Embed Size (px)
Citation preview

Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this photo and/or video. If you don’t want
your photo taken, please let us know.
Thank you!
DISCLAIMER

PHI includes, but is not limited to:- Patient name- Date of birth- Address- Occupation- Name of patient’s friends/family- Other identifiable features, i.e.
scars, tattoos, hair/eye color
Please DO NOT disclose any Protected Health Information (PHI)

Palliative Care ECHO ClinicWe are Nevada's Leading Forum for
Interdisciplinary Palliative CareWe aim to:
Collaborate with an interdisciplinary team of palliative care providers in Nevada
Assemble a forum of health care practitioners throughout the state of Nevada whom Project ECHO supports and prepares to deliver basic palliative care
Raise the quality of life for Nevadans living with serious illness
Establish a resource of expertise and education for a diverse health care audience on practices, resources and policy in palliative care

Palliative Care Where? In the Nursing Home!Jessica Cate, PharmD, BCPS, BCGPClinical Pharmacy SpecialistGeriatrics and Home Based Primary CareVA Sierra Nevada Health Care System
Kelly Conright, MD, CMDInternal Medicine, Geriatric Medicine, HPMHPM Fellowship Director, UNRSOM Attending Physician, GECVA Sierra NV Health Care System
Jonathan McCaleb, MD, CMDUNRSOM Associate Professor of Family MedicineGeriatrics, Hospice and Palliative Medicine Attending Physician, GEC VA Sierra NV Health Care System

Conflicts of Interest
None

Learning Objectives• Define nursing home populations
• Describe palliative care needs of nursing home populations
• Discuss one important palliative advance care planning tool for people in nursing homes
• Recognize palliative medication prescribing / deprescribing approaches in nursing home residents (case presentation)

Which of the following are “typical” nursing home patients?
• 72 y.o. woman who had her broken hip repaired and needs physical therapy to regain her physical independence
• 89 y.o. man who has advanced dementia and needs help dressing, bathing, transferring, and toileting
• 63 y.o. man who has Huntington’s disease, who needs help with all of his ADL’s, recently had an aspiration event, and has not woken up nor eaten for the past 3 days
• 70 y.o. woman with stage IV squamous cell cancer of the face, a new cholangiocarcinoma, and a recent stroke with left sided weakness who wants physical therapy to walk again and then go home

Who are Nursing Home Patients?

Rehabbed to Death

Palliative Care Implications
• High rates of burdensome transitions• ED Visits• Hospitalization• IV medicines and feeding tubes
• High rates of uncontrolled symptoms• Eating problems, weight loss, delirium, pressure ulcers,
constipation

Palliative Care Interventions
• Advanced Care planning• Goals of care conversations• Code Status• POLST
• Serious Illness Conversation Guide


Case
• JD 86 year-old male with past medical history of dementia with agitation and sundowning, hypertension, DMII, COPD, hyperlipidemia, and osteoarthritis
• Dependent for most ADLs and all IADLs• Bowel and bladder incontinent • FAST 6E• Admitted to a nursing home for care, family no longer able to
care for him

Palliative care prescribing
• Adding• Changing• Discontinuing

Deprescribing
“Process of withdrawal of an inappropriate medication, supervised by a health care professional with the goal of managing
polypharmacy and improving outcomes.”

Deprescribing
• Part of good prescribing, backing off when doses are to high or stopping medication that are no longer needed or may be causing harm
• When to consider• Goals of care• No longer effective• Completed• Unsafe
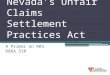
Benefit• Evidence for
ongoing indication
• Evidence for effectiveness
Risk• Known adverse
effects• Age-related
changes• Increased
comorbidities and medications

Benefits to deprescribing
• Reduced side effects• Reduced risk of drug interactions• Decreased pill burden• Improved quality of life

Potential risks of deprescribing
• Adverse drug withdrawal• Symptoms caused by removing the medication
• Increased risk of adverse event• Longer duration of therapy• Higher doses • Short half life• History of dependence/abuse• Lack of patient ‘buy-in’

Barriers to deprescribing• Patients
• “Giving up”• Afraid to stop medications that have taken for several years
• Several prescribers• Unclear history or duration on therapy• Lack of clear medication list• Fear of ‘withdrawal’ or adverse drug events• Family• Disease specific guidelines

Steps to deprescribing1.Thorough medical history/medication review2. Identify indications for all medications 3. Identify potentially inappropriate medications, those with less
evidence for benefit or those associate with harm4.Assess each medication for eligibility for deprescribing5.Prioritize medications for deprescribing6.Develop a plan for tapering and monitoring7.Provide support to patients, family and caregivers8.Document

Things to consider
• Most trials do not include > 75 y/o patients with multiple conditions
• Extrapolating evidence to older adults could be harmful• Time to benefit in number needed to treat (NNT)

Resources for deprescribing• Beers Criteria
• Released by the American Geriatrics Society • 2019 update • Medications to avoid or use cautiously in elderly• Evidence based, comprehensive
• START/STOP• START: Screening Tool to Alert doctors to the Right Treatment • STOPP: Screening Tool of Older Persons potentially inappropriate
Prescriptions• Deprescribing.org
• Proton pump inhibitors (PPI), benzodiazepines, antipsychotics (behavioral symptoms of dementia and insomnia), antihyperglycemics, and cholinesterase inhihtors

Medications to target
• Aspirin• Statins• Antihypertensives• Antihyperglycemics• Proton pump inhibitors (PPI)• Bisphosphonates• Memory medications

Back to JD – Case cont.• Medication list:
• Aspirin 81mg daily• Atorvastatin 40mg daily• Lisinopril 20mg daily• Amlodipine 10mg daily• Furosemide 20mg daily• Potassium chloride 20meq daily• Insulin glargine 10 units at bedtime• Insulin aspart 5 units with meals• Omeprazole 40mg daily• Donepezil 10mg daily
• Memantine 10mg BID• Albuterol inhaler prn• Olodaterol 2 puffs once daily• Tiotropium 2 puffs once daily• Diphenhydramine 50mg at bedtime
prn• Naproxen prn (use is sparingly)

Case cont.
• Patient has been refusing recent labs and vitals• Last known pertinent labs/vitals
• BP 102/72; HR 52• A1c 6.9%• Scr 1.1• Weight 52kg (downward trend over the last year)
• Last BM 4 days prior to evaluation• Appearing euvolemic, no LE edema noted

Deprescribing JD medications• Indications and/or possibly inappropriate
• Furosemide• Omeprazole• Diphenhydramine
• Prioritizing• ADRs
• Amlodipine• Diphenhydramine
• Prescribing cascade• Furosemide, potassium chloride
• Risk outweighs benefit• Donepezil and/or memantine• Insulin
• Lack of literature support• Atorvastatin• Aspirin

Recommendations for JD• Discontinue diphenhydramine, can use melatonin if needed• Discontinue insulin aspart; if no more labs or blood sugar
monitoring would discontinue insulin glargine as well• Discontinue naproxen, start acetaminophen prn (or consider
topicals)• Discontinue amlodipine
• Follow for improvement in edema, possibly d/c furosemide and potassium at follow-up
• Follow-up BP if remains well below goal can taper down lisinopril• Taper omeprazole• Discontinue aspirin and atorvastatin• Change to combination olodaterol/tiotropium• Add polyethylene glycol for bowels

Outcomes
• JD responded well to minimizing medications• Bowel movements became regular, every 1-2 days (his
preference)• No worsening of behaviors or notable decline in memory• BP remained well below goal, able to taper off lisinopril as well


Questions?

Survey
Please complete this brief survey. Your feedback is vital to our continued improvement of Project ECHO Nevada programming!
Thank you!

Thank you!
• Thank relevant partners• Next session date/topic• Advertise relevant resources/ECHOs

References• Rehabbed to Death: Breaking the Cycle JAGS 2019 Flint, et al• Palliative care: Nursing home Up to Date, Oct 2019• Reeve E, Gnjidic D, Long, Hilmer S. A systematic review of the emerging
definition of 'deprescribing' with network analysis: implications for future research and clinical practice. Br J Clin Pharmacol 2015;80(6):1254-68.
• Reeve E, Shakib S, Hendrix I, Roberts MS, Wiese MD. Review of deprescribing processes and development of an evidence-based patient-centered deprescribing process. Br J Clin Pharmcol 2014;78(4):738-747.
• American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 updated AGS Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;00:1-21, 2019.