Embed Size (px)
Citation preview

DISCRIMINATION BEGINS IN THE WOMB: EVIDENCE OF SEX-SELECTIVEPRENATAL INVESTMENTS
PRASHANT BHARADWAJ & LEAH K. NELSON†
ABSTRACT. This paper investigates whether boys receive preferential prenatal treatment in a settingwhere son preference is present. Using micro health data from India, we highlight sex-selective prena-tal investments as a new channel via which parents can practice discriminatory behavior. We find thatmothers visit antenatal clinics and receive tetanus shots more frequently when pregnant with a boy. Pref-erential prenatal treatment of males is greater in regions known to have strong son preference and amongwomen whose previous children are female. We successfully rule out other mechanisms such as selectiverecall, medical complications that might cause male babies to receive greater prenatal care in general,son preference-based fertility stopping rules and reverse causality due to sex selective abortions. Ourcalculations suggest that sex-selective prenatal care in tetanus use explains between 4-10.5% of excessfemale neonatal mortality in India. We find similar results using data from other countries like China,Bangladesh and Pakistan; thus, we show the extent of sex selective prenatal care in large parts of Southand Southeast Asia.JEL Classifications: I18, J13, J16
† DEPARTMENT OF ECONOMICS, UNIVERSITY OF CALIFORNIA, SAN DIEGO
E-mail address: [email protected], [email protected]: October 2010.Thanks to Achyuta Adhvaryu, Sonia Bhalotra, Julie Cullen, Gordon Dahl, Gordon Hanson, James Fenske, Karthik Muralid-haran and Tavneet Suri for comments. Thanks also to Dr. Matangi Bala and Dr. Ram Krishnamoorthi for patiently answeringquestions related to prenatal care. Karina Litvak provided excellent research assistance. We thank the China Health andNutrition Survey, funded by NIH (R01-HD30880, DK056350, and R01-HD38700), and the Carolina Population Center andthe Chinese CDC for providing these data.
1

2 BHARADWAJ & NELSON
1. INTRODUCTION
Sex-based discrimination has been studied extensively in the context of son preference inSouth and Southeast Asia (Dreze and Sen 1989, Gupta 1987, Qian 2008). Differential care given toboys over girls and sex-selective abortions has resulted in an estimated 30 to 70 million "missing"women in India and China alone. While one might expect economic growth to erode such discrim-ination, son preference (as evidenced by skewed sex ratios) has been persistent despite high growthrates in these countries (Gupta et al. 2003). As a result, a large literature has tried to explain theobserved skewed ratios through post-birth discrimination strategies. Some of the channels examinedare (but not limited to) differential vaccination rates (Oster 2009), allocation of household resources(Pitt and Rosenzweig 1990), breastfeeding behavior (Jayachandran and Kuziemko 2009) and parentaltime allocation (Barcellos, Carvalho, and Lleras-Muney 2010). The papers that do examine sex-baseddiscrimination before birth focus on sex-selective abortions (Portner 2009, Meng 2010, Bhalotra andCochrane 2010). However, an unanswered question in this literature is whether parents invest less inprenatal care when pregnant with a girl, while still carrying the girl to term.1 Such discrimination canhave sizeable consequences as prenatal care is an essential component of the overall health of the child.
Maternal inputs during pregnancy can affect important outcomes such as neonatal survivaland birth weight (Gortmaker 1979, Bharadwaj and Eberhard 2010). In India, attending prenatal careis correlated with a 27% decrease in the probability of neonatal mortality (NFHS). Tetanus shots takenduring pregnancy play a particularly important role in neonatal survival;2 about 38% of child deaths(under 5 years) occur in the neonatal stage. Neonatal tetanus is the leading cause of neonatal deaths inIndia (Zupan and Aahman 2005, Gupta and Keyl 1998) and results in nearly 200,000 neonatal deathsper year in South and Southeast Asia (UNICEF 2000). Early childhood health not withstanding, wealso know from previous research that in utero events and childhood endowments affect later life health,IQ and labor market outcomes (Almond and Mazumder 2005, Black, Devereux, and Salvanes 2007,Behrman and Rosenzweig 2004, Almond, Chay, and Lee 2002).
This paper examines whether sex-selective prenatal care occurs in countries of South andSoutheast Asia, with an emphasis on India.3 We find significant differences in the prenatal health carechoices of women when they are pregnant with boys relative to when they are pregnant with girls. InIndia women are 1.1 percentage points more likely to attend prenatal care when pregnant with a boyand receive a significantly greater number of tetanus shots. In northern India, where sex discriminationis known to be more prevalent, women are 4.6% more likely to seek prenatal care and 3% percent morelikely to receive tetanus shots if they are pregnant with a boy. In the same region, women are 16% more
1Osmani and Sen (2003) examine fetal health in the context of sex-based discrimination, however, they do so from the channelof maternal health, and do not examine direct discrimination based on the sex of the fetus.2Blencowe et al (2010) summarize decades of research on the importance of tetanus immunization during pregnancy byconcluding that there is "clear evidence of the high impact of two doses of tetanus toxoid immunization given at least 4weeks apart on neonatal tetanus." After examining field studies that use various methods, they estimate that the decrease intetanus-related neonatal morality due to vaccination is around 94%. Other estimates from developing countries range from70% in rural Bangladesh to 88% in India (Rahman et al. 1982, Gupta and Keyl 1998) .3In this paper we are not able to distinguish between taste-based and statistical discrimination. Hence, in this exercise, wesimply document differential treatment for sons relative to daughters. The mechanism that drives these actions could be ataste for sons or a demand for sons based on the rates of returns to or costs of raising a son.

SEX-SELECTIVE PRENATAL CARE 3
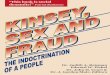
likely to deliver their baby in a non-home environment if pregnant with a boy. We also find that womenwhose previous children were mainly girls tend to discriminate more when the current fetus is male(see Figure 1). Moreover, for a subset of the Indian data, we find that prenatal discrimination occurslargely among mothers who report having received an ultrasound during pregnancy. We find similarevidence in other countries of South and Southeast Asia were sex discrimination has been documented.For example, in China, women pregnant with boys are nearly 6% percent more likely to seek prenatalcare. Mothers in Pakistan are 6% more likely to take iron supplements and mothers in Bangladeshattend prenatal care 7% more frequently when pregnant with a boy.
Apart from examining a new parental avenue for gender discrimination, we also bring newperspective to the vast literature on parental investments (Rosenzweig and Zhang 2009, Ashenfelter andRouse 1998, Behrman, Rosenzweig, and Taubman 1994) that examines whether schooling or nutrition-based investments reinforce (or are affected by) the distribution of initial endowments. The notionof "initial endowments" is often related to birth weight (Loughran, Datar, and Kilburn 2004) or theresidual of a human capital production function (Pitt and Rosenzweig 1990).4 Our paper adds to theliterature on parental investments by showing that initial endowments (even within families) are subjectto preferences over gender. Thus, beyond the usual concerns with endogenous endowment formationlike maternal behavior, genetic correlations et cetera, we put forth gender preferences as an additionalchannel for consideration when examining the impact of initial endowments on short and long termoutcomes.
A common policy to address sex discrimination is to prohibit health professionals from re-vealing the sex of the fetus during ultrasound exams, as India did in the mid-1990s. Despite the legalefforts of the government, sex-selective abortions have risen in recent years in India (Arnold, Kishor,and Roy 2002, Bhalotra and Cochrane 2010) and the policy focus has been on trying to stamp it out;we make the point that even if all policy efforts were diverted to reduce the incidence of sex-selectiveabortions, an unintended consequence of such efforts could be a rise in differential investments in pre-natal care. Our calculations suggest preferential treatment in one such investment, tetanus shots, canexplain 4-10.5% of the excess female neonatal mortality. Hence, if gender equality is a priority, policymust be concerned about the possibility of discriminatory prenatal care leading to long term differencesin the outcomes for men and women.
There are several identification problems that arise in the analysis of sex-based discrimination.The four main problems we address are selective recall, biological characteristics of male fetuses thatmay drive the need for additional prenatal care, son preference-based fertility stopping rules and sex-selective abortions. First, what if mothers are more likely to remember prenatal investments whenthey give birth to a boy? We mitigate this concern by examining periods before ultrasound technologybecame widely available and by assessing prenatal care that takes place early in the pregnancy, beforesex determination is possible. We do not find any evidence that male fetuses received extra prenatal carebefore ultrasound technology became widespread or before parents know the gender of the fetus. Asidefrom helping us rule out selective recall bias, this result suggests that this form of gender discrimination
4More recently, Aizer and Cunha (2010) measure initial endowment as scores from the Bailey test administered to 8 monthold babies.

4 BHARADWAJ & NELSON
is a recent phenomenon and one that likely goes hand-in-hand with technological advances (portableultrasounds in particular). Second, what if the biological needs of a male fetus dictates greater prenatalcare? To address this issue, we examine data on pregnancy complications. We do not find that womenexperience increased medical complications during pregnancies that result in a male birth. Moreover,if there were biological reasons for differential prenatal investments along the dimensions of iron pillsor tetanus shots,5 then we should observe that males in countries with no son preference also receivemore prenatal investments. We do not find any evidence towards this when we examine countries likeThailand, Ghana and Sri Lanka where son preference is rather weak.
Third, what if son preference-based stopping rules increase the probability of observing amale birth at higher birth orders? We account for this by directly including birth order and existing sexratios of the other children as controls in all specifications, as well as restricting the analysis to childrenwho are "young enough" at the time of the survey (we adopt this approach from Barcellos, Carvalho,and Lleras-Muney (2010)). As preferences for gender composition might be correlated with sex of thelast observed child, looking only at the most recent birth when the child is "young enough" allows us tostudy prenatal investments before parents are able to adjust their fertility based on the sex of the mostrecent child.6
Fourth, the presence of sex-selective abortions - which we do not observe in our data - areproblematic to our approach for several reasons. In the presence of selective abortions, our regressionsamples omit the subset of mothers who abort female fetuses. Any selection bias that results fromtheir omission will likely lead to an underestimate of the true gender gap in prenatal care as familiesthat perform sex-selective abortions represent a highly discriminatory part of the population and thesemothers would not have sought prenatal care had they been forced to take their female pregnancies toterm. Another concern arises if the receipt of prenatal care influences the gender of observed live birthsvia ultrasounds done at the time of prenatal check up and subsequent selective abortion. We show thatsuch reverse causation does not explain our results by examining investment behavior for the sampleof mothers who have attended prenatal care at least once and have thus already made abortion-relateddecisions. Even in this restricted sample, we find that mothers who are pregnant with boys continue toseek more prenatal care than their counterparts carrying daughters. This result is critical, as it indicatesthat sex determination leads to other forms of gender discrimination, above and beyond its effect onskewed sex ratios through sex-selective abortions. Finally, mothers who sex-selectively abort may havesystematically different preferences over prenatal care; if this is true, then non-randomness of fetalgender due to sex-selective abortions and unobserved preferences of these women may lead to a classicomitted variable bias. To address this issue, we show that even among children of the same mother,boys tend to receive greater prenatal care than girls. Hence, if omitted parental preferences are time
5In several conversations with medical practitioners, we learned that while there are significant biological differences amongfemale and male fetuses, these differences do not result in differential medical recommendations regarding prenatal carevisits, tetanus shots or iron pills.6A caveat here is that this method assumes no sex selective abortion. We show that even after adjusting the Barcellos etal (2010) strategy to account for potential reverse causality due to sex selective abortions, our estimated gender gap is stillsizeable and significant. Moreover, we provide reasons to believe that these estimates represent a lower bound for the truelevel of sex-selective prenatal care. We explain this in further detail later in the paper.

SEX-SELECTIVE PRENATAL CARE 5
invariant, then comparing the outcomes of siblings accounts for those variables. In our regressions,we also control for wealth and education, two critical factors that may determine both likelihood ofcommitting selective abortion and receiving prenatal care (Bhalotra and Cochrane 2010, Portner 2009).
The remainder of this paper is organized as follows: Section 2 provides a simple methodolog-ical framework for examining whether sex-selective prenatal investments occur and discusses possibleeconometric biases, Section 3 describes the various data sets we use in this paper, Section 4 discussesthe results and their ability to explain excess female neonatal mortality as well as presents a wide arrayof robustness checks that we employ and Section 5 concludes.
2. METHODOLOGY AND ESTIMATION ISSUES
Papers examining son preference in the US have examined the role of gender bias in dif-ferences in prenatal care (Dahl and Moretti 2004, Lhila and Simon 2008) using receipt of ultrasoundscanning during pregnancy as indication that the parents know the sex of the child. Unfortunately, dataon ultrasound receipt is inconsistent across the rounds of the National Fertility and Health Survey (for aselect subset of the Indian sample we do have this information; we discuss the use of this data in detailin the results section). However, we rely on the idea that in the absence of ultrasounds or other methodsof sex determination, there should be no systematic reason to find that males receive greater prenatalcare. This section describes our basic estimation strategy and outlines the various problems that couldhinder inference as well as our attempt to deal with each potential source of bias.
2.1. Basic Specification
Our strategy is built on the premise that under equal treatment or lack of knowledge of fetalgender, the eventual outcome of the pregnancy in terms of the gender of the child should not affectprenatal investments. To the best of our knowledge, doctor recommendations regarding basic prena-tal investments like iron pills, tetanus shots or regular prenatal check ups do not vary systematicallyby the gender of the child. Thus finding that antenatal visits, consumption of iron supplements andtetanus shots are more likely during a pregnancy that results in a male is strong suggestive evidence ofdiscrimination.
The empirical methodology this paper adopts is quite simple. If parents want to discriminatebased on the sex of fetus, pregnancies that result in a male child should be pregnancies with greaterobserved prenatal care along various dimensions. The basic specification we estimate is:
Cihj = βMaleihj + ηXihj +Dj + εihj(1)
Where Cihj is the type of prenatal investment for child i in household h in state j such as prenatal care,iron pills, tetanus shots, et cetera. Maleihj takes the value of 1 when the child is male. The questionsare retrospective, so the woman is asked about type of prenatal care while pregnant with a given childand then that particular child’s sex is noted (more details concerning the survey data can be found inthe next section). Xihj is a host of control variables that include birth order, age and education of themother, dummies of year of birth of the child, wealth quintiles and a dummy for whether or not themother resides in an urban area. Dj captures state fixed effects. If prenatal sex discrimination exists

6 BHARADWAJ & NELSON
and if males are favored, we should find that β is greater than zero.7 Several important identificationissues emerge when following this approach. We now review each problem and our proposed solutionsin detail.
2.2. Selective recall
It is possible to find a positive β if mothers are simply more likely to report receiving prenatalcare when pregnant with a boy even if actual prenatal care is not gender-biased. If males are indeedpreferred, then activities that led to a male birth might be better remembered. To counter this potentialselective recall concern we adopt two approaches. First we rely on the timing of spread of ultrasoundtechnology. Ultrasound availability in India is well documented. There are reports in India that the firstultrasound clinic was opened in the Punjab in 1979 (Washington Post, May 2006), but widespread useof ultrasound was not achieved until the mid to late 1990s (Miller 2001, Bhalotra and Cochrane 2010).8
The advent of ultrasounds - in particular, portable sonogram machines - has made sex determinationless risky, easier to access and less expensive (about $12 each, according to The Economist, March2010). Anecdotal evidence suggests that even rural areas are visited by itinerant doctors who carryultrasound machines from town to town, offering sex determination without official prenatal care (NewYork Times, May 2001).9 Thus, to tackle to issue of selective recall, we estimate of equation 1 usingthe NFHS survey conducted in 1992, before ultrasounds spread to many regions in India. If mothersare no more likely to remember prenatal care when they deliver boys than when they deliver girls, weexpect to find that β is small and statistically insignificant for this sample.
A second approach is to exploit the timing of prenatal care. Sex determination is typicallypossible in the third or fourth month of pregnancy. In the absence of selective recall, we should findthat prenatal care taken early in the pregnancy before sex determination is possible does not system-atically differ for female versus male fetuses. Thus we would expect β to be small and statisticallyindistinguishable from zero for prenatal investments made during the first four months of gestation.
7A related issue is that β might vary depending on the sex ratio of the previous children. Due to son preference-based fertilitystopping rules, "who" becomes a mother at each birth order is a selected sample. Suppose we restrict the sample to peoplewhose previous children are all girls (conditional on family size).
Cihj = βGMaleihj + γXihj +Dj + vihj
The coefficient we get onMale in this sample (βG) will likely be different from the coefficient onMale if we were to estimateequation 2 for families whose previous births are all male (call this βM ). Hence, β from equation 1 should be interpreted as aweighted averaged of βG and βM , where the weights depend on the fraction of the population that discriminate against girlsin their last birth. We show estimates of βG and βM for various birth orders in Figure 1. As expected βG > βM across mostof the birth orders.8Prior to ultrasounds, sex determination was accomplished primarily through the use of amniocentesis, a more invasiveprocedure involving the removal of amniotic fluid through a needle inserted into the maternal abdomen. For an excellentreview on the timing of ultrasound technology spread see Bhalotra and Cochrane (2010).9As we present results from China later in the paper, it is useful to mention that in China, ultrasound technology becameavailable as early as 1965 in a few counties but coverage did not accelerate until the 1980s; by the end of the 1980s muchof the country had access to an ultrasound machine (Meng 2010). For details on the spread of ultrasound machines and itsconsequences for sex-selective abortion in China, please see Meng (2010).

SEX-SELECTIVE PRENATAL CARE 7
2.3. Medical complications
It is possible that male fetuses simply require more prenatal care than female fetuses. Hence,a concern could be that medical reasons rather than gender discrimination drive parents to give moreprenatal care to male fetuses than female fetuses. We attempt to rule out this alternate explanation byexamining data on pregnancy complications. The NFHS collects detailed data on pregnancy complica-tions such as fatigue, night blindness, excessive bleeding, et cetera. Our concern would be mitigated ifpregnancies that end in a male birth are not associated with significantly more complications than thoseending in a female birth.
2.4. Son preference based fertility stopping rules
One potential source of bias in equation 1 arises due to son preference-based stopping rules.A consequence of son preference-based fertility stopping rule is that the probability the youngest childis male is increasing in the age of the last child, as parents have more time to adjust their total fertilityfollowing the birth (Barcellos, Carvalho, and Lleras-Muney 2010). Conditional on family size, thiswould imply that a family whose most recent birth was female would have weaker son preference evenafter controlling for birth order and the existing sex ratio of the child’s siblings. Since the questions onprenatal care are asked only for the youngest child of the mother, our results are susceptible to bias dueto such a stopping rule. As a robustness check, we employ the methodology developed in Barcellos,Carvalho, and Lleras-Muney (2010).
The main idea behind the Barcellos, Carvalho, and Lleras-Muney (2010) methodology is toexamine families where the last child is "young enough" such that parents have not had time to adjusttheir fertility based on the gender of the most recent birth - for this sample, parents who have just had agirl are similar to parents to have just had a boy, conditional on the sex ratio of the previous children andthe number of children. However, their methodology relies on the absence of sex-selective abortions.Nevertheless, we include it in our robustness check and find the estimates to be unchanged; if anythingthe "young enough" sample results are slightly larger in magnitude than the overall sample results.
2.5. Sex selective abortions
The potential for sex-selective abortions brings about three additional concerns in our estima-tion: sample selection bias, reverse causality and omitted variables bias. These concerns are certainlyrelated, but dealing with each separately provides insight into various estimation techniques we use toaccount for these issues.
2.5.1. Sample selection. Because we only observe the gender and prenatal care of pregnancies re-sulting in live births, our sample omits those female fetuses who were terminated before birth. Thisintroduces bias into our estimates if those who abort female fetuses would have given their unborndaughters significantly different levels of prenatal care if forced to take them to term than those whochoose to take female fetuses to term. We believe that parents who perform sex selective abortions arethose for whom son preference (and female discrimination) is strongest; if these parents were forcedto carry the female fetus to term, it is likely that these girls would receive less prenatal care than those

8 BHARADWAJ & NELSON
born to parents who prefer to take their female pregnancies to term. Hence, we expect our results to beunderestimates of the true extent of gender discrimination in prenatal care.
2.5.2. Reverse causality. The presence of sex-selective abortions could also bring into question thedirection of causation between prenatal care and fetal gender. If ultrasounds are a routine proceduretaken during formal prenatal visits, then women who seek prenatal care may discover they are carryinggirls and choose to abort, leading to a mechanical correlation between the gender of the fetus andmeasures of prenatal care. Our estimation of equation 1 compares the prenatal care received by boysand girls who have not been selectively aborted. Because fewer girls survive past the first prenatalcheckup (and thus drop out of our sample), we should observe that a higher proportion of boys receiveprenatal care than girls under sex-selective abortions. This would lead us to the false conclusion thatthe gender of the unborn child determines prenatal care - our estimate of β in equation 1 would bepositive - when in fact prenatal care determines the gender of the children we observe in our sample.
Without information on the exact timing of ultrasound receipt in relation to subsequent pre-natal care (which is not available in the NFHS), we are unable to isolate the direction of causationbetween the first prenatal visit and fetal gender. However, we can identify the causal effect of fetal gen-der on additional prenatal care, conditional on knowing the gender of the child and choosing to take thepregnancy to full term. If we assume that women who have been to at least 1 prenatal checkup knowthe sex of their unborn child, then their decision to pursue additional prenatal care is not subject to thesame argument of reverse causality because they make these subsequent decisions after choosing notto abort their unborn child. In practice, we can restrict the estimation sample to those women who havegone to at least 1 prenatal visit (where we assume that they learned the sex of the child) and estimatethe following regression:
Additional Cihj = βMaleihj + ηXihj +Dj + εihj
β now captures the gender differential in prenatal care that occurs after the first checkup andis free of any reverse causality concerns. We can further restrict the sample to those women whose firstprenatal checkup occurred after the fifth month of pregnancy and are thus the most likely to learn thesex of the fetus during the first checkup. Note that this approach does not solve the problem related tosample selection, and the possibility of sex-selective abortions still leads to a potential underestimateof the true degree sex-selective prenatal investments.
2.5.3. Other omitted variables. If we instead interpret the problem of sex-selective abortions as a casein which the propensity to perform selective abortions is an omitted variable in our regressions, we areleft with a classic problem of endogeneity; the sex of the child is no longer random and is potentiallycorrelated with εihj . In general, the direction of bias depends on the relationship between factors thatinfluence sex-selective abortions and how these factors affect the demand for prenatal care. In ourattempt to deal with the this type of bias, we also control for various factors like wealth and educationwhich might be important determinants of sex-selective abortions. If abortions are costly, then also

SEX-SELECTIVE PRENATAL CARE 9
including a control for family wealth is important, as wealthier families are both more likely to have amale child (by aborting female fetuses)10 and better able to afford prenatal care.11
If parental preferences over gender composition of children and factors that jointly determinesex-selective abortions and prenatal care are time invariant, then a mother fixed effects specificationshould be a robust way of countering the endogeneity concerns raised in the previous section. Insome cases we have information on prenatal care for the previous two births of the same woman.In this instance, we can test whether sons receive greater prenatal care using a mother fixed effectsspecification. The basic specification in this case is:
Cih = φMaleih + ηXih +Mh + εih(2)
Where Cih is the type of prenatal investment for child i born to a mother in household h. Maleih
takes the value of 1 when the child is male, Xih consists of control variables such as dummy variablesfor year of birth of the child, birth order and the existing sex ratio of children. Mh captures motherfixed effects including time invariant preferences for gender and prenatal care. Hence, if prenatal sexdiscrimination exists, we should find that φ is greater than zero.
As long as parental preferences for gender composition and unobserved determinants of selec-tive abortions and prenatal care are captured by the mother fixed effect, there is no reason to think thatMaleih is correlated with εih in equation 2 and the fixed effects specification provides an alternativeway of examining the presence of selective prenatal care. However, the caveat is that the sample onlyincludes mothers who have given birth twice in the five years prior to the survey. Hence, there mightbe some concerns with drawing conclusions about the general population from this sample.
3. DATA
The data on pregnancies and prenatal investments used in this paper come from a wide arrayof sources that vary by country. The Indian sample is created using the 1998-9 and 2005-6 roundsof the National Family Health Survey (NFHS). The Bangladeshi sample draws from four waves ofthe Demographic and Health Survey (DHS), including the 1996-7, 1999-2000, 2004 and 2007 rounds.Lastly, the Chinese data come from the China Health and Nutrition Survey (CHNS), an ongoing projectthat collects panel data from 9 provinces. For this paper, we use the 1991, 1993, 1997, 2000, 2004 and2006 rounds. Additional robustness checks uses samples drawn from other DHS rounds in Pakistan(2006-7), Ghana (1993, 1998, 2003, 2008), Sri Lanka (1987) and Thailand (1987). The NFHS and allDHS rounds are comprised of nationally representative samples with respect to each country. AppendixTable 1 displays general descriptions of all samples used in this paper.
Although the data in the paper are collected from many different sources, the method ofconstructing the estimation samples is very similar across all countries. Within each country we use
10While the daily agricultural wage in India was around 57 rupees/day in 1998-9 (and also in 2000-1), the cost of an abortionranges from Rs. 500 (by makeshift midwives) to over Rs. 5000 when performed by a doctor. Because the wealth quintilecalculated by DHS is nationally representative, we employ national sampling weights in all regressions that include wealth.11According to Portner (2010) women with at least one boy and women with less than 8 years of education almost neverpractice sex-selective abortions during subsequent pregnancies. We get largely similar results when we restrict our sample tomothers who have had at least one boy and with low levels of wealth and education (results not shown).

10 BHARADWAJ & NELSON
the sample of ever married women generally between the ages of 15 and 49. Information is collectedretrospectively about the pregnancy history of each woman, including detailed prenatal investment datafrom the most recent pregnancy previous to the survey. In the 1998 round of the NFHS, mothers reportinformation about their two most recent pregnancies, allowing for the construction of a panel datasetsuitable for fixed effects estimation (see previous section). We collect basic information such as ageand educational attainment about mothers and wealth quintile of the family, as well as geographicaldata about their place of residence which is used to generate the spatial fixed-effects included in allsubsequent regressions. Summary statistics for mother characteristics are presented in Appendix Table2 for India (not shown for the remaining countries). Average educational attainment is generally lowbut displays considerable variation across countries. In India, the average mother in the sample is 28years old and has completed only primary school.
With the exception of the fixed effects specifications, we restrict our attention to the mostrecent birth previous to the survey. In order to obtain the most accurate information, we consider onlythose births that have occurred in the 5-year span leading up to the survey round. Appendix Table 2indicates that about 55% of pregnancies are male in India. In countries with low or no son preference(Ghana, Sri Lanka and Thailand), male pregnancies occur only 51% to 52% of the time; however incountries with stronger son preference (China, Bangladesh, Pakistan), the ratio is generally higher,with 56% of Chinese pregnancies resulting in live birth being male.12 We focus our attention on thefollowing measures of prenatal investments, although not all variables are available for all rounds inall countries: prenatal care and the number of visits, tetanus shots received and iron supplements takenduring pregnancy and whether the mother chose to deliver her child in a health facility or at home.Appendix Table 2 displays the summary statistics for these outcomes of interest. Prenatal care andreceipt of tetanus shots is fairly common, occurring in about 72% and 78% of pregnancies in India,respectively. However, Indian women choose to give birth in a non-home facility for only 35% ofpregnancies.
4. RESULTS
We first present all of our results and robustness checks for the Indian case. In section 5.2,we show that the gender gap in prenatal care extends beyond India and can be found in other countrieswhere son preference is known to be prevalent (Pakistan, Bangladesh, China); we also present resultsfor countries with little known son preference (Ghana, Sri Lanka and Thailand) as a benchmark forcomparison. Finally, in section 5.3 we use our results to assess the impact of differential prenatal careon excess female neonatal mortality in India.
In Table 1, we estimate equation 1 for various subsamples of the National Family HealthSurvey in India. Overall, we see that males tend to receive significantly more prenatal investmentsacross almost every type of prenatal care (Appendix Table 3 shows that the coefficient of interestis stable across specifications where the independent variables are added one at a time). When werestrict the analysis to the northern region of India (Punjab, Haryana, Himachal Pradesh, Uttar Pradesh
12Perhaps due to the One Child Policy, birth order is not available in the Chinese data and most mothers in the sample haveone or no children. Instead, we include pregnancy number as a control variable.

SEX-SELECTIVE PRENATAL CARE 11
and Rajasthan), we see a much larger magnitude of discrimination for certain types of prenatal caretreatments; this difference between the northern sample and full sample is significant for prenatal care,the number of prenatal visits, the days iron supplements are taken and the place of delivery (results notshown but are available upon request). This is consistent with other studies that find more skewed sexratios in these regions (Jha et al. 2006), suggesting higher levels of son preference as well as greateravailability of ultrasound technology (as noted earlier, Punjab was one of the first states to receive thistechnology). Mothers attend prenatal checks up more frequently (9%) and take more tetanus shots(4%) when pregnant with a boy. Moreover, mothers are nearly 3 percentage points more likely toinvest in prenatal care when pregnant with a boy. We see slightly larger magnitudes (compared to thefull sample) for samples where the previous children of the women are majority female (the childrenprior to the latest birth), although the differences in magnitudes in this sample relative to those in thefull sample are not significant (results not shown; available upon request). If son preference is present,we should find that samples where women previously have had female children should be even morelikely to differentially invest if their most recent pregnancy is a boy. For this sample of majority femalein the past children of the mother, we find the magnitudes to be quite large - males are 1.7 percentagepoints more likely to receive tetanus shots than females, and nearly 1.5 percentage points more likelyto receive some sort of prenatal care. Hence, for India, we find strong, consistent evidence that womenutilize more prenatal care options when pregnant with a boy than when they are pregnant with a girl.
As mentioned earlier, we have ultrasound receipt information for a subset of the Indian sam-ple. While the 2005-6 round asks about ultrasound usage during each pregnancy in the past 5 years,the 1998-99 round only asks about ultrasound usage among the sample of women who had at least oneprenatal check up. Having ultrasound receipt information is critical to our work as ultrasounds are alikely necessity to know the sex of the child. In order to make the samples comparable, we first poolthe surveys and restrict the sample to those women who had at least 1 prenatal check up. Within thissample, we examine whether mothers pregnant with males and receiving an ultrasound visit prenatalclinics multiple times. Because this sample of women are those who have already attended a prenatalcheckup, they are the most likely to pursue additional prenatal care. Accordingly, the high samplemeans of these outcomes (often as high as 95-98%) lead us to believe that an extreme value distributionis more appropriate and thus we employ logit specifications when using this sample. Table 2 Panel Afinds that males are more likely to make multiple prenatal visits when an ultrasound is received. Theyare also more likely to receive a tetanus shot when they report having had an ultrasound, although thisis statistically significant only for the northern region and for the sample whose previous children aremainly female. These results stand in contrast to those for women who do not receive ultrasounds andare therefore unlikely to know the sex of their unborn child. With the exception of tetanus shots in thefull sample, women who do not report receiving ultrasounds do not systematically discriminate in favorof male fetuses. The differences in coefficients on the male dummy variable in the two samples (thosewith and without ultrasounds) are statistically significant across all specifications, with the exceptionof tetanus in the full sample and antenatal visits in the majority female sample.
Panel B examines all births in the 2005-6 survey (since ultrasound information was askedof everyone, not just mothers who had a prenatal check up). We use similar outcome measures as

12 BHARADWAJ & NELSON
Panel A to keep matters consistent, but also because a very large fraction of those who report havinghad an ultrasound also report having attended prenatal care at least once (98.75%). Panel B is alsoconsistent with our results so far, showing that women who receive ultrasounds take differentially bettercare of their male fetuses (although the results for the sample with majority female is not statisticallysignificant). In the samples of women who did not receive an ultrasound during their pregnancies, wefind no evidence of gender discrimination in prenatal care, although the difference in coefficients acrossthe ultrasound and non-ultrasound samples is statistically significant only for antenatal checkups in thefull and northern samples.
However, there are several important caveats involved with using the ultrasound data. First,the ultrasound variable is likely be measured with noise. Given the illegality of sex determination,many women may be reluctant to admit that they have received an ultrasound during their pregnancy.Moreover, as discussed in an earlier section, ultrasound technology has become available even throughunofficial channels. Women who determine the sex of their baby without having to engage in formalprenatal care may be less likely to recall or report that they have received an ultrasound. For bothof these reasons, we might expect the proportion of our sample who actually received ultrasoundsto be much higher than the 14% and 27% reported in the 1998-9 and 2005-6 rounds of the NFHS,respectively.
4.1. Robustness Checks
As mentioned earlier, four main identification issues arise when examining sex-selectiveprenatal care - selective recall, male fetus-specific pregnancy complications, endogeneity due to sonpreference-based fertility stopping rules and bias due to sex-selective abortions. The results in Tables5-10 show that our findings are robust to these concerns.
First, we estimate the relationship in equation 1 for births prior to widespread availability ofultrasound or sex determination technology. In Table 3, we do not find any evidence towards prenataldiscrimination among births that occurred in the late 1980s in India. As mentioned earlier, ultrasoundtechnology appears to have become widespread in the 1990s. Under selective recall, we should findmothers reporting greater prenatal care for male babies even in the absence of ultrasound receipt. An-other way to rule out the possibility of selective recall is to examine prenatal care outcomes that occurbefore fetal gender is detectable. In Table 4 we exploit the timing of the first prenatal checkup andshow that there is no gender gap in prenatal care that occurs within the first four months of pregnancy,when the sex of the fetus is unknown. In contrast, there is a large and significant gap in care that takesplace in the final five months of pregnancy. Thus we believe that the existence of selective recall cannotexplain this pattern of discrimination in our results, even within the same pregnancy. 13
Second, we estimate whether being pregnant with a boy leads to more complications duringthe pregnancy. If carrying a male were more physically taxing than carrying a girl, then we might findthat women pregnant with boys are more likely to seek prenatal care for reasons other than gender
13While we lack data on the timing of prenatal visits after the first, the outcome for column 2 of Table 4 is constructed usinginformation on the timing of the first visit and the total number of prenatal visits. See the notes to the table for a detaileddescription of how this variable is constructed.

SEX-SELECTIVE PRENATAL CARE 13
discrimination. Table 5 estimates whether being pregnant with a boy is significantly related to com-plications during pregnancy in India. Except for the category of "night blindness" we do not find anyevidence to support the idea that male fetuses medically require greater prenatal care through increasedcomplications. Moreover, the size of the coefficient on night blindness is extremely small compared tothe average level of night blindness experienced by mothers in the sample. 14
Third, following Barcellos, Carvalho, and Lleras-Muney (2010) we restrict the sample tofamilies where the youngest child is less than 2 years old to minimize the bias due to families adjustingtheir fertility after realizing the sex of the child. The first three columns of Table 6 display the resultsusing this sample. For outcomes such as prenatal care, tetanus shots and delivery in a non-home facility,our original results hold and the magnitudes of the gender gap are slightly larger. One drawback of thismethod is that it relies on the assumption of no sex-selective abortions. As we indicated earlier, thepresence of selective abortions can bring about two important sources of bias: sample selection andreverse causation. While the bias due to sample selection likely works in the opposite direction of ourresult, reverse causation could potentially bias our estimates upwards. To account for this possibility,we further restrict the sample to those who have made at least one prenatal visit and focus on whetherthese women seek higher levels of additional prenatal care when carrying boys than when carryinggirls (columns 3 - 6 of Table 6). Again, we find that even in this restricted sample, male fetuses receivesignificantly more care than female fetuses and the magnitude of the gender gap remains substantial.Thus we find no evidence that any bias due to gender-based stopping rules is driving our results.15
Our final concern has to do with reverse causality due to sex selective abortions. If motherslearn the sex of their child during a prenatal visit and choose to abort if female fetuses, then we wouldfind a mechanical correlation between prenatal care visits and sex of the child due to sex selectiveabortions, rather than sex selective prenatal care. As we proposed in an earlier section, one approachthat minimizes the potential for reverse causality is to restrict the sample to those who have madeat least one prenatal visit and examine the gender gap in subsequent prenatal care. The first threecolumns of Table 7 display the results for this approach. We find that even in this sample (in whichreverse causation is highly unlikely) there remains a sizeable gender gap in prenatal care undertakenafter the first visit. Moreover, when we take an even more conservative approach by restricting thesample to women who make their first prenatal visit in the final five months of pregnancy (for whomthe assumption of discovering the sex of the child during the first visit is most credible), we find thatthere remains a high degree of gender discrimination in prenatal care. Although the gender gap is not
14A concern might be that if women carrying male fetuses do need greater prenatal care, then perhaps Table 5 does not reflectdifferential complications by male because mothers take greater prenatal care while pregnant with a male. We rule out thispossibility by showing that for the sample that does not receive any prenatal care, we find that carrying a male child does notlead to more complications (table not shown, available upon request). The other category that shows up significant in thisregression is anemia. However, the sign on this is negative, suggesting that mothers when carrying a male do more thingsto avoid becoming anemic - a common way to do this is to take iron pills. This is consistent with the finding that motherspractice greater prenatal care when pregnant with a male.15Table 8 (mother fixed effects) is another way to account for the endogeneity problem if preferences over gender compositionare time invariant. When we restrict the Barcellos et al (2010) sample even further to those children under the age of 1 at thetime of the survey, the dummy on male is no longer significant across many specifications (results not shown). However, themagnitude of the coefficients are similar to those in Table 1, suggesting that our original estimates do not suffer heavily frombias arising from son preference-based stopping rules.

14 BHARADWAJ & NELSON
significant for tetanus shots and non-home delivery, we believe this is largely due to the considerabledrop in sample size and more importantly, the magnitude of the of the gender gap is consistent with ourmain results, indicating that reverse causality is not likely to be sole explanation for our results.
Lastly, Table 8 estimates the fixed effects specification in equation 2 for India where we havedata on the previous two births of the mothers. We find similarly consistent results for a wide range ofprenatal investments. Even within families, mothers appear to make more investments when pregnantwith a boy as opposed to a girl. Compared with the estimates of Table 1, the fixed effects estimates areslightly larger in magnitude, although the samples are not the same (the mother fixed effects samplecontains mothers who gave birth twice in the five years prior to the survey in 1998). Mothers are 4.3%more likely to consume iron pills and visit prenatal clinics nearly 4% more frequently when pregnantwith a boy.
4.2. Results from other countries
Since the DHS collects extensive prenatal care data, we can extend our analysis to othercountries in South and Southeast Asia.16 We estimate equation 1 for China, Bangladesh, and Pakistan -countries where son preference and gender discrimination has been well established in previous studies(Das Gupta et al. 2003) - and find that the gender bias in prenatal care is not limited to India but is ratherpervasive in Southeast Asian countries with a history of son preference. As part of a larger robustnesscheck, we estimate equation 1 for Sri Lanka and Thailand where son preference is weak (Arnold,Kishor, and Roy 2002, Hua 2001, Prachuabmoh, Knodel, and Alers 1974). As a final robustness check,we investigate whether sex-selective prenatal care is practiced in Ghana, a country with no known sonpreference (Garg and Morduch 1998).
The first four rows of Appendix Table 4 display the results of estimating 1 for countriesthat are known to have son preference: China, Bangladesh, and Pakistan (both the full sample andthe region of Punjab).17 Overall, the results from these samples exhibit patterns consistent with sex-selective discrimination in prenatal care. In China, women are 5% more likely to get some prenatalcare when pregnant with a boy, and visit antenatal clinics nearly 10% more frequently. In Bangladesh,women are 2.8 percentage points more likely to get a tetanus shot when pregnant with a boy. We donot find significant estimates in the decision to seek prenatal care, although we do find that womenvisit prenatal clinics 7% more frequently when pregnant with a boy. In Pakistan, we find that womenvisit prenatal clinics more often and are 6% more likely to consume iron pills when pregnant witha boy. In Paskistani Punjab, a region with a large number of missing women (Gechter 2010), themagnitude of discrimination is even larger for some prenatal outcomes; for example, mothers are 13%more likely to take iron pills. Taken all together, the evidence in Appendix Table 4 implies that thepractice of sex-selective prenatal investments extends beyond India and is widespread across areaswith well documented son preference.
16In principle, all DHS countries can be used in this analysis. Based on our reading of the literature on son preference andgender discrimination, we believe we have focussed on a part of the world where this is most relevant.17Note that not all outcomes are available for China.

SEX-SELECTIVE PRENATAL CARE 15
Finally, we estimate equation 1 for countries with no (or at least lesser) established son pref-erence. The last three rows of Appendix Table 4 displays the estimates for Sri Lanka, Ghana andThailand. While almost all specifications are statistically insignificant, what is relevant for us is thatthe magnitudes are quite small. At a minimum, these coefficients are smaller than what we found forcountries with known son preference. The estimates in Sri Lanka and Thailand are consistent withlower levels of son preference and none are statistically significant. These results also help rule outthe possibility of factors confounding son preference in prenatal investments; there is no evidence ofselective recall or biological factors which indicate that boys are more likely to receive prenatal carefor reasons other than son preference.
4.3. Impact on excess female neonatal mortality
A question of interest in this context is, "How many more girls would there be under equaltreatment of prenatal care"? In this paper, we attempt to answer this question by examining the genderdifferential in maternal tetanus vaccinations rather than general prenatal care. This is mainly becauseprenatal care is multidimensional in nature and can vary from facility to facility; this makes it difficult toassess the causal role that prenatal care plays in determining infant or child mortality. However, tetanusis a rather specific infection to which neonates are particularly susceptible. Moreover, as mentionedearlier, tetanus shots have a large impact on reducing neonatal deaths due to tetanus. Hence, in thissection, we calculate (with some assumptions) the number of girls that would have been saved in theneonatal stage had there been no gender bias in the receipt of tetanus immunizations.
While neonatal deaths occur more frequently among males, this does not mean that thereare no "excess" female deaths in the neonatal stage. In our sample for India, the observed neonataldeath rate is 2.24% for girls. Female neonatal mortality rate in Ghana and Italy is around 1.93%.Using the sex ratio in neonatal mortality from these countries (since they are presumed to be free of sonpreference), we impute a neonatal mortality rate for women in India to be around 1.94%.18 Thus excessfemale neonatal mortality - the amount that the rate exceeds what we expect under equal treatment - is0.31 percentage points in India.19
Our estimates from Table 1 suggest that males are 1.6% more likely to receive tetanus shotsthan females (this is our smallest effect across all specifications for India). This implies that for every100 boys, only 98.4 girls receive tetanus shots. If we take estimates from Rahman et al. (1982), wewould believe that babies face a mortality rate that is 3.03 times higher in the neonatal stage if themother did not receive a tetanus shot. Since 80.3% of all mothers pregnant with girls receive tetanusshots, the implied neonatal mortality rate for those whose mothers were received the shots is 1.6% and4.85% for those whose mothers did not.
18Ulizzi and Zonta (2002) find that the sex ratio in neonatal deaths is 0.59. Given that we observe a 958 neonatal deathsamong boys in our sample, the natural rate for girls would be 1.94% in order to maintain the proper sex ratio. That is, thenumber of neonatal deaths among girls that we expect in order to yield the sex ratio of 0.59 is given by 958/(958+x)=0.590,i.e. 665.7 deaths. Since we have 34,239 female births in our sample, this implies a natural or equal treatment neonatalmortality rate of 665.7/34,239=1.94% for girls.19Please see the appendix for details on all calculations in this section.

16 BHARADWAJ & NELSON
This means that had the 1.6 girls that did not receive tetanus shots actually received one, 0.012more girls would have survived than in the case of differential treatment. Hence, unequal allocationof tetanus shots can explain around 3.9-4.0% of the "excess" female mortality in the neonatal stage(depending on whether we use the benchmark estimate from Italy or Ghana). If instead we use ourlargest estimates that males are 4.34% more likely to receive tetanus shots (from Table 8, the motherfixed effects table), we conclude that unequal allocation of tetanus immunizations can explain around10.1%-10.5% of the excess female neonatal mortality (again, depending on which estimate for equaltreatment we use). Therefore, we believe that discriminatory practices with regards to tetanus vacci-nations during the prenatal period can explain between 4-10.5% of the excess female mortality in theneonatal period.20
5. CONCLUSION
This paper examines whether preference for sons in certain countries in South and SoutheastAsia leads parents to differentially invest in their unborn children. We find evidence that in countriesknown to have son preference - namely India, China, Bangladesh and Pakistan - parents invest in greaterprenatal care when pregnant with a boy. We successively rule out confounding factors such as biologicalbiases, the presence of sex-selective abortion, son preference-based fertility rules and selective recall ofprenatal care. Moreover, we find no evidence of sex-selective prenatal care in countries with weak orno son preference nor do we see gender biased investments in years before widespread availability ofsex determination. Hence, the weight of the evidence points towards gender discrimination in prenatalinvestments. Specifically in India, we find sex-selective prenatal care in tetanus to have importantconsequences in relation to female neonatal mortality rates. Female neonatal mortality is higher thanwhat it should be under equal treatment in India; we estimate that equal treatment of tetanus shotsshould decrease this gap by 4-10.5%.
We believe our results contribute to the literature in three ways. First, our paper adds tothe growing body of work examining consequences of son preference in South and Southeast Asia.We believe we are the first to give empirical evidence that such son preference leads to sex-selectiveprenatal investments in these regions. These sizeable gender differentials in prenatal investments arelikely to be the cause of the large observed disparity in short-term health outcomes between girls andboys. In our Indian sample, boys are born with greater birth weight and have a lower probability ofbeing low birth weight.21 While this is not causal, it is consistent with boys receiving greater prenatalcare. Correlations between various dimensions of prenatal care (such as tetanus shot receipt and ironpill supplements) and outcomes such as neonatal deaths and birth weight show that babies that receivesome prenatal care are better off. Hence, sex-selective prenatal care can be associated with differentialbirth weight and neonatal death rates among boys and girls.
Second, policy in countries like India is focused on a natural and important outcome of sex-based discrimination - survival rates of females measured via sex ratios at different ages. Given the
20If we instead use our estimates from the ultrasound sample, we find a lower bound estimate that discrimination in tetanusshot receipt explains 0.6% of excess female neonatal mortality.21The correlations discussed in this section are not shown but are available upon request.

SEX-SELECTIVE PRENATAL CARE 17
findings from the vast literature linking early childhood health (such as birth weight) and later lifeoutcomes, our results imply that effect of gender discrimination in prenatal care might also be seen inthe long run via decreased labor market opportunities or decreased educational attainment for women.Hence, even if the imbalance of sex ratios improves over time, we should worry about the possibilityof sex-selective prenatal care.
Third, we provide a unique perspective on the literature concerned with parental investmentsbased on child endowments. Our study brings into question the very process of the endowment for-mation - child endowments, often measured as birth weight are themselves the result of parental pref-erences over gender. Hence, studies investigating such relationships in developing countries with sonpreference must seriously consider the possibility that parents differentially invest based on the sex oftheir unborn child.

18 BHARADWAJ & NELSON
REFERENCES
AIZER, A., AND F. CUNHA (2010): “Child Endowments, Parental Investments and the Development of Human Capital,”Brown University Working Paper.
ALMOND, D., K. CHAY, AND D. LEE (2002): “Does low birth weight matter? Evidence from the US population of twinbirths,” University of California, Berkeley, Center for Labor Economics Working Paper, 53.
ALMOND, D., AND B. MAZUMDER (2005): “The 1918 influenza pandemic and subsequent health outcomes: an analysis ofSIPP data,” American Economic Review, 95(2), 258–262.
ARNOLD, F., S. KISHOR, AND T. ROY (2002): “Sex-selective abortions in India,” Population and Development Review,28(4), 759–785.
ASHENFELTER, O., AND C. ROUSE (1998): “Income, Schooling, and Ability: Evidence from A New Sample of IdenticalTwins,” Quarterly Journal of Economics, 113(1), 253–284.
BARCELLOS, S., L. CARVALHO, AND A. LLERAS-MUNEY (2010): “Child Gender and Parental Investments in India: AreBoys and Girls Treated Differently?,” Mimeo, UCLA.
BEHRMAN, J., AND M. ROSENZWEIG (2004): “Returns to birthweight,” Review of Economics and Statistics, 86(2), 586–601.
BEHRMAN, J., M. ROSENZWEIG, AND P. TAUBMAN (1994): “Endowments and the allocation of schooling in the familyand in the marriage market: The twins experiment,” Journal of Political Economy, 102(6), 1131–1174.
BHALOTRA, S., AND T. COCHRANE (2010): “Where have all the young girls gone? On the rising trend in sex selection inIndia,” University of Bristol Working Paper.
BHARADWAJ, P., AND J. EBERHARD (2010): “Atmospheric Air Pollution and Birth Weight,” Working Paper.BLACK, S., P. DEVEREUX, AND K. SALVANES (2007): “From the Cradle to the Labor Market? The Effect of Birth Weighton Adult Outcomes*,” The Quarterly Journal of Economics, 122(1), 409–439.
DAHL, G., AND E. MORETTI (2004): “The demand for sons: Evidence from divorce, fertility, and shotgun marriage,” NBERWORKING PAPER SERIES.
DREZE, J., AND A. SEN (1989): Hunger and public action. Oxford University Press, USA.GARG, A., AND J. MORDUCH (1998): “Sibling rivalry and the gender gap: Evidence from child health outcomes in Ghana,”Journal of Population Economics, 11(4), 471–493.
GECHTER, M. (2010): “Examining the Sex Ratio in Pakistan,” Working Paper, Pomona College.GORTMAKER, S. (1979): “The effects of prenatal care upon the health of the newborn.,” American Journal of Public Health,69(7), 653.
GUPTA, M. (1987): “Selective discrimination against female children in rural Punjab, India,” Population and developmentreview, 13(1), 77–100.
GUPTA, S., AND P. KEYL (1998): “Effectiveness of prenatal tetanus toxoid immunization against neonatal tetanus in a ruralarea in India,” The Pediatric infectious disease journal, 17(4), 316.
HUA, C. (2001): A society without fathers or husbands: the Na of China. MIT Press, Cambridge.JAYACHANDRAN, S., AND I. KUZIEMKO (2009): “Why do mothers breastfeed girls less than boys? Evidence and implica-tions for child health in India,” NBER Working paper.
JHA, P., R. KUMAR, P. VASA, N. DHINGRA, D. THIRUCHELVAM, AND R. MOINEDDIN (2006): “Low male-to-female sexratio of children born in India: national survey of 1.1 million households,” The Lancet, 367(9506), 211–218.
LHILA, A., AND K. SIMON (2008): “Prenatal Health Investment Decisions: Does the Child’s Sex Matter?,” Demography.LOUGHRAN, D., A. DATAR, AND M. KILBURN (2004): “The Interactive Effect of Birth Weight and Parental Investment onChild Test Scores,” RAND Labor and Population Working Paper WR-168.
MENG, L. (2010): “Prenatal Sex Selection and Missing Girls in China: Evidence from the Diffusion of Diagnostic Ultra-sound,” Working Paper.
MILLER, B. (2001): “Female-selective abortion in Asia: Patterns, policies, and debates,” American anthropologist, pp.1083–1095.

SEX-SELECTIVE PRENATAL CARE 19
OSMANI, S., AND A. SEN (2003): “The hidden penalties of gender inequality: fetal origins of ill-health,” Economics &Human Biology, 1(1), 105–121.
OSTER, E. (2009): “Proximate Causes of Population Gender Imbalance in India,” Demography.PITT, M., AND M. ROSENZWEIG (1990): “Estimating the intrahousehold incidence of illness: Child health and gender-inequality in the allocation of time,” International Economic Review, 31(4), 969–989.
PORTNER, C. (2009): “The Determinants of Sex Selective Abortions,” Mimeo, University of Washington.PRACHUABMOH, V., J. KNODEL, AND J. ALERS (1974): “Preference for sons, desire for additional children, and familyplanning in Thailand,” Journal of Marriage and the Family, 36(3), 601–614.
QIAN, N. (2008): “Missing Women and the Price of Tea in China: The Effect of Sex-Specific Earnings on Sex Imbalance*,”Quarterly Journal of Economics, 123(3), 1251–1285.
RAHMAN, M., L. CHEN, J. CHAKRABORTY, M. YUNUS, A. CHOWDHURY, A. SARDER, S. BHATIA, AND G. CURLIN
(1982): “Use of tetanus toxoid for the prevention of neonatal tetanus. 1. Reduction of neonatal mortality by immunizationof non-pregnant and pregnant women in rural Bangladesh.,” Bulletin of the World Health Organization, 60(2), 261.
ROSENZWEIG, M., AND J. ZHANG (2009): “Do Population Control Policies Induce More Human Capital Investment?Twins, Birth Weight and China’s One-Child Policy,” Review of Economic Studies, 76(3), 1149–1174.
ZUPAN, J., AND E. AAHMAN (2005): “Perinatal mortality for the year 2000: estimates developed by WHO,” Geneva: WorldHealth Organization.

20 BHARADWAJ & NELSON
APPENDIX A. CALCULATING THE CONTRIBUTION OF DIFFERENTIAL TETANUS IMMUNIZATIONS
TO EXCESS FEMALE MORTALITY
Girls are more likely to survive than boys in the neonatal period for genetic and biologicalreasons. We use female neonatal mortality rate in the Ghanian DHS data as a measure of the "natural"neonatal mortality rate for girls. Restricting the sample to the 1998, 2003 and 2008 rounds (in order tobe comparable to the NFHS time frame used in our regressions), the female neonatal mortality rate is1.93%. When we use the results of a study in Italy (Ulizzi and Zonta 2002) we impute a natural rate of1.94%; thus we are confident that this represents an accurate measure of neonatal mortality among girlsin the absence of differential treatment and use it in all calculations below.22 The neonatal mortality rateis 2.24% among girls in our sample from India. This implies that the excess female neonatal mortalityis 2.24-1.93=0.31 percentage points.
According to Rahman et al. (1982), babies are 67% less likely to die in the neonatal periodif their mothers received tetanus shots during pregnancy; this implies that babies whose mothers didnot receive tetanus shots are 3.03 times as likely to die.23 As mentioned before, the neonatal mortalityrate is 2.24% among girls in the Indian sample. Since 80.3% of all mothers pregnant with girls receivetetanus shots, the implied neonatal mortality rate for those whose mothers were received the shotssolves 0.803x + 3.03(1-0.803)x=2.24. This yields a mortality rate of 1.6% for female children born towomen who received tetanus shots and 4.85% for those whose mothers did not.
Our estimates in Table 1 show that women are 1.6% less likely to receive tetanus shotswhen pregnant with girls than when pregnant with boys. This means that for every 100 boys whoreceive tetanus immunization through their mothers, only 98.4 girls do. If mothers were equallylikely to receive tetanus shots (regardless of fetal gender) then the remaining 1.6 girls out of 100would have tetanus immunity. Under equal treatment the number of girls who die from tetanus is0.23(0.016)100=0.368 per 100, where 23% of neonatal deaths are due to tetanus in India (UNICEF2000) and the neonatal mortality rate is 1.6% (calculated above).24 Under differential treatment, where1.6 girls are born to mothers who have not had tetanus shots, 0.23((1.6)0.0485+(100-1.6)0.016)=0.380girls die per 100 because the 1.6 girls without tetanus immunity face a higher mortality rate of 4.85%(calculated above). Thus, the difference in tetanus shots leads to a difference in observed neonatalmortality of 0.380-0.368=0.012 deaths per 100 girls.
Therefore, the gender gap in tetanus shots can explain 0.012/0.31=3.86% of excess femaleneonatal deaths in India (or 3.98% if we use the Italian benchmark). If we repeat all of the calculationsusing the upper bound of our estimates for India (the mother fixed effect specification, results in Table
22Ulizzi and Zonta (2002) find that the sex ratio in neonatal deaths is 0.59. Given that we observe a 958 neonatal deathsamong boys in our sample, the natural rate for girls would be 1.94% in order to maintain the proper sex ratio. That is, thenumber of neonatal deaths among girls that we expect in order to yield the sex ratio of 0.59 is given by 958/(958+x)=0.590,i.e. 665.7 deaths. Since we have 34,239 female births in our sample, this implies a natural neonatal mortality rate of665.7/34,239=1.94% for girls.23We consider this to be a conservative measure, as Blencowe et al (2010) find an 94% reduction in neonatal tetanus whenmothers are immunized.24Again, this is likely to be a conservative estimate; Gupta and Keyl (1998) find that tetanus accounts for 23-73% of allneonatal deaths.

SEX-SELECTIVE PRENATAL CARE 21
4) we find that differential tetanus treatment accounts for 10.1% of the gap between the natural andobserved rates of neonatal mortality (10.5% using the imputed rate from Italy). Hence we believe thatthe gender bias in prenatal tetanus immunizations can explain 4%-10.5% of excess female neonatalmortality.

0.02
0.03
0.04
0.05
0.06
0.07
Ge
nd
er D
iffe
re
nti
al
FIGURE 1. Gender Differentials in Prenatal Care, by birth order and
sex composition of previous children
BB
GG
GGG
-0.01
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
Second Born Third Born Fourth Born
Ge
nd
er D
iffe
re
nti
al
FIGURE 1. Gender Differentials in Prenatal Care, by birth order and
sex composition of previous children
B
GBB
GG
BBB
GGG

Prenatal Care
(1=Yes,
0=No)
Number of
Prenatal visits
Tetanus Shot
(1=Yes,
0=No)
Number of
Tetanus Shots
Iron Pills
(1=Yes,
0=No)
Days Took
Iron
Supplement
Non-Home
Delivery
(1=Yes,
0=No)
(1) (2) (3) (4) (5) (6) (7)
Full Sample 0.011** 0.058* 0.011** 0.039*** 0.000 0.349 0.017***
(0.006) (0.030) (0.005) (0.014) (0.006) (0.938) (0.005)
Mean of Dependent Variable 0.688 2.780 0.777 1.680 0.590 39.7 0.312
Observations 32233 32012 32017 32017 32166 17698 31073
R-squared 0.311 0.477 0.191 0.176 0.242 0.296 0.374
Northern Region 0.028** 0.189*** 0.022* 0.056** 0.004 2.603* 0.038***
(0.011) (0.048) (0.011) (0.027) (0.012) (1.452) (0.009)
Mean of Dependent Variable 0.601 2.122 0.685 1.435 0.488 29.0 0.236
Observations 8369 8304 8324 8324 8349 4161 8106
R-squared 0.274 0.466 0.182 0.175 0.228 0.291 0.413
Majority Female Sample 0.015* 0.073* 0.017** 0.051** -0.001 -0.169 0.007
(0.008) (0.044) (0.008) (0.021) (0.009) (1.439) (0.008)
Mean of Dependent Variable 0.704 2.864 0.793 1.714 0.603 41.7 0.324
Observations 14413 14302 14321 14321 14387 7904 13941
R-squared 0.317 0.482 0.186 0.172 0.240 0.301 0.371
TABLE 1. Sex-Selective Prenatal Investments in India
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to most recent birth of ever married women (ages 15-49) within 5 years previous to survey. NFHS surveys from
1998 and 2004 used. Days took iron supplements is available only for the 2004 survey. National sample weights are used in all regressions.
Controls include: state fixed effects, birth year fixed effects, survey year fixed effects, household wealth quintile fixed effects, mother's age,
mother's education, dummy for urban, birth order, and existing sex ratio of children (defined as the ratio of boys to the total number of births
prior to the most recent one). Northern region is defined as the following states: Haryana, Himachal Pradesh, Punjab, Rajasthan, Uttar Pradesh,
and New Dehli.
Coefficient on Male in various
samples
Outcomes

PA�EL A - 1998 & 2005 Survey data,
restricted to women who had atleast 1
prenatal check up With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
Male 0.530** 0.117* 0.170 0.041 0.692** 0.080 0.938** 0.110 0.589* 0.085 0.673** 0.106
(0.223) (0.061) (0.233) (0.080) (0.299) (0.118) (0.396) (0.153) (0.314) (0.094) (0.314) (0.123)
Constant 3.184*** 2.388*** 5.517*** 2.292*** 2.226 0.362 5.690*** 1.809** 6.865*** 2.161*** 3.548*** 1.302**
(1.086) (0.300) (1.137) (0.307) (1.441) (0.575) (1.852) (0.822) (1.574) (0.404) (1.364) (0.526)
P-value of the test that the coefficient on
Male is the same in the with and without
ultrasound samples
Mean of Dependent Variable 0.963 0.868 0.974 0.938 0.950 0.844 0.971 0.923 0.964 0.872 0.975 0.941
State Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Year Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Birth Year Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Observations 5171 16870 5970 16891 1605 3772 1542 3785 2226 7522 2541 7542
PA�EL B - 2005 Data, all womenWith
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
With
Ultrasound
Without
Ultrasound
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
Male 0.479** 0.036 0.075 0.058 0.675** 0.064 0.729* 0.125 0.351 -0.015 0.376 0.047
(0.213) (0.053) (0.245) (0.058) (0.318) (0.093) (0.401) (0.099) (0.289) (0.082) (0.334) (0.090)
Constant 4.500*** 1.292*** 3.055*** 1.887*** 0.937 -1.399*** 3.841** 0.500 4.635*** 0.929** 2.310 1.377**
(1.029) (0.266) (0.996) (0.309) (1.344) (0.411) (1.699) (0.457) (1.129) (0.431) (1.597) (0.554)
P-value of the test that the coefficient on
Male is the same in the with and without
ultrasound samples
Mean of Dependent Variable 0.947 0.555 0.971 0.761 0.944 0.574 0.971 0.685 0.948 0.567 0.970 0.776
State Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Year Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Birth Year Fixed Effects Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Observations 4557 13138 4759 13164 1240 3035 1249 3044 2074 5701 2083 5716
Notes: Coefficients (not marginal effects) reported. Sample is restricted to most recent birth (within 5 years previous to the 2005-6 survey only) of ever married women. Other controls included are mother's age and education, birth order of most
recent birth, dummies for each household wealth quintile, an urban area dummy and existing sex ratio of children (defined as the ratio of boys to the total number of births prior to the most recent one).
At least 2 Antenatal Visits Tetanus Shot (1=Yes,0=No) At least 2 Antenatal Visits Tetanus Shot (1=Yes,0=No) At least 2 Antenatal Visits Tetanus Shot (1=Yes,0=No)
0.043 0.946
Robust standard errors in parentheses
0.065 0.143 0.224 0.093
*** p<0.01, ** p<0.05, * p<0.1
0.057 0.051 0.152 0.093
Full Sample Northern Region Majority Female
0.074 0.600
TABLE 2. Sex-Selective Prenatal Investments in India: Births to Women with and without Ultrasounds (Logit specification)
Majority Female
At least 2 Antenatal Visits Tetanus Shot (1=Yes,0=No) At least 2 Antenatal Visits
Full Sample Northern Region
Tetanus Shot (1=Yes,0=No) At least 2 Antenatal Visits Tetanus Shot (1=Yes,0=No)

Prenatal Care
(1=Yes, 0=No)
Number of
Prenatal visits
Tetanus Shot
(1=Yes, 0=No)
Number of
Tetanus Shots
Iron Pills (1=Yes,
0=No)
Non-Home
Delivery (1=Yes,
0=No)
(1) (2) (3) (4) (5) (6)
Male -0.001 0.072 -0.011 0.023 -0.001 -0.001
(0.012) (0.066) (0.012) (0.023) (0.013) (0.011)
Mean of Dependent Variable 0.632 2.530 0.725 2.114 0.624 0.309
Observations 4218 4216 4211 3049 4218 4217
R-squared 0.328 0.441 0.240 0.119 0.239 0.384
Male
Mean of Dependent Variable
Observations
R-squared 0.321
TABLE 4. Sex-Selective Prenatal Investments in India: Timing of Prenatal Care
Notes: Sample is restricted to most recent birth of ever married women (ages 15-49) within 5 years previous to
survey. Receiving prenatal care after four months of pregnancy is defined as 1 if women make their first
prenatal visit after four months of pregnancy or if they make their first prenatal visit during the first four months
of pregnancy but make multiple visits over the course of the pregnancy and as 0 otherwise. Controls include:
state fixed effects, birth year fixed effects, survey year fixed effects, mother's age, mother's education, dummy
for urban, birth order, and existing sex ratio of children (defined as the ratio of boys to the total number of births
prior to the most recent one). National sample weights are used in all regressions.
(2)
0.013**
(0.006)
0.435
32233
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to most recent birth occuring in 1992 or earlier by ever married women (ages 15-49). Wealth index is not available for over
90% of the sample so it is not included. Controls include: state fixed effects, birth year fixed effects, survey year fixed effects, mother's age, mother's
education, dummy for urban, birth order, and existing sex ratio of children (defined as the ratio of boys to the total number of births prior to the most
recent one).
TABLE 3. Sex-Selective Prenatal Investments in India: Pre-Ultrasound Period (births in 1992 and earlier)
Robust standard errors in parentheses
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Prenatal Care Received WITHIN
First Four Months of Pregnancy
(1=Yes, 0=No)
(1)
0.007
(0.006)
0.659
32233
0.244
Prenatal Care Received AFTER First
Four Months of Pregnancy (1=Yes,
0=No)

Night
Blindness
(1=Yes,
0=No)
Blurred Vision
(1=Yes,
0=No)
Convulsions
(1=Yes,
0=No)
Swelling
(1=Yes,
0=No)
Fatigue
(1=Yes,
0=No)
Anemia
(1=Yes,
0=No)
Excessive
Bleeding
(1=Yes,
0=No)
Any
Complication
(1=Yes,
0=No)
(1) (2) (3) (4) (5) (6) (7) (8)
Male 0.009** 0.003 0.002 -0.006 0.006 -0.015** 0.000 0.001
(0.003) (0.004) (0.004) (0.005) (0.005) (0.007) (0.002) (0.005)
Mean of Dependent Variable 0.117 0.133 0.125 0.250 0.482 0.256 0.039 0.596
Observations 32225 32236 32225 32237 32236 13911 32217 32252
R-squared 0.059 0.087 0.058 0.025 0.054 0.059 0.008 0.052
Prenatal Care
(1=Yes,
0=No)
Tetanus Shot
(1=Yes,
0=No)
Non-Home
Delivery
(1=Yes,
0=No)
At least 2
Prenatal Visits
At least 2
Tetanus Shots
(1=Yes,0=No)
Non-hone
Delivery
(1=Yes,
0=No)
(1) (2) (3) (4) (5) (6)
Male 0.014* 0.013* 0.020*** 0.016** 0.017** 0.022**
(0.007) (0.007) (0.007) (0.007) (0.008) (0.009)
Mean of Dependent Variable 0.685 0.776 0.297 0,880 0.831 0.399
Observations 18149 18061 17581 12897 12914 12583
R-squared 0.313 0.186 0.360 0.097 0.070 0.331
*** p<0.01, ** p<0.05, * p<0.1
TABLE 5. Gender and Pregnancy Complications in India
Robust standard errors in parentheses
Notes: Sample is restricted to most recent birth of ever married women (ages 15-49) within 5 years previous to the survey. Controls include: state fixed effects, birth
year fixed effects, survey year fixed effects, mother's age, mother's education, dummy for urban, birth order, and existing sex ratio of children (defined as the ratio of
boys to the total number of births prior to the most recent one). National sample weights are used in all regressions .
TABLE 6. Sex-Selective Prenatal Investments in India: Children Aged 0-23 months at Time of Survey
Full SampleMothers Who Receive At Least 1 Prenatal
Checkup
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to most recent birth of ever married women (ages 15-49) within 1 year previous to the survey. Sample is
further restricted to births of children aged 0-23 months at the time of the survey. Days took iron supplements is available only for
the 2004 survey. Controls include: state fixed effects, birth year fixed effects, survey year fixed effects, mother's age, mother's
education, dummy for urban, birth order, and existing sex ratio of children (defined as the ratio of boys to the total number of births
prior to the most recent one). National sample weights are used in all regressions .

At least 2
Prenatal Visits
At least 2
Tetanus Shots
(1=Yes,0=No)
Non-hone
Delivery
(1=Yes,
0=No)
At least 2
Prenatal Visits
At least 2
Tetanus Shots
(1=Yes,0=No)
Non-hone
Delivery
(1=Yes,
0=No)(1) (2) (3) (4) (5) (6)
Male 0.013** 0.013** 0.018*** 0.027** 0.012 0.018
(0.005) (0.006) (0.007) (0.011) (0.011) (0.012)
Mean of Dependent Variable 0.889 0.848 0.419 0.813 0.783 0.280
Observations 22983 23016 22351 7547 7630 7365
R-Squared 0.091 0.063 0.342 0.082 0.069 0.216
Prenatal Care
(1=Yes,
0=No)
Number of
Prenatal visits
Tetanus Shot
(1=Yes,
0=No)
Number of
Tetanus Shots
Iron Pills
(1=Yes, 0=No)
Non-Home
Delivery
(1=Yes,
0=No)
(1) (2) (3) (4) (5) (6)
Male 0.022 0.112* 0.031** 0.082** 0.029* 0.004
(0.015) (0.064) (0.015) (0.034) (0.016) (0.013)
Birth Order 0.017 0.209 0.018 0.016 0.032 -0.019
(0.041) (0.181) (0.040) (0.095) (0.043) (0.036)
Existing Sex Ratio of Children 0.020 0.093 -0.017 -0.021 0.006 -0.016
(0.018) (0.084) (0.018) (0.044) (0.021) (0.017)
Mean of Dependent Variable 0.626 2.297 0.715 1.460 0.544 0.267
Mother Fixed Effects Yes Yes Yes Yes Yes Yes
Birth Year Fixed Effects Yes Yes Yes Yes Yes Yes
Observations 6304 6293 6287 6287 6329 6308
R-squared (within) 0.030 0.005 0.011 0.007 0.013 0.003
Number of Mothers 3968 3962 3956 3956 3982 3969
TABLE 7. Sex-Selective Prenatal Investments in India: Additional Prenatal Care
All with At Least 1 Prenatal VisitAll with First Prenatal Checkup during the Final
5 Months of Prengancy
TABLE 8. Sex-Selective Prenatal Investments in India: Mother Fixed Effects Specification
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to two most recent births of ever married women (ages 15-49). Sample includes only mothers who report prenatal
investment information for at least 2 births in the 5 years within previous to the survey. Existing sex ratio is defined as the ratio of boys to the total
number of births prior to the most recent one.
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to most recent birth (within 5 years previous to the 2005-6 survey only) of ever married women. Controls include:
state fixed effects, birth year fixed effects, survey year fixed effects, mother's age, mother's education, dummy for urban, birth order, and existing
sex ratio of children (defined as the ratio of boys to the total number of births prior to the most recent one). National sample weights are used in
all regressions .

India China Bangladesh Pakistan Ghana Sri Lanka Thailand
Survey years
(1992-3), 1998-
9, 2005-6
1991, 1993,
1997, 2000,
2004, 2006
1996-7, 1999-
2000, 2004 2006-7
1993, 1998,
2003, 2008 1987 1987
Birth years 1995-2006 1989-2006 1991-2007 2001-2007 1988-2008 1982-1987 1982-1987
Number of observations 36755 1482 15916 5063 14290 2190 1986
Level of spatial fixed effects State Community Region District Region Region Region
Number of communities, states or regions 29 235 6 54 10 7 5
Mother Characteristics Observations Mean Standard Dev. Min Max
Age 36755 28.08 5.52 15 49
Education 36755 0.90 1.00 0 3
National Wealth Quintile 36755 2.95 1.37 1 5
Pregnancy Characteristics
Mean
(Standard Dev.) Observations
Mean
(Standard Dev.) Observations
Mean
(Standard Dev.) Observations
Male 0.55 36755
Birth order 3.48 36755 3.46 20041 3.50 16714
(1.78) (1.76) (1.79)
Existing Sex Ratio of Children 0.49 36755 0.47 20041 0.51 16714
(0.39) (0.39) (0.39)
Ultrasound Receipt (1=Yes,0=No): 1998-9
only 0.14 9140 0.14 4986 0.13 4154
Ultrasound Receipt (1=Yes,0=No): 2004-5
only 0.27 18888 0.28 10353 0.26 8535
Prenatal Care (1=Yes, 0=No) 0.72 32233 0.73 17503 0.71 14730
Number of Prenatal visits 3.09 32012 3.16 17377 3.01 14635
(3.17) (3.20) (3.13)
Tetanus Shot (1=Yes, 0=No) 0.78 32017 0.79 17376 0.77 14641
Number of Tetanus Shots 1.64 32017 1.66 17376 1.61 14641
(1.03) (1.02) (1.04)
Iron Pills (1=Yes, 0=No) 0.61 32166 0.62 17458 0.61 14708
Days Took Iron Supplement 45.53 17698 46.32 9654 44.58 8044
(63.08) (63.52) (62.55)
Non-Home Delivery (1=Yes, 0=No) 0.35 31073 0.36 16869 0.33 14204
Notes: Education of mother is the highest level of educational attainment: 0 = no education, 1 = primary school, 2 = secondary school, 3 = higher
education. Sample includes most recent births by ever married women (ages 15-49) within 5 years previous to the survey. Existing sex ratio is
defined as the ratio of boys to the total number of births prior to the most recent one. Statistics describe the sample and are thus not weighted.
APPE�DIX TABLE 1. Description of Regression Samples.
Country
APPE�DIX TABLE 2. Summary Statistics for India
All Male Female

No Controls
Geographic and
Survey Controls
Adding Child-level
Controls
Adding Mother-
level Controls
Adding Household-
level Controls
(1) (2) (3) (4) (5)
Male 0.016** 0.017*** 0.016*** 0.013** 0.011**
(0.007) (0.006) (0.006) (0.006) (0.006)
Urban 0.133*** 0.116*** 0.071*** 0.026***
(0.007) (0.007) (0.007) (0.007)
Birth Order -0.042*** -0.033*** -0.028***
(0.002) (0.002) (0.002)
Existing Sex Ratio of Children -0.029*** -0.025*** -0.023***
(0.007) (0.007) (0.007)
Mother's Age 0.002** 0.156***
(0.001) (0.010)
Mother's Education 0.087*** 0.196***
(0.003) (0.012)
Family Wealth is in 2nd Quintile 0.001
(0.001)
Family Wealth is in 3rd Quintile 0.058***
(0.004)
Family Wealth is in 4th Quintile 0.064***
(0.009)
Family Wealth is in 5th Quintile 0.115***
(0.009)
Constant 0.679*** 0.939*** 1.100*** 0.968*** 0.916***
(0.005) (0.011) (0.020) (0.024) (0.025)
State Fixed Effects No Yes Yes Yes Yes
Year Fixed Effects No Yes Yes Yes Yes
Birth Year Fixed Effects No No Yes Yes Yes
Dummy Variable for Each HH Wealth QuintileNo No No No Yes
Observations 32233 32233 32233 32233 32233
R-squared 0.000 0.250 0.276 0.300 0.311
APPE�DIX TABLE 3. Sex-Selective Prenatal Investments in India: Robustness to Different Sets of Control Variables
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1
Notes: Sample is restricted to most recent birth of ever married women (ages 15-49) within 1 year previous to the survey. Days took iron
supplements is available only for the 2004 survey. Existing sex ratio is defined as the ratio of boys to the total number of births prior to the most
recent one. National sample weights are used in all regressions.
Dependent Variable: Prenatal Care (1=Yes, 0=�o)

Coefficient on Male in various
countries
Prenatal
Care (1=Yes,
0=No)
Number of
Prenatal
visits
Tetanus Shot
(1=Yes,
0=No)
Number of
Tetanus
Shots
Non-Home
Delivery
(1=Yes,
0=No)
(1) (2) (3) (4) (5)
China 0.046* 0.346* na na
(0.027) (0.205)
Bangladesh 0.003 0.076** 0.028*** 0.039* 0.001
(0.009) (0.037) (0.009) (0.021) (0.003)
Pakistan 0.018 0.184* 0.020 0.016 0.006
(0.015) (0.100) (0.016) (0.039) (0.014)
Pakistan (Punjab Region) 0.019 0.268* 0.015 0.014 0.026
(0.021) (0.152) (0.023) (0.056) (0.020)
Sri Lanka 0.002 na 0.010 na 0.014
(0.008) (0.016) (0.014)
Thailand 0.005 na 0.020 na 0.014
(0.017) (0.022) (0.018)
Ghana -0.013** 0.010 0.004 0.003 0.003
(0.006) (0.078) (0.009) (0.024) (0.010)
APPE�DIX TABLE 4. Sex-Selective Prenatal Care in Other Countries
Notes: Sample is restricted to most recent birth of ever married women (under the age of 52 in China and
ages 13-49 in Bangladesh) within 5 years previous to the survey. Tetanus information and wealth index
is not available for China. Wherever available, controls include: state fixed effects, birth year fixed
effects, survey year fixed effects, mother's age, mother's education, dummy for urban, birth order, and
existing sex ratio of children (defined as the ratio of boys to the total number of births prior to the most
recent one). National sample weights are used in all regressions. Due to the One Child Policy in China,
we do not control for existing sex ratio and we include pregnancy number rather than birth order.
Outcome
Robust standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1