Embed Size (px)
Citation preview

Director Siena Crosslinking Center®[email protected]
www.mazzottacosimo.com
The Author declares no financial interest

Reeves SW, Stinnett S, Adelman RA, et al. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. Am J Ophthalmol. 2005;140:607–11.
«…Keratoconus is more severe in children than in adults,.....
the age of the youngest child included in the study was 6 years ”
Beltaief O, Farah H, Kamoun R, Ben Said A, Ouertani A. Penetrating keratoplasty in children. Tunis Med. 2003;81(7):477–81.
«Keratoconus represents one of the most common causes of pediatric corneal transplantation causing about 15–20 % of all corneal transplants in children »
Ertan A, Muftuoglu O. Keratoconus clinical findingsaccording to different age and gender groups. Cornea. 2008;27(10):1109–13.
« Young age is associated with more severe forms of keratoconus and faster progression »
KC in Pediatrics

Caporossi A, Mazzotta C, et al. Riboflavin UVA-induced corneal collagen cross-linking in pediatricpatients.
Cornea. 2012;31:227–31.
« Childhood onset cases have a more aggressive progression than those of later onset »
Chatzis N, Hafezi F, et al. Progression of keratoconus and efficacy of pediatric [corrected] corneal collagen cross-linking in children and adolescents.
J Refract Surg. 2012 Nov;28(11):753-8.
“Progression of keratoconus was seen in 88% of children at 1 year………CXL in children and adolescents should be performed as soon as the diagnosis has been made”
KC in Pediatrics

Acute or Post acute Corneal Hydrops risk higher in Paediatrics eye-rubbers
suffering from allergy
Laura E. DowniePediatrics 2014;134:e596-e601
Eye Contact Lens. 2017 Oct 4.
Allergy and Eye-RubbingAccelerate
Keratoconus Progression

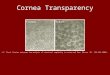
THERE ARE FEW STUDIES REGARDING TURNOVER OF COLLAGEN
Cornea- Fundamentals of cornea and external disease Mosby 1997 by Krachmer, Mannis and Holland Vol I, Chapter 1, page 13: “The turnover of collagen molecules in the cornea is slow, requiring 2 to 3 years”
“After CXL the turnover time is increased to about factor 2 x, thus you can calculate with about 7 years.” E. Spoerl
Invest Ophthalmol Vis Sci. ; 55(3): 1549–1554. doi:10.1167/iovs.13-13042.
Biomechanical Changes After Repeated Collagen Cross-Linkingon Human Corneas Assessed In Vitro Using Scanning Acoustic MicroscopyIthar M. Beshtawi, Riaz Akhtar, M. Chantal Hillarby, Clare O’Donnell, Xuegen Zhao,Arun Brahma, Fiona Carley, Brian Derby, and Hema Radhakrishnan
“The corneal collagen turnover ranges between 2 and 7 years. However, collagen crosslinking is expected to increase the half-life of the stromal collagen to more than 10 years”
Dahl BJ, Spotts E, Truong JQ. Corneal collagen cross-linking: An introduction and literaturereview. Optometry. 2012; 83:33–42.
Corneal Collagen Turnover


1
m3
m
6
m
1
y
Mazzotta C. American Journal of Ophthalmology 2008
CXL DELAY CORNEAL COLLAGEN TURN OVER FROM 2-3 TO 6-7 YEARS + 1 YMazzotta C. Cornea 2017, in Press
One year for Repopulation

Review of Literature Crosslinking for CXL in Pediatrics
From: Godefrooij DA, Soeters N, Imhof SM, Wisse RP. Cornea. 2016 Jul;35(7):954-8.

Siena CXL Pediatrics Largest Study
Cornea. 2012 Mar;31(3):227-31.
The first “Siena CXL Pediatrics Study” involved 152 keratoconus eyes:
• 94 eyes (61%) had 12 months of follow-up• 81 eyes (53%) were at 24 months of follow-up • 77 eyes (51%) at 36 months of follow-up

Cornea. 2016 Jul;35(7):954-8.
Progression= change in K max of 1.0 Diopter or more.

Nov 18 2017 05:17:33:298PM
RE: CORNEA-D-17-00849R2, entitled "Corneal Collagen Crosslinking With Riboflavin and
Ultraviolet-A Light for Pediatric Keratoconus: Ten-Year Results."
Dear Dott Mazzotta:
I am pleased to inform you that your work has now been accepted for publication in Cornea.
Thank you for submitting your interesting and important work to the journal.
With Kind Regards,
Alan Sugar, M.D.
Editor-in-Chief
Cornea
Paper accepted in press
Cornea 2017, in press
Corneal Collagen Crosslinking With Riboflavin and Ultraviolet-A Light for Pediatric
Keratoconus: Ten-Year Results.
Mazzotta C, Traversi C, Baiocchi S, Bagaglia S, Caporossi O, Villano A and Caporossi A

Baseline data of the 10 yrs follow-up Siena CXL Pediatric Study
The original Siena study of CXL inpediatrics involved 152 keratoconuseyes
• 94 eyes (61%) had 12 months offollow- up
• 81 eyes (53%) were at 24 months offollow-up
• 77 eyes (51%) at 36 months offollow-up and
• 62 eyes (40%) completed the ten-years follow-up.
The 60% of eyes were lost in 10 years.
Prospective longitudinal cohort study comprising 62 eyes of 47 patients who completed ten-years follow-up. Thirty-eight patients (80%) were male, and mean age at the time of treatment was
14.11 ±2,43 years (range: 8-18yrs)
STATISITCAL ANALYSIS 2-tailed paired samples Student t test Differences with P < 0.05 were considered significantData were collected and analyzed with PRISM 6.0 GraphPad Software (La Jolla, California USA).

0
0,2
0,4
0,6
0,8
PRE OP1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
CDVA LogMAR
0
0,2
0,4
0,6
PREOP
1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
UDVA (LogMAR)
Results
UDVA improved at all follow-up times, with the difference becoming statistically significant at the 6th months (P > 0.05) 1-2-3-4-5-6-7-8-9-
10 year (P = 0.001), visits,
CDVA improved significantly afterundergoing cross-linking at allfollow-up visits, with theexception of the 3rd month after
treatment (P = 0.3299)
from 0.45 to 0.23 LogMAR (P = 0.0001)
from 0.14 to 0.1 LogMAR (P = 0.019)

52
53
54
55
56
57
PREOP
1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
Kmax (D)Results
K max value improved significantly 6 months after treatment (P = 0.0454), and this improvement remained statistically significant up to 8th year follow-up (P = 0.0454), Over the 8th year follow-up the K max improvement loose its
statistically significance*
from 55.45 to 54.33 D* to 54.52 D 10 yrs
0
2
4
PREOP
1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
t-CYL (D)
from 2.9 to 2.7 D 10 yrs
T-Cyl value showed not statistically significant changes along the entire
follow-up

0,9
1
1,1
PRE OP1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
Coma
350
400
450
500
PREOP
1M 3M 6M 1Y 2Y 3y 4y 5y 6y 7y 8y 9y 10y
Minimum Corneal Thickness
from 453 µm to 407.2 1° m, to 429 at 3° m µm – n.s.s. to 1-y : 454 µm,
Results
Coma values improved becoming statistically significant since the 1th postoperative month (P 0.0001) maintaining a
long-term statistical significance
MCT value decreased significantly at 1st postoperative month (P = 0.0001) and 3rd month (P = 0.020), returning to baseline value at 6th month, maintaining a substantial stability
up to 10-years follow-up
from 1.01 to 0.9 µm

Statistically significant functional improvement of UDVA and CDVA in nearly 80 % of patients 18 years and under after 10-years follow- up. The 19% of patients in this cohort, up 24 to 36 months after CXL, showed a not statistically significant
tendency of keratometry readings regression, returning at their baseline values.
Overall Study Results

Temporary haze (12.7%). 2 patients showed a K max progression up to 3.2 D requiring an additional epithelium-off CXL retreatment (4.2%) up 24 to 36 m, and this outcome was similar with the findings reported by Raiskup et al. Interestingly none of these patients showed a decline of one or more lines in either UDVA or CDVA. Both patients were younger than 15 years old at the time of the inclusion in the CXL treatment protocol and suffered from severe allergic conjunctivitis with intense eye-rubbing that were considered as possible causes of poorer response.
Adverse Events
Overall 10-yrs follow-up progression rate was about 24 %, including 13 eyes
of 9 patients with K max progression over 1 D and 2 eyes of 2 patients who
underwent deep anterior lamellar keratoplasty.

Results
• The astigmatism was not significantly reduced. Corneal symmetry improved over a
5-years period increasing the quality of vision thus maintaining astigmatism.
• The overall progression rate, intended as K max change of 1 D or more was
reported in 20% of eyes and in 19% of patients, excluding the 2 eyes (3.2%) of the
2 patients (4.2%) requiring a deep anterior lamellar keratoplasty (DALK) 5 and 6
years after CXL respectively due to rigid gas permeable(RGP) intolerance.
• Including these 2 cases among the overall adverse events, the 10-years progression
rate included 24 % of patients.
• Among cases with documented progression, 10 patients (21%) aged 12.4 years on
average (range 10-15 years), at the time of the inclusion in the treatment protocol,
showing a statistically not significant K max progression between the 7th and the
10th year follow-up.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
KC progression, age effect and CXL protection window
Progressive Age stiffening
Age (years) 10 20 30 40
Keratoconus progression
CXL
CXL
CXL
100%
90%
50%
70%
30%
80%
60%
40%
15 25 35
CXL can delay corneal collagen turnover from 2-3 to 6-8 yearsconferring an estimated protection window of 7-8 yrs

• Conventional Epithelium-Off CXL is both safe and effective conferring a long-term KC stability after 10-year follow-up in nearly 80% of pediatric patients. The study demonstrates the ability of CXL to slow down KC progression, improving functional performance.
• The mechanism of corneal collagen turnover is counterbalanced from CXL effect and by the expected age-related corneal stiffening
• The long-term stability may be correlated to CXL-induced delay in corneal collagen turnover and to the age-related corneal stiffening and keratoconus stabilization.
• According to 10-yrs follow-up data, parents of the younger patients must be informed that 6 to 8 years after CXL, the corneal collagen turnover may induce a loss of CXL effect duration in about 24% of cases. A new keratoconus instability or progression could be registered and if so the treatment could be repeated if necessary.
• Early Diagnosis, Rapid decision !
• Do CXL Treatment without awaiting progression !!
• Close monitoring especially in allergic-eye-rubbers young patients !!!
• No fear to retreat if necessary !!!!
Discussion and Recommendations