Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1991;54:863-869
Dissection of the extracranial vertebral artery:report of four cases and review of the literature
P Hinse, A Thie, L Lachenmayer
AbstractFour cases of cervical vertebral artery(VA) dissection are reported. In threepatients VA dissection was associatedwith neck trauma. All patients wereyoung or middle-aged (range 27 to 49years). In two there was a history ofmigraine. Pain preceded neurologicalsymptoms from hours to six weeks.Three patients had neurological deficitsincluding elements of the lateralmedullary syndrome, and one experien-ced recurrent transient ischaemicattacks in the vertebrobasilar territory.Angiographic findings included irregularstenosis, occlusion and pseudoaneurysm;in two patients VA abnormalities werebilateral. All patients were treated withanticoagulants and improved. In areview of 28 cases with traumatic dis-section and 29 cases with spontaneousdissection of the VA reported in theliterature, distinct clinical and angio-graphic features emerge. Aetiologyremains obscure in most cases of spon-taneous dissection and management isstill controversial.
Department ofNeurology, UniversityofHamburg,Hamburg, GermanyP HinseA ThieL LachenmayerCorrespondence to:Dr Hinse, Department ofNeurology, University ofHamburg, Martinistr 52, 200Hamburg 20, GermanyReceived 15 June 1990 andin final revised form2 January 1991.Accepted 9 January 1991.
Mural artery dissection is produced by pene-tration of blood into the vessel wall causingnarrowing of the lumen and pseudoaneurys-mal dilation. Thrombus may lead to completeocclusion of the arterial lumen and serve as anembolic source for distal branch occlusion.Dissection results from intimal tear or primaryhaemorrhage from the vasa vasorum. Althoughdissection of the extracranial VA is less com-mon than dissection of the carotid artery inthe neck,' there has been an increasingnumber of reports on both traumatic andspontaneous VA dissection in the literatureemphasising its significance as a potentialcause of stroke in young and middle-agedadults.The prevalence of VA dissection remains
unknown. A substantial number of cases maygo unrecognised as prodromal symptoms are
not always easily interpreted and the clinicalcourse often proves to be benign. Yet earlydiagnosis is essential because of importantimplications for treatment. To support earlydiagnosis we report four cases and review theliterature on clinical and angiographic featuresofVA dissection.
Case reportsPatient 1A 39 year old woman with no history ofhypertension or cardio-vascular disease wasinvolved in a motor car accident on 17 March1989. She had suffered whiplash injuries of theneck twice previously (1978 and 1982) with-out complications of the nervous system.
Immediately after the accident sheexperienced severe, aching pain in the upperpart of the right neck radiating to the ear. Shewas treated with a neck collar for two weeks,but pain persisted. On 28 April, six weeksafter the accident, she had sudden severevertigo and nausea. Hours later she progres-sively developed dysarthria, dysphagia, weak-ness of the right face and numbness of the leftside of her body. She was admitted to ourhospital the next day.Examination revealed an alert and oriented
patient with normal cardiopulmonary func-tions. Speech was dysarthric, and she haddifficulty swallowing. Other neurologicalabnormalities included a right Horner's syn-drome, right facial weakness, paresis of theright soft palate and minimal left hemiparesis.The deep tendon reflexes were increased in theleft limbs but plantar responses were bothflexor. Sensation to touch, pain and vibrationwas considerably diminished on the left faceand limbs. CT scan showed a cerebellarinfarct corresponding to the right posteriorinferior cerebellar artery (PICA) distribution.Continuous-wave (CW) Doppler detected a
weak flow signal at the mastoid loop of theright VA that could not be traced intracran-ially by transcranial Doppler. Flow velocitiesin the left VA were increased suggesting com-pensatory flow, and the basilar artery dis-played normal flow velocities.
Transfemoral digital subtraction angio-graphy (DSA) on the day of admissionrevealed severe irregularities and stenosis ofthe third (V3) and fourth (V4) segment of theright VA. Filling of the right PICA wasdelayed. The left VA showed irregularities inits V4 segment without relevant narrowing ofthe lumen. Carotid and basilar angiogramswere normal (fig la).The patient was heparinised, and after 35
days anticoagulation was continued withphenprocoumon over a three month period.The clinical course was favourable: when
she was transferred for rehabilitation sixweeks after admission there was still a hemi-
863
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Hinse, Thie, Lachenmayer
It
AV
.
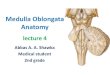
Figure la) Patient 1. Left and right vertebral angiograms. Severe irregularities andstenosis of V3 and V4 segments of the right VA (arrows). Mild irregularities of the leftVA without relevant narrowing of the lumen (arrow). b) Patient 1. Follow upangiography eleven weeks later, showing occlusion of the right VA distal to the PICA(arrow). Normal left vertebral angiogram.
sensory deficit but other neurological symp-toms had resolved. Follow up angiographyfour months after the trauma showed totalocclusion of the right VA distal to the PICA.Left vertebral angiogram was normal (fig Ib).
Patient 2A 40 year old previously healthy womanbumped into another person while skiing.Initially there was no disturbance of concious-ness but she suffered a severe headache. A fewhours after the accident, she suddenlydeveloped nausea and vertigo. Her speechbecame slurred and she had difficulty in swal-lowing. She was immediately transferred toanother hospital. On admission she was alertand oriented with stable vital functions.Neurological examination revealed rotatorynystagmus, increasing on right lateral gaze.Speech was dysarthric. There was diminution
of touch and pain perception on the left faceand the right extremities. The corneal res-ponse was impaired on the left. The gag reflexwas absent and slight pharyngeal and palatalweakness was found on the left. The deeptendon reflexes were symmetrical andpyramidal tract signs were negative. Therewas no weakness of the extremities, but shehad dysmetria of the left arm.Angiography revealed complete occlusion
of the left VA at the level of the first cervicalvertebra. There was retrograde filling of thedistal 1 5 cm of the left VA, but the left PICAcould not be visualised. The right VA and BAgave a normal angiographic appearance (fig 2).The patient was heparinised and trans-
ferred to our hospital. Follow up angiographysix weeks after the accident showed completerecanalisation of the left VA. There was asmall aneurysmatic dilatation at the intra-cranial segment. MRI visualised an infarctionin the left dorsolateral medulla oblongata,correlating to the clincial findings. In additionmultiple small infarcts were found in theterritory of the left posterior cerebral arteryand in both cerebellar hemispheres.The patient gradually improved and she
was discharged six weeks after the accidentwith a mild neurological deficit.
Patient 3A 49 year old man with a history of migrainewas looking up during his work at a buildingsite and suddenly experienced an intense,sharp pain in the right side of the neck. Healso noticed a numbness in the right face.One week later after waking he noted un-
steadiness of gait with a tendency to fall to the
Figure 2 Patient 2. Left vertebral angiogram, lateralview. Complete occlusion of the left VA at the level of thefirst vertebra.
864
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Dissection of the extracranial vertebral artery: report offour cases and review of theliterature86
right. Hours later he progressively developedhoarseness, nausea, vertigo, dysarthria, dys-phagia and paraesthesias of the left limbs.On admission neurological examination
revealed a right Wallenberg's syndrome withcrossed sensory deficit, right Homer's syn-drome, right palatal paresis, weakness of theright vocal cord and mildly dysarthric speech.There was no paresis of the extremities andtendon reflexes were symmetrical.CT scan showed marked global cerebellar
atrophy. CW-Doppler suggested occlusion ofthe right VA. A transfemoral DSA revealed atotal occlusion of the right VA at the third andfourth segments (fig 3). Only a short distalstump was filled by retrograde flow from theleft VA. The right PICA could not be visual-ised. Left VA angiogram was normal.Anticoagulation was started with heparin.
Neurological symptoms improved rapidly,and he was discharged two weeks after admis-sion with a mild left hemisensory deficit spar-ing the face. Neck pain, however, improvedonly slowly; on an outpatient visit two monthslater he still complained of right nuchaltenderness. Doppler examination six monthslater revealed complete recanalisation of theright VA.
Patient 4In this 28 year old woman hypertension hadbeen diagnosed earlier resulting in a one yeartreatment with a beta blocking agent. Afterdiscontinuation of therapy blood pressureremained normal. She was using oral con-traceptives and had occasionally suffered frommigrainous headaches.On 13 December 1989, she experienced
sudden, intense left cervical pain radiating tothe left shoulder. She consulted an ortho-
Figure 3 Patient 3. Leftvertebral angiogram,lateral view. Only a short
distal stump of the
occluded right VA is filledby retrograde flow from the
left VA (arrow).
paedic specialist who performed repeatedchiropractic manipulations and prescribed acervical collar. Pain subsided gradually after afew days, but on 23 December she experi-enced severe rotatory vertigo which recurredseveral times during subsequent days. It wascombined with unsteadiness of gait, nauseaand vomiting. On two occasions vertigo wasinitiated as she looked back over the rightshoulder.
She was admitted to our hospital on 4January 1990. There was slight unsteadinessof gait with drift to the right, but neurologicalexamination was otherwise normal. CT scanrevealed a cerebellar infarction in the leftPICA territory. Neither the VAs nor thebasilar artery could be detected with normalflow signals by pulsed Doppler, but thismethod failed to clarify the exact vascularpathology.
Transfemoral DSA showed a long irregularstenosis of the second (V2) segment of theright VA extending to the ClI level. (fig 4a).The left VA was occluded in its entire lengthwith collateralisation by the ascending cervicalartery which joined the left VA at the ClIlevel. The left PICA was poorly filled.Heparin was administered for the first
21 days and substituted by coumarin. Therewas no recurrence of vertigo and neurologicalfindings were normal at discharge. Dopplersonography and repeat angiography fourmonths later revealed recanalisation of the leftVA. On the right VA there were still mildcalibre irregularities (fig 4b), but the lumenhad normalised.
Review of literatureWe reviewed 28 cases with traumatic (table 1)and 29 cases with spontaneous dissection (table2) of the extracranial VA from the literature,including 15 cases reported by Chiras,2 whichare not listed in table 2. In traumatic VAdissection there were 10 males and 18 females;age ranged from seven to 60 years, with a meanage of 34 years. In spontaneous dissection therewere eight males and 21 females; mean age was40 years, ranging from 26 to 64 years.
Pain occurred in 19 patients (68%) withtraumatic and in 22 cases (76%) with spon-taneous VA dissection. In most cases (33 of 41)it was localised in the neck and occiput; diffuse,non-localised headache was noted in eightcases. Brainstem or cerebellar infarctionoccurred in 25 cases with traumatic VA dissec-tion, bilateral in 10. Of 15 cases with unilateralbrainstem ischaemia, 1 1 showed clinical signsof Wallenberg's syndrome, implicating thedorsolateral medulla to be the main site ofinfarction.Brainstem infarction occurred in 19 of 29
patients with spontaneous VA dissection, threeof which were bilateral. Lateral medullaryinfarction was noted in 10 patients. In fivepatients, only transient symptoms attributableto vertebrobasilar ischaemia occurred, andthree patients remained asymptomatic.Angiography was performed in all reported
cases. In traumatic dissections unilateral VAabnormalities were found in 20 patients, six
865
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Hinse, Thie, Lachenmayer
RA.'IA
!gi.4"o
tA
*
..
.:
.!.....* ... :g, :.
.:.
£:
A t\^ oc
-S .. o.; {Figure 4a) Patient 4. Left and right vertebral angiograms showing a long, "string-like" stenosis at the V2 segment of the right VA (arrows). Occlusion of the left VA withcollateralisation by the ascending cervical artery which joins the left VA at the Cl level(arrowhead). b) Patient 4. Follow up angiography performed-four months later.Recanalisation of the left VA, normalisation of the lumen of the right VA.
showed bilateral lesions, and in one patient VAangiography was normal. In four patientsunilateral dissection was combined with con-genital hypoplasia of the contralateral VA,bilateral VA hypoplasia was found in onepatient. In 19 cases dissection was localised atthe V3 segment of the VA; V2 was affected intwo, V2 and V3 were involved in five patients.Stenosis of the VA was found in 17 cases,occlusion in 10 and pseudoaneurysm in fourpatients. In spontaneous dissection, angio-graphy showed bilateral abnormalities in 14cases, and 15 patients had unilateral VAinvolvement. Stenosis was found in 33,occlusion in seven and pseudoaneurysm in fivecases. In 10 cases angiographic findings were
confined to the V1 and/or V2 segment of theVA; in 13 cases V2 and V3 were both involved,and in 16 cases dissection occurred at the V3segment only. In five cases there was angio-graphic evidence of fibromuscular dysplasia(FMD), three of whom showed associateddissecting aneurysms of the internal carotidartery.
In spontaneous dissection the clinical coursewas favourable in 22 cases, in one patient severeneurological deficits persisted, and four patientsdied. In two cases outcome was not mentioned.In 16 cases of traumatic VA dissection therewas substantial improvement of symptoms, insix cases outcome was fatal (four of which hadbilateral brainstem infarction) and in two casessevere neurological deficits remained. In fourcases outcome was not reported.
DiscussionVertebral artery dissection occurs predomin-antly in middle-aged adults: 68% of patientswith traumatic VA dissection and 80% withspontaneous dissection were aged 30-50 years.There was a female preponderance in bothgroups, 64% of patients with traumatic dissec-tion and 72% of patients with spontaneousdissection were female.
Symptoms and prognosisPain is a frequent, but not invariable prodromalsymptom in traumatic and spontaneous VAdissection.22' In traumatic dissection it occursimmediately after the trauma (in eight of 14reviewed cases) or delayed for hours to days (insix of 14 cases).
Pain is usually characterised as severe, dulland non-throbbing, with sudden onset, andmost frequently localised in the upper part ofthe neck and occiput, ipsilateral to the side ofdissection. It was an early symptom in all ourpatients. Initially consulted physicians in threeof our patients (1, 3, and 4) misinterpreted thepain to be of musculoskeletal origin andphysical therapy was initiated in all whichfailed to produce substantial relief.
Extracranial cerebral arteries are known tobe pain sensitive.22 Pain in VA dissection ismost likely caused by excitation of nociceptorsin the vessel wall, although, the exact mechan-ism of pain is still not fully understood.23Clinically, visceral pain caused by arterial dis-section is frequently difficult to differentiatefrom pain of musculoskeletal origin, especiallyin cases of traumatic VA dissection in whomtenderness of neck muscles may result fromtrauma. Neck and posterior head-painassociated with VA dissection will thereforerarely be correctly diagnosed as long as symp-toms of brainstem ischaemia are absent.
In our patients there was an interval betweenthe onset of pain indicating the initiation ofdissection, and the ischaemic event, rangingfrom a few hours (case 2), one week (cases 3 and4) to six weeks (case 1). This is also a commonfinding in patients reported in the literature: in11 of 25 cases (44%) with traumatic VAdissection onset of ischaemic events wasdelayed with the interval ranging from a few
866
-.: -' 400
i-,-i
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Dissection of the extracranial vertebral artery: report offour cases and review of the literature
Table 1 Reported cases of traumatic dissection of extracranial vertebral artery
Reference Age Sex Trauma Clinical Syndrome Angiography Outcome
Carpenter'3 42 M Fell out of a tree L lat medulla, spinal cord LVA dissection and occlusion at C6 DiedSimeone'4 40 M Car accident Brainstem (bilateral) Prox. occlusion of LVA, RVA occlusion at C2-3 DiedLorenz3 39 F Chiropract manipulation Brainstem (bilateral) LVA narrowing, hypoplastic RVA, BA occlusion DiedMehalic4 40 M Chiropract manipulation R lat medulla RVA narrowing at Cl-2, atherosclerotic LVA and BA Slight deficit
30 F Chiropract manipulation Brainstem (bilateral) RVA narrowing at C1-2, hypoplastic LVA Severe deficitDavidson5 42 F Chiropract manipulation R pons Pseudoaneurysm ofRVA at C2 Moderate
deficitEaston' 48 F Chiropract manipulation Cerebellum Normal Neurolog.
deficit44 F Chiropract manipulation L lat medulla Extreme narrowing of LVA between PICA and BA Minimal
deficitsParkin' 23 F Chiropract manipulation Brainstem (bilateral) Distal LVA occlusion, hypoplastic RVA, thrombus in BA Moderate
deficitZimmermann' 7 M Chiropract manipulation Left occipital lobe, cerebellum LVA occlusion at C2 filling defect of BA NormalKrueger' 25 M Chiropract manipulation Brainstem (bilateral) (Postmortem) LVA and RVA narrowing at C1-2 Died
39 F Chiropract manipulation Brainstem (bilateral), both Severe stenosis of RVA at foram, magnum, hypoplastic LVA Bilateraloccipital lobes hemianopsia
Shermann'° 48 F Chiropract manipulation Brainstem (bilateral) Hypoplastic RVA and LVA Neurolog.deficit
44 F Chiropract manipulation L lat medulla, cerebellum Hypoplastic LVA, ending at PICA35 M Chiropract manipulation Brainstem (bilateral) LVA narrowing at C1-2 with pseudoaneurysm24 M Chiropract manipulation Brainstem RVA occlusion at Cl Mild deficit60 F Chiropract manipulation Brainstem (unilateral) Perforation ofRVA Died
Schellhas" 36 F Chiropract manipulation Brainstem (bilateral) LVA dissection at Cl, RVA dissection at C1-2 Severe deficit31 F Chiropract manipulation L lat medulla LVA dissection at C1, focal stenosis ofBA Gradual
improvement32 F Chiropract manipulation R lat medulla RVA dissection at Cl20 M Sport accident R lat medulla RVA occlusion at C2
Katirji" 26 F Chiropract manipulation R lat medulla cerebellum Dissection of RVA and LVA at C1-6, bilateral aneurysms at Mild deficitC5
31 F Spott accident Brainstem (unilateral) RVA narrowing between C2 and C7 Normal51 M Chiropract manipulation R lat medulla RVA occlusion at C1-2 Steady
improvement34 M Sport accident Brainstem (bilateral) Irregularity of LVA, BA and both PCAs Died
Present report 39 F Car accident R lat medulla Severe RVA stenosis at C1-2, LVA irregularities at the Gradualintracranial segment improvement
40 F Sport accident L lat medulla LVA occlusion at C2 Mild deficit28 F Chiropract manipulation Recurrent vertebrobasilar TIA Irregular RVA stenosis from C2-C6, LVA occlusion Normal
LVA = left vertebral artery; RVA = right vertebral artery; BA = basilar artery; PICA = posterior inferior cerebellar artery; ICA = internal carotid artery;PCA = posterior cerebral artery.
hours to four days. A six week interval found inone of our patients is remarkable in thatpresumed thrombosis and embolism apparen-tly did not occur until six weeks after theprobable moment of arterial injury.
It exemplifies the importance of a carefulsearch for recent trauma in patients with VAdissection. In this patient, post-traumatic stiff-ness of cervical muscles had mostly resolvedduring these six weeks, but severe unilateralneck pain persisted which can retrospectivelybe interpreted as a clue to the diagnosis ofarterial dissection. In 28 of 39 patients withfocal cerebral ischaemia symptoms initiallyevolved suddenly (19 cases) or progressively (9cases). In 11 patients symptoms initially fluc-tuated, reflecting recurring cerebral ischaemia
during a two to four week period after onset.
Three of our patients (cases 1, 2, 3) showedclinical and radiological evidence of lateralmedullary infarction. Wallenberg's syndromewas found in 50% of patients with brainsteminfarction associated with VA dissection re-
ported in the literature. The clinical course wasfavourable in all our patients: there was no
recurrence of ischaemic events during followup (three to six months) and symptomsimproved considerably in all.
Substantial improvement ofsymptoms com-monly occurs in surviving patients with VAdissection, probably due to young age and thelack of artherosclerotic disease in most: it wasobserved in 75% of patients with spontaneous
dissection and in 52% of patients with
Table 2 Reported cases of spontaneous dissection of extracranial vertebral artery
Reference Age Sex Predisposing Factors Clinical Syndrome Angiography Outcome
Bostrom" 56 F Hypertension Sudden post-op death Post-mortem: dissection ofRVA and LVA at C2-4 DiedOkawara" 43 M Painted the ceiling R lat medulla RVA occlusion at CI-2, LVA narrowing Gradual
improvementEaston' 38 F Turned head while Brainstem (bilateral) RVA narrowing at Cl Died
drivingRingel" 49 M FMD hypertension R hemisphere signs Post-mortem: dissection of RVA at C2, dissection ofLVA at Died
C6, dissection of both ICAs at C2Mokri" 35 F Hypertension No definite post circulation Luminal irregularities of RVA and LVA at C2. Occlusion of L Normal
symnptoms ICA, subcranial aneurysm ofR ICABradac" 35 F Brainstem (unilateral) LVA stenosis and aneurysm at C1-2 Partial improvementShermann" 38 F Tumed head while Brainstem (bilateral), RVA narrowing at C1 Died
driving cerebellumAlpert"o 26 F No definite post circulation Severe narrowing of L ICA and R ICA. Mild narrowing of Normal
symptoms prox. RVA, diffuse narrowing of LVA throughout its lengthCaplan2' 31 F L lat medulla RVA narrowing at C2, LVA stenosis at C2 Normal
39 M Past trauma L lat medulla RVA stenosis at Cl, LVA occlusion at Cl Normal27 F Oral contraceptives L lat medulla Intracran. stenosis of LVA hypoplastic RVA Significant residual
deficit41 M L lat medulla LVA occlusion at CI-2 stenosis of RVA at Cl Mild deficit38 F L cerebellar LVA occlusion and aneurysm at C6 Normal
Present report 49 M Migraine R lat medulla Distal RVA occlusion Mild deficit
867
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Hinse, Thie, Lachenmayer
traumatic VA dissection. Long term follow updid not reveal recurrence of cerebral ischaemiain any of the reported cases.On the other hand, fatal outcome is not rare:
it was seen in six of28 (21 %) cases of traumaticand in four of 29 (14%) cases of spontaneousdissection.
AngiographyDiagnosis is essentially based upon angiogra-phy. Characteristic angiographic findings inboth traumatic and non traumatic VA dissec-tion include: 1) long irregular, luminal stenosis;2) occlusion of the artery; 3) pseudoaneurysm,and 4) "double lumen".25 Stenosis is by far themost common finding in both traumatic (54%)and spontaneous dissection (78%). It is causedby subintimal haematoma. Frequently dissec-tion extends circumferentially around thelumen over a long segment, giving rise to acharacteristic "string-like" appearence.25Luminal surface irregularities may be due tointimal folding. Narrowing of the lumen oftenproves to be severe and complete occlusion mayensue.
In our patients angiography revealed severestenosis in two cases (1 and 4) and occlusion inthree (2, 3 and 4). Pathological findings werelocated at the V3 segment in all patients, in onepatient (case 4) dissection also involved the V2segment. The V3 segment is most frequentlyaffected in both traumatic and non-traumaticdissection, but there is significant higherincidence of V1/V2 involvement in spon-taneous dissection (54% of the reported cases).There is a high incidence of bilateral VA
involvement in spontaneous dissection (50% ofthe reported cases) suggesting a predisposingarteriopathy, the nature of which remainsobscure in most cases.
Doppler ultrasoundTo our knowledge, the role of Dopplerultrasound in VA dissection has not beenstudied systematically. In dissection of theinternal carotid artery high-resistance Dopplerflow patterns in arteries proximal to the lesionhave been described.2627 Findings includedreduced flow velocities, alternating flow direc-tion, and high-amplitude Doppler signals.
In our patients, Doppler ultrasound duringthe acute phase correctly detected VAocclusion in two patients (cases 3, 4). It failed toidentify the exact lesion type in two arteries(cases 1, 4), but showed some abnormality thatencouraged angiographic examination. Followup findings (cases 3, 4) disclosed recanalisationof previously occluded vessels.
AetiologyIn traumatic VA dissection, mechanicalstretching and compression of the artery maycause intimal tearing and consecutiveintramural haematoma. Most reported caseshave been associated with chiropractical neckmanipulation,''2 commonly consisting ofabrupt and forceful rotational head movement,with or without hyperextension of the head.The VA is most susceptible to mechanical
injury at its mobile distal part after leaving the
transverse foramen of the axis and beforeentering the intracranial cavity. Theanatomical relationship between the VA and itsneighbouring bony structures and ligaments,and the special mechanisms of head and neckmovement may account for the unique vulner-ability to mechanical injury at the atlanto-axiallevel.4""1 162829 A reduction of vertebral bloodflow during rotational and hyperextensive headmovements has been demonstrated angio-graphically.""'5
In most cases of spontaneous VA dissectionaetiology remains obscure. The disordermostly affects younger and otherwise healthyadults. Of particular interest is the relationshipbetween minor neck trauma often resultingfrom ordinary head movement and VA dissec-tion. In one ofour cases (3), dissection occurredwith pronounced retroflexion of the head whilelooking up. Other reports6 10 36 have stressed thetemporal coincidence of trivial neck traumaand the onset of VA dissection. In these casesthere is a striking discrepancy between therelatively minor force of injury and the severityof vascular lesion suggesting enhanced arterialvulnerability. Various predisposing conditionshave been discussed including FMD, hyper-tension, migraine, and then use of oral con-traceptives.2 15 17 2137 Of 29 cases reported in theliterature such factors were noted in 17: hyper-tension (10 cases), FMD (six cases), oral con-traceptives (five cases) and migraine (fourcases). FMD has long been recognised as apredisposing factor for arterial dissection,2 17but the significance of hypertension, migraineand oral contraceptive use in the pathogenesisofVA dissection is still obscure. In 28 cases oftraumatic VA dissection only three patientshad a history of hypertension with no pre-existing cardiovascular disease in the rest. Postmortem examination performed in five fatalcases revealedl no evidence of vascular muralchanges suggesting degenerative or inflam-matory arteriopathy.-01214
TherapyThere is no general agreement on thebest management of VA dissection. Initialtreatment with anticoagulants has beenrecommended" 12 35 36 to prevent progressivethrombosis and thromboembolism. All of ourpatients were heparinised after diagnosis wasestablished. Duration of heparinisation rangedfrom five days (patient 3) to 35 days (patient 1).Anticoagulation with coumadin was continuedin two, the other patients received antiplateletagents after initial heparinisation. We did notobserve any complications of anticoagulanttherapy and there was no recurrence ofischaemic symptoms during follow up (rangethree to six months). Repeat angiography orDoppler sonography after four monthsrevealed recanalisation of the previouslyoccluded VA in patients 3 and 4 and occlusionof the previously stenosed VA in patient 1.
Cerebral ischaemic symptoms may occur as aconsequence of haemodynamic failure, or bythromboembolism with obstruction of distalvessels. Embolism can be postulated whenstenosis is haemodynamically insignificant and/
868
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from

Dissection of the extracranial vertebral artery: report offour cases and review of the literature
or when there is arteriographic evidence ofdistal embolus.3539 In the case of embolisminitial anticoagulant therapy seems to bereasonable. If dissection includes theintracranial VA segment, subarachnoidhaemorrhage should be excluded beforeanticoagulants are administered. If the use ofanticoagulants is contraindicated, patientsmight benefit from antiplatelet drugs.We prefer to perform repeat angiography
three months after initiation of anticoagulanttherapy to decide on further therapy.Anticoagulants are discontinued if spontan-eous recanalisation occurred, and the arteriallumen appears smooth. If the vessel remainsoccluded, we prefer to continue anticoagulantsfor six months followed by antiplatelet drugsfor two years. In the case of persistingpseudoaneurysm, we use the same regime, butfurther study on the natural history of theselesions is urgently needed.
1 Culebras A, Hodge CJ, Petro GR. Carotid and vertebraldissecting hematomas. In JF Toole, ed. Handbook ofClinical Neurology, Vol 10 (54). Vascular diseases Part II.Amsterdam: Elsevier, 1989.
2 Chiras J, Marciano S, Molina JV, Toubul J, Poirier B, BoriesJ. Spontaneous dissecting aneurysm of the extracranialvertebral artery (20 cases). Neuroradiology 1985;27:327-33.
3 Lorenz R, Vogelsang HG. Thrombose der Arteria basilarisnach chiropraktischen Manipulationen an der Halswirbel-saule. Dtsch med Wschr 1972;97:36-43.
4 Mehalic T, Farhat SM. Vertebral artery injury from chiro-practic manipulation of the neck. Surg Neurol 1974;2:125-9.
5 Davidson KC, Weiford EC, Dixon GD. Traumatic ver-tebral artery pseudoaneurysm following chiropracticmanipulation. Radiology 1975;115:651-2.
6 Easton JD, Sherman DG. Cervical manipulation and stroke.Stroke 1977;8:594-7.
7 Parkin PJ, Wallis WE, Wilson JL. Vertebral artery occlusionfollowing manipulation of the neck. NZ Med J 1978;88:441-3.
8 Zimmermann AW, Kumar AJ, Gadoth N, Hodges FJ,Traumatic vertebrobasilar occlusive disease in childhood.Neurology (Minneap) 1978;28:185-8.
9 Krueger BR, Okazaki H. Vertebral-basilar distributioninfarction following chiropractic cervical manipulation.Mayo Clin Proc 1980;55:322-32.
10 Sherman DG, Hart RG, Easton JD. Abrupt change in headposition and cerebral infarction. Stroke 1981;12:2-6.
11 Schellhas KP, Latchaw RE, Wending LR, et al.Verterobasilar injuries following cervical manipulation.JAMA 1980;244:1450-3.
12 Katirji MB, Reinmuth OM, Latchaw RE. Stroke due tovertebral artery injury. Arch Neurol 1985;42:242-8.
13 Carpenter S. Injury of neck as cause of vertebral arterythrombosis. J Neurosurg 1961;18:849-53.
14 Simeone FA, Goldberg HI. Thrombosis of the vertebralartery from hyperextension injury ofthe neck. JNeurosurg1968;29:540-4.
15 Bostrom K, Liliequist B. Primary dissecting aneurysm oftheextracranial part of the internal carotid and vertebralarteries. Neurology 1967;17:179-86.
16 Okawara S, Nibbelink D. Vertebral artery occlusion follow-ing hyperextension and rotation of the head. Stroke1974;5:640-2.
17 Ringel S, Harrison S, Norenberg M, Austin J. Fibromus-cular dysplasia: multiple "spontaneous" dissectinganeurysms of the major cervical arteries. Ann Neurol1977;1 :301-4.
18 Mokri B, Housero W, Sundt TM. Idiopathic regressingarteriopathy. Ann Neurol 1977;2:466-72.
19 Bradac GB, Kaernbach A, Bolk-Weischedel D, Finck GA.Spontaneous dissecting aneurysm of cervical cerebralarteries. Neuroradiology 1981;21:149-54.
20 Alpert J, Gerson L, Hall R, Hallmann G. Reversibleangiopathy. Stroke 1982;13:100,105.
21 Caplan LR, Zarins CK, Hemmati M. Spontaneous dissec-tion of the extracranial vertebral arteries. Stroke1985;16:1030-8.
22 Norregaard TV, Moskowitz MA. Substance P and thesensory innervation of intracranial and extracranial felinecephalic arteries. Brain 1985;108:517-33.
23 Tatemichi TK, Mohr JP. Migraine and stroke. In: BarnettHJ, Stein BM, Mohr JP, Yatsu FM, eds. Stroke: patho-physiology, diagnosis and management, Vol 2. New York:Churchill Livingstone, 1986:860.
24 Caplan LR, Stein RW. Stroke. A clinical approach. Butter-worths: Boston, 1986.
25 Goldberg HI. Cerebral Angiography. In: Barnett HJ, SteinBM, Mohr JP, Yatsu FM, eds. Stroke: pathophysiology,diagnosis and management, Vol 1. New York: ChurchillLivingstone, 1986:232-5.
26 Hennerici M, Steinke W, Rautenberg W. High resistanceflow pattern in extracranial carotid dissection. Arch Neurol1989;46:670-2.
27 Eljamel MSM, Humphrey PRD, Shaw MDM. Dissectionofthe cervical internal carotid artery. The role ofDoppler/Duplex studies and conservative management. J NeurolNeurosurg Psychiatry 1990;53:379-3.
28 Schneider RC, Gosch HH, Taren JA, et al. Blood vesseltrauma following head and neck injuries. Clin Neurosurg1972;19:312-54.
29 Tatlow WFT, Banner HG. Syndrome of vertebral arterycompression. Neurology 1957;7:331-40.
30 Faris AA, Poser CM, Wilmore DW, Agnew CH. Radiologicvisualization of neck vessels in healthy men. Neurology(Minneap) 1963;13:386-96.
31 Brown BSJ, Tissington-Tatlow WF. Radiographic studiesofthe vertebral arteries in cadavers. Effects ofposition andtraction on the head. Radiology 1963;81:80-8.
32 Barton JW, Margolis MT. Rotational obstruction of thevertebral artery at the atlantoaxial joint. Neuroradiology1975;9:1 17-20.
33 Husni EA, Bell HS, Storer J. Mechanical occlusion of thevertebral artery: a new clinical concept. JAMA1966;1%:475-8.
34 de Kleyn A, Nieuwenhuyse P. SchwindelanfaIle und Nys-tagmus bei einer bestimmten Stellung des Kopfes. Actaoto-laryng 1927;1 1:155.
35 Sheehan S, Bauer RB, Meyer JS. Vertebral artery compres-sion in cervical spondylosis: Arteriographic demonstra-tion during life of vertebral artery insufficiency due torotation and extension of the neck. Neurology1960;10:968-86.
36 Hart RG, Easton JD. Dissections. Stroke 1985;16:925-7.37 Alexander CB, Burger PC, Goree JA. Dissecting aneurysms
of the basilar artery in 2 patients. Stroke 1979;10:294-9.38 Hart RG, Easton JD. Dissections and trauma of cervico-
cerebral arteries. In: Barnett HJ, Stein BM, Mohr JP,Yatsu FM, eds. Stroke: pathophysiology, Vol 2. Diagnosisand management. New York: Churchill Livingstone,1986:775-88.
39 Hart RG. Vertebral artery dissection. Neurology 1988;38:987-9.
869
on April 24, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.54.10.863 on 1 O
ctober 1991. Dow
nloaded from












![Case Report Woven Coronary Artery Disease Successfully ...[ ]A.Yldrm,D.O guz, and R. Olguntrk, Woven right and aneurysmatic le coronary artery associated with Kawasaki disease in a](https://img.pdfslide.us/doc/110x75/60e1a40e001edc4ead069e1e/case-report-woven-coronary-artery-disease-successfully-ayldrmdo-guz-and.jpg)