A Transbronchial 14 1 7
5B Endobronchial 8 6 75
5C Endobronchial 8 8 100
5D Endobronchial 4 4 100 90.0
6A Transbronchial 12 1 8
6B Transbronchial 12 0 0
6C Endobronchial 9 1 11
6D Endobronchial 11 4 36 23.5*
6E† Endobronchial 7 0 0 † 25 †
8A Transbronchial 11 4 36
8B Endobronchial 7 1 14
8C Endobronchial 9 2 22
8D Endobronchial 5 3 60 28.6
*Average success rate while incorporating sample 6E is 23.5%.
† Due to issues we had with generating suitable sections from sample 6E for MALDI-MS imaging wehave recalculated the average success for sample 6 excluding the data from biopsy E, updated resultis 25%.
Comparison of drug detection in samples from distal (transbronchial) and proximal (endobronchial) lung.

Page 12/22
The non-statistical, non-quantitative comparison reported here was conducted to demonstrate that moredrug was detected in the proximal regions of the lung compared to the distal regions. Inhaled drugsemitted from a device generating polydisperse particle sizes are more likely to deposit higher amounts ofdrug in the proximal lung and larger airways than the distal lung and alveoli [17].
The signal for the fragment ions of ipratropium were found to be of greater intensities in endobronchialsamples relative to the TBC samples (Figure 3). Table 4 summarises the average detection success rateby MALDI-MS imaging per biopsy sample. The drug foci were also greater in number across theendobronchial biopsy samples compared to the TBC samples. In addition, except for TBC sample 8A, theproportion of sample sections where drug was detected per biopsy was greater for endobronchial biopsysamples (range 23.5 – 90%) compared to the TBC samples (range 7 –36%). For sample 8 (diagnosedwith NSIP), the average detection frequencies for the TBC and endobronchial biopsies were similar at36% and 28.6%, respectively.
DiscussionHere we report the �rst ever successful detection and localisation of inhaled drug in the distal lung ofhistologically con�rmed �brotic lung parenchyma in participants with a clinical diagnosis of �brotic ILD.This was achieved through the combination of TBC, LC-MS/MS, MALDI-MS imaging and histopathology.
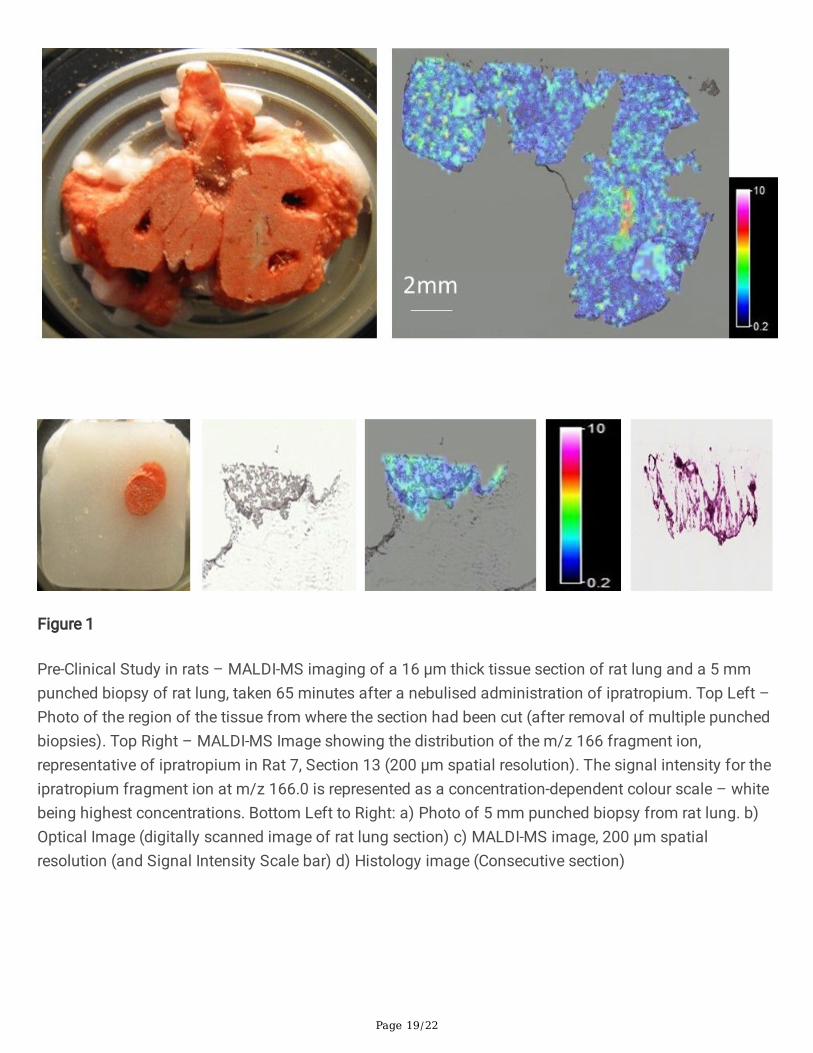
A scaled preclinical study was initially conducted in rats to optimise assay conditions, due to theanticipated challenges with respect to the detection of a single clinical dose of ipratropium in relativelysmall lung biopsy samples. The preclinical study allowed sample handling methods and detection limitsof ipratropium in rat lung samples (similar in size to human cryobiopsy samples) to be assessed by LC-MS/MS and MALDI-MS imaging. Widespread and even distribution of ipratropium was observed, seeOnline Data Supplement, in both rat lung sections and equivalent sized biopsies to those expected fromTBC.
A total of seven participants were dosed with ipratropium bromide, with �ve participants providing bothTBC and endobronchial samples. LC-MS/MS analysis demonstrated the presence of drug in allparticipants’ TBCs, suggesting that ipratropium was able to deposit in the distal lung, the area that ismost affected in IPF.
Drug aerosol particle size by medical nebuliser is polydisperse, therefore containing a mix of differentparticle sizes. Particle size was not measured as we did not perform any drug delivery quanti�cation.According to product literature the combination of a Porta Neb compressor (Phillips Respironics,Amsterdam, Netherlands) running at 6 L/min with a SideStream aerosolising chamber (Respironics,Tangmere, UK) achieves a mass median diameter of < 5 µm in 80% of droplets generated. Salbutamolnebulised using the same compressor/nebuliser con�guration gave a mean mass median aerodynamicdiameter (MMAD) of 2.2 µm (SD 0.4) and a mean geometric standard deviation 3.45 µm (SD 1.1) (18).Aerosol droplet size in�uences the location of particle deposition and alveolar deposition peaks at about1.5 µm (19). It was therefore reasonable to assume that the compressor/nebuliser con�guration would
Page 13/22
create aerosol droplets of su�ciently small size to reach the target tissue. Due to insu�cient TBC orendobronchial control material being available to prepare calibration standards no drug quanti�cationmeasurements were made in this study.
Using LC-MS/MS requires homogenisation of the tissue hence results in a loss of anatomical and spatialinformation but allows the analysis of a larger sample and thereby can provide increased sensitivity.Conversely, MALDI-MS imaging provides spatial and regional information but is limited by the smallsampling size. Due to the small sampling size used (typically 100 µm x 100 µm) achieving su�cientsensitivity in the clinical study proved di�cult and LC-MS/MS analysis was used to con�rm drug waspresent in biopsies. Although current MALDI-MS imaging sensitivity was generally unable to fully pro�ledrug distribution in the TBCs, it was su�ciently sensitive to detect ipratropium in certain foci. Therequirement for the coincident presence of both fragment ions in the MALDI-MS imaging data, at a signalto noise ratio threshold of 3:1 or greater as the threshold for the identi�cation of ipratropium to bepositively recorded as well as the fact that the drug in the remaining biopsy fraction was detected by LC-MS/MS, provides increased con�dence that ipratropium was detected by MALDI-MS imaging.
MALDI-MS imaging detected ipratropium in four participants’ TBC samples (Fig. 2), three of whom alsohad �brotic regions identi�ed within the TBC research samples. In some instances, e.g. Figure 3D (iii), thefoci of ipratropium are not directly overlying the biopsy sample. This is likely due todiffusion/delocalisation of ipratropium from the periphery of the sample section during the samplefreezing process within the embedding material and/or during the thaw-mounting process of the samplesection onto the glass slide in preparation for MALDI-MS imaging. It is the authors’ opinion that this stillconstitutes the positive identi�cation/detection of ipratropium in the sample section.
In all �ve participants, MALDI-MS imaging detected ipratropium in the endobronchial samples. Moreipratropium foci and higher ipratropium signal intensities were detected in the proximal lung samplesthan distal lung samples even though proximal lung samples were smaller in size. This was expected, asin general inhaled drugs emitted from a device generating polydisperse particle sizes are more likely todeposit higher amounts of drug in the proximal lung and larger airways than the distal lung and alveoli[17]. In addition, with only 10–30% of nominal dose expected to reach the lung (due to the e�ciency ofthe nebuliser device) [20] and the estimated surface area of the human lung varying between 50 to 75 m2
[21], it is expected to be challenging to detect drug deposited in 5 mm2 distal lung TBC samples and ifdetected, would likely be close to the limit of the detection of any MALDI-MS imaging technique.
This proof of concept study has several limitations. There was a difference between the demonstrateddetection of ipratropium in the pre-clinical study versus the clinical study, despite using what wasconsidered a scaled dose. The human ipratropium dose of 500 mcg was converted to 0.5 mcg/g in lungtissue by assuming a human lung weight of 1000 g. A similar assumption was made for rat lung weightof 1.5 g and the 0.5 mcg/g lung tissue dose was matched between the species. As this was anexperimental study, we were not in a position to quantify the rat to human “disconnect”; we do not havesystemic (plasma) data or quanti�ed human lung concentrations. Indeed, the pre-clinical work was only
Page 14/22
performed to allow study sample workup and methodologies to be put in place. Possible explanations forthe observed “disconnect” could be the effect of impaired lung function of the participants, pulmonaryclearance mechanisms, or a degree of wash out of drug due to the administration of topical anaestheticduring the bronchoscopy. In the pre-clinical rat study, the lung levels for ipratropium appeared to beconsistent throughout the 5–65 minute time period. We assumed that this would be the same in humans,but this may not be the case. The delay of up to 60–70 minutes before biopsy may have contributed tosome dissolution and absorption of the ipratropium in the airways. However, whilst topically active,ipratropium as a quaternary ammonium compound, is poorly absorbed [22] but has a reported shortsystemic half-life of 1.6 hrs [23]. Exact correlation with the underlying histopathology was sometimesconfounded due to delocalization of drug, presumably during sample processing, together withlimitations to the histological assessments resulting from the use of the embedding material and sectionthickness needed for sample preparation. While we were able to prove that inhaled ipratropium doesdeposit in distal, �brosed lung in participants with ILD, we were not always able to show the exactlocation within the biopsy samples with con�dence. As we were operating close to the limits of detectionof the current instrument (MALDI), we could not show the potential drug distribution. Therefore, in furtherstudies we would recommend use of an increase in drug dose and/or greater MALDI-MS sensitivity.
The advent of TBC has brought translational research opportunities by allowing minimally invasive andrapid access to lung interstitial tissue and therefore the potential to study relatively large distal lungbiopsies without the need for a Video Assisted Thoracoscopic Surgery or open surgical approach. Afurther advantage over surgical acquisition of samples is the fact that participants are self-ventilatingthroughout the procedure which in this study should lead to a more physiological drug distribution than inventilated participants. Time from nebulisation to biopsy is also reduced as the participant can benebulised in the bronchoscopy suite directly before receiving sedation.
In this proof of concept study, we are able to present con�rmation that inhaled drug therapy is a feasibleroute of administration for �brotic ILD. However, further work is needed to encompass the in�uences ofthe varying physicochemical properties of different pharmaceutical formulations to be used in IPF tooptimise distal delivery. Similarly, development of an inhaled therapy would also require anunderstanding and evaluation of drug clearance particularly since �brotic interstitium between thealveolar epithelium and the blood supply would likely impair drug penetration into the blood vessels.
Future studies using this unique and the powerful combination of TBC and Mass Spectrometry have thepotential to evaluate the ability of an inhaled, or systemic dosed molecule to reach the lung, and may inparticular shorten the early clinical phase of an inhaled drug where target engagement is important todemonstrate early in development.
ConclusionWe have demonstrated in this study for the �rst-time using LC-MS/MS and MALDI-MS imaging that adrug taken via the inhaled route can deposit in distal �brotic lung tissues. All participants had a �brotic

Page 15/22
ILD with overall moderately impaired lung function. To our knowledge, this is the �rst study to directlyassess the deposition of non-radiolabeled drugs to the distal lungs of participants with ILDs andcorrelating histology with drug deposition in these participants.
Ipratropium was detected in all TBC and endobronchial samples tested indicating that drug depositionreached the peripheral lung, a region that is most affected in IPF.
This study, therefore, in addition to the study by Usmani et al, 2018 [17] suggests that ILD participantswith established �brosis can bene�t from treatments administered by the inhaled route.
AbbreviationsAEs adverse events
f �brotic
H&E haematoxylin and eosin
ILD interstitial lung disease
IPD idiopathic pulmonary �brosis
LC-MS/MS Liquid Chromatography - tandem Mass Spectrometry
MALDI-MS Matrix Assisted Laser Desorption Ionisation – Mass Spectrometry
TBC Transbronchial cryobiopsy
DeclarationsEthics approval and consent to participate
This study was approved by London Camden and Kings Cross Research Ethics Committee and registeredon clinicaltrials.gov (NCT03136120). All patients gave informed consent
Consent for publication
Not applicable.
Availability of data and materials
Within 6 months of this publication, anonymized individual participant data, the annotated case reportform, protocol, reporting and analysis plan, data set speci�cations, raw dataset, analysis-ready datasetand clinical study report will be available for research proposals approved by an independent review
Page 16/22
committee. Proposals should be submitted to www.clinicalstudydatarequest.com. A data accessagreement will be required.
Funding
This work was undertaken at University College London Hospital/ University College London whoreceived a proportion of funding from the Department of Health’s NIHR Biomedical Research Centre’sfunding scheme. Funding for this study was also provided by GlaxoSmithKline (GSK Study ID: 205053;NCT: 03136120).
JCP received funding as a Medical Research Council New Investigator and from Breathing Matters.
Competing interests
TAM, JCP, JS and RT were recipients of research funding by GlaxoSmithKline (GSK).
Authors Contributions
TAM, EO, EJ, AC, JM, PM and JCP designed the study. TAM, RT and JS performed the clinical study. PMand JM performed the MALDI-MS imaging and LC-MS/MS analysis. RLT performed histopathologicalanalysis. EJ was the study statistician. TAM and PM drafted the manuscript and all authors approved the�nal version.
Authors' information
TAM: Respiratory Physician and Interventional Bronchoscopist who, with RT, established CLB at UCLH,and the �rst CLB service in UK.
RT: Respiratory Physician and Interventional Bronchoscopist who, with TAM, established CLB at UCLH,and the �rst CLB service in UK.
JCP: Clinical Lead of the NHS National ILD Service at UCLH
PSM: MALDI Mass Spectrometry Analyst who performed the Imaging experiments at GSK in UK.
EO: GSK Scientist who co-designed the study, authored the protocol/Study report and provided scienti�coversight of study
MVB: GSK Early Development Leader for the �brosis discovery performance unit at the time
JM: DMPK Investigator at GSK who, contributed to the design of the study and performed the LC-MS/MSanalysis.
RLT: Pathologist working in Non-Clinical Safety, GSK UK
Acknowledgements
Page 17/22
The Authors would like to thank Christoph Nordmann at Bruker Daltonics, Bremen, Germany and NigelDeeks (DMPK, GSK Research, UK) for their invaluable technical assistance.
References1. Flaherty KR, Wells AU, Cottin V, Devaraj A, Walsh SLF, Inoue Y, Richeldi L, Kolb M, Tetzlaff K,
Stowasser S, Coeck C, Clerisme-Beaty E. Nintedanib in Progressive Fibrosing Interstitial LungDiseases. N Engl J Med 2019; 381(18): 1718-1727.
2. Bannerjee D, Khair OA, Honeybourne D. Impact of sputum bacteria on airway in�ammation andhealth status in clinical stable COPD. Eur Respir J 2004; 23: 685-692.
3. Troy LK, Grainge C, Corte TJ, Williamson JP, Vallely MP, Cooper WA, Mahar A, Myers JL, Lai S,Mulyadi E, Torzillio PJ, Phillips MJ, Jo HE, Webster SE, Lin QT, Rhodes JE, Salamonsen M, Wrobel JP,Harris B, Don G, Wu PJC, Ng BJ, Oldmeadow C, Raghu G, Lau EMT. Diagnostic accuracy oftransbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): a prospective,comparative study. The Lancet Respiratory Medicine 2020; 8 (2): 171-181.
4. Prideaux P, Stoeckli M. Mass Spectrometry imaging for drug distribution studies. J. Proteomics 2012;75: 4999-5013.
5. Solon EG, Schweitzer A, Stoeckli M, Prideaux B. Autoradiography, MALDI-MS, and SIMS-MS Imagingin Pharmaceutical Discovery and Development. The AAPS Journal 2010; 12(1): 11-26.
�. Trim P, Henson C, McEwen A, Snel MF, Claude E, Marshall PS, Clench M. Matrix-assisted laserdesorption/ionisation – ion mobility-mass spectrometry imaging of vinblastine in whole body tissuesections. Rapid Commun. Mass Spectrom 2008; 22(10): 1503-1509.
7. Marshall PS, Toteu-Djomte V, Bareille P, Perry H, Biggadike K. Correlation of skin blanching andpercutaneous absorption for glucocorticoid receptor agonists by Matrix-assisted laserdesorption/ionisation mass spectrometry imaging. Chem. 2010; 82(18): 7787-7794.
�. Tomlinson L, Hassall D, Fuchser J, Baumert M, West A, Marshall PS. Using a single, high massresolution mass spectrometry platform to investigate ion suppression effects observed during tissueimaging. Rapid Commun. Mass Spectrom 2014; 28 (9): 995-1003.
9. Goodwin RJA. Sample Preparation for Mass Spectrometry Imaging: Small Mistakes can lead to BigConsequences. J. Proteomics 2012; 75: 4893-4911.
10. Weaver EM, Hummon AB. Imaging Mass Spectrometry: From Tissue Sections to Cell Cultures. Adv.Drug Delivery Rev. 2013; 65: 1039-1055.
11. Cobice DR, Goodwin RJA, Andren PE, Nilsson A, Mackay CL, Andrew R. Future Technology Insight:Mass Spectrometry Imaging as a Tool in Drug Research and Development. Br. J. Pharmacol. 2015;172: 3266-3283.
12. Amstalden van Hove ER, Smith DF, Heeren RMA. A Concise Review of Mass Spectrometry Imaging. J.Chromatogr. A. 2010; 1217: 3946-3954.
Page 18/22
13. Nilsson A, Goodwin RJA, Shariatgorji M, Vallianatou T, Webborn PJH, Andren PE. Mass SpectrometryImaging in Drug Development. Anal. Chem. 2015; 87: 1437-1455.
14. Schulz S, Becker M, Groseclose MR, Schadt S, Hopf C. Advanced MALDI MS imaging inpharmaceutical research and drug development. Curr. Opin. Biotechnol. 2019; 55: 51-59.
15. Fehniger TE. Direct Demonstration of Tissue Uptake of an Inhaled Drug: Proof-of-Principle Studyusing Matrix-Assisted Laser Desorption Ionization Mass Spectrometry Imaging. Anal. Chem. 2011;83: 8329-8336.
1�. Lillie RD, Pizzolato P, Donaldson PT. Nuclear stains with soluble metachrome metal mordant lakes.Histochemistry 1976; 49: 23-35.
17. Usmani OS, Biddiscombe M, Fahy WA, Lukey P, Marshall RP. Meah S, Oballa E, Simpson JK, MaherTM. The topical study of inhaled drug (salbutamol) delivery in idiopathic pulmonary �brosis.Respiratory Research 2018; 19(1): 25.
1�. Mazhar SH, Ismail NE, Newton, DA, Chrysytn H. Relative lung deposition of salbutamol followinginhalation from a Spacer and as SideStream jet nebulizer following an acute exacerbation. Br. J. Clin.Pharmacol. 2008; 65(3): 334-337.
19. Usmani OS, Biddiscombe MF, Underwood SR, Barnes PJ. Characterization of the generation ofradiolabelled monodisperse albuterol particles using the spinning-top aerosol generator. J. Nucl.Med. 2004; Jan:45(1): 69-73.
20. Ipratropium Summary of Products Characteristics. www.medicines.org.uk/emc/product/3818/smpc
21. Hasleton PS. The Internal surface of the adult human lung. J. Anat. 1972; 112(3): 391-400.
22. George R, Light R, Matthay M and Matthay R. (2005). Chest Medicine. Essentials of pulmonary andcritical care medicine. (5th ed.). Lippincott Williams & Wilkins.
23. Almadhoun K, Sharma S. Bronchodilators. In: StatPearls. Treasure Island (FL): StatPearls Publishing:March 16, 2020.
Figures
Page 19/22
Figure 1
Pre-Clinical Study in rats – MALDI-MS imaging of a 16 µm thick tissue section of rat lung and a 5 mmpunched biopsy of rat lung, taken 65 minutes after a nebulised administration of ipratropium. Top Left –Photo of the region of the tissue from where the section had been cut (after removal of multiple punchedbiopsies). Top Right – MALDI-MS Image showing the distribution of the m/z 166 fragment ion,representative of ipratropium in Rat 7, Section 13 (200 µm spatial resolution). The signal intensity for theipratropium fragment ion at m/z 166.0 is represented as a concentration-dependent colour scale – whitebeing highest concentrations. Bottom Left to Right: a) Photo of 5 mm punched biopsy from rat lung. b)Optical Image (digitally scanned image of rat lung section) c) MALDI-MS image, 200 µm spatialresolution (and Signal Intensity Scale bar) d) Histology image (Consecutive section)
Page 20/22
Figure 2
Representative MALDI-MS images, histology images and MS/MS for each participant. (TBC Samples).Each representative �gure depicts the MALDI-MS image (100 µm pixel size) for the biopsy sample sectionand its corresponding histology image, a photograph of the frozen embedded biopsy sample and massspectra showing both fragment ions (at m/z 123.9 and 166.0), obtained at the site of con�rmedipratropium detection (referred to as ipratropium or drug foci). Note: For clarity, the MALDI-MS images for
Page 21/22
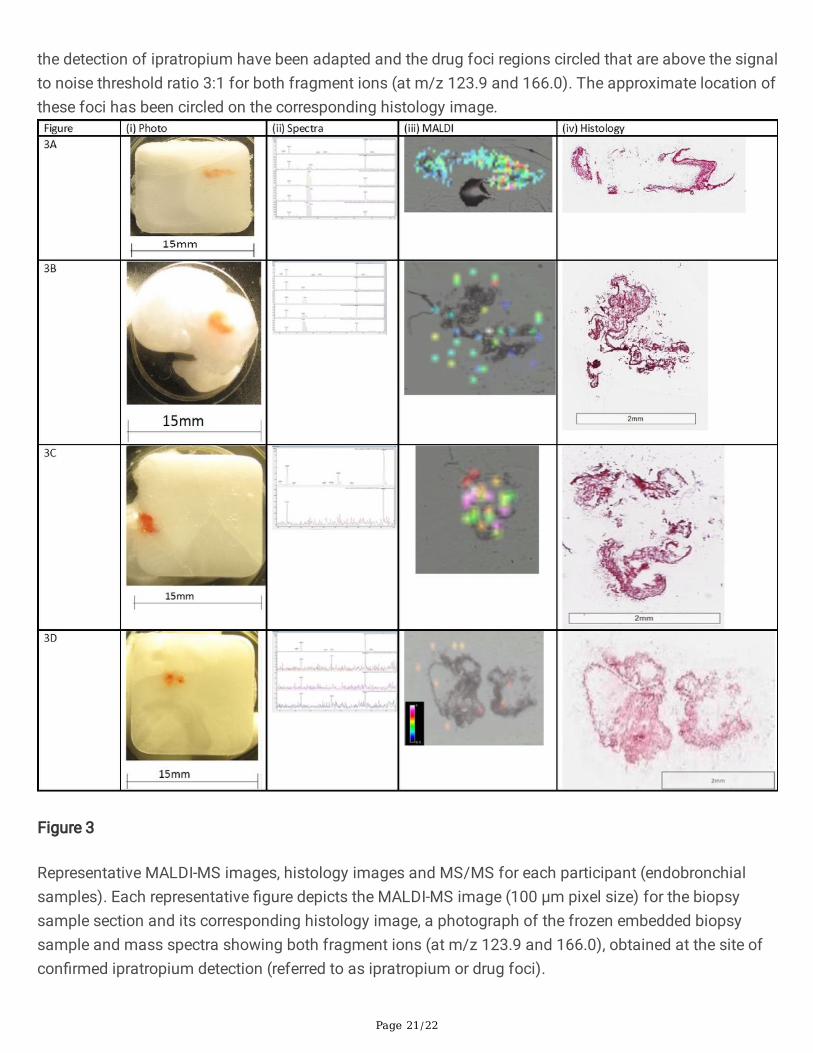
the detection of ipratropium have been adapted and the drug foci regions circled that are above the signalto noise threshold ratio 3:1 for both fragment ions (at m/z 123.9 and 166.0). The approximate location ofthese foci has been circled on the corresponding histology image.
Figure 3
Representative MALDI-MS images, histology images and MS/MS for each participant (endobronchialsamples). Each representative �gure depicts the MALDI-MS image (100 µm pixel size) for the biopsysample section and its corresponding histology image, a photograph of the frozen embedded biopsysample and mass spectra showing both fragment ions (at m/z 123.9 and 166.0), obtained at the site ofcon�rmed ipratropium detection (referred to as ipratropium or drug foci).

Page 22/22
Figure 4
Images showing MALDI-MS imaging hit on consecutive sample sections, 4A32 (i) and 4A33 (ii) andapproximate location of MALDI hit (middle). Bottom: (A) Co-location of MALDI-MS imaging and Histologyin TBC and Zoomed-in region (B) depict the approximate location of the MALDI-MSI hit present within a�brotic area of TBC sample 4A31, possibly co-located with a small airway. (C) and zoomed-in region (D)of TBC sample 5A23 illustrate lung architecture consistent with pulmonary �brosis and the approximatelocation of the MALDI-MSI hits appear to co-locate with a small airway.