Embed Size (px)
Citation preview

ADOLESCENT GYNECOLOGY 0889-8545/00 $15.00 + .00
DISORDERS OF EXCESSIVE HAIRGROWTH IN THE ADOLESCENT
Leo Plouffe, Jr, MD, eM
The problem of excessive hair growth in women has challengedclinicians for a long time. In a 1963 monograph on hirsutism." RobertB. Greenblatt, acknowledged by many physicians as one of the foundingfathers of contemporary reproductive endocrinology, wrote, liThe hairyfemale, a subject of much anguish and concern to herself and herfamily, has been the object of great curiosity to men and women ofall generations, a bewildering puzzlement and decided challenge tophysicians from time immemorial."
Indeed, excessive hair growth in women has long been the subjectof curiosity and fascination. One of the most famous illustrations ofexcessive hair growth dates back to 1631. In his painting "La Barbuda,"the Spanish painter Ribera depicts a woman holding her newborn babywhile displaying a thick beard rivaling that of her husband. The paintingis said to have been commissioned by the king of Spain, highlightingthe deep fascination with such a condition."
Today, the terms hirsutism and virilization are used to describe theclinical spectrum of disorders of excess hair growth in women. Muchprogress has been accomplished in the past decades in understandingthe cause and management of these conditions. This article reviewsthe current approach to these conditions when they present in theadolescent woman.
From Lilly Research Laboratories, United States Medical Endocrine Division, Eli Lilly andCompany, Indianapolis, Indiana
OBSTETRICS AND GYNECOLOGY CLINICS OF NORTH AMERICA
VOLUME 27 • NUMBER 1 • MARCH 2000 79

80 PLOUFFE
DEFINITION
It is helpful to clarify some of the terms used to refer to disordersof excessive hair growth in women. Hirsutism refers to the "appearanceof excessive coarse (terminal) hair in a pattern not normal in the female.":" This definition highlights the abnormal distribution of excesshair growth, such as facial, chest, or upper abdominal hair. In contrast,hypertrichosis refers to growth of hair in excess of the normal whilelimited to a normal pattern of distribution.' The latter condition isbeyond the scope of this discussion but is frequently associated with theuse of medications such as antiepileptics."
Virilization refers to the concurrent presentation of hirsutism witha broad range of signs suggestive of androgen excess, such as acne,frontotemporal balding, deepening of the voice, a decrease in breastsize, clitoral hypertrophy, increased muscle mass, and amenorrhea oroligomenorrhea. Virilization is seen much less frequently than hirsutismand may reflect a severe underlying pathologic condition, such as amalignancy.
Although these definitions may seem semantic in nature, they areof great clinical relevance. Hypertrichosis is a totally separate entity.Hirsutism and virilization are more closely linked, and hirsutism mayactually be the first manifestation of a condition that ultimately will leadto virilization if left untreated. In this context, one must consider therange of causes that may account for either isolated hirsutism or virilization.
BASIC FACTS ABOUT HAIR
Several facts regarding hair and hair growth are relevant to theworkup of these disorders.w " Hair grows from individual hair folliclesthat are part of a pilosebaceous gland unit. The number of hair folliclesis set from birth. The number of hair follicles is also comparable betweenmen and women. The main difference between sexes is the degree ofdifferentiation of the hair.
The growth of hair can follow one of several patterns. Humansdisplay continuous hair growth in contrast to many animal species thathave a cyclical or seasonal pattern. In addition, hair grows in a so-called"mosaic pattern," that is, in any given area, hairs are in a different stageof development. The end result is a stable and static number of hairs ina given area despite a constant but stable turnover. This growth patternis important clinically. Some conditions may cause a high level of synchrony between the growth cycles of hair, leading to the appearance ofeither massive hair loss (alopecia) or excess hair for a limited periodof time.
The number of hairs in any given area of the body is highly variable,with the scalp generally being the best endowed with more than 100,000.

DISORDERSOF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 81
Scalp hair generally has a growth cycle of about 2 to 6 years and displaysa growth rate of about 12 cm/year. By contrast, hair in other areas ofthe body tends to have a much shorter life cycle, ranging from 1 to 6months. This shorter life cycle accounts for the shorter length of hair inother parts of the body. It also means that 3 to 6 months will passbefore the effect of any therapy modifying hair growth can be assessed,corresponding to the turnover of hair in a given area.
The growth cycle of hair comprises three discrete phases (remembered by the mnemonic, ACT).56 Anagen refers to the growth phase andcomprises 85% to 90% of the life cycle of hair. Catagen is the rapidinvolution phase, and the telogen phase is the quiescent part of thecycle. The second and third phases constitute 10% to 15% of the entirelife cycle. The growth phase, or anagen, is primarily influenced bydisorders that stimulate hair growth as well as therapeutic modalities.
Three types of hair can present. Lanugo hair refers to the body hairseen in the fetus and newborn. This term should be reserved to thisstage of life. The fine adult hair covering the body is referred to as vellushair. The thick pigmented hair seen in areas such as the scalp and pubicareas represents terminal hair.
There is a marked range in the appearance of terminal hair, whichcan sometimes be misleading in a clinical setting. The thickness ofterminal hair varies greatly from one individual to another, dependingprimarily on genetic and, possibly, nutritional factors. In addition, thecolor of the pigment may influence the way the hair is perceived. Black,red, or blond pigmented hair will be more or less apparent dependingon the individual's complexion and skin color.
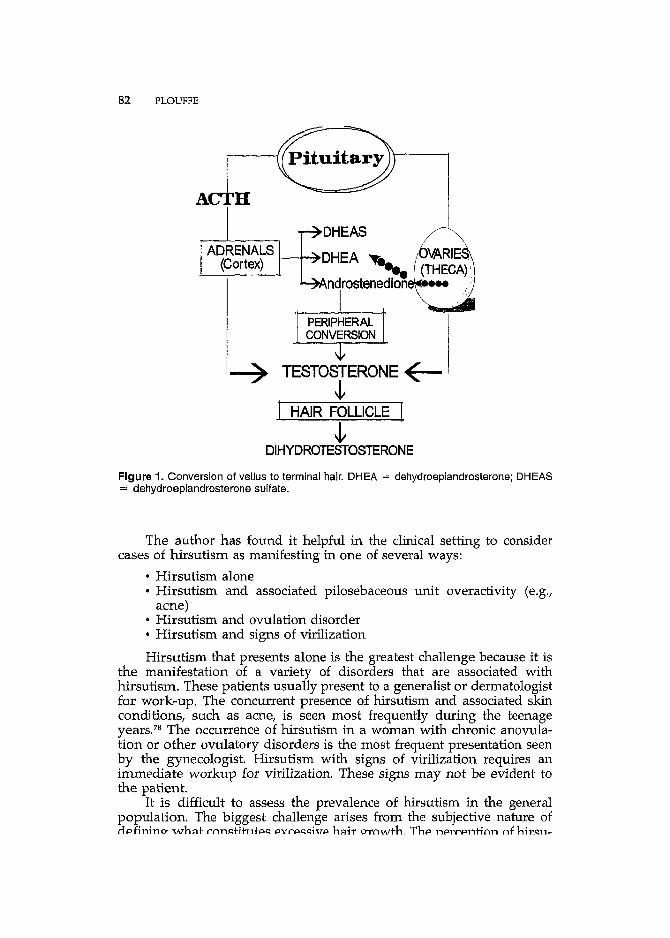
Only certain areas of the body depend on androgen input for hairgrowth. These areas include the face, neck, chest, abdomen, axillary,upper arms, inner thighs, and pubic regions. Part of the scalp is alsoandrogen-sensitive. The androgen metabolism within the pilosebaceousunit is complex and involves the interaction of testosterone with theandrogen receptor as well as intracellular conversion of testosterone tothe more potent dihydrotestosterone by the enzyme 5~-reductase.6o Theandrogenic stimulation of the pilosebaceous unit in these areas leads tothe conversion of vellus to terminal hair (Fig. 1). In contrast, hairs onthe forearms, hands, and lower legs are less influenced by androgenicmechanisms.
PRESENTATIONS OF HIRSUTISM
Most cases of virilization seen clinically are acute and striking innature. They seldom remain unrecognized and usually prompt immediate medical intervention. In contrast, hirsutism presents in a variety ofways and depends on several factors. Numerous studies have attemptedto assess the prevalence of hirsutism or underlying disorders.
82 PLOUFFE
AC H
ADRENALS(Cortex) -t--~DHEA ".,
ndrostenedion_...
I
~ TESTOSTERONE~~
J HAIR FOLLICLE [
~DIHYDROTESTOSTERONE
Figure 1. Conversion of vellus to terminal hair. DHEA = dehydroepiandrosterone; DHEAS= dehydroepiandrosterone sulfate.
The author has found it helpful in the clinical setting to considercases of hirsutism as manifesting in one of several ways:
• Hirsutism alone• Hirsutism and associated pilosebaceous unit overactivity (e.g.,
acne)• Hirsutism and ovulation disorder• Hirsutism and signs of virilization
Hirsutism that presents alone is the greatest challenge because it isthe manifestation of a variety of disorders that are associated withhirsutism. These patients usually present to a generalist or dermatologistfor work-up. The concurrent presence of hirsutism and associated skinconditions, such as acne, is seen most frequently during the teenageyears." The occurrence of hirsutism in a woman with chronic anovulation or other ovulatory disorders is the most frequent presentation seenby the gynecologist. Hirsutism with signs of virilization requires animmediate workup for virilization. These signs may not be evident tothe patient.
It is difficult to assess the prevalence of hirsutism in the generalpopulation. The biggest challenge arises from the subjective nature ofc1pfinino- W'h::lt ('nn."tihltp" p)((,pl;l"ivp h::lir o-rn1Alth Thp npr('pntinn nfhirl;ll1-

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 83
tism by the patient may be influenced by several factors, including thedegree of hair growth in relatives and racial and ethnic factors.
Few studies have focused on the prevalence of hirsutism. Suchstudies have incorporated some form of an objective assessment scale todetermine hair excess. In a study conducted in Wales and reported in1964, approximately 10% of women presented with some degree ofhirsutism, and nearly 4% had true disfigurement." A more recent studyconducted in the southeast United States evaluated a randomly selectedpopulation of 369 women for the prevalence of hirsutism.w Dependingon the clinical threshold selected, 2% to 8% of the women were foundto have hirsutism, with no racial difference between black and whitewomen. These estimates of prevalence are remarkably concordant considering the variance in time and geographic location.
The frequency with which one sees the various presentations ofhirsutism varies greatly. Azziz et aJ5 studied a population of hirsutewomen in Alabama. Of the 132 women, more than 70% presented withconcurrent ovulation disorder. Similar findings were reported in thestudy of a group of women of primarily Arabic origin.34 In contrast, ina study of more than 600 women undergoing cosmetic electrolysis, morethan 70% of women self-reporting hirsutism had normal menstrual cycles."
Approximately 2% to 10% of the population manifests some evidence of hirsutism. The underlying cause and accompanying presentations vary greatly from one population to another. The clinician mustremain alert when formulating an appropriate differential diagnosis forthese patients.
CAUSE OF HIRSUTISM
The clinical approach to the patient with hirsutism rests on a solidunderstanding of the potential causes of excess hair growth. Severalclassification systems have been proposed for these causes.v 26, 38 Thefollowing system offers a simple and logical approach:
• Excess androgen production• Relative circulating androgen excess and low binding globulins• Excess end-organ response• Patient perception
Disorders of Excess Androgen Production andCirculating Levels
Excess androgen production is the most common triggering factorfor hirsutism. The source of androgens can be exogenous but is mostcommonly endogenous. There are two primary endogenous sources ofandrogens: the adrenal glands and the ovaries.
A ...:1 ............. "'1 .... _...:I...._ .......n............'V' .....n'·H·' ...".... ..... 'Y'T 'h.n l~..."l""'r\rl ......,. rrrvr,n.hfl..,,11,,1' ..-1~+I"\""~~"""I""\r1

84 PLOUFFE
steroid synthesis enzyme deficiency, to a malignant adrenal neoplasticprocess, or to other conditions such as Cushing's syndrome. Three recognized steroidogenic adrenal enzyme deficiencies have been linked withhirsutism: (1) 21a.-hydroxylase deficiency, (2) ll~-hydroxylase deficiency,and (3) 313-ol-dehydrogenase deficiency. 55 These disorders may be evident from the prenatal or neonatal period with ambiguous genitalia inthe female, usually referred to as the classic form of the disorder," ThenoncIassic forms of these enzymatic defects are linked with hirsutism.wThe genetic basis of this class of disorders recently has been elucidated.w 46,53
21a.-Hydroxylase deficiency is the most common of these disorders.Estimates of the prevalence of this condition among hirsute womenrange from <1% to >10%.9 There is a wide range in the prevalence ofthe noncIassic form of the disorder depending on the specific ethnicgroup studied. Estimates range from 1 in 300 in an Italian population to1 in 50 in Slavs to 1 in 40 in Hispanics in the United States to 1 in 27 inAshkenazi [ews." The likelihood of identifying this disorder dependsgreatly on the origin of the population.
Although hirsutism is associated with the nonclassic form of 21C/.hydroxylase deficiency, heterozygous carriers for 21C/.-hydroxylase deficiency do not seem at increased risk for hirsutism." 1113-Hydroxylasedeficiency among hirsute women has been demonstrated with a prevalence of approximately 5%.41 The link between hirsutism and 3~-ol
hydroxysteroid dehydrogenase deficiency has been viewed with somedegree of skepticism.v- 69 Recent studies using molecular diagnostic techniques support this enzyme deficiency as an etiologic factor, albeit, apotentially rare one. 52
Cushing's syndrome and disease can be seen in adolescents; however, the presentation may differ from that in adults, with weight gainand growth retardation as the primary manifestation." Hirsutism as wellas acne and other cutaneous manifestations are associated with thiscondition in this patient pcpulation.F Although it is rare, Cushing'ssyndrome should be considered in the differential diagnosis.
The most common cause of androgen excess of ovarian origin ispolycystic ovary syndrome (PCaS) and its many linked disorders."peas is discussed in more detail elsewhere in this issue. On occasion, aneoplastic ovarian process may be involved."
Disorders of Relative Androgen Excess and SexHormone-Binding Globulin
Usually, less than 3% of testosterone circulates freely in serum. Mostandrogens circulate in a bound form, primarily to sex hormone-bindingglobulin (SHBG). Any condition that impacts on the levels of SHBG orother binding proteins can lead to a relative excess of circulating androgens. Several conditions that decrease SHBG levels have been identified.In patients with hirsutism, the major conditions linked with abnormal
DISORDERSOF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 85
SHBG levels include peas (chronic anovulation) and obesity;" Severalother factors are known to affect the levels of SHBG or its bindingpotential, including medications.
Disorders of Excess Responsivity to Androgen
Once androgens reach target cells, they must interact with theandrogen receptor, which is encoded by a gene on the X chromosome.Testosterone is converted within the cell to dihydrotestosterone, a morepotent androgen, under the action of Sex-reductase. Excess activity of 5exreductase is recognized as a cause of hirsutism. Mutations in the androgen receptor have also been linked to hirsutism.
Two genes encoding different types of Sex-reductase, type 1 and type2, have been identified. Recent studies suggest that the type 1 enzymeis involved in hirsutism." Recent studies have identified mutationswithin the androgen receptor that account for excess responsiveness tocirculating androgens, including mutations in the highly polymorphicregion of the androgen receptor/" Another proposed mechanism of excess responsivity is preferential inactivation of the X chromosome withgreater androgen sensitivity."
Disorders of Perception and Self-Image
Hirsutism is a condition that is subjective in nature by definition.Although a certain threshold level may be proposed on semiobjectivescoring scales, the patient's perception of the condition is most important. Semiobjective scales compile a score from a number of differentsites, such as the face, the chest, and the perineum, whereas patientspotentially perceive these areas and the presence of hair in these regionsas very different. The presence of a few coarse facial hairs may beconsidered a medical emergency by Some patients, whereas other patients with coarse hirsutism remain unconcerned.
In teenagers, the concurrent appearance of acne and hirsutism cancompound the sense of distress. The clinician must consider both elements when formulating a management plan. The clinician should bereassuring and show appropriate concern but should also establish reasonable medical expectations.
One dangerous path to avoid is heeding to the concerns of a teenager who desires therapy for excessive hair growth limited to nonandrogen-dependent areas, such as the forearms or the lower legs. Hairgrowth in these areas is genetically determined and independent of theendogenous androgenic environment. It is inappropriate to perform aworkup for this presentation, and any therapeutic attempt will be futile.

86 PLOUFFE
Other Conditions
Several medical conditions have been associated with hirsutism:Disorders of excess androgen production
Ovarian disorderspcas (includes HAIRAN: hyperandrogenism, insulin resis-
tance, acanthosis nigricans)Severe insulin resistanceHyperthecosisTumorsEnzyme deficiency (17-ketosteroid reductase)
Adrenal disordersCongenital adrenal hyperplasia (Zlee-hydroxylase /l1l?>-hy
droxylase /313-hydroxysteroid dehydrogenase)Cushing's syndromeTumors
Disorders of sexual differentiation (mixed gonadal dysgenesis)Relative circulating androgen excess/low binding globulins
DrugsPregnancyAnorexia nervosa, malnutrition
Excess end-organ responseGenetic or idiopathicRacial or familial
OtherHypothyroidismH yperprolactinemiaAcromegalyCentral nervous system lesions
Multiple sclerosisEncephalitis
PorphyriaStressSyndromes
Hurler'sTrisomy Ede LangeAchard-Thiers
The mechanism underlying the hirsutism is often unclear. In somecases, the hirsutism may be related to drug effects. An example isthe hirsutism described in patients receiving medications for seizuredisorders."
BASIC APPROACH TO THE DIAGNOSIS OFHIRSUTISM AND VIRILIZATION
Diagnosis in the patient presenting with hirsutism or virilization issimple if one follows a methodical approach. Several algorithms have

DISORDERS OF EXCESSIVE HAIR GROWfH IN THE ADOLESCENT 87
been proposed, but there is considerable overlap.v 26,38 This sectionoutlines the author's approach to diagnosis in the teenage patient.
The first step consists of identifying the true nature of the presentation. In some cases, the patient presents because of an ovulatory disorder,and, although clinically apparent, hirsutism is not reported or noticedby the patient. In other cases, the patient may present with the primarycomplaint of hirsutism, although a fully normal complement of hair ispresent. In rare instances, signs of virilization are manifest. Defining theproblem accurately is essential to further investigations and the ultimatetreatment of the patient.
When hirsutism is evident to the clinician but is not reported by thepatient, the clinician must bring up the issue using tact, He or sheshould not give the teenager a message that she is grossly abnormal andcreate a new problem for her. The hirsutism may be idiopathic and areflection of the genetic and familial background of the patient. Raisingthe issue of hirsutism may make the teenager highly self-conscious andmay create a self-image problem when it did not exist before.
A careful history must be taken. Specifically, the timing and thechronologie progression of the excess hair growth must be established.In the teenage woman, one must document the age of onset of pubertaldevelopment and the progression. Any evidence of precocious pubertyassociated with a history suggestive of androgen hyperactivity is particularly relevant in determining the need for further steps in the workupand is highly suggestive of an adrenal enzyme defect. The presence ofany associated medical condition must be noted. The family history isimportant and should focus not only on problems that may suggestandrogen excess disorders but also the familial pattern of hair growth.The evaluation of this group of patients frequently requires completionof the physical examination and a return to history taking to elucidatethe diagnosis.
The physical examination should focus on establishing the presenceof hirsutism and quantifying it, if present. Several different scales havebeen proposed to assess the level of hirsutism. In addition, the clinicianshould identify the presence of acne and virilization and rule out thepresence of hypertrichosis versus hirsutism. The presence of skin hyperpigmentation, acanthosis nigricans, is suggestive of insulin resistanceand is often associated with peas. Other relevant elements during thephysical examination include the measurement of height, weight andblood pressure. These parameters may suggest conditions of androgenexcess related to adrenal enzyme deficiencies. Clinical evidence of anyof the associated medical conditions, such as galactorrhea, should benoted. Tanner staging is appropriate in the early adolescent patient torelate the presentation to the stage of pubertal development. The presence of hirsutism before Tanner stage 3 to 4 is alarming and suggests aserious underlying pathology. Visual examination of the external genitalia is critical in identifying early signs of virilization. For many teenagers,this examination may represent the first gynecologic evaluation, andappropriate consideration should be given to this aspect. Visualizationof the external genitalia will suffice versus a full pelvic examination.

88 PLOUFFE
~:v~;~~~~~I 2 3 4
'P :L:f ? !'1 'Y, i':1 '2.,',j3) • ~ ) = \ ):n::'\ ) :.':J;';~'\
I 2 3 4
(+\ (~\ /f\ !'*\I 2 3 4
8~8~I 2 3 4
(-t,\ (~~\ (Jj (:~t\I 234
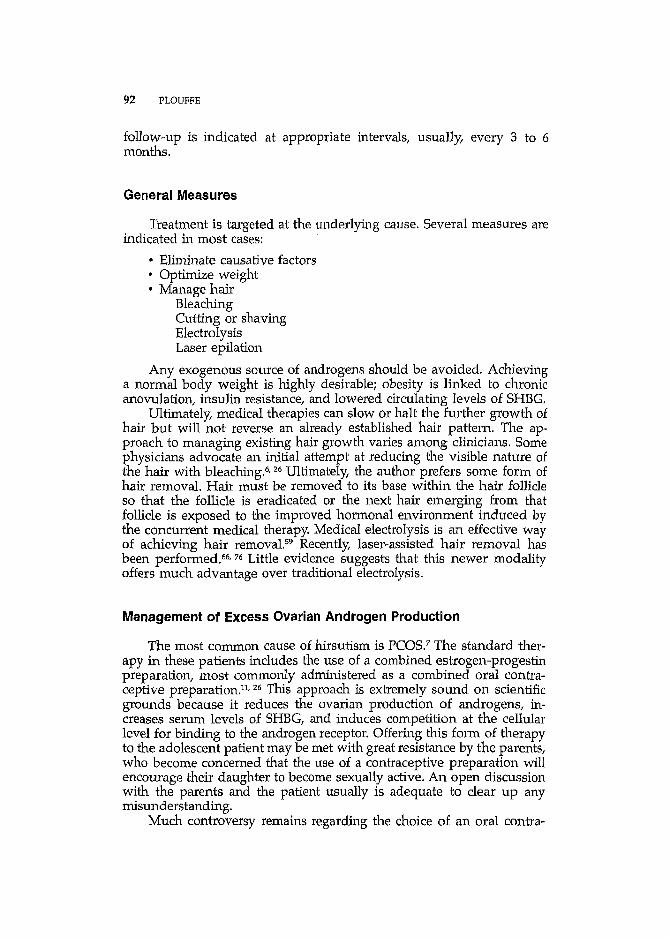
Figure 2. Hirsutism scoring system. (From Ehrmann DA, Rosenfield RL: An endocrinologicapproach to the patient with hirsutism. J CUn Endocrinol Metab 1990; 71:1-4. © 1990, byThe Endocrine Society; with permission.)
An adequate evaluation of hirsutism requires an objective methodfor assessing the amount of hair growth. Some clinicians obtain detailedphotographs so that they can follow the progression or regression ofhair over time. Although this practice may be appropriate in somesettings, in the author's experience, most teenagers dislike this approach.In addition, high-quality photography is required for the method to bevalid. The use of a semiobjective scoring system is preferred, such as theFerriman and Gallwey system (Fig. 2). No absolute cutoff level defineshirsutism on the Ferriman and Gallwey scale, but most investigatorsand clinicians choose a score between 6 and 12 as the lower end forhirsutism.
The author solicits the full cooperation of the patient when usingthe Ferriman and Gallwey scale. The physician and patient assess thescore together, and the completed scoring sheet is placed in the patient'schart. At a follow-up visit, the patient can repeat the scoring and evaluate for herself the progress over time.
When the patient presents with virilization, a full investigation iswarranted. Virilization is the clinical manifestation of gross androgenexcess. The workup focuses on the identification of the source of androgen excess:
• Rule out exogenous androgenTestosterone or other androgenic preparation
• Evidence of endogenous androgen excessSerum total testosteroneSerum dehydroepiandrosterone sulfate (DHEAS)

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 89
• Imaging studiesPelvic ultrasonography (ovaries)Adrenal imaging
UltrasonographicCT or MR imaging
• Specialized studiesSelective venous catheterization (adrenal or ovaries)Radioisotopic studies
These cases are rare, and one should consult liberally. A full workupmust be completed to avoid jumping to conclusions too early. The authorand many of his colleagues are aware of several cases in which aninvasive and irreversible operation was performed before reaching anappropriate diagnosis of a condition that could have been treated medically.
Controversy remains regarding what investigations are appropriatein the patient presenting with hirsutism. The real issue is to define theultimate goal of laboratory investigations. One must distinguish betweenclinically relevant investigations and laboratory tests that belong to therealm of structured clinical scientific investigation protocols.
For some clinicians, the clinical finding that the patient has anovulatory disorder and hirsutism is sufficient evidence to initiate atreatment plan. Although this approach way be highly cost-effective, itis unacceptable in the adolescent patient. At a minimum, the patientshould undergo an investigation to determine the cause of the ovulatorydisorder. An accurate diagnosis is essential in this age group beforeundertaking a management plan that will span several decades of life.
At the other extreme, some clinicians propose an elaborate workupthat includes sophisticated assays and provocative testing. This approachis appropriate in the context of structured clinical investigations performed to determine the prevalence of certain conditions. For mostclinicians, such tests are not available. Possibly worse, the tests that areavailable are based on a different assay system that does not truly reflectthe findings outlined in reported studies.
The best clinical approach seems to be a "middle-of-the-road" position. The goal of the investigations should be to rule out serious potentially life-threatening conditions and to gain information that may helpguide the treatment approach." Recommended investigations are as follows:
Evaluation of androgen productionTestosterone (total or free)DHEASIn selected cases
17-Hydroxyprogesterone (fasting morning sample)3a-Androstanediol glucuronide
Evaluation of accompanying medical disorderOvulation disorder (follicle-stimulating hormone [FSH] and lu
teinizing hormone [LH])

90 PLOUFFE
Thyroid dysfunctionHyperprolactinemia (prolactin)
Other investigations (in selected cases)Androgen production
Androstenedione3a-Androstanediol glucuronideProvocative testing
Corticotropin stimulation testInsulin resistance determination
Evaluation of androgen production is appropriate. Either total orfree testosterone can be measured. Evaluation of total testosterone willhelp to rule out a gross excess of androgen, as will measurement ofDHEAS. Measurement of free testosterone will provide evidence ofsubtler androgen excess in a patient. The challenge clinically is the widerange of assays for free testosterone and the lack of uniformity indetermining normal and abnormal ranges. Obtaining a free testosteronelevel may add little information for clinical management. An alternativeto the measurement of free testosterone is the evaluation of SHBG;however, there are also wide variations in the measurement of serumlevels and a wide range of normal levels.
The need to screen for a form of adrenal enzyme deficiency isgenerally accepted'< 53; however, the ethnic origin of the patient may bea better guide in the selection of patients for testing. The simplest wayto test is to obtain a fasting morning plasma 17-hydroxyprogesteronelevel." Several investigators advocate the routine use of provocativetesting to screen for these disorders."
To rule out accompanying medical disorders, the workup shouldinclude tests to detect an ovulation disorder, thyroid dysfunction, orprolactin excess if there is any suggestion from the history or clinicalexamination that one or more of these conditions may be present. Adetailed discussion of the investigations for these medical conditions isbeyond the scope of this article.
Several other investigations may be appropriate depending on theclinical presentation. Measurement of androstenedione has been advocated for a long time} but its clinical relevance is unclear. Similarly, manystudies have advocated the evaluation of 3a-androstanediol glucuronideas a measure of peripheral androgen metabolism." Although this assayis appropriate in the research setting} it has limited value in the clinicalsetting, primarily because of wide variations in the clinical assays usedto measure this metabolite and related compounds. An evaluation ofthyroid function, prolactin} FSH, and LH, may be appropriate in somepatients, but the author does not believe these tests should be includedroutinely in the workup of the adolescent with hirsutism unless there issuggestive evidence for one of these disorders.v 26, 38
Numerous protocols exist for provocative adrenal testing in searchof an adrenal enzyme deficiency.3,53 These protocols are appropriate tomake a specific diagnosis. Some clinicians advocate the routine testing

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 91
of all patients for these disorders. Their ultimate impact on the management of hirsutism is often moot, and the author prefers to reserve testingfor specific conditions. Patients with a family history suggestive of anadrenal enzyme deficiency or who belong to an ethnic or racial groupin which the disorder is highly prevalent may be more appropriate fortesting. Recent reports have proposed the use of ovarian suppressivetesting in the evaluation of these patients," This investigation should beconsidered experimental at present. It is most appropriate to conductprovocative testing in a setting in which it is performed regularly andin which appropriate laboratory standards have been established andare maintained. The same recommendations apply to testing for insulinresistance.
A battery of additional tests can be useful in clinching a finaldiagnosis. These tests include ultrasonography of the ovaries and adrenal glands and CT or MR imaging of the adrenals. These modalitiesshould be reserved for patients in whom a final diagnosis cannot bemade without this information.
There is great variation in the laboratory investigations that arerecommended in the evaluation of hirsutism. The clinician must clearlyoutline the goals of the investigations and be intimately familiar with themethods used. Appropriate sensitivity should be given to the number oftests and procedures to which the patient will be submitted beforeformulating a diagnosis and treatment plan.
THERAPEUTIC OPTIONS
The goal of therapy in the patient presenting with virilization isclear. It consists of identifying the underlying cause and correcting it.Most often, the virilization is related to a malignant process and requiresa surgical approach.
In contrast, the management of hirsutism is generally multifaceted.It involves two separate but linked goals: (1) the prevention of furtherstimulation of hair growth and (2) cosmetic correction of the problem.The management plan should be structured and clear to the patientfrom the onset. The basic steps in the management of hirsutism areas follows:
• Define the problem• Quantify the degree of hirsutism• Identify pathophysiology• Correct the problem, whether acute or chronic• Define success with the patient• Follow-up
When selecting the appropriate therapeutic modality to correct thehirsutism, the clinician should consider both a short- and long-termperspective. A key element of any therapeutic plan is to define whatwill ultimately be viewed as successful therapy by the patient. Regular
92 PLOUFFE
follow-up is indicated at appropriate intervals, usually, every 3 to 6months.
General Measures
Treatment is targeted at the underlying cause. Several measures areindicated in most cases:
• Eliminate causative factors• Optimize weight• Manage hair
BleachingCutting or shavingElectrolysisLaser epilation
Any exogenous source of androgens should be avoided. Achievinga normal body weight is highly desirable; obesity is linked to chronicanovulation, insulin resistance, and lowered circulating levels of SHBG.
Ultimately, medical therapies can slow or halt the further growth ofhair but will not reverse an already established hair pattern. The approach to managing existing hair growth varies among clinicians. Somephysicians advocate an initial attempt at reducing the visible nature ofthe hair with bleachmg.v 26 Ultimately, the author prefers some form ofhair removal. Hair must be removed to its base within the hair follicleso that the follicle is eradicated or the next hair emerging from thatfollicle is exposed to the improved hormonal environment induced bythe concurrent medical therapy. Medical electrolysis is an effective wayof achieving hair removal." Recently, laser-assisted hair removal hasbeen performed.w " Little evidence suggests that this newer modalityoffers much advantage over traditional electrolysis.
Management of Excess Ovarian Androgen Production
The most common cause of hirsutism is PCOS.7 The standard therapy in these patients includes the use of a combined estrogen-progestinpreparation, most commonly administered as a combined oral contraceptive preparation.t- 26 This approach is extremely sound on scientificgrounds because it reduces the ovarian production of androgens, increases serum levels of SHBG, and induces competition at the cellularlevel for binding to the androgen receptor. Offering this form of therapyto the adolescent patient may be met with great resistance by the parents,who become concerned that the use of a contraceptive preparation willencourage their daughter to become sexually active. An open discussionwith the parents and the patient usually is adequate to clear up anymisunderstanding.
Much controversy remains regarding the choice of an oral contra-

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 93
ceptive preparation for the management of hirsutism. Based on primarilypreclinical data, some investigators believe that certain progestins arepreferable to others." Other researchers maintain that all preparationsare comparable in efficacy."
Comparative studies have been reported, and others are underway.Some studies have failed to demonstrate any clinical difference amongdifferent preparations." In the United States, the only oral contraceptivepreparation for which data have been presented to the Food and DrugAdministration to obtain an on-label indication for acne is the combination of ethinyl estradiol and norgestimate (Ortho Tri-Cyclen packageinsert [Ortho-McNeil Pharmaceutical, Raritan, NJ]). No preparation inthe United States has received on-label approval for the management ofhirsutism. In many other countries, cyproterone acetate is available andis used as the progestin component of oral contraceptives.
Another therapeutic approach for excess androgen productionfrom the ovaries is to achieve ovarian suppression with a long-actinggonadotropin-releasing hormone analogue (GnRHa). The effectivenessof this therapy has been demonstrated in the context of functionalovarian androgen overproduction as well as malignant ovarianconditions.v " This approach is effective as a single-agent treatmentmodality, with long-acting GnRHa preparations including leuprolide,buserelin, triptorelin, and goserelin,v 19,57,61 Because of the hypoestrogenic consequence of this form of therapy a more rational long-termmanagement strategy is to combine long-acting GnRHa therapy withestrogen or estrogen-progestin therapy.t- 45, 57 It is unclear whether thiscombined form of therapy offers any advantage over more traditionalapproaches.l- 4, 13,14,39,57
Over the past decade, there has been increasing interest in therelationship between PCOS and insulin resistance. Two cutaneous manifestations of insulin resistance are hirsutism and acanthosis nigricans.Several studies have looked at the effects of insulin-sensitizing agentson PCOS and hirsutism. The agents studied to date include metforminand troglitazone.v
Management of Excess Adrenal Androgen Production
Most patients who present with adrenal androgen overproductionas the source of hirsutism have a steroid synthesis enzymatic defect. Forthese patients, the primary therapeutic modality is metabolic correctionof the disorder, usually with exogenous corticosteroids.
Agents to suppress adrenal androgen production, such as dexamethasone, have been advocated as essential components in the medicalmanagement of hirsutism." The author believes there is a limited role forcorticosteroid therapy in the management of hirsutism in the adolescentpatient unless it is absolutely mandated and a definite adrenal enzymedeficiency has been idennfied,s« 62

94 PLOUFFE
Management Directed to the Target Organ and Cells
Several therapies target the androgen receptor as they compete withtestosterone during binding. These therapies include antiandrogens suchas spironolactone, flutamide, and ketoconazole. Although not currentlyavailable in the United States, cyproterone acetate is widely used inother countries in the management of hirsutism.v- 63, 73, 74
Spironolactone is by far the best studied antiandrogenic agent forhirsutism and is the gold standard with which other preparations arecompared.w 57, 62, 65 Mechanisms of action of spironolactone in the management of hirsutism include androgen receptor blockade, the suppression of adrenal androgen biosynthesis, and increased metabolic clearanceof testosterone with increased conversion of androgens to estrogens."The usual dosage ranges from 50 to 200 mg/ d in two divided doses.Spironolactone is used concurrently with oral contraceptives in a wellestablished combination regimen.
Flutamide acts by blocking the androgen receptor and decreasingadrenal androgen production." It has been shown to be effective in themanagement of hirsutism.w 50, 51 One report suggests that flutamide mayhave a role as a primary therapeutic modality in patients with PCOS.20Several studies have investigated the combination of flutamide with anoral contraceptive. Although this combination is effective, few datasuggest a marked increase in efficacy in comparison with the oral contraceptive regimen alone."
Ketoconazole has been shown to be equally effective as other treatment modalities.s- 40 Its use has been associated with hepatic failure, andthe author cannot justify its use over other equally effective options."
Finasteride inhibits Sa-reductase and reduces androgen input withinthe cell. Recent studies suggest a potential role for finasteride in themanagement of hirsutism.15, 17, 28, 29, 63, 79 It is unclear whether it offersmuch advantage over other therapies. In addition, the agent is teratogenic, and undermasculinization of a male fetus would most likely resultwith exposure to finasteride during pregnancy. More research is neededbefore this therapy can be used in a clinical setting.
Several clinical trials have compared the various agents targetingthe androgen receptor or cellular mechanism. Some of these studies,such as trials of cimetidine, have demonstrated little clinical efficacy.Overall, there seems to be little difference between the effectiveness ofthese agents.s- 30, 33
Selecting the Best Medical Therapy
Current data suggest that most therapies for hirsutism are comparable in efficacy. The dominant consideration in the selection of treatmentis the safety and tolerability of the approach. The choice should be madein close consultation with the patient.
Correction of an underlying medical disorder is the primary thera-

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 95
peutic target. This treatment includes correction of a thyroid disorder orhyperprolactinernia or long-term therapy for an adrenal enzyme deficiency. Because many patients who present with hirsutism manifestsigns of peas, oral contraceptives are a frequent treatment modality.
The best therapy encompasses an approach that is familiar to theclinician and that instills confidence. For most patients, this regimenincludes an oral contraceptive preparation and an antiandrogen, usually,spironolactone. The first step in management of the refractory patientshould be to assess adherence to the therapy and the selection of thespecific contraceptive preparation. Although most oral contraceptivesare effective, in some patients, the response differs markedly from onepreparation to another, and the least androgenic preparations should betried before moving on to other forms of therapy. In patients receivinglow-dose spironolactone, the dosage should be increased to 200 mg/ dbefore switching to another antiandrogen.
Approximately 75% to 80% of patients can be expected to show aresponse. An interval of 3 to 6 months is needed before an effect oftreatment is seen. Once a positive response is achieved, the treatmentshould be continued for at least another 6 months and, in most cases,should be continued for a number of years. Although little informationis available on the appropriate duration of therapy, some improvementin the underlying condition can be expected over time.
For patients who are truly refractory to an approach combining oralcontraceptives and spironolactone, other therapeutic modalities can beconsidered. Many of these therapies are still experimental, and patientsshould be monitored closely.
FUTURE PERSPECTIVES
Knowledge of the hair growth cycle is increasing." These scientificinsights may ultimately yield new therapeutic approaches focused onthe specific phase of hair cell growth relevant to hirsutism." New therapeutic compounds under development may provide improved efficacyand safety when compared with current progestational or antiandrogenic agents.s- 37,65
SUMMARY
Virilization is most often the reflection of a serious underlyingcondition. Diagnosis and management should be prompt, thorough, andcomprehensive. Hirsutism is the manifestation of a variety of disorders.It may be associated with serious acute medical conditions, chronicdisorders, or idiopathic. The diagnosis should be methodical and adjusted to the nature of the clinical presentation. Several therapeuticmodalities are effective and produce satisfactory results for most patients.

96 PLOUFFE
References
1. Acien P, Mauri M, Gutierrez M: Clinical and hormonal effects of the combinationgonadotrophin-releasing hormone agonist plus oral contraceptive pills containing ethinyl-oestradiol (EE) and cyproterone acetate (CPA) versus the EE-CPA pill alone onpolycystic ovarian disease-related hyperandrogenisms. Hum Reprod 12:423-429, 1997
2. Ambrosi B, Re T, Passini E, et al: Value of buserelin testing in the evaluation of hirsutewomen. J Endocrinol Invest 19:204-209, 1996
3. Azziz R, Owerbach D: Molecular abnormalities of the 21-hydroxylase gene in hyperandrogenic women with an exaggerated 17-hydroxyprogesterone response to short-termadrenal stimulation. Am J Obstet Gynecol 172:914-918, 1995
4. Azziz R, Ochoa TM, Bradley EL [r, et al: Leuprolide and estrogen versus oral contraceptive pills for the treatment of hirsutism: A prospective randomized study. J ClinEndocrinol Metab 80:3406-3411, 1995
5. Azziz R, Waggoner WT, Ochoa T, et al: Idiopathic hirsutism: An uncommon cause ofhirsutism in Alabama. Fertil Steril 70:274-278, 1998
6. Barth JH: The life-cycle of hair: Normal and abnormal growth patterns. In Adashi EY,Rock j.A, Rosenwaks Z (eds): Reproductive Endocrinology, Surgery, and Technology.Philadelphia, Lippincott-Raven, 1996, pp 1489-1499
7. Berga 5L: The obstetrician-gynecologist's role in the practical management of polycysticovary syndrome. Am J Obstet Gynecol 179(6 Pt 2):S109-5113, 1998
8. Bertoli A, Fusco A, Magnani A, et al: Efficacy of low-dose GnRH analogue (Buserelin)in the treatment of hirsutism. Exp Clin Endocrinol Diabetes 103:15-20, 1995
9. Blanche H, Vexiau P, Clauin 5, et al: Exhaustive screening of the 21-hydroxylase genein a population of hyperandrogenic women. Hum Genet 101:56-60, 1997
10. Botchkarev VA, Welker P,Albers KM, et al: A new role for neurotrophin-3: Involvementin the regulation of hair follicle regression (catagen). Am J Pathol 153:785-799, 1998
11. Burkman RT [r: The role of oral contraceptives in the treatment of hyperandrogenicdisorders. Am JMed 98(1A):130S-136S, 1995
12. Cara JF, Rosenfield RL: Androgens and the adolescent girl. In Sanfilippo IS, MuarmD, Lee PA (eds): Pediatric and Adolescent Gynecology. Philadelphia, WB Saunders,1994, pp 250-277
13. Carmina E, Lobo RA: Gonadotrophin-releasing hormone agonist therapy for hirsutismis as effective as high dose cyproterone acetate but results in a longer remission. HumReprod 12:663-666, 1997
14. Carr BR, Breslau NA, Givens C, et al: Oral contraceptive pills, gonadotropin-releasinghormone agonists, or use in combination for treatment of hirsutism: A clinical researchcenter study. J Clin Endocrinol Metab 80:1169-1178, 1995
15. Castello R, Tosi F, Perrone F, et al: Outcome of long-term treatment with the 5 alphareductase inhibitor finasteride in idiopathic hirsutism: Clinical and hormonal effectsduring a l-year course of therapy and l-year follow-up. Ferti! Steri! 66:734-740, 1996
16. Chien RN, Yang LI, Lin PY, et al: Hepatic injury during ketoconazole therapy inpatients with onychomycosis: A controlled cohort study. Hepatology 25:103-107, 1997
17. Ciotta L, Cianci A, Calogero AE, et al: Clinical and endocrine effects of finasteride, a5 alpha-reductase inhibitor, in women with idiopathic hirsutism. Fertil 5teri! 64:299306, 1995
18. Coenen CM, Thomas CM, Borm GF, et al: Comparative evaluation of the androgenicityof four low-dose, fixed-combination oral contraceptives. Int J Fertil Menopausal Stud40(suppl 2):92-97, 1995
19. Dahlgren E, Landin K, Krotkiewski M, et al: Effects of two antiandrogen treatmentson hirsutism and insulin sensitivity in women with polycystic ovary syndrome. HumReprod 13:2706-2711, 1998
20. De Leo V, Lanzetta D, D' Antona D, et al: Hormonal effects of flutamide in youngwomen with polycystic ovary syndrome. J Clin Endocrinol Metab 83:99-102, 1998
21. De Leo V, la Marca A, Lanzetta D, et al: Effects of flutamide on pituitary andadrenal responsiveness to corticotrophin releasing factor (CRF). Clin Endocrinol (Oxf)49:85-89, 1998
22. Dodin S, Faure N, Cedrin I, et al: Clinical efficacy and safety of low-dose flutamide

DISORDERS OF EXCESSIVEHAIR GROWTH IN THE ADOLESCENT 97
alone and combined with an oral contraceptive for the treatment of idiopathic hirsutism. Clin Endocrinol (Oxf) 43:575-582, 1995
23. Dumesic DA, Herrmann RR, O'Brien AM: Estimated prevalence of undiagnosed glucose intolerance from hyperandrogenic anovulation among women requesting electrolysis. Int J Ferti! Womens Med 42:255-260,1997
24. Dunaif A: Hyperinsulinemic hyperandrogenemia. In Adashi EY, Rock JA, Rosenwaks Z(eds): Reproductive Endocrinology, Surgery, and Technology. Philadelphia, LippincottRaven, 1996, pp 1521-1537
25. Ebling FJ: The biology of hair. Dermatol Clin 5:467-481, 198726. Emans SJ, Laufer MR, Goldstein DP: Endocrine abnormalities associated with hirsu
tism. In Pediatric and Adolescent Gynecology, ed 4. Philadelphia, Lippincott-Raven,1998, pp 263-301
27. Erenus M, Yucelten 0, Gurbuz 0, et al: Comparison of spironolactone-oral contraceptive versus cyproterone acetate-estrogen regimens in the treatment of hirsutism. FertilSteril 66:216-219, 1996
28. Erenus M, Yucelten 0, Durmusoglu F, et al: Comparison of finasteride versus spironolactone in the treatment of idiopathic hirsutism. Fertil Steril 68:1000-1003, 1997
29. Faloia E, Filipponi S, Mancini V, et al: Effect of finasteride in idiopathic hirsutism. JEndocrinol Invest 21:694-698, 1998
30. Falsetti L, De Fusco 0, Eleftheriou G, et al: Treatment of hirsutism by finasteride andflutamide in women with polycystic ovary syndrome. Gynecol Endocrinol 11:251257, 1997
31. Falsetti L, Rosina B, De Fusco D: Serum levels of 3u-androstanediol glucuronide inhirsute and nonhirsute women. Eur J Endocrinol 138:421-424, 1998
32. Foster RH, Wilde MI: Dienogest. Drugs 56:825-833, 199833. Fruzzetti F, Bersi C, Parrini 0, et al: Treatment of hirsutism: Comparisons between
different antiandrogens with central and peripheral effects. Ferti! Steri! 71:445-451, 199934. Gatee GB, Al Attia HM, Salama IA: Hirsutism in the United Arab Emirates: A hospital
study, Postgrad Med J 72:168-171, 199635, Gokmen 0, Senoz S, Gulekli B, et al: Comparison of four different treatment regimens
in hirsutism related to polycystic ovary syndrome, Gynecol Endocrinol 10:249-255,1996
36, Greenblatt RB: Factors influencing the growth of sexual hair, In The Hirsute Female,Springfield, IL, Charles C. Thomas, 1963, pp 3-19
37, Guarna A, Belle C, Machetti F, et al: 19-Nor-1O-azasteroids: A novel class of inhibitorsfor human steroid 5u-reductases 1 and 2, J Med Chern 40:1112-1129, 1997
38, Habif TP: Hair Diseases in Clinical Dermatology, ed 2. St. Louis, CV Mosby, 1990,pp 598-615
39. Heiner JS, Greendale GA, Kawakami AK, et al: Comparison of a gonadotropinreleasing hormone agonist and a low dose oral contraceptive given alone or togetherin the treatment of hirsutism, J Clin Endocrinol Metab 80:3412-3418, 1995
40. Isik AZ, Gokmen 0, Zeyneloglu HB, et al: Low dose ketoconazole is an effective anda relatively safe alternative in the treatment of hirsutism, Aust N Z J Obstet Gynaecol36:487-489, 1996
41. Kelestimur F, Sahin Y, Ayata D, et al: The prevalence of non-classic adrenal hyperplasiadue to 11 beta-hydroxylase deficiency among hirsute women in a Turkish population.Clin Endocrinol (Oxf) 45:381-384, 1996
42. Kelestimur F, Sahin Y: Comparison of Diane 35 and Diane 35 plus spironolactone inthe treatment of hirsutism, Ferti! Steri! 69:66-69, 1998
43. Knochenhauer ES, Cortet-Rudelli C, Cunnigham RD, et al: Carriers of 21-hydroxylasedeficiency are not at increased risk for hyperandrogenism. J Clin Endocrinol Metab82:479-485, 1997
44, Knochenhauer ES, Key TJ, Kahsar-Miller M, et al: Prevalence of the polycystic ovarysyndrome in unselected black and white women of the southeastern United States: Aprospective study, J Clin Endocrinol Metab 83:3078-3082, 1998
45. Lemay A, Faure N: Sequential estrogen-progestin addition to gonadotropin-releasinghormone agonist suppression for the chronic treatment of ovarian hyperandrogenism:A pilot study, Clin Endocrinol Metab 79:1716-1722, 1994

98 PLOUFFE
46. Mastorakos G, Chrousos GP: Adrenal hyperandrogenism. In Adashi EY, Rock JA,Rosewaks Z (eds): Endocrinology, Surgey, and Technology. Philadelphia, LippincottRaven, 1996, pp 1539-1553
47. Mestayer C, Berthaut I, Portois MC, et al: Predominant expression of 5a-reductasetype 1 in pubic skin from normal subjects and hirsute patients. J Clin EndocrinolMetab 81:1989-1993, 1996
48. Moghetti P, Castello R, Negri C, et al: Flutamide in the treatment of hirsutism: Longterm clinical effects, endocrine changes, and androgen receptor behavior. Fertil Steril64:511-517, 1995
49. Morin-Papunen LC, Koivunen RM, Ruokonen A, et al: Metformin therapy improvesthe menstrual pattern with minimal endocrine and metabolic effects in women withpolycystic ovary syndrome. Pertil Steril 69:691-696, 1998
50. Muderris II, Bayram F, Sahin Y, et al: The efficacy of 250 mg/ day flutarnide in thetreatment of patients with hirsutism. Fertil Steril 66:220-222, 1996
51. Muderris II, Bayram F, Sahin Y, et al: A comparison between two doses of flutamide(250 mg/ d and 500 mg/ d) in the treatment of hirsutism. Fertil Steril 68:644-647, 1997
52. Nayak S, Lee PA, Witchel SF: Variants of the type II 3beta-hydroxysteroid dehydrogenase gene in children with premature pubic hair and hyperandrogenic adolescents.Mol Genet Metab 64:18-92, 1998
53. New MI, Rapaport R: The adrenal cortex. In Sperling NA (ed): Pediatric Endocrinology.Philadelphia, WB Saunders, 1996, pp 281-314
54. O'Driscoll JB, Mamtora H, Higginson J, et al: A prospective study of the prevalenceof clear-cut endocrine disorders and polycystic ovaries in 350 patients presenting withhirsutism or androgenic alopecia. Clin Endocrinol (Oxf) 41:231-236, 1994
55. Pang S: Congenital adrenal hyperplasia. Baillieres Clin Obstet Gynaecol 11:281-306,1997
56. Paus R: Principles of hair cycle control. J Dermatol 25:793-802, 199857. Pazos F, Escobar-Morreale HF, Balsa J, et al: Prospective randomized study comparing
the long-acting gonadotropin-releasing hormone agonist triptorelin, flutamide, andcyproterone acetate, used in combination with an oral contraceptive, in the treatmentof hirsutism. Ferti! Steril 71:122-128, 1999
58. Prelevic GM: Hirsutism and the polycystic ovary syndrome. In Ginsburg J (ed): DrugTherapy in Reproductive Endocrinology. New York, Oxford University Press, 1996,pp 67-85
59. Richards RN, Meharg GE: Electrolysis: Observations from 13 years and 140,000 hoursof experience. J Am Acad Dermatol 33:662-666, 1995
60. Rittmaster RS: Clinical relevance of testosterone and dihydrotestosterone metabolismin women. Am J Med 98(lA):17S-21S, 1995
61. Rittmaster RS, Arab DM, Lehman L: Dose-response effect of depot, leuprolide acetateon serum androgens in hirsute women. Fertil Steril 65:912-915, 1996
62. Rittmaster RS: Functional hyperandrogenism. In Adashi EY, Rock JA, Rosenwaks Z(eds): Reproductive Endocrinology; Surgery, and Technology. Philadelphia, LippincottRaven, 1996, pp 1501-1520
63. Sahin Y, Bayram F, Kelestimur F, et al: Comparison of cyproterone acetate plusethinyl estradiol and finasteride in the treatment of hirsutism. J Endocrinol Invest21;348-352, 1998
64. Sawaya ME, Shalita AR: Androgen receptor polymorphisms (CAG repeat lengths) inandrogenetic alopecia, hirsutism, and acne. J Cutan Med Surg 3:9-15, 1998
65. Schmidt JB: Other antiandrogens. Dermatology 196:153-157, 199866. Sommer S, Render C, Burd R, et al: Ruby laser treatment for hirsutism: Clinical
response and patient tolerance. Br J Dermatol 138:1009-1014, 199867. Stratakis CA, Mastorakos G, Mitsiades NS, et al: Skin manifestations of Cushing
disease in children and adolescents before and after the resolution of hypercortisolemia. Pediatr Dermatol 15:253-258, 1998
68. Sullivan EJ: Art in dermatopathology. [usepe de Ribera. An interpreter of the skinthrough art. Am J Dermatopathol1:159-162, 1979
69. Sundararaman PG, Ammini AC, Khurana ML, et al: Late onset adrenal hyperplasia

DISORDERS OF EXCESSIVE HAIR GROWTH IN THE ADOLESCENT 99
due to 3 beta-hydroxy-delta 5-steroid dehydrogenase deficiency in north Indian hirsutewomen. Indian I Med Res 105:27-31, 1997
70. Swart E, Lochner ID: Skin conditions in epileptics. Clin Exp Dermatol17:169-172, 199271. Thorneycroft IH: Update on androgenicity. Am J Obstet Gynecol 180(2 Pt 2):288-294,
199972. Tosi A, Misciali C, Piraccini BM, et al: Drug-induced hair loss and hair growth:
Incidence, management and avoidance. Drug Saf 10:310-317, 199473. van Wayjen RG, van den Ende A: Experience in the long-term treatment of patients
with hirsutism and / or acne with cyproterone acetate-containing preparations: Efficacy,metabolic and endocrine effects. Exp Clin Endocrinol Diabetes 103:241-251, 1995
74. Venturoli S, Ravaioli B, Bagnoli A, et al: Contraceptive and therapeutic effectivenessof two low-dose ethinylestradiol and cyproterone acetate regimens in the treatment ofhirsute patients. Eur I Contracept Reprod Health Care 3:29-33, 1998
75. Vottero A, Stratakis CA, Ghizzoni L, et al: Androgen receptor-mediated hypersensitivity to androgens in women with nonhyperandrogenic hirsutism: Skewing of X-chromosome inactivation. J Clin Endocrinol Metab 84:1091-1095, 1999
76. Wheeland RG: Laser-assisted hair removal. Dermatol Clin 15:469-477, 199777. White E, Plouffe L [r, Gallup DG: Case of an androgen producing gonadal stromal
ovarian tumor suppressed by a long-acting GnRH agonist-leuprolide. Journal ofPelvic Surgery 2:1-5, 1996
78. Winter IS: Hyperandrogenism in female adolescents. Curr Opin Pediatr 488-493, 199379. Wong IL, Morris RS, Chang L, et al: A prospective randomized trial comparing
finasteride to spironolactone in the treatment of hirsute women. J Clin EndocrinolMetab 80:233-238, 1995
80. Wong IL, Lobo RA: Ovarian androgen-producing tumors. [n Adashi, EY Rock JA,Rosenwaksz (eds): Endocrinology, Surgery, and Technology. Philadelphia, LippincottRaven, 1996, pp 1571-1598
Address reprint requests toLeo Plouffe, [r, MD, CM
Lilly Research LaboratoriesUnited States Medical Endocrine Division
Drop Code 4121Eli Lilly and CompanyIndianapolis, IN 46285
e-mail: [email protected]