Embed Size (px)
Citation preview

1
MacrophageActivationSyndrome–KillorBeKilled
RandyQ.Cron,MD,PhD
UniversityofAlabamaatBirmingham
September22,2017UniversityofMissouri
5th AnnualJames&NancyCassidyRheumatologySymposium
Disclosures(last12months)
RandyQ.Cron,M.D.,Ph.D.
SOBI– investigatorinitiatedclinicaltrialofanakinra totreatMAS
CaseofPediatricMAS
•14yo girlwithCHPsince6mo.(dailyfeversto104,totalbodypanniculitis &lipoatrophy)•Presentswithabdominalpain&hepatomegaly,sizeof7-yearold® CsA &steroids•Onemonthlater,abdominalpain,seizure,GCSof7,CSFprotein, D-dimers,pancytopenia, ferritin, IFNg,IL-12•Multi-organsystemfailure(heart,lungs,kidney,liver,pancreas,bonemarrow,coagulopathy,CNS)
Behrens EM, Kreiger PA, Cherian S, Cron RQ. J Rheumatol. 2006 Oct;33(10):2081-4.

2
CaseofPediatricMAS- Pathology
Behrens EM, Kreiger PA, Cherian S, Cron RQ. J Rheumatol. 2006 Oct;33(10):2081-4.
Bone marrow
CD68 stain for skin -histiocytes
Skin biopsy at 9 mo.
CaseofPediatricMAS- Therapy
Behrens EM, Kreiger PA, Cherian S, Cron RQ. J Rheumatol. 2006 Oct;33(10):2081-4.
Hemophagocytic Lymphohistiocytosis(HLH)criteria
3
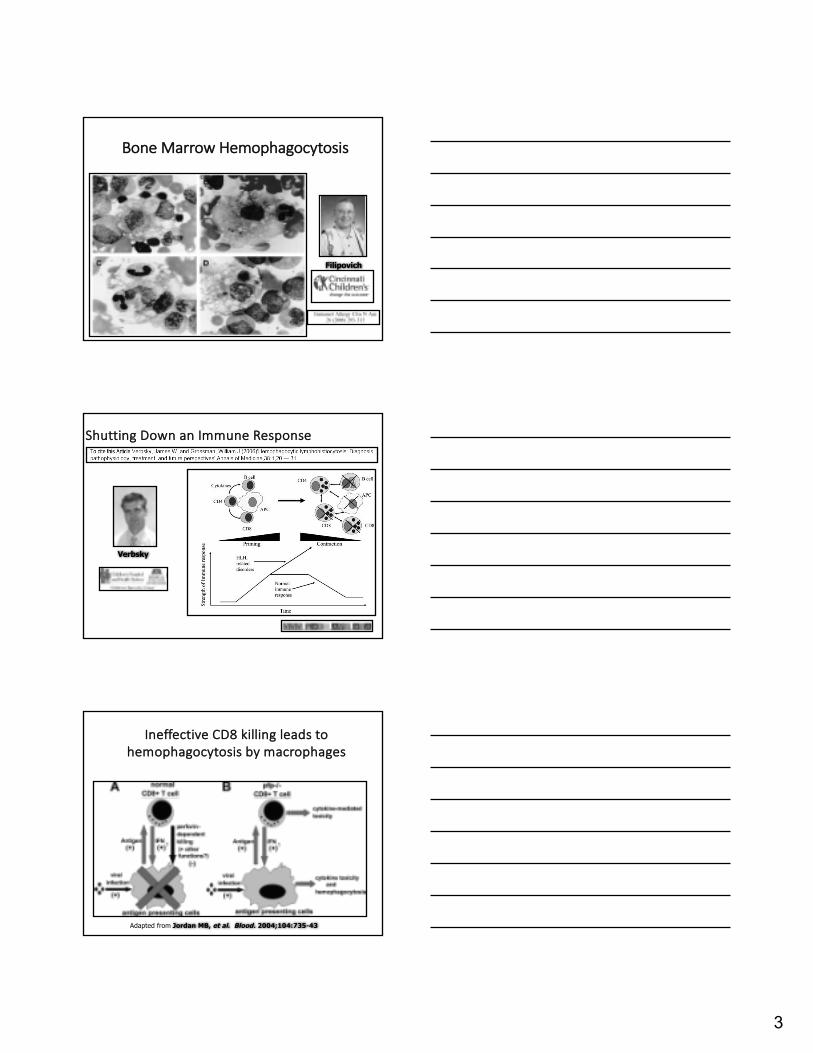
BoneMarrowHemophagocytosis
Filipovich
ShuttingDownanImmuneResponse
Verbsky
IneffectiveCD8killingleadstohemophagocytosisbymacrophages
Adapted from Jordan MB, et al. Blood. 2004;104:735-43

4
HLHAssociatedMutations
MPRSTX 11?
Courtesy: Dr. Alexei Grom
WhathavewelearnedfromthePrimarymodels?
• Requirementforinfection– EBVinSAP-/- mice(murineg-herpesvirus68)– LCMVinpfp -/-,MUNC-13-4-/-,Rab27a-/- mice–NeitherlisterianorMCMVinMUNC-13-4-/- mice–Animalsdeficientincytotoxicexocytosisareessentiallynormaluntilchallengedwithcertaininfections.
5
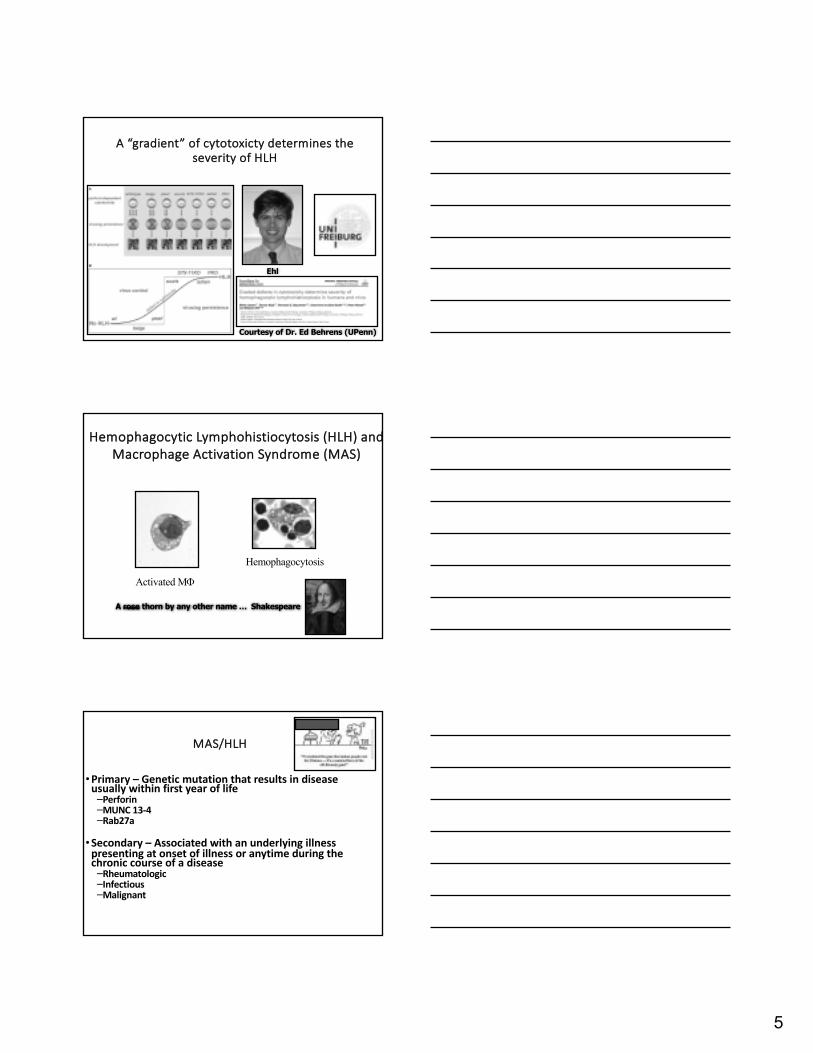
A“gradient”ofcytotoxicty determinestheseverityofHLH
Ehl
Courtesy of Dr. Ed Behrens (UPenn)
Hemophagocytic Lymphohistiocytosis (HLH)andMacrophageActivationSyndrome(MAS)
Activated MF
Hemophagocytosis
A rose thorn by any other name … Shakespeare
MAS/HLH
•Primary– Geneticmutationthatresultsindiseaseusuallywithinfirstyearoflife–Perforin–MUNC13-4–Rab27a
•Secondary– Associatedwithanunderlyingillnesspresentingatonsetofillnessoranytimeduringthechroniccourseofadisease–Rheumatologic–Infectious–Malignant
6
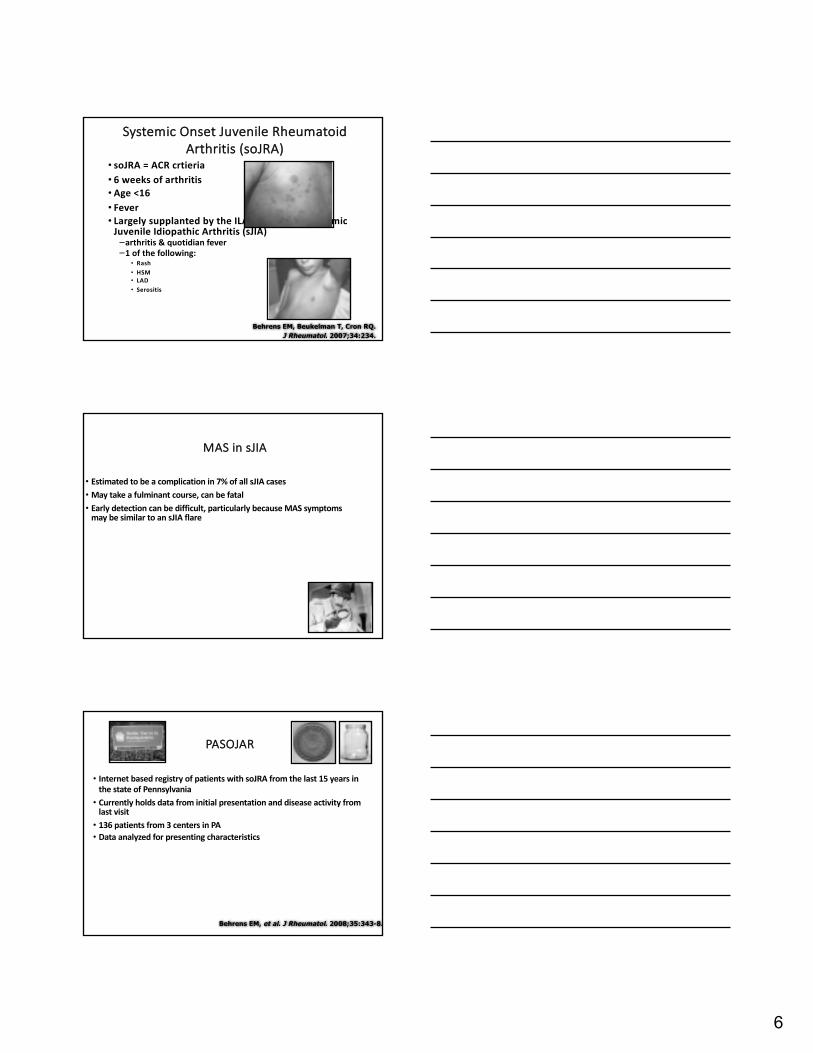
SystemicOnsetJuvenileRheumatoidArthritis(soJRA)
• soJRA=ACRcrtieria• 6weeksofarthritis• Age<16• Fever• LargelysupplantedbytheILARcriteriaforsystemicJuvenileIdiopathicArthritis(sJIA)–arthritis"idianfever–1ofthefollowing:
• Rash• HSM• LAD• Serositis
Behrens EM, Beukelman T, Cron RQ.J Rheumatol. 2007;34:234.
MASinsJIA
• Estimatedtobeacomplicationin7%ofallsJIAcases• Maytakeafulminantcourse,canbefatal• Earlydetectioncanbedifficult,particularlybecauseMASsymptomsmaybesimilartoansJIAflare
PASOJAR
• InternetbasedregistryofpatientswithsoJRAfromthelast15yearsinthestateofPennsylvania• Currentlyholdsdatafrominitialpresentationanddiseaseactivityfromlastvisit• 136patientsfrom3centersinPA• Dataanalyzedforpresentingcharacteristics
Behrens EM, et al. J Rheumatol. 2008;35:343-8.
7
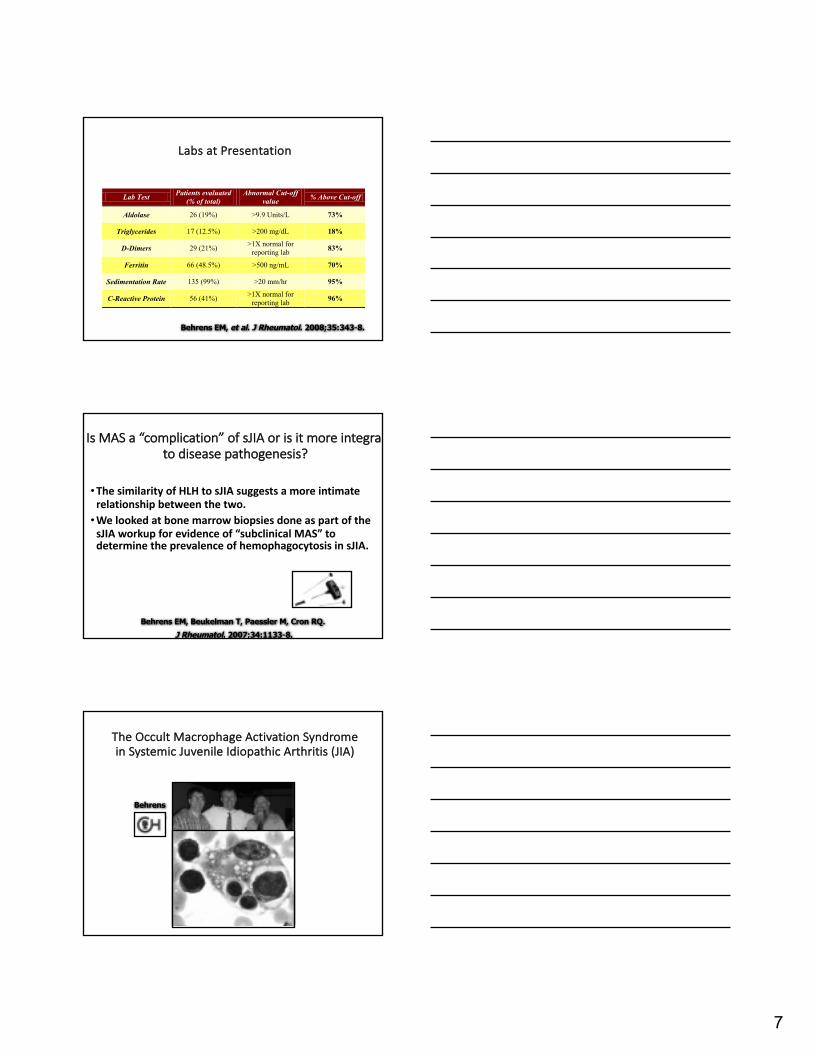
LabsatPresentation
Lab Test Patients evaluated (% of total)
Abnormal Cut-off value % Above Cut-off
Aldolase 26 (19%) >9.9 Units/L 73%
Triglycerides 17 (12.5%) >200 mg/dL 18%
D-Dimers 29 (21%) >1X normal for reporting lab 83%
Ferritin 66 (48.5%) >500 ng/mL 70%
Sedimentation Rate 135 (99%) >20 mm/hr 95%
C-Reactive Protein 56 (41%) >1X normal for reporting lab 96%
Behrens EM, et al. J Rheumatol. 2008;35:343-8.
IsMASa“complication”ofsJIAorisitmoreintegraltodiseasepathogenesis?
•ThesimilarityofHLHtosJIA suggestsamoreintimaterelationshipbetweenthetwo.•WelookedatbonemarrowbiopsiesdoneaspartofthesJIA workupforevidenceof“subclinicalMAS”todeterminetheprevalenceofhemophagocytosis insJIA.
Behrens EM, Beukelman T, Paessler M, Cron RQ.J Rheumatol. 2007;34:1133-8.
TheOccultMacrophageActivationSyndromeinSystemicJuvenileIdiopathicArthritis(JIA)
BehrensCHOP
8
Patient ID Cytopenia ESR CRP D-
dimer Fibrinogen Ferritin Triglyceride Initial
BM Read
BM Review
1 None 83 10.4 Normal Normal
2 None 77 28.9 1421 Normal HPC
3 Anemia 98 43.08 497 Normal HPC
4 None 96 Normal Unavailable
5 None 38 4.25 47 Normal Normal
6 Anemia 80 18.7 428 97 Normal Normal
7 Anemia 72 8.12 Normal Normal
8 None 92 4.19 6.36 98 Normal Normal
9 Anemia 50 7.7 2.39 419 Normal Normal
10 None 15 5.51 188 Normal Normal
11 Anemia 4.3 10.22 530 51 Activated MФ
Activated MФ
12 Anemia 135 15.5 5.47 427 Frank HPC
Frank HPC
13 Anemia 56 Normal Activated MФ
14 Normal HPC
15 None 89 12.5 10.29 568 8810 207 Frank HPC
Frank HPC
16 None 90 4.6 1.00 609 Frank HPC
Frank HPC
Control 1 None 131 3.0 Normal Normal
Control 2 None 80 4.8 Normal Normal
Control 3 None 56 4.6 14.9 968 Normal Normal
Control 4 None 43 4.6 0.86 449 Normal Normal
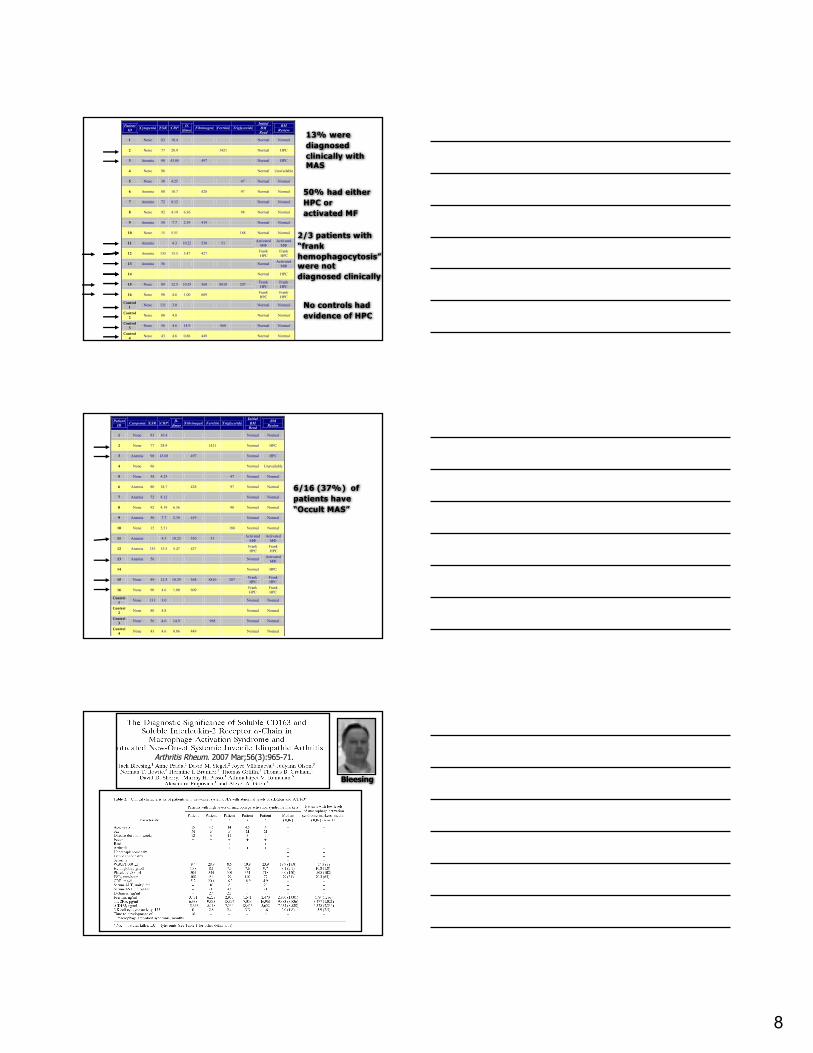
13% were diagnosed clinically with MAS
2/3 patients with “frank hemophagocytosis” were not diagnosed clinically
No controls had evidence of HPC
50% had either HPC or activated MF
6/16 (37%) of patients have “Occult MAS”
Patient ID Cytopenia ESR CRP D-
dimer Fibrinogen Ferritin Triglyceride Initial
BM Read
BM Review
1 None 83 10.4 Normal Normal
2 None 77 28.9 1421 Normal HPC
3 Anemia 98 43.08 497 Normal HPC
4 None 96 Normal Unavailable
5 None 38 4.25 47 Normal Normal
6 Anemia 80 18.7 428 97 Normal Normal
7 Anemia 72 8.12 Normal Normal
8 None 92 4.19 6.36 98 Normal Normal
9 Anemia 50 7.7 2.39 419 Normal Normal
10 None 15 5.51 188 Normal Normal
11 Anemia 4.3 10.22 530 51 Activated MФ
Activated MФ
12 Anemia 135 15.5 5.47 427 Frank HPC
Frank HPC
13 Anemia 56 Normal Activated MФ
14 Normal HPC
15 None 89 12.5 10.29 568 8810 207 Frank HPC
Frank HPC
16 None 90 4.6 1.00 609 Frank HPC
Frank HPC
Control 1 None 131 3.0 Normal Normal
Control 2 None 80 4.8 Normal Normal
Control 3 None 56 4.6 14.9 968 Normal Normal
Control 4 None 43 4.6 0.86 449 Normal Normal
Bleesing
Arthritis Rheum. 2007 Mar;56(3):965-71.

9
ConceptofOccultMASinsJIA• BehrensEM,etal. JRheumatol.2007;34:1133-8.
– 37%haveoccultMASbybonemarrowexam
• BlessingJ,etal. ArthritisRheum.2007;56:965-71.
– 31%haveoccultMASbysCD25andsCD163
– 2/5developedfulminantMAS
Grom
IL-18 >47,750 pg/ml > MASGreen = MAS
Not active
Shimizu
Clin Immunol. 2015 Oct;160(2):277-81.
arthritis
MAS

10
MASDiagnosticGuidelinesforsJIA
Ravelli A, et al. J Pediatr. 2005;146:598-604.
Ravelli
HLH vs. MAS criteria• Primary HLH• Fever• Splenomegaly• Peripheral cytopenia (2 or more
lineages)– Hgb < 10.0 g/dl (<9.0 in <4 wks of age)– Platelets <100E9/L– Neutrophils <1.0E9/L
• Hypertriglyceridemia or hypofibrinogenemia– Triglycerides >265 mg/dL– Fibrinogen <150 mg/dL
• Hemophagocytosis– Bone marrow, spleen, LN, CSF
• Low or absent NK cell activity• Ferritin >500 mg/L• Soluble CD25 >2,400 U/ml
• HLH = 5 or more criteria OR molecular diagnosis c/w HLH
• (Pediatr Blood Cancer. 2007;48:124-31.)
• sJIA MAS• Labs
– Platelets < 262E9/L– AST > 59 U/L– WBC < 4.0E9/L– Fibrinogen < 2.5 g/L
• Clinical– CNS dysfunction (irritable, seizure,
coma, lethargy, disorientation)– Hemorrhages (purpura, easy
bruising, mucosal bleeding)– Hepatomegaly (>3 cm below costal
arch)
• MAS = ≥2 lab OR 2 or 3 clinical and/or lab (bone marrow showing hemophagocytosis only when in doubt)
• (J Pediatr. 2005;146:598-604.)
11
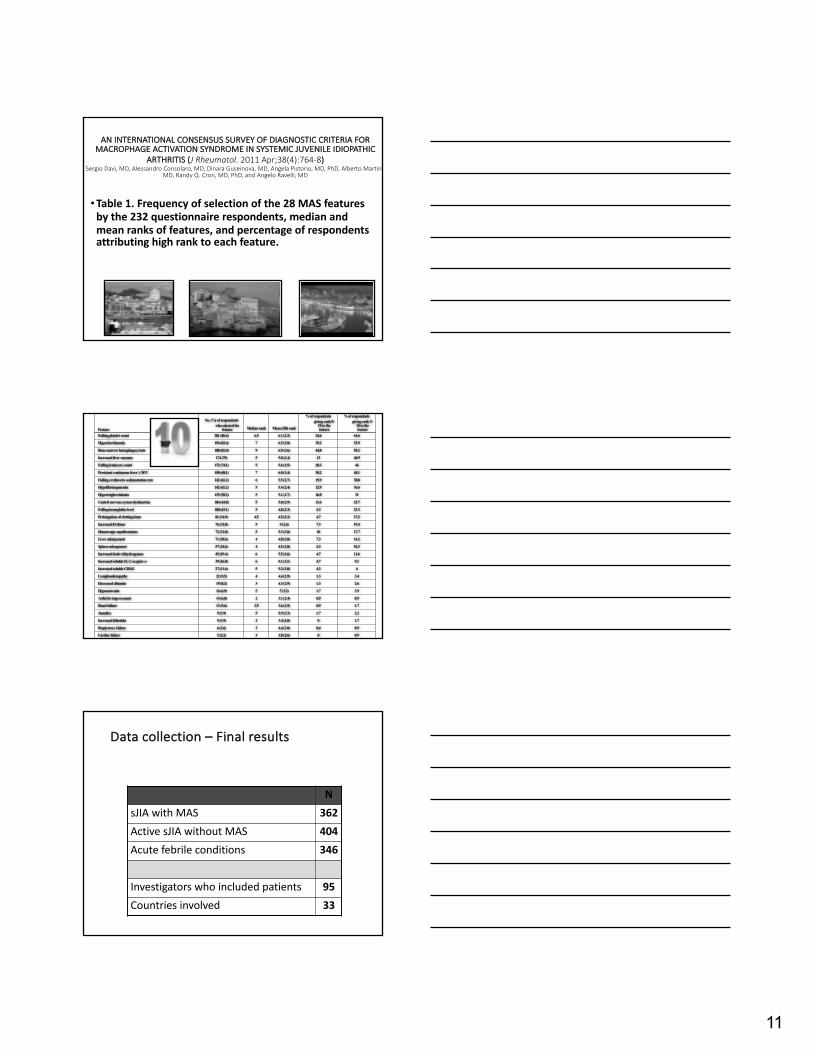
ANINTERNATIONALCONSENSUSSURVEYOFDIAGNOSTICCRITERIAFORMACROPHAGEACTIVATIONSYNDROMEINSYSTEMICJUVENILEIDIOPATHIC
ARTHRITIS(JRheumatol.2011Apr;38(4):764-8)SergioDavì,MD,AlessandroConsolaro,MD,DinaraGuseinova,MD,AngelaPistorio,MD,PhD,AlbertoMartini,
MD,RandyQ.Cron,MD,PhD,andAngeloRavelli,MD
•Table1.Frequencyofselectionofthe28MASfeaturesbythe232questionnairerespondents,medianandmeanranksoffeatures,andpercentageofrespondentsattributinghighranktoeachfeature.
Feature
No. (%) of respondents who selected the
feature Median rank Mean (SD) rank
% of respondents giving rank 8-
10 to the feature
% of respondents giving rank 5-
10 to the feature
Falling platelet count 201 (86.6) 6.5 6.1 (2.3) 24.6 61.6
Hyperferritinemia 194 (83.6) 7 6.5 (3.0) 39.2 53.9
Bone marrow hemophagocytosis 188 (81.0) 9 6.9 (3.6) 44.8 55.2
Increased liver enzymes 174 (75) 5 5.0 (2.4) 13 40.9
Falling leukocyte count 172 (74.1) 5 5.6 (2.5) 20.3 46
Persistent continuous fever ≥ 38°C 158 (68.1) 7 6.0 (3.4) 30.2 40.1
Falling erythrocite sedimentation rate 142 (61.2) 6 5.5 (2.7) 15.9 38.8
Hypofibrinogenemia 142 (61.2) 5 5.4 (2.4) 12.9 36.6
Hypertrigliceridemia 135 (58.2) 5 5.1 (2.7) 16.8 31
Central nervous system dysfunction 104 (44.8) 5 5.0 (2.9) 11.6 23.7
Falling hemoglobin level 100 (43.1) 5 4.8 (2.3) 4.3 23.3
Prolongation of clotting times 81 (34.9) 4.5 4.5 (2.3) 4.7 17.2
Increased D-dimer 76 (32.8) 5 5 (2.6) 7.3 19.4
Hemorragic manifestations 72 (31.0) 5 5.3 (3.0) 10 17.7
Liver enlargement 71 (30.6) 4 4.8 (2.8) 7.3 14.2
Spleen enlargement 57 (24.6) 4 4.5 (2.8) 4.3 10.3
Increased lactic dehydrogenase 45 (19.4) 6 5.5 (2.6) 4.7 11.6
Increased soluble IL-2 receptor α 39 (16.8) 6 5.1 (3.1) 4.7 9.1
Increased soluble CD163 27 (11.6) 5 5.2 (3.0) 4.3 6
Lymphoadenopathy 22 (9.5) 4 4.4 (2.9) 1.3 3.4
Decreased albumin 19 (8.2) 3 4.3 (2.9) 1.3 2.6
Hyponatremia 16 (6.9) 5 5 (3.2) 1.7 3.9
Arthritis improvement 14 (6.0) 2 3.1 (2.4) 0.9 0.9
Renal failure 13 (5.6) 2.5 3.6 (2.9) 0.9 1.7
Jaundice 9 (3.9) 5 5.9 (3.3) 1.7 2.2
Increased bilirubin 9 (3.9) 2 3.4 (2.0) 0 1.7
Respiratory failure 6 (2.6) 3 4.4 (3.0) 0.4 0.9
Cardiac failure 5 (2.2) 3 3.8 (2.6) 0 0.9
Datacollection– Finalresults
NsJIAwithMAS 362ActivesJIAwithoutMAS 404Acutefebrileconditions 346
Investigatorswhoincludedpatients 95Countriesinvolved 33

12
Clinical,laboratoryandhistopathologic characteristics,currenttreatmentandoutcomeofmacrophageactivationsyndromecomplicatingsystemicjuvenile
idiopathicarthritis:amultinational,multicenterstudyof362patients
No of available data N (%)
Fever 355 341 (96.1)
Hepatomegaly 350 245 (70)Splenomegaly 347 201 (57.9)Lymphadenopathy 346 178 (51.4)
Active arthritis 354 230 (65)CNS involvement
Lethargy SeizuresIrritabilityConfusionHeadacheMood changesComaOther
349 122 (35)35 (10)32 (9.1)17 (4.9)13 (3.7)11 (3.1)
7 (2)6 (1.7)30 (8.6)
Heart involvementPericarditisPericardial effusionArrhythmiaHeart failureCardiomegalyOther
353 90 (25.5)31 (8.8)26 (7.3)5 (1.4)4 (1.1)4 (1.1)20 (5.6)
Minoia F, Davi S, Horne A, et al. Arthritis Rheumatol. 2014;66(11):3160-9.
Horne, Minoia, Davi
Minoia F, et al. J Rheumatol. 2015;42:994-1001.
InternationalconsensusconferenceonMASclassificationcriteria
Villa Quartara della Castagna, Genoa, Italy, 21-22 March 2014

13
Finaldefinition(>80%consensus)– selectedfrom982computermodeled
Afebrile patientwithknownorsuspectedsJIAis classified as havingMASif thepatient has:
Ferritin>684ng/L
ANDatleast2ofthefollowing4laboratoryvariables:
• Platelets≤181x109/mL• AST>48U/L• Triglycerides>156mg/dL• Fibrinogen≤360mg/mL
Ravelli A, et al. Arthritis Rheumatol. 2016;68:566-76.Ravelli A, et al. Annals Rheum Dis. 2016;75:481-9.
Conference Participants
Horne

14
1
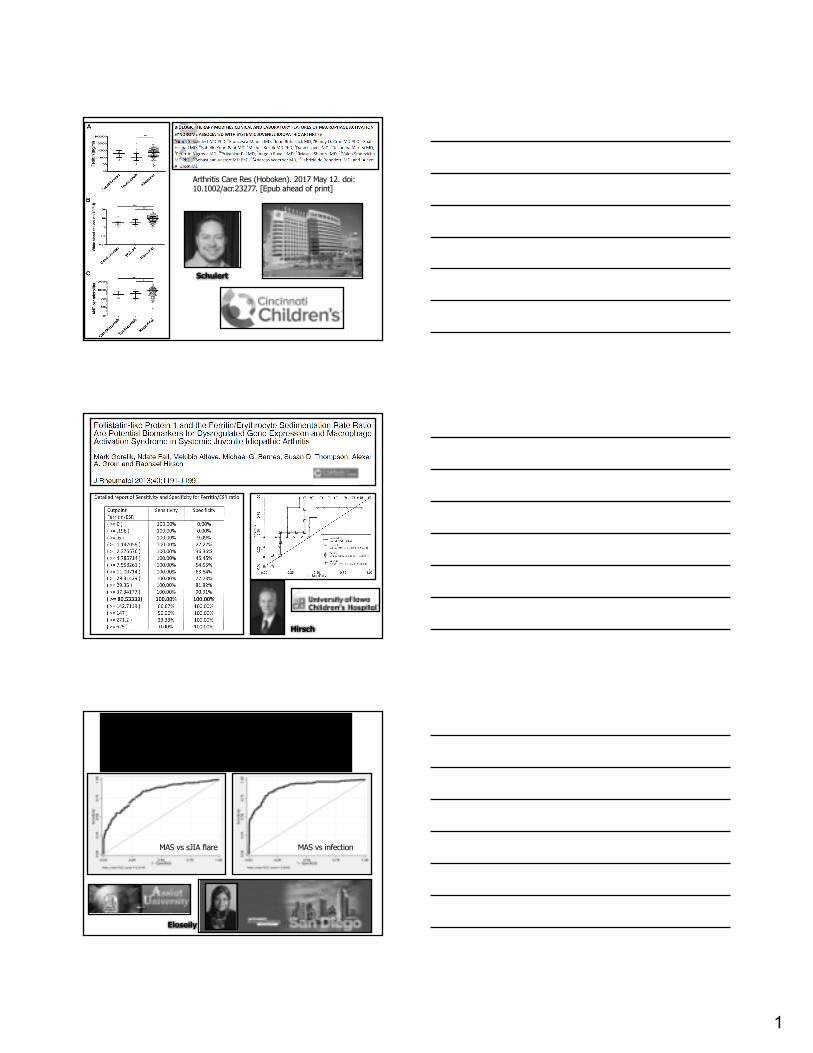
Arthritis Care Res (Hoboken). 2017 May 12. doi: 10.1002/acr.23277. [Epub ahead of print]
Schulert
Hirsch
The ferritin to ESR ratio is a simple measure to distinguish macrophage activation syndrome from systemic arthritis flare
Eloseily, E.M.A., Minoia, F., Beukelman, T., Ravelli, A., and Cron, R.Q(upcoming talk at the American College of Rheumatology Annual
Scientific Meeting, San Diego, CA, November 6, 2017)
MAS vs sJIA flare MAS vs infection
Eloseily

2
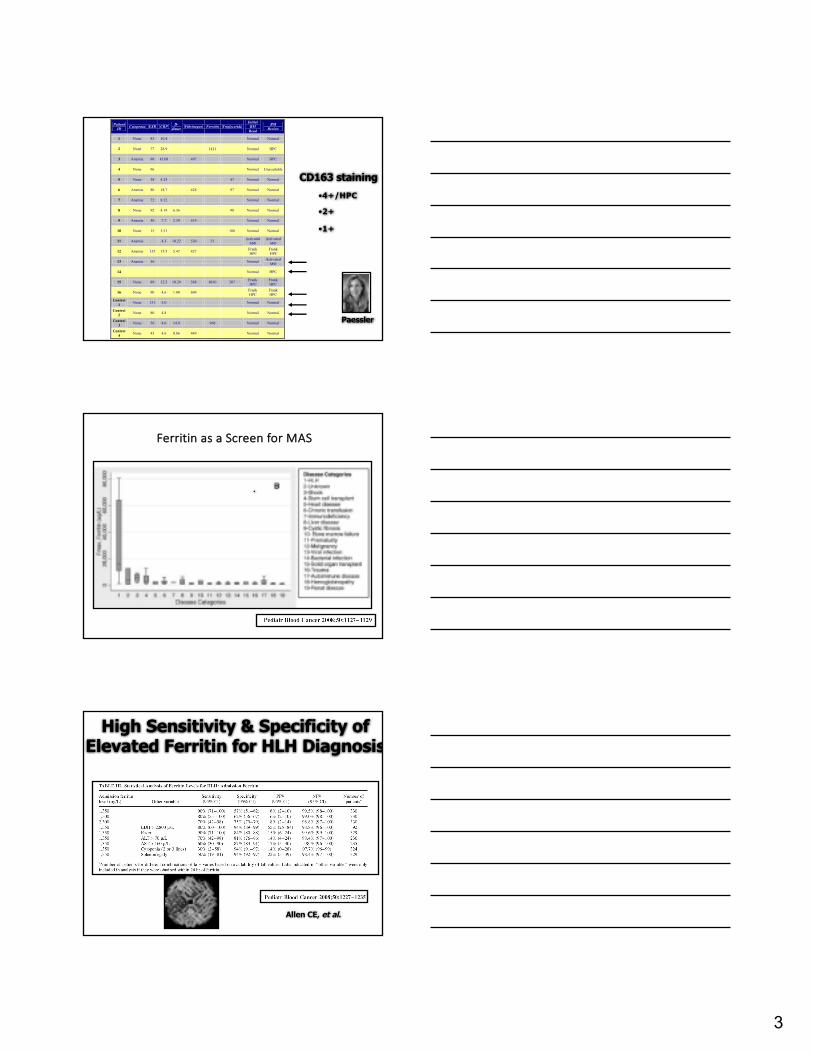
CD163Haptoglobinreceptor
•MorespecificmarkerforMF thanCD68•Abletohighlight“overstuffed”MF thatmightbemissedonroutinestaining
3/4 = dead
Unknown MAS
Mono. Leishmania
?? CMV
EBV
CD163higherpowerimages
Initial read - Frank HPC Initial read - NormalInitial read - NormalClinical dx of MAS
Normal
Behrens E, Beukelman T, Paessler M, Cron RQ.
J Rheumatol. 2007;34:1133-8.
3
Patient ID Cytopenia ESR CRP D-
dimer Fibrinogen Ferritin Triglyceride Initial
BM Read
BM Review
1 None 83 10.4 Normal Normal
2 None 77 28.9 1421 Normal HPC
3 Anemia 98 43.08 497 Normal HPC
4 None 96 Normal Unavailable
5 None 38 4.25 47 Normal Normal
6 Anemia 80 18.7 428 97 Normal Normal
7 Anemia 72 8.12 Normal Normal
8 None 92 4.19 6.36 98 Normal Normal
9 Anemia 50 7.7 2.39 419 Normal Normal
10 None 15 5.51 188 Normal Normal
11 Anemia 4.3 10.22 530 51 Activated MФ
Activated MФ
12 Anemia 135 15.5 5.47 427 Frank HPC
Frank HPC
13 Anemia 56 Normal Activated MФ
14 Normal HPC
15 None 89 12.5 10.29 568 8810 207 Frank HPC
Frank HPC
16 None 90 4.6 1.00 609 Frank HPC
Frank HPC
Control 1 None 131 3.0 Normal Normal
Control 2 None 80 4.8 Normal Normal
Control 3 None 56 4.6 14.9 968 Normal Normal
Control 4 None 43 4.6 0.86 449 Normal Normal
CD163 staining•4+/HPC
•2+
•1+
Paessler
FerritinasaScreenforMAS
.
High Sensitivity & Specificity of Elevated Ferritin for HLH Diagnosis
Allen CE, et al.
4
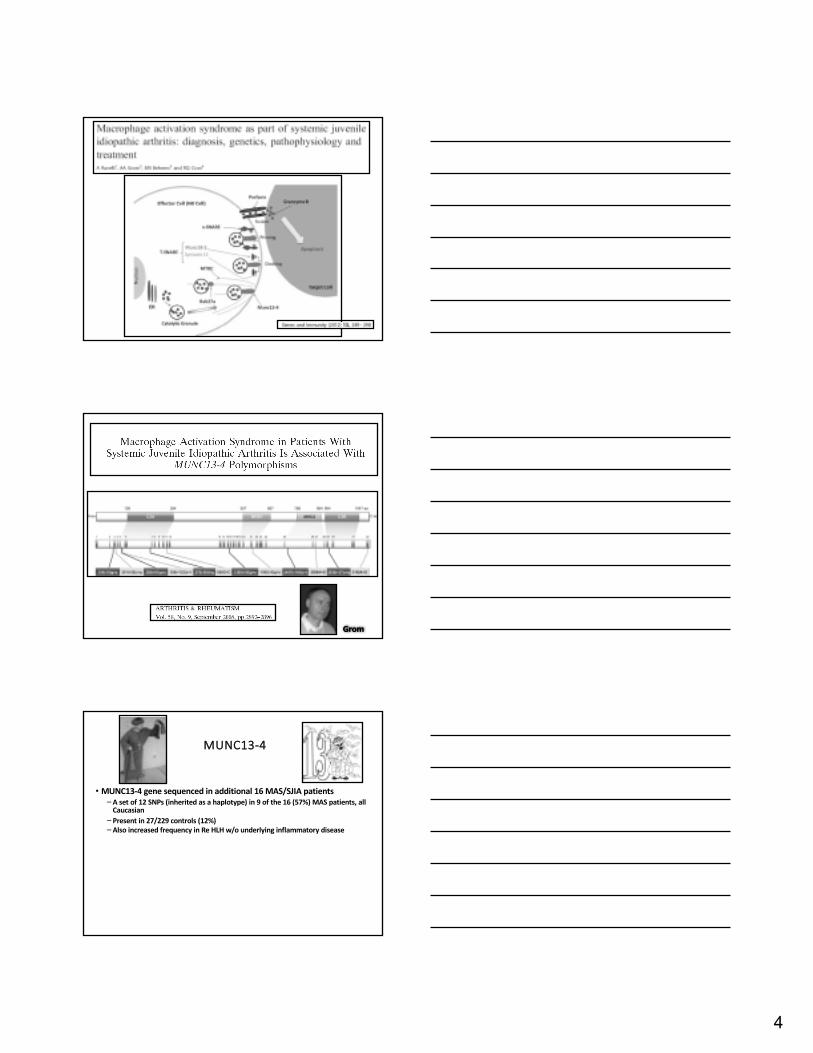
Grom
MUNC13-4
• MUNC13-4genesequencedinadditional16MAS/SJIApatients–Asetof12SNPs(inheritedasahaplotype)in9ofthe16(57%)MASpatients,allCaucasian
– Presentin27/229controls(12%)–AlsoincreasedfrequencyinReHLHw/ounderlyinginflammatorydisease
5
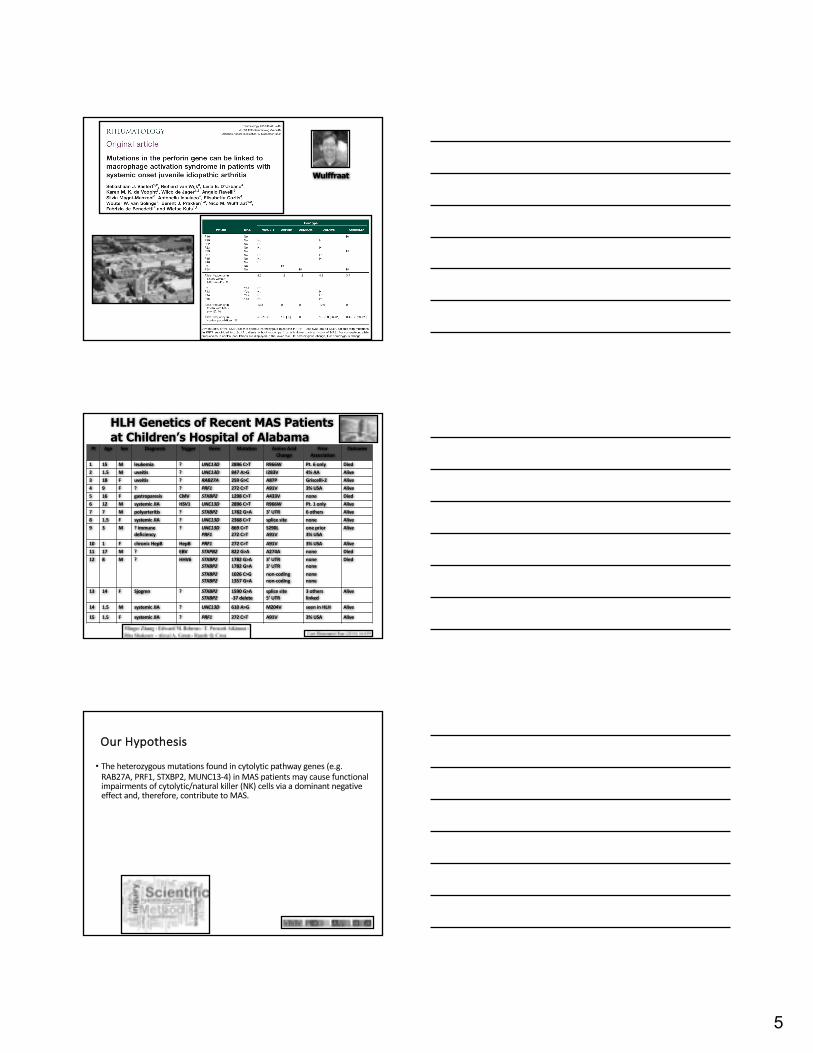
Wulffraat
Pt Age Sex Diagnosis Trigger Gene Mutation AminoAcidChange
PriorAssociation
Outcome
1 15 M leukemia ? UNC13D 2896C>T R966W Pt.6only Died2 1.5 M uveitis ? UNC13D 847A>G I283V 4%AA Alive3 18 F uveitis ? RAB27A 259G>C A87P Griscelli-2 Alive4 9 F ? ? PRF1 272C>T A91V 3%USA Alive5 16 F gastroparesis CMV STXBP2 1298C>T A433V none Died6 12 M systemicJIA HSV1 UNC13D 2896C>T R966W Pt.1only Alive7 7 M polyarteritis ? STXBP2 1782G>A 3’UTR 6others Alive8 1.5 F systemicJIA ? UNC13D 2368C>T splicesite none Alive9 3 M ?immune
deficiency? UNC13D
PRF1869C>T272C>T
S290LA91V
oneprior3%USA
Alive
10 1 F chronicHepB HepB PRF1 272C>T A91V 3%USA Alive11 17 M ? EBV STXPB2 822G>A A274A none Died12 8 M ? HHV6 STXBP2
STXBP2STXBP2STXBP2
1782G>A1782G>A1026C>G1357G>A
3’UTR3’UTRnon-codingnon-coding
nonenonenonenone
Died
13 14 F Sjogren ? STXBP2STXBP2
1590G>A-37delete
splicesite5’UTR
3otherslinked
Alive
14 1.5 M systemicJIA ? UNC13D 610A>G M204V seeninHLH Alive
15 1.5 F systemicJIA ? PRF1 272C>T A91V 3%USA Alive
HLH Genetics of Recent MAS Patients at Children’s Hospital of Alabama
OurHypothesis
• Theheterozygousmutationsfoundincytolytic pathwaygenes(e.g.RAB27A,PRF1,STXBP2,MUNC13-4)inMASpatientsmaycausefunctionalimpairmentsofcytolytic/naturalkiller(NK)cellsviaadominantnegativeeffectand,therefore,contributetoMAS.

6
Approach
1. Make cDNA by reverse transcription from the human NK-92 cell line total RNA;
2. Generate patient mutation by site-directed mutagenesis of wild-type cDNA;
3. Generate lentiviral expression vectors;
4. Transduce human NK-92 cell line to express wild-type and mutant genes;
5. Measure transduced NK cell functions: cytolysis of K562 (NK target cell), CD107a mobilization/cell surface expression, IFNgexpression, granzyme B polarization during immunologic/cytolytic synapse formation (by confocal microscopy), & interaction with other cytolytic pathway proteins by PLA and co-immunoprecipitation.
Zhang Funded by Kaul Pediatric Research Institute
(STXBP2)
7
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
1.11
66.5
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
12.3MFI = 2994
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
2.21
51.8
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
18MFI = 2797
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
4.17
33.9
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
23.2MFI = 2651
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
7.1
18.4
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
26.8MFI = 2625
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
1.56
48.4
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
28.4MFI = 2489
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
2.14
45
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
28MFI = 2527
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
4.81
27.8
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>31.9
MFI = 2524
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<GFP
-A>
9.08
15
0 102 103 104 105<eFLUOR450-A>
0102
103
104
105
<7AA
D-A
>
35.1MFI = 2629
STXBP2 mSTXBP2
0.5:1
1:1
2:1
4:1
E:T
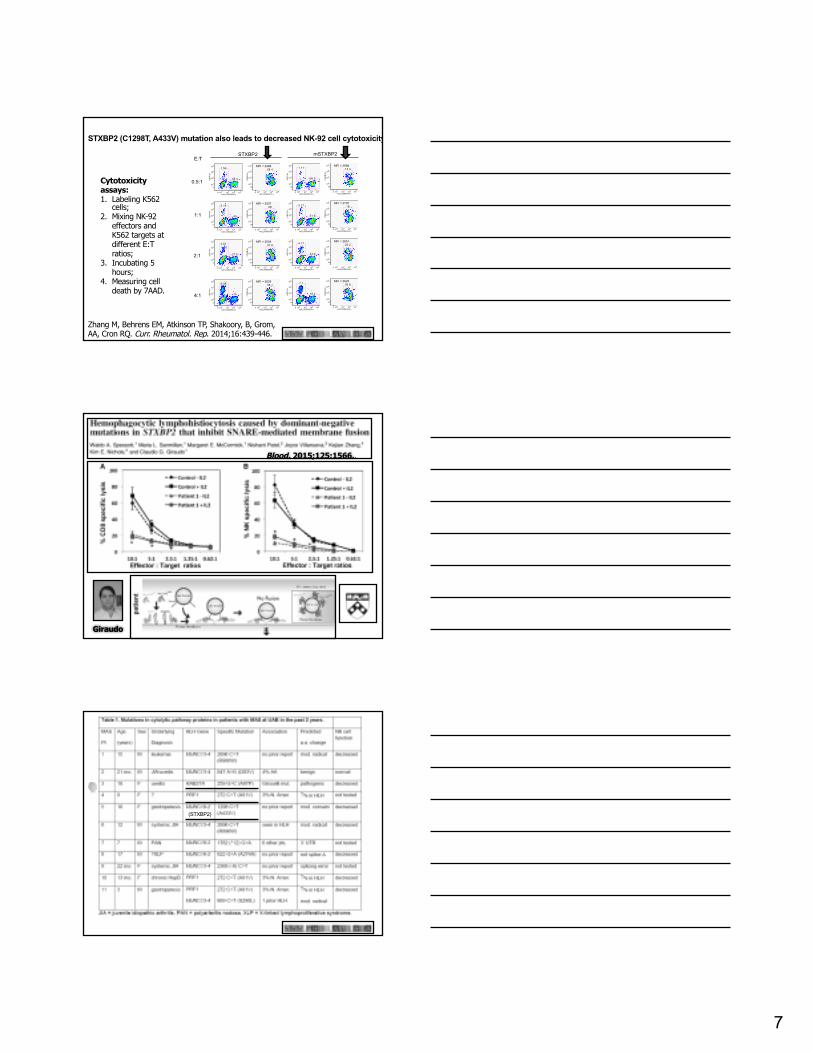
STXBP2 (C1298T, A433V) mutation also leads to decreased NK-92 cell cytotoxicity
Zhang M, Behrens EM, Atkinson TP, Shakoory, B, Grom, AA, Cron RQ. Curr. Rheumatol. Rep. 2014;16:439-446.
Cytotoxicity assays: 1. Labeling K562
cells;2. Mixing NK-92
effectors and K562 targets at different E:T ratios;
3. Incubating 5 hours;
4. Measuring cell death by 7AAD.
Blood. 2015;125:1566..
Giraudo
(STXBP2)

8
MASPatientPresentation•18-year-oldwhitefemalepresentedwith2weeksoffever (>102oF)andabdominalpain.•Examrevealedfebrile,semi-coherentfemalewithhepatosplenomegaly.• Labfindingsincluded:pancytopenia,severehepatitis,coagulopathy,ferritin8,446ng/ml,triglycerides,sCD25,sCD163,CD163stainingofbonemarrow,¯¯NKcellfunction,andESRof10mm/hr.
ResponsetoImmunosuppression
•Rxwithcyclosporin,•highdosecorticosteroids•andanakinra.
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503.
Rab27aA87PmutationdecreasesNKcelllyticactivity,whichisexacerbatedinthe
presenceofIL-6
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503.
9
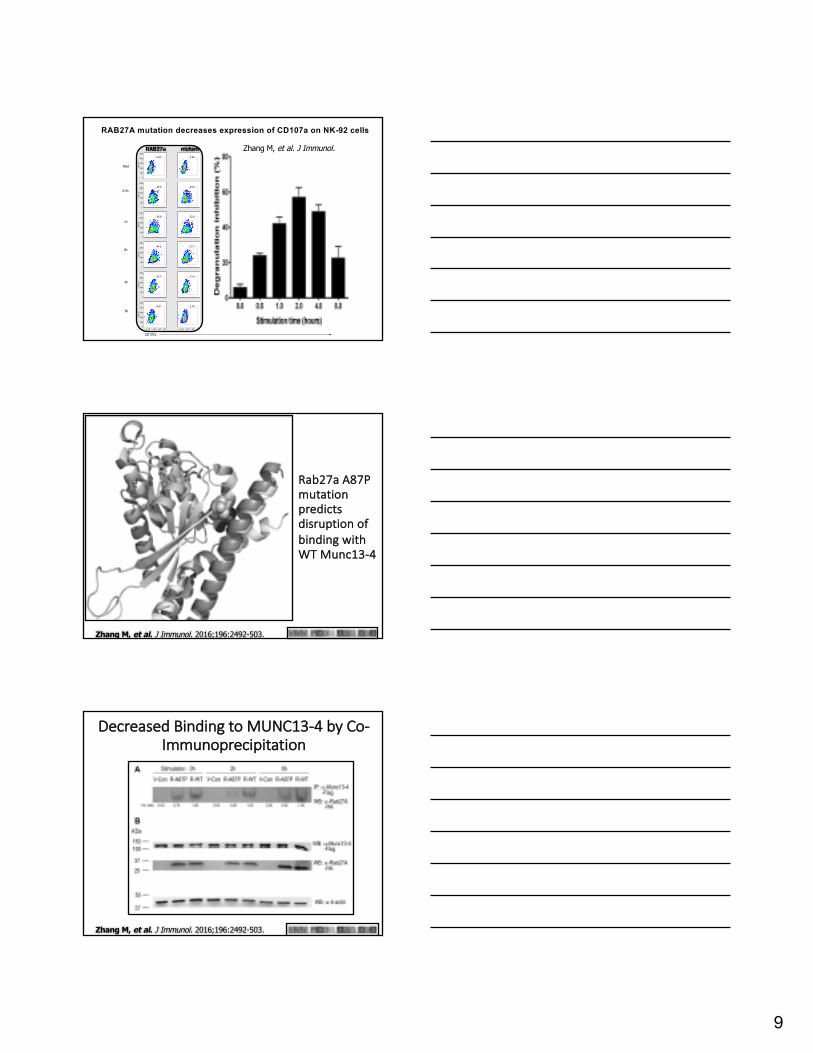
RAB27A mutation decreases expression of CD107a on NK-92 cells
0
50K
100K
150K
200K
250K
SS
C-A
0.67
0
50K
100K
150K
200K
250K
SS
C-A
26.9
0
50K
100K
150K
200K
250K
SS
C-A
39.9
0
50K
100K
150K
200K
250K
SS
C-A
44.2
0
50K
100K
150K
200K
250K
SS
C-A
22.7
0 102 103 104 1050
50K
100K
150K
200K
250K
SS
C-A
4.81
0.83
23.6
32.6
31.7
13.4
0 102 103 104 105
2.79
0.75
22.3
27.2
21.4
9.6
0 102 103 104 105
1.67
0.61
23.4
32
24.2
8.97
0 102 103 104 105
1.58
0.83
22.9
27.8
18.9
6.88
0 102 103 104 105
1.1
0.68
20.6
28.2
19.9
6.52
0 102 103 104 105
1.18
CD107a
Med
0.5h
1h
2h
4h
8h
RAB27A mRAB27A PRF1 mPRF1 STXBP2 mSTXBP2RAB27a mutant Zhang M, et al. J Immunol.
Rab27aA87PmutationpredictsdisruptionofbindingwithWTMunc13-4
Zhang M, et al. J Immunol. 2016;196:2492-503..
DecreasedBindingtoMUNC13-4byCo-Immunoprecipitation
Zhang M, et al. J Immunol. 2016;196:2492-503..
10
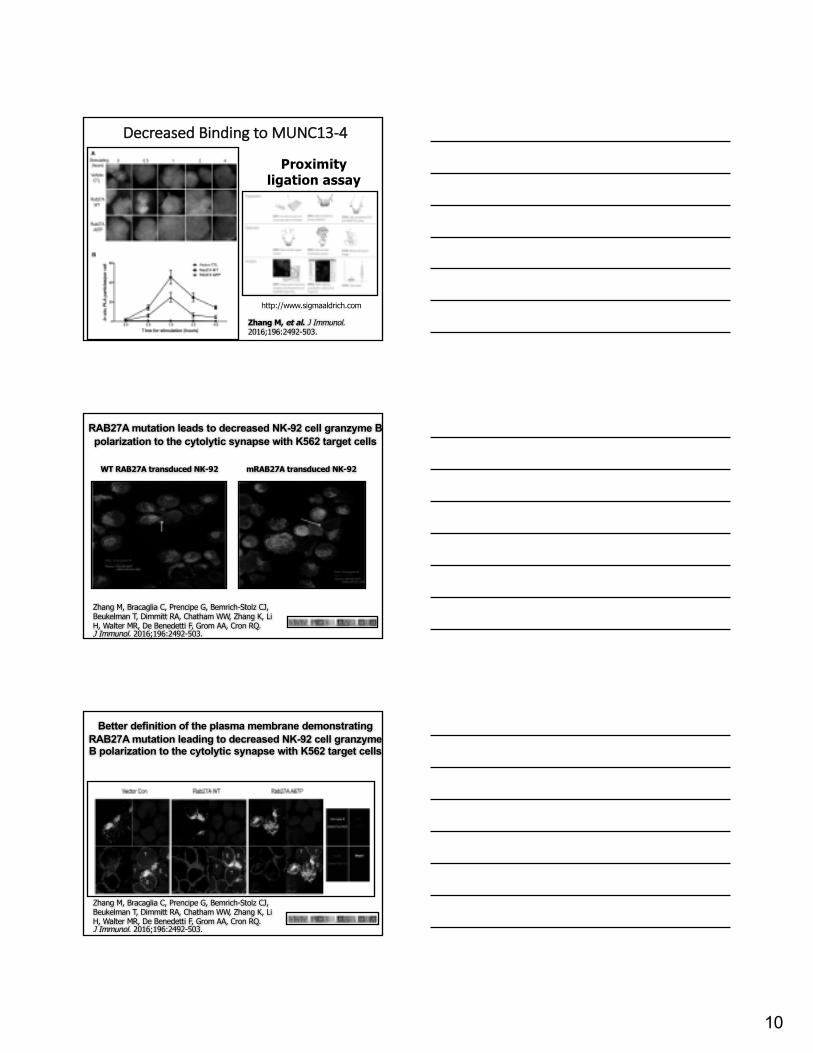
DecreasedBindingtoMUNC13-4
http://www.sigmaaldrich.com
Proximity ligation assay
Zhang M, et al. J Immunol. 2016;196:2492-503..
RAB27A mutation leads to decreased NK-92 cell granzyme B polarization to the cytolytic synapse with K562 target cells
WT RAB27A transduced NK-92 mRAB27A transduced NK-92
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503..
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503..
Better definition of the plasma membrane demonstrating RAB27A mutation leading to decreased NK-92 cell granzymeB polarization to the cytolytic synapse with K562 target cells

11
DelayedPolarizationofCytolytic Granules
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503..
DelayedPolarizationofCytolytic GranulesTimeCourse
Zhang M, et al. J Immunol. 2016;196:2492-503..
J Exp Med. 2015;212:307 Jenkins
QVD inhibits caspases required for target cell death
Increased synapse dwell time results in cytokine production

12
IncreasedIFNg ExpressionbyRab27aA87PMutantNKCells
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503..
Rab27aA87PinanotherpatientdecreasesNKcelldegranulation&cytolytic activity
Zhang M, Bracaglia C, Prencipe G, Bemrich-Stolz CJ, Beukelman T, Dimmitt RA, Chatham WW, Zhang K, Li H, Walter MR, De Benedetti F, Grom AA, Cron RQ.J Immunol. 2016;196:2492-503..
Conclusion
• Theheterozygous(A87P)RAB27AmutationlikelycontributestodecreasedNKcellactivityandsubsequentclinicalMASinthepatientsbearingthemutationviaapartialdominantnegativeeffect.
13
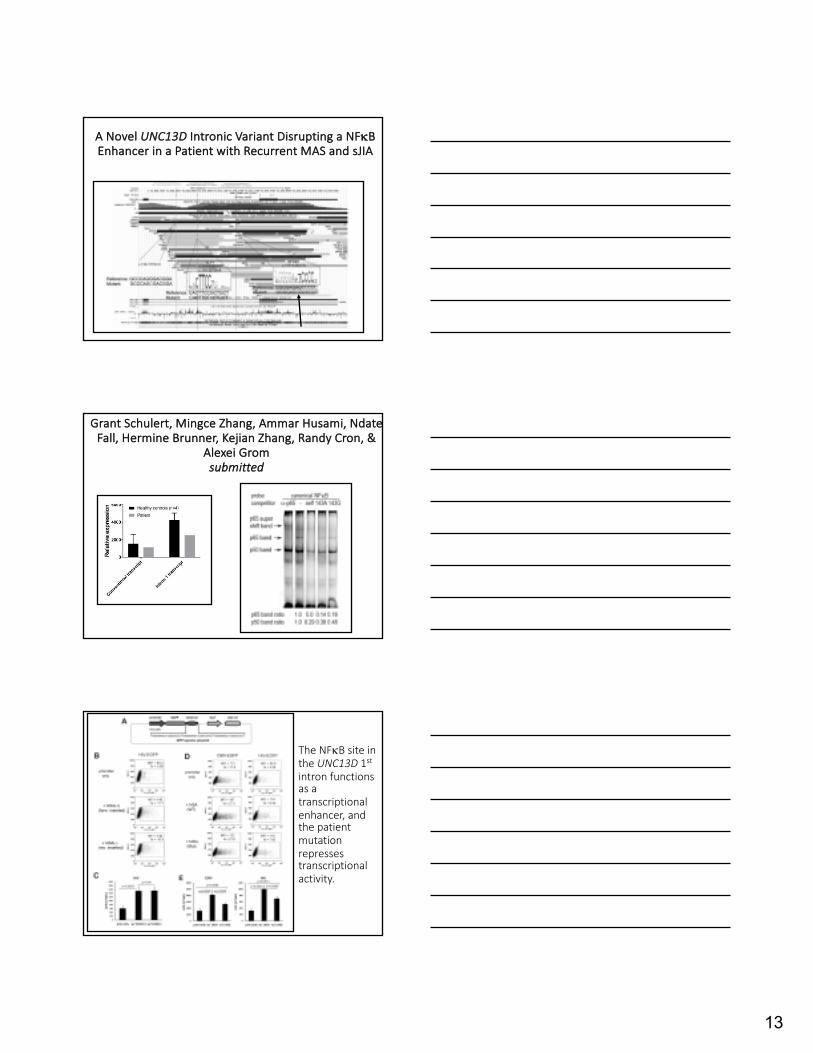
ANovelUNC13D Intronic VariantDisruptingaNFkBEnhancerinaPatientwithRecurrentMASandsJIA
GrantSchulert,MingceZhang,AmmarHusami,NdateFall,HermineBrunner,KejianZhang,RandyCron,&
AlexeiGromsubmitted
TheNFkBsiteintheUNC13D 1stintronfunctionsasatranscriptionalenhancer,andthepatientmutationrepressestranscriptionalactivity.

14
De Benedetti

1
Extentoftheproblem?
HLH/MAS
MODSSIRSCulture negativesepsis
Fever & ferritin
Carcillo
Harms
GenesAssociatedwithHLH/MAS
Cron RQ, et al. Expert Rev Clin Immunol. 2015;11:1043-53.

2
Sample Gene Variant Identifier Variant type
PredictionSIFT/Polyphen
1000 Genomes MAF
ExAC MAF
Conservation (phyloP)
7,11
PRF1 c.272C>T(p.A91V) rs35947132 Missense Damaging/Probably damaging
0.013 0.031 3.6
4 LYST c.8913T>G(p.N2971K) rs34702903 Missense Tolerated/Possibly damaging
0.0006 0.002 0.77
1,11,14
LYST c.5945C>T(p.T1982I) rs146591126 Missense Tolerated/Benign 0.0016 0.006 3.03
7 LYST c.11086G>A(p.V3696I) rs147221131 Missense Tolerated/Benign 0.0002 0.0008 2.87
Two have PRF1 A91V mutations and 5 have LYSTmutations of the 14 analyzed (36%). Schulert
Schulert G, et al. J Infect Dis. 2016;213:1180-8.
PRF1(C272T,A91V)mutationalsodecreasesNK-92cellcytotoxicity
Schulert G, et al. J Infect Dis. 2016;213:1180-8.
3
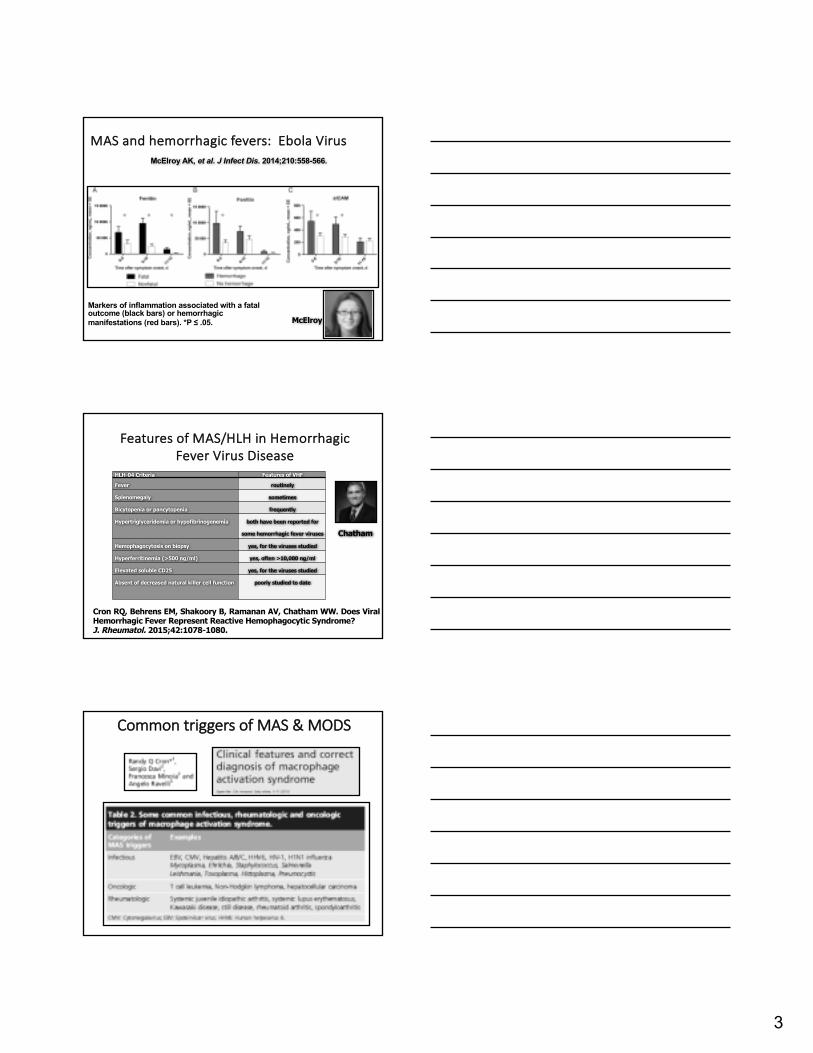
MASandhemorrhagicfevers:EbolaVirus
Markers of inflammation associated with a fatal outcome (black bars) or hemorrhagic manifestations (red bars). *P ≤ .05.
McElroy AK, et al. J Infect Dis. 2014;210:558-566.
McElroy
FeaturesofMAS/HLHinHemorrhagicFeverVirusDisease
Cron RQ, Behrens EM, Shakoory B, Ramanan AV, Chatham WW. Does ViralHemorrhagic Fever Represent Reactive Hemophagocytic Syndrome?J. Rheumatol. 2015;42:1078-1080.
HLH-04 Criteria Features of VHF
Fever routinely
Splenomegaly sometimes
Bicytopenia or pancytopenia frequently
Hypertriglyceridemia or hypofibrinogenemia both have been reported for
some hemorrhagic fever viruses
Hemophagocytosis on biopsy yes, for the viruses studied
Hyperferritinemia (>500 ng/ml) yes, often >10,000 ng/ml
Elevated soluble CD25 yes, for the viruses studied
Absent of decreased natural killer cell function poorly studied to date
Chatham
CommontriggersofMAS&MODS
4
High Prevalence of MODSin the PICU
Pediatric MODS has a High Mortality Rate
MASRxOutline
• Highdosecorticosteroids• Cyclosporin A• Cyclophosphamide• ReviewofHLH-94&HLH-2004• Plasmaexchange• Biologictherapies:
–IVIg–ATG–Anti-CD20–TNFinhibition–IL-1antagonism–IL-6RmAb–Others

5
PulseSolumedrolRxforMAS
• Hadchouel M,Prieur AM,Griscelli C. Acutehemorrhagic,hepatic,andneurologicmanifestationsinjuvenilerheumatoidarthritis:possiblerelationshiptodrugsorinfection.JPediatr.1985;106:561-6.
• Syndromeofhemorrhagic,neurologic,hepatic,hematologic,andmetabolicmanifestations– distinctfromReyesyndrome.
• FallingESRandplateletcountandfibrinogenlevels
• 7JIA(6systemic)childrentreatedwithhighdosesteroids
• 2deaths
“Any sufficiently advanced technology is indistinguishable from magic.” - Arthur C. Clarke
24 patients with MAS (18 sJIA, 2 poly JIA, 2 SLE, 2 unclassified)High spiking fevers: 24 Hepatosplenomegaly: 14Hemorrhagic diathesis: 6 Pulmonary involvement: 12
Neurologic involvement (coma or seizures): 12 HLH on bone marrow: 14/17
Treatment (29 episodes) – 2 fatalitiesIVIg failed in 4/4 pulse steroids 1st line rx success: 15/21CsA was rapidly effective all who failed steroids and in 5 patients as 1st line rx
CyclosporinAtoTreatMASinJIA
Stéphan JL,etal. Rheumatology(Oxford).2001;40:1285-92.
Prieur
HLH-2004Protocol

6
“Success”ofHLH-94[VP-16,CsA,Dexamethasone,BMT]
Blood. 2002;100:2367-73.
Henter
IVIgforMAS
•MaybebetterforinfectionassociatedMAS–HotA,MadouxMH,Viard JP,Coppéré B,Ninet J. Successfultreatmentofcytomegalovirus-associatedhemophagocytic syndromebyintravenousimmunoglobulins.AmJHematol.2008;83:159-62.[CMV]
–AsciG,Toz H,OzkahyaM,Cagirgan S,Duman S,Sezis S,OkE. High-doseimmunoglobulintherapyinrenaltransplantrecipientswithhemophagocytichistiocyticsyndrome.JNephrol.2006;19:322-6.[multipledifferentinfections]
– Larroche C,Bruneel F,AndréMH,Bader-Meunier B,Baruchel A,Tribout B,Genereau T,Zunic P;Comité d'Evaluation etdeDiffusiondesInnovationTechnologiques (CEDIT).[Intravenouslyadministeredgamma-globulinsinreactivehemaphagocytic syndrome.Multicenterstudytoassesstheirimportance,bytheimmunoglobulinsgroupofexpertsofCEDIToftheAP-HP]AnnMedInterne(Paris). 2000;151:533-539.[variousviralinfections]
– ChenRL,LinKH,LinDT,SuIJ,HuangLM,LeePI,Hseih KH,LinKS,LeeCY.Immunomodulationtreatmentforchildhoodvirus-associatedhaemophagocyticlymphohistiocytosis.BrJHaematol.1995;89:282-90.[EBVandHHV-6]
Anti-thymocyteGlobulinforMAS
Fischer

7
PlasmaExchangeforMAS
Anti-CD20forMAS
Sano T, Sakai H, Takimoto K, Ohno H.Rituximab alone was effective for the treatment of a diffuse large B-cell lymphoma associated with hemophagocytic syndrome. IntJ Clin Oncol. 2007;12:59-62.
Balamuth NJ, Nichols KE, Paessler M, Teachey DT.Use of rituximab in conjunction with immunosuppressive chemotherapy as a novel therapy for Epstein Barr virus-associated hemophagocytic lymphohistiocytosis. J PediatrHematol Oncol. 2007;29:569-73.
Nichols
ProposedPathophysiologyofMAS
Jordan Behrens

8
TNFinhibition&MAS
• CASEREPORTS
•MASfollowingetanercept therapy:– JRheumatol.2007;34:241-2– JClin Rheumatol.2001;7:252-6.– JRheumatol.2003;30:401-3.
•MASresolvedbyetanercept therapy:– Pediatr BloodCancer.2008;50:419-21.–ModRheumatol.2008;18:72-5.–AmJHematol.2006;81:59-61.[infliximab]– JRheumatol.2001;28:2120-4.– SwissMedWkly.2002;132:414-22. Prahalad
Successful treatment of severe pediatric rheumatic disease associated macrophage activation syndrome with IL-1 inhibition following conventional immunosuppressive
therapy: case series with 12 patients.
Miettunen PM, Aru N, Jayanthan A, Behrens EM, Cron RQ.Rheumatology (Oxford). 2011 Feb;50(2):417-9.
Miettunen
IL-1ImbalanceinMAS
IL-1b
IL-1b (red) complexed with IL-1Ra
Anakinra (rhIL-1Ra)

9
ProposaltoTreatEbolaHemorrhagicFeverwithIL-1Blockade
Chatham WW, Cron RQ. The Rheumatologist. 8(12):1, 21-23.
Opal Dinarello Shakoory
Crit Care Med. 2016 44:275-81.
Anakinra forMASClinicalTrialatUAB/CoA
• ClinicalTrials.govIdentifier:• NCT02780583
OfficialTitle: RandomizedPlaceboControlledTrialofSubcutaneousrhIL-1Ra(Anakinra)intheManagementofHospitalizedPediatricandAdultPatientsWithMacrophageActivationSyndrome
Chatham

10
First4patientsamplesforWGS
33 yo WM with fevers, pancytopenia, AST/ALT elevations, AKI, very high ferritin (108,000) coagulopathy (d-dimer >20,000). No identified infectious/viral triggers. Screen fail for protocol due to AKI. Probable AOSD. Complete response to pulse steroids, CsA, anakinra--off steroids, off CsA, now on q.o.d. anakinra without relapse.
24 yo AA female with SLE presented with flare of rash, arthritis, altered mental status, pancytopenia, LFT elevations, coagulopathy, very high ferritin. No infectious trigger. Better with pulse steroids, anakinra, brief course of CsA x 2 weeks, Now back on SoC SLE meds, no relapse off CsA/off anakinra.
21 yo AA female arthralgias, malar rash, alopecia and oral ulcers March 2017. Diagnosed SLE(positive ANA, anti-SSA Ab, anti-Smith Ab at that time) and started on pred 60mg, Plaquenil 200mg in addition to levothyroxine for hypothyroidism. As steroids tapered developed headache, fever, aseptic meningitis CSF: (40 WBCs, 61% segs, 39% lymphs/monos, protein 89, glucose 39); blood CSF cultures negative. Despite 80 mg/d Solumedrol, HCQ has ongoing fever, progressive pancytopenia (1.86/24/85k), increased ferritin (2,600), coagulopathy w/ high d-dimer (8557), elevated LDH (841) elevated TG (321), elevated CRP (50).
9 yo AA male with 2 weeks of fever, cervical LN, malar rash, hepatomegaly, and parotitis. Diagnosed with SLE (+ANA, +Sm, +dsDNA, low complements, ferritin 13K) and MAS (pancytopenia, coagulopathy, elevated transaminases, altered mental status). Started on clinical trial. Doing well as an outpatient, currently on mycophenolate mofetil and tapering corticosteroids.
PotentialPathogenicVariants
1. All 4 patients have at least one heterozygous (mostly missense) mutation in a known HLH gene.
2. Still disease patient has a LYST mutation, same mutation as found in 3 patients who died from H1N1 influenza (J Infect Dis. 2016 ;213:1180-8).
3. First adult SLE patient has a STXBP2 mutation, and pediatric SLE patient has AP3B1 mutations.
4. Second adult SLE patient has mutations (mostly missense) in 5 different HLH genes: AP3B1 (same mutations as pediatric patient), LYST, PRF1, STX11, & UNC13D.
5. This same SLE patient also has a rare 1st intronicmutation in UNC13D.
Anakinra forMASTrialPatientMutations
Pt #
Age Sex Diagnosis Trigger Gene Mutation Amino acid change
Freq-uency
Outcome
1 33 M AOSD present LYST 5945 C>T Thr 1982 Ile 0.6% Alive
2 24 F SLE present STXBP2 646 G>A Val 216 Ile 0.4% Alive
3 9 M SLE present AP3B1AP3B1
1038 T>C3023_3025del
Asn 346 AsnAla 1008 del
1.1%18%
Alive
4 21 F SLE EBV AP3B1AP3B1LYSTPRF1STX11UNC13DUNC13D
1038 T>C3023_3025del7793 T>A403 G>A829 A>G904 C>Tc.118-174 C>T
Asn 346 AsnAla 1008 delPhe 2598 TyrVal 135 MetThr 277 AlaLeu 302 Phe1st intron
1.1%18%0.8%0.1%1.1%0.3%?
Alive
mut. likely deleterious

11
PolygenicmutationsinthecytotoxicitypathwayincreasesusceptibilitytodevelopHLHimmunopathologyinmice
SepulvedaFE,etal.Blood.2016;127:2113-21.
AS=Rab27+/- x STX11+/-; AP=Rab27+/- x PRF1+/-; ASP=Rab27+/- x STX11+/- x PRF1+/-
UNC13D(Munc13-4)1st IntronVariants
c.118-174 C>T
9 patients with severe cytokine-release syndrome benefited from anti-IL-6R monoclonal antibody therapy. N=30
Grupp
12
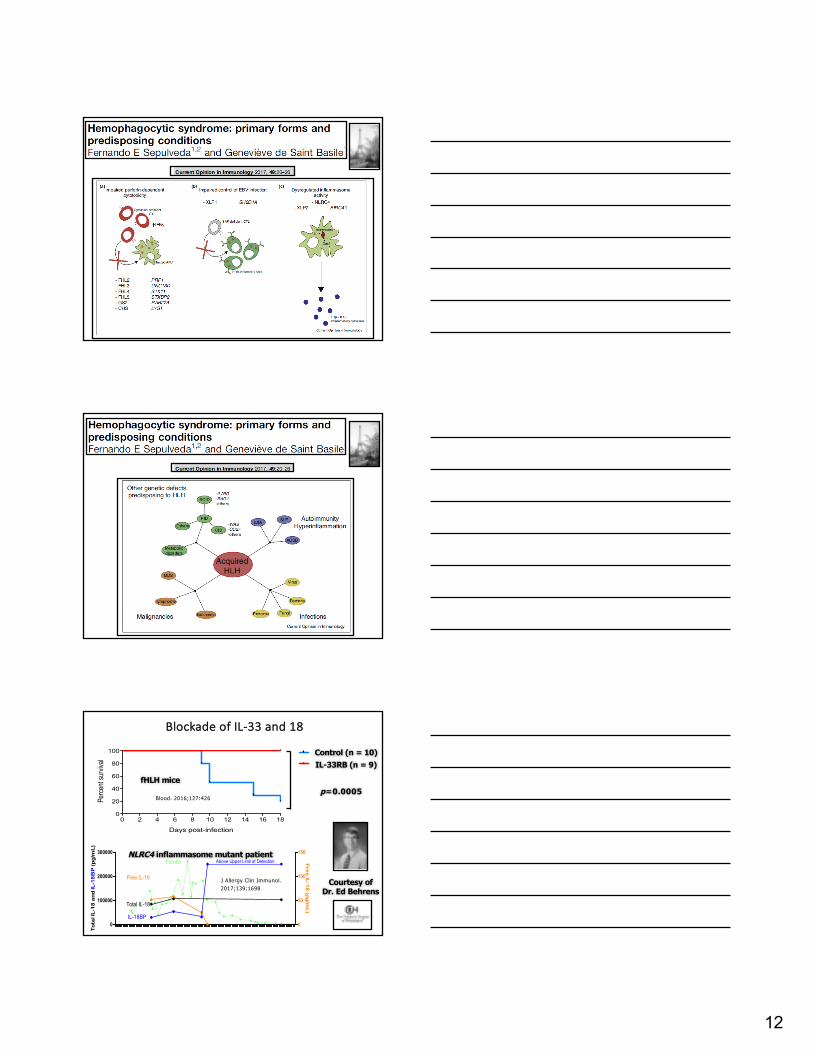
BlockadeofIL-33and18
Control (n = 10)IL-33RB (n = 9)
Survival
0 2 4 6 8 10 12 14 16 180
20
40
60
80
100 Control
IL-33RB
Days post-infection
Perc
ent s
urviv
al
p=0.0005
0
100000
200000
300000
0
50
100
150
To
tal I
L-1
8 a
nd
IL-1
8B
P (p
g/m
L)
Above Upper Limit of Detection
IL-18BP
Free IL-18
Total IL-18
Fre
e IL
-18
(pg
/mL
)
Ferritin
Courtesy of Dr. Ed Behrens
fHLH mice
NLRC4 inflammasome mutant patient
J Allergy Clin Immunol. 2017;139:1698
Blood. 2016;127:426

13
Prf1-/-
In Press
In Press
Anti-interferon-gammatrial
NI-0501: A Study to Investigate the Safety and Efficacy of an Anti-IFNγ mAb in Children Affected by Primary Hemophagocytic Lymphohistiocytosis
Children and adolescents, up to and including 18 years old at diagnosis of primary HLH, who, after having received conventional therapy, continue to have active disease, are potentially eligible. Children or adolescents with intolerance to HLH conventional treatment can also participate in the study.
“AllWeareSayingisGiveCytokineInhibitionaChance”
• Corticosteroids– sure,ofcourse• Cyclosporin A– youbetcha• Cytotoxicdrugs– canyouwait?• CytokineAntagonism– worthatry
– TNFa (probablynot)– IL-1(lookspromising)– IL-6,IL-18,IL-33,IFNg (???)– JAKinhibition(???)
"Imagination is more important than knowledge..." - Albert Einstein
Expert opinion.
14
Future Possibilities:Anakinra Treatment of
Hospitalizable Fever with Elevated Ferritin
ferritin ~$30 per testanakinra ~$130 per 100 mg dose
Lives saved - priceless
EarlyAggressiveTherapy
“Evendoctorswithgreatknowledgeandtechnicalskillcanhavemediocreresults;morenebulousfactorslikeaggressivenessandconsistencyandingenuitycanmatterenormously.”–Atul Gawande,MD,MPH (HarvardSchoolofPublicHealth)
• http://www.newyorker.com/fact/content/?041206fa_fact• (in:The New Yorker)
Funding
KAUL PEDIATRIC RESEARCH INSTITUTE

15
Questions??