Embed Size (px)
Citation preview

1
Discrepancies between objective findings and subjective state of health in the process of rehabilitation and their effects on health-
related quality of life
Reinhold Jagsch
Faculty of Psychology,
University of Vienna, Austria
Correspondence to:
Reinhold Jagsch
Liebiggasse 5/3rd floor A-1010 Vienna
Austria
Telephone: + 43 - 1 - 4277 – 478 93
Fax: + 43 - 1 - 4277 – 478 99
e-mail:[email protected]

2
Summary. Background: This article provides an overview of studies in which
assessments of specific functional capacity, made by experts on the one hand
(objective) and by patients on the other (subjective) were compared in various patient
groups. In essence, these data reveal marginal or insignificant associations.
Methods: Based on these considerations, a theoretical differential-diagnosis model of
objective findings/subjective state of health is presented. By dichotomization of
specific functional capacity at these two levels, the model permits the classification of
a patient cohort into four sub-groups: Patients with concurrence between subjective
and objective assessments are referred to as “the fortunate” while those with a
negative concurrence are termed “the unfortunate”. In case of discrepancies between
these two levels, for instance when patients’ subjective assessment was good
although their condition was obviously poor, they are considered to be in a so-called
“disease paradox”. Alternatively, patients whose subjective assessment of their
condition was poor although the objective findings were positive, were considered to
be in a so-called “health dilemma”.
Results: The study in a sample of patients who had received an artificial hip joint for
mobility disorders revealed striking differences in health-related quality of life (HrQol).
Comparisons of HrQoL data pre- and post-operatively in the whole sample
demonstrated an improvement in five of six dimensions (loss of energy, pain,
emotional reaction, sleeping problems, and problems in physical mobility, p<0.01) of
the Nottingham Health Profile. Specifically, after grouping patients accordingly to the
proposed model striking positive changes in HrQoL were registered in patients of the
fortunate and disease paradox groups while the improvements in the health dilemma
and unfortunate groups were minimal.

3
Conclusion: Timely identification of these patients in the process of rehabilitation
would significantly contribute to the achievement of a good health-related quality of
life for all patients.
Key words: Health-related quality of life, Nottingham Health Profile, functional
capacity, total hip arthroplasty

4
Introduction
One of the first researchers who focused on this point of intersection between
medicine and clinical psychology and conducted a specific and comprehensive study
of the discrepancies between the judgments of medical experts and those of patients
in respect of their state of health was Myrtek (1998). In his theory of illness behavior,
Myrtek described a scheme of four categories consisting of two congruent groups
which he named healthy and ill persons in the medical sense. Apart from these, he
identified two discrepant groups which he assigned “inappropriate illness behavior”
(in 1978 Pilowsky had termed this phenomenon “abnormal illness behavior”).
Depending on their inclination, he named these groups “healthy ill persons” or “ill
healthy persons”, as evidenced by the title of his book.
A few years earlier, in 1991, Filipp and Ferring had made a similar formal
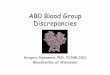
classification, a division into four categories. In their description of subjectivity and
objectivity in the determination of quality of life, they also distinguished between four
groups: In case of concurrence of subjective and objective evaluations of quality of
life they referred to the persons as “the fortunate”; in case of negative concurrence
the authors referred to the individuals as “the unfortunate”. In case of discrepancies
between these two levels, for instance when the individuals’ subjective assessment
was good although their objective state was evidently poor, these persons were
considered to be in a paradox situation, i.e. in a “satisfaction paradox”. Alternatively,
the individuals were deemed to be in a “dissatisfaction dilemma” when their
subjective assessment of their condition was poor despite the presence of positive
environmental factors (Figure 1).

5
objective surrounding subjective evaluation of one´s own life
factors good bad good
the fortunate
dissatisfaction dilemma
bad
satisfaction paradox the unfortunate
Figure 1. Original scheme of Filipp and Ferring (1991) describing general quality of life.
These concepts were demonstrated by results from practical experience, based on a
psychological study of Brickman, Coates and Janoff-Bulman (1978). The authors
requested three groups of test persons to asses their state of happiness, i.e. their
subjective state. The first group consisted of lottery winners, the second of patients
who had suddenly been confronted with the diagnosis of paraplegia following a life-
threatening accident, and the third was a control group. An evaluation of the
assessments of their current status revealed that the patients’ subjective state was –
as expected – highly significantly poorer than that of the control group. However, it
was striking to note that the subjective state of lottery millionaires, apparently favored
by fortune, was hardly better than that of the control group. The probands’ prognostic
assessments of their state of health at a fictitious time-point in the near future (about
one year) were entirely unexpected for the layman: Despite extremely diverse
external environmental factors, the three groups gave nearly identical estimates of
their future subjective states.
Discrepancies between objective findings and subjective state of health in the health sector
Accordingly, several studies have shown that associations between doctors’
estimations of health-related stresses and the corresponding evaluations of patients
remain insignificant. In a large preventive study focusing on cardiovascular disease in

6
middle-aged men, Robra, van der Heyden and Machens (1982) observed
pathologically elevated cholesterol and blood sugar levels in 20.7% and 12.0%,
respectively. Smoking and obesity are known to be major risk factors for
cardiovascular disease. However, if one considers the medical history and the state-
of-health data of the high-risk group, persons deemed to be at great risk reported
milder symptoms than did persons with no risk factors. The agreement between the
doctors’ estimations of the health status of middle-aged women and the women’s
own evaluations was reported to be 22% by a Swedish group; the authors
considered this value significant but low. Correlative associations between individual
symptoms and the estimations explained only 1 to 12% of the underlying variance
(Mellner & Lundberg, 2003). Similarly, objective stress values in a healthy population
showed only moderate agreement with the corresponding assessments obtained by
questionnaires (Lindholm, Brevinge, Bergh, Körner & Lundholm, 2003). This
phenomenon is observed in patients with physical disease as well: In a randomized
group of patients with different somatic diagnoses, Mabe, Hobson, Jones and Jarvis
(1988) requested the treating physicians to assess the severity of symptoms on a
seven-point Likert scale. A comparison of these assessments with those of patients
revealed a non-significant correlation value of 0.10; a large majority of the patients
over-estimated the severity of their symptoms. Michel, Kohlmann and Raspe (1997)
established a moderate agreement (kappa = 0.47) between the treating physicians
and the patients in respect of the severity of symptoms in a specific patient group
(back pain). Filipp and Ferring (1991) report an insignificant correlation coefficient of r
= 0.17 in a random sample of gastroenterological patients.
Confirmation of the presence of a wide discrepancy between the objective and the
subjective state of health reported by patients, and the theoretical models proposed

7
for this phenomenon in the published literature, will be investigated here in order to
answer the following question: Is it possible to identify the above mentioned four
groups on the basis of the clinical condition (specific functional capacity) of patients in
the process of rehabilitation within a precisely defined cohort?
Explanation of terms
For the following study the above mentioned theoretical models were used and
modified as follows: The modified Viennese model was based on one variable that is
accessible to objective as well as subjective assessment, namely the so-called
specific functional capacity. What does “specific” functional capacity here mean; in
what way does it differ from a “general” functional capacity that may be present?
Owing to the Babylonian confusion of terms, which is frequently mentioned in the
literature (Leplege & Hunt, 1997) – Tully and Cantrill (1999) call it the “semantic
minefield” – a digression is given here, which delineates the medical and
psychological constructs used in this study.
The extent of “health-related quality of life” as determined by the patients was
selected as the outcome variable because, on the one hand, one of the goals of
rehabilitation is to improve the patient’s quality of life (Richter, Schwarz, Eisemann &
Bauer, 2003; WHOQoL Group, 1995) and, on the other hand, quality of life is
considered to be a dynamic construct that may change in the course of time, e.g.
when a critical event in life occurs or the patient undergoes a severe type of medical
treatment (Allison, Locker & Feine, 1997). The term quality of life actually originated
in the social sciences. It was coined in welfare economics in the beginning of the 20th
century. Quality of life achieved socio-political significance, especially in the USA,
from the mid-sixties of the last century. It entered Europe somewhat later, where it
was offered as an alternative to counter the pre-eminence of purely quantitative

8
thought. In other words, purely economical indices were complemented by social
factors. In the health sector, the concept of quality of life research, i.e. the concept of
health-related quality of life became established only in the beginning of the
nineteen-eighties. Although one would presume that a subject like health-related
quality of life of patients should be of major importance in this sector, i.e. for medical
specialists, psychologists and health-care personnel, a scientific discussion about the
theory and measurement of this construct started rather late. After individual survey
instruments had been constructed and tested in practice, the last few years have
witnessed a revival, a kind of retrospective look at the theoretical and methodological
principles of quality of life research, coupled with considerations as to how such
research can be systematically integrated in the evaluation, quality assurance and
planning of future health care services (Bullinger, Ravens-Sieberer & Siegrist, 2000).
The reason is to be found in the indeterminateness and poor tangibility which
persisted for a long time around this construct. Quality of life is a construct that is
considered familiar by many because of its practical context, but has not been
scientifically defined until the present day. The importance of health-related quality of
life clearly lies in the fact that it has made a significant contribution to a
transformation – farther away from a purely mechanistic-physiological view of the
anonymous patient, and closer to a holistic appraisal of the individual. The main
points of focus of this concept are the individual, his/her thoughts and feelings, state
of health, and ability to cope with the disease (Rosenberg, 1995). Despite the
absence of a comprehensive and widely accepted definition, experts agree that
health-related quality of life must be regarded as a multi-dimensional construct
consisting of the following main components (Bullinger & Hasford, 1991):
physical state (general state, mobility, pain),

9
psychological state (cognitive and emotional factors),
social integration (integration and social support), and
coping with activities of daily living (functional competence).
In this context, subjectivity, i.e. self-reports of patients is given emphasis. In fact, the
measurement of quality of life in health and illness is determined by the patient’s
subjective assessment (Bullinger et al., 2000; Majani, Giardini & Scotti, 2005; Ormel,
Lindenberg, Steverink & von Korff, 1997; Ravens-Sieberer, Cieza & Bullinger, 2001).
Both “functional competence” and various aspects of the “physical state” address
elements of the above mentioned term “functional capacity”. The basic distinction to
be made between the grouping variable (assignment of individual patients to the
experimental groups) and the dependent variable (outcome in respect of the health-
related quality of life of patients) is based on the two components “assessment level”
and “degree of generality”. In order to divide patients into the four categories
mentioned above, one would have to use a construct that allows the evaluation of
specific functional impairments (i.e. not general functions) at two levels (objective
versus subjective). Orthopedic experts have standardized calculation formulae which
they use to quantify behavior samples obtained in catamnestic investigations in order
to include, or weight, several factors like limitations in flexion or joint mobility in the
overall evaluation. On the other hand, these disabilities or limitations can be
subjectively evaluated by the patients themselves. The patient is asked to provide
information on these subjects by the use of targeted questions in specific functional
questionnaires. Thus, the first condition is the possibility to evaluate the same
construct (specific functional capacity) simultaneously from a subjective viewpoint (by
the patient) and from the external viewpoint (a trained expert who has extensive

10
experience). With the help of appropriate operationalization, it should be possible to
identify discrepancies or agreements/concordances between objective findings
(objective assessment of the expert) and subjective states of health (subjective
assessment of the progress of rehabilitation by the patient himself/herself). The
second condition is that a multi-dimensional concept of evaluation should be applied
for the outcome. It may include functional aspects (such as those in the survey of
quality of life) but, in terms of its concept, should address function (or functional
limitations which have been empirically proven to aggravate, for instance with
advancing age) at a general level. The following examples of items from the
investigation instruments will demonstrate this distinction in a descriptive way: The
item “I can move only within the house” (item 10 of the quality of life questionnaire
known as the Nottingham Health Profile) investigates the ability “physical mobility” at
a general level, non-specifically, with the options “yes” versus “no”, while the question
“Can you stand for 30 minutes without interruption (e.g. in a queue)?” (item 6 of the
Hannover functional questionnaire), a function that was impaired by the disease, is
inquired specifically, with the option of grading one’s response.
In a meta-analysis published in 1999, Smith, Avis and Assmann mention that the
terms “quality of life” and “health status” have often been used interchangeably, but
refer to two distinct concepts. Empirical evidence of the distinction between specific
functional capacity (as registered objectively by the expert and also subjectively by
the patient) and general functional aspects (such as those included in quality of life
questionnaires) was provided recently by Fritz and Piva (2003) from back pain
research. Using the Physical Impairment Index (PII) constructed by Waddell’s
research group (Waddell, Somerville, Henderson & Newton, 1992), a questionnaire
that investigates the “specific functional capacity” of back pain patients, Fritz and Piva

11
(2003) studied aspects of reliability and validity in patients with acute symptoms. In
the course of this investigation the authors were able to establish a significant
correlation of r = 0.43 (explained variance, 18.5%) for both instruments that measure
“specific functional capacity” at both levels of assessment (objective versus
subjective). The correlation between PII and the physical component score of the
quality of life instrument SF-36 was significant at the level of 5%, but poorly relevant
with a coefficient of r = 0.28 (explained variance, 7.8%), while the correlation with the
mental component score was r = 0.00.
A prerequisite at the theoretical level, in order to conduct such empirical studies in
the field of objective findings/subjective state of health, is that the construct used to
assign patients to the respective groups according to concordant or discrepant
judgments must be specific and also accessible to objective and subjective
assessment. On the other hand, in order to avoid overlapping and confounding of
group and outcome variables, the construct to be used as the study outcome should
be purely subjective and not specific, but general.
Model to study Objective findings/Subjective state of health
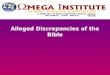
A new theoretical base was created with this procedure. It reversed the model of
Filipp and Ferring (1991) described above in Figure 1 for differential-diagnostic
purposes in the field of somatic diseases. The modified Viennese model no longer
serves to describe components of quality of life at different levels. Rather, the
congruent or discrepant assessments of experts and patients on the basis of
functional assessments in the process of rehabilitation serve to determine different
groups whose health-related quality of life then is compared as the outcome (Figure
2).

12
objective findings,
subjective patient´s evaluation of functional capacity
expert´s evalution of patient´s functional
capacity
good less good
good
the fortunate health dilemma
less good
disease paradox the unfortunate
Figure 2. Viennese “Objective findings/Subjective state of health-model” (“Befund/Krankheitserleben”-model).
Pilot study: Patients, Material, and Methods
Orthopedic patients are very suitable for the implementation and empirical testing of
the said pre-conditions, particularly because appropriate survey instruments are
either available or being used in a standardized manner in this specialty. In the
following investigation, which was conducted in cooperation with the Orthopedic
Hospital Speising in Vienna, the Harris Hip Score (Harris, 1969) was used as the
objective instrument to measure the specific functional capacity of orthopedic patients
while the Hannover Functional Questionnaire (Kohlmann & Raspe, 1996; Kohlmann
et al., 1999) was employed as the subjective instrument. The first is a classification
instrument used by orthopedists to assess the success of hip surgery. Four different
dimensions evaluate the patient’s current functional capacity as assessed by the
orthopedist: mobility, functional activity, pain and deformity. The sum of the four
weighted scores is used to assign the patient to one of four categories on a scale
from 0 to 100 (very good: 90–100, good: 80–90, moderate: 70–80 and poor: less
than 70). The questionnaire to survey subjective functional capacity contains 18
items with which the patient assesses his/her impairment of motor activities in daily

13
life in a three-categorical format (“yes”, “yes but with difficulty”, “no”; a copy of the
questionnaire can be found in Knahr, Kryspin-Exner, Jagsch, Freilinger & Kasparek,
1998, page 325). Low scores indicate good functional capacity. Thus, the two
instruments to assess specific function are poled in opposite directions.
The sample consisted of patients who had received total arthroplasty for age-related
signs of wear in the hip joint. The assessments of the orthopedist and the patients
themselves in respect of the specific functional capacity, using the instruments
available for this purpose, before the operation and from the catamnestic
investigation after one year, were analyzed. The results used to compare the two
time points have been reported elsewhere (Knahr et al., 1998). The patients were
assigned to the groups at the time point of catamnesis (one year post-surgery)
because the functional evaluation here is based on the patients’ rehabilitative status.
The group classification was operationalized by respective dichotomization of the two
assessments into “good” and “not good” based on the data from the empirical
sample, so that statements like “good compared to the assessments of other
patients” or “less good compared to the assessments of other patients” were
rendered possible. From a practical point of view the procedure was implemented by
dividing the scores of patients and experts at the median value.
The investigated sample consisted of 139 patients who had been operated on in the
Orthopedic Hospital Speising in Vienna. Of this initial cohort, 101 patients (72.7%)
could be examined one year after the operation. The mean age of the patients at the
time of surgery was 64.2 years (SD, 12.7 years; range, 25 to 88 years); the
female/male ratio was 2:1 (63.4% were women). The diagnoses were mainly
idiopathic coxarthrosis and necrosis of the femoral head; the principal symptoms
were pain and limitation of mobility. Part 1 of the Nottingham Health Profile (NHP)

14
was used as the instrument to measure health-related quality of life. A validated
German translation of this questionnaire has been provided by Kohlmann, Bullinger
and Kirchberger-Blumstein (1997). Part 1 consists of a total of 38 items to be
answered in a yes/no format. These 38 items are assigned to six different sub-scales:
loss of energy (EN, 3 items),
pain (PA, 8 items),
negative emotional reaction (EM, 9 items),
sleeping difficulties (SL, 5 items),
social isolation (SO, 5 items), and
limitation of physical mobility (PM, 8 items).
This instrument was selected because it is very economical (takes 5 to 10 minutes)
and possesses good test criteria (the Cronbach alpha value for the internal
consistency of the sub-scales is between 0.65 and 0.85 (Jagsch & Pils, 2006;
Kohlmann et al., 1997). For comparing baseline as well as continuous
sociodemographic and disease-specific data (age and duration of symptoms) one-
way ANOVA was used with following post-hoc Scheffé tests, Chi2-tests for
categorical data (gender). t-tests for dependent samples were used to compare
means between the time points. In case of non-normal distribution of data,
nonparametric Wilcoxon’s signed-ranks test was used. The level of significance was
set at 5%.

15
Results
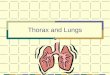
The data of the entire cohort show that the operation leads to a significant
enhancement of health-related quality of life. There were significant improvements in
five of the six sub-scales after one year. Only in the social sector the scores
remained constant; the baseline data already showed very good social integration
before surgery (Figure 3).
postpre
100
80
60
40
20
0
EN **
PA **
EM **
SL **
SO
PM **
37
64
56
32
52
17
26
31
77
38
50
Figure 3. Changes in health-related quality of life of the whole sample of patients (N=101).
** p<0.01

16
To date, the five-year catamnesis has been performed for about 50% of the initial
cohort (about 70 patients). This assessment showed that the enhancement in health-
related quality of life can be retained over a long period of time (Knahr, Jagsch &
Kryspin-Exner (2003).
For the subsequent analysis the patients were divided into the four groups described
above, using a double median split, at the catamnesis investigation performed one
year after surgery. The empirical mean was 93 for the Harris Hip Score and 33.33 for
the Hannover functional questionnaire; the correlation between the two functional
scores was -0.54 (explained variance, 29.2%). In all, about three quarters of the
patients were able to achieve concurrence between subjective and objective
assessments; these patients consisted of nearly equal numbers of the “fortunate” (38
patients; 37.6%) and the “unfortunate” (37 patients; 36.6%). The remaining one
quarter was divided into 15 patients in the “disease paradox” (14.9%) and 11 patients
in the “health dilemma” (10.9%) (Figure 4).
unfortunate 36.6%
DP 14.9%
HD 10.9%
fortunate 37.6%
Figure 4. Distribution of the patients according to the four subgroups. HD = health dilemma, DP = disease paradox

17
Comparisons between the four groups revealed no differences concerning gender
distribution (Chi2=1.011, df=3, p=0.798) or duration of symptoms (F=1.052, df=3,
p=0.373). Differences in age yet showed a significant result in the four group ANOVA
comparison (F=2.836, df=3, p=0.042) but proved insignificant then in the following
post-hoc Scheffé tests (p>0.10). The analysis of the baseline scores at the time of
surgery revealed only marginal differences between the four random sample
fractions. The “fortunate” and the “unfortunate” differed only in the sub-scale “physical
mobility” (p=0.031; post-hoc Scheffé test). As predicted, “fortunate” patients achieved
the greatest advancements in health-related quality of life. In this group, significant
improvements (p<0.01) were registered in all dimensions except social isolation,
analogous to the total sample (Figure 5a).
postpre
100
80
60
40
20
0
EN **
PA **
EM **
SL **
SO
PM **
13
56
17
49
8
23
11
78
11
36
Figure 5a. Changes in health-related quality of life of the “fortunate” (n=38). ** p<0.01

18
Likewise, as expected, the “unfortunate” patients achieved the poorest results,
characterized by a concurrent poor evaluation of the rehabilitative functional capacity.
Improvements (p<0.01) were registered only for pain (Figure 5b).
postpre
100
80
60
40
20
0
EN
PA **
EM
SL
SO
PM
64
71
79
46
54
2927
56
79
6359
Figure 5b. Changes in health-related quality of life of the “unfortunate” ( =37). ** p<0.01
In the comparison of the groups, the patients of the “health dilemma” group also
revealed the same longitudinal pattern; improvements (p<0.01) were registered only
for pain while the other scales showed no statistical differences compared to the
baseline values (Figure 5c).

19
postpre
100
80
60
40
20
0
EN
PA **
EM
SL
SO
PM
51
60
5
40
47
13
21
34
69
4548
Figure 5c. Changes in health-related quality of life of the health dilemma patients (n=11). ** p<0.01
The data of the “disease paradox” group, on the other hand, were quite similar to
those of “fortunate” patients, but on a slightly lower level: significant improvements for
pain, sleeping difficulties, physical mobility (p<0.01) and emotional reaction (p<0.05)
(Figure 5d).

20
postpre
100
80
60
40
20
0
EN
PA **
EM *
SL **
SO
PM **
22
69
78
25
56
16
31
21
73
40
62
Figure 5d. Changes in health-related quality of life of the disease paradox patients (n = 15). ** p<0.01, * p<0.05
The changes are shown in detail in Table 1.
Table 1. Significance of changes of the whole sample and of the four subsamples in the subscales of NHP whole sample fortunate HD DP unfortunate df=100 df=37 df=10 df=14 df=36 EN t=2.680, p=0.009 t=4.093, p<0.001 t=0.430, p=0.676 t=1.784, p=0.096 t=-0.597, p=0.554 PA t=12.293, p<0.001 t=14.409, p<0.001 t=4.113, p=0.002 t=6.136, p<0.001 t=3.966, p<0.001 EM t=3.073, p=0.003 t=3.284, p=0.002 t=1.099, p=0.298 t=2.355, p=0.034 t=-0.273, p=0.787 SL t=6.209, p<0.001 t=5.771, p<0.001 t=0.841, p=0.420 t=3.944, p=0.001 t=1.666, p=0.104 SO t=0.884, p=0.379 t=-0.467, p=0.644 Z=-1.732, p=0.083 Z=-0.577, p=0.564 t=0.850, p=0.401 PM t=8.573, p<0.001 t=12.005, p<0.001 t=0.886, p=0.397 t=6.219, p<0.001 t=1.697, p=0.098 Note. HD = health dilemma, DP = disease paradox; EN = loss of energy, PA = pain, EM = emotional reaction, SL = sleeping problems, SO = social isolation, PM = problems in physical mobilty

21
Discussion
In conclusion, this procedure showed that a characterization of patients in terms of
agreement versus discrepancy of functional capacity at the subjective and objective
levels yielded extremely diverse results in respect of the health-related quality of life
of these patients. Improvements only in one out of six subscales could be found for
all patients of all four groups, that is pain. In all other subscales except social
isolation a much more differentiated result can be seen where mainly the subjects’
personal estimation of their current functional capacity seems to be of much greater
importance than the objective assessment: “fortunate” patients and patients of the
“disease paradox” mainly benefit from the intervention while the other two groups
with exception of the pain section do not. These findings may help to draw
conclusions concerning differential diagnosis and the subsequent treatment of these
patients. Additional medical and/or psychological services should not be randomly
distributed among all patients according to the “watering can” principle, but rather
should be focused on the two groups that particularly are in need of such resources,
i.e. the “unfortunate” patients and patients of the “health dilemma”. The goal is to
improve health-related quality of life. Patients of the “disease paradox”, on the other
hand, appear to possess inner “health resources” to a great degree, which enable
them to grade their individual state better than the expert. As a result, their quality of
life achieves approximately the same level as that reported by “fortunate” patients.
The model of objective findings/subjective state of health presented here may help to
be used for a need-oriented application of rehabilitation services in the future bringing
together both macro- and micro-health needs (Asadi-Lari, Packham & Gray,
2003). Thus, a future plan may be to create a diversified rehabilitation program on
basis of the patient groups of the proposed model, in order to help activate such

22
potential inner “health resources” in this process and thus guarantee the best
possible health-related quality of life for all patients with different needs.

23
References
Allison, P.J., Locker, D. & Feine, J.S. (1997). Quality of life: A dynamic construct.
Social Science & Medicine, 45, 221–230.
Asadi-Lari, M., Packham, C. & Gray, D. (2003). Need for redefining needs. Health
and Quality of Life Outcomes, 1, 34.
Brickman, P., Coates, D. & Janoff-Bulman, R. (1978). Lottery winners and accident
victims: Is happiness relative? Journal of Personality and Social Psychology, 36,
917–927.
Bullinger, M. & Hasford, J. (1991). Evaluating quality-of-life measures for clinical trials
in Germany. Controlled Clinical Trials, 12, S91–S105.
Bullinger, M., Ravens-Sieberer, U. & Siegrist, J. (2000). Gesundheitsbezogene
Lebensqualität in der Medizin – eine Einführung. In M. Bullinger, J. Siegrist & U.
Ravens-Sieberer (Hrsg.), Lebensqualitätsforschung aus medizinpsychologischer
und -soziologischer Perspektive. Jahrbuch für Medizinischen Psychologie (S. 11–
21). Göttingen: Hogrefe.
Filipp, S.-H. & Ferring, D. (1991). Zur inhaltlichen Bestimmung und Erfassung von
Lebensqualität im Umfeld schwerer körperlicher Erkrankungen [On the
conceptualization and assessement of quality of life in the context of severe
physical diseases]. Praxis der Klinischen Verhaltensmedizin und Rehabilitation, 4,
274–283.
Fritz, J.M. & Piva, S.R. (2003). Physical Impairment Index: Reliability, validity, and
responsiveness in patients with acute low back pain. Spine, 28, 1189–1194.
Harris, W.H. (1969). Traumatic arthritis of the hip after dislocation and acetabular
fractures: Treatment by mold arthroplasty. An end-result study using a new
method of result evaluation. Journal of Bone and Joint Surgery (Am.), 51, 737–
755.
Jagsch, R. & Pils, K. (2006). Which instrument is more suitable to assess health-
related quality of life: Nottingham Health Profile or Short-Form 36? Wiener
Medizinische Wochenschrift, 156 (5/6), 149–157.
Knahr, K., Jagsch, R. & Kryspin-Exner, I. (2003). Long-term quality of life evaluation
of patients with total hip arthroplasty. Hip International, 13, 167–176.
Knahr, K., Kryspin-Exner, I., Jagsch, R., Freilinger, W. & Kasparek, M. (1998).
Beurteilung der Lebensqualität vor und nach Implantation einer Hüft-
Totalendoprothese [Evaluating the quality of life before and after implantation of a

24
total hip endoprothesis]. Zeitschrift für Orthopädie und ihre Grenzgebiete, 136,
321–329.
Kohlmann, T., Bullinger, M. & Kirchberger-Blumstein, I. (1997). Die deutsche Version
des Nottingham Health Profile (NHP): Übersetzungsmethodik und
psychometrische Validierung. Sozial- und Präventivmedizin, 42, 175–185.
Kohlmann, T. & Raspe, H.H. (1996). Der Funktionsfragebogen Hannover zur
alltagsnahen Diagnostik der Funktionsbeeinträchtigung durch Rückenschmerzen
(FFbH-R) [Hannover Functional Questionnaire in ambulatory diagnosis of
functional disability caused by backache]. Rehabilitation (Stuttg.), 35, I–VIII.
Kohlmann, T., Richter, T., Heinrichs, K., Peschel, U., Knahr, K. & Kryspin-Exner, I.
(1999). Entwicklung und Validierung des Funktionsfragebogens Hannover für
Patienten mit Arthrosen der Hüft- und Kniegelenke (FFbH-OA). In Verband
deutscher Rentenversicherungsträger (Hrsg.), 8.
Rehabilitationswissenschaftliches Kolloquium, Tagungsband. DRV-Schriften Bd.
12 (S. 40–42). Frankfurt am Main: VDR.
Leplege, A. & Hunt, S. (1997). The problem of quality of life in medicine. Journal of
the American Medical Association, 278, 47–50.
Lindholm, E., Brevinge, H., Bergh, C.-H., Körner, U. & Lundholm, K. (2003).
Relationships between self-reported health related quality of life and measures of
standardized exercise capacity and metabolic efficiency in amid-aged and aged
healthy population. Quality of Life Research, 12, 575–582.
Mabe, P.A., Hobson, D.P., Jones, L.R. & Jarvis, R.G. (1988). Hypochondriacal traits
in medical inpatients. General Hospital Psychiatry, 10, 236–244.
Majani, G., Giardini, A. & Scotti, A. (2005). Subjective impact of osteoarthritis flare-
ups on patient´s quality of life. Health and Quality of Life Outcomes, 3, 14.
Mellner, C. & Lundberg, U. (2003). Self- and physician-rated general health in
relation to symptoms and diseases among women. Psychology, Health &
Medicine, 8, 123–134.
Michel, A., Kohlmann, T. & Raspe, H. (1997). The association between clinical
findings on physical examination and self-reported severity in back pain. Results
of a population-based study. Spine, 22, 296–303.
Myrtek, M. (1998). Gesunde Kranke, kranke Gesunde. Bern: Huber.

25
Ormel, J., Lindenberg, S., Steverink, N. & von Korff, M. (1997). Quality of life and
social production functions: A framework for understanding health effects. Social
Science & Medicine, 45, 1051–1063.
Pilowsky, I. (1978). A general classification of abnormal illness behaviours. British
Journal of Medical Psychology, 51, 131–137.
Ravens-Sieberer, U., Cieza, A. & Bullinger, M. (2001). Lebensqualität aus
Patientensicht. Eröffnung einer neuen Perspektive für die Medizin [Quality of life
from the patient's point of view. Opening up a new perspective for medicine].
Chirurgische Praxis, 59, 3–12.
Richter, J., Schwarz, M., Eisemann, M. & Bauer, B. (2003). Quality of life as an
indicator for successful geriatric inpatient rehabilitation – A validation study of the
“Vienna List”. Archives of Gerontology and Geriatrics, 37, 265–276.
Robra, B.P., van der Heyden, E. & Machens, D. (1982). Herz-Kreislauf-
Vorsorgeprogramm VW/Salzgitter. Auswertung der Ergebnisse 1974 bis 1979.
Niedersächsisches Ärzteblatt, 21, 757–766.
Rosenberg, R. (1995). Health-related quality of life between naturalism and
hermeneutics. Social Science & Medicine, 41, 1411–1415.
Smith, K.W., Avis, N.E. & Assmann, S.F. (1999). Distinguishing between quality of
life and health status in quality of life research: A meta-analysis. Quality of Life
Research, 8, 447–459.
Tully, M.P. & Cantrill, J.A. (1999). Subjective outcome measures – A primer.
Pharmacy World and Science, 21, 101–109.
Waddell, G., Somerville, D., Henderson, I. & Newton, M. (1992). Objective clinical
evaluation of physical impairment in chronic low back pain. Spine, 17, 617–628.
WHOQoL Group (1995). World Health Organization quality of life assessment
(WHOQoL): Position paper from the World Health Organization.
Social Science & Medicine, 41, 1403–1409.