Embed Size (px)
Citation preview

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com 1
Long-term Safety and Efficacy of High-Fluence Collagen Crosslinking of the Vehicle
Cornea in Boston Keratoprosthesis Type 1
A. John Kanellopoulos, MDDirector, Laservision.gr Institute, Athens, Greece
Clinical Professor NYU Medical School, NYFinancial Interest: Consultant for Alcon, Avedro, Allergan, i-Optics,
Keramed
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
PurposeThe purpose of this study was to evaluate safety and efficacy of very high-fluence collagen crosslinking as a means of increasing cornea rigidity and reducing enzymatic digestion in the vehicle cornea of Boston keratoprosthesis (Kpro) Type1 performed.

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
MethodsEleven consecutive Kpro cases (5 with repeat cornea graft failure, 4 ocular cicatricial pemphigoid, and 2 chemical burn) received donor-vehicle cornea pre-treatment with very high-fluence prophylactic collagen crosslinking in two sessions.
The donor cornea was initially cross-linked with intrastromal riboflavin instillation through a femtosecond-laser-created pocket; followed by superficial CXL.
All cases, at the completion of the CXL pre-treatment, had the cornea center trephined with femtosecond laser; the vehicle cornea was trephined with a 9-mm donor punch and the Kpro Type1 was fitted onto the cross-linked donor cornea.

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
Video

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
Surgical techniqueInner donor cornea collagen cross-linking through the femtosecond laser-created pocket.
FS200 femtosecond laser programming interface
Screen capture of the 8-mm diameter, 400 μm deep femtosecond laser assisted pocket creation
Intrastromal infusion of 0.1% riboflavin solution with the olive-tip cannula.
Femtosecond laser assisted pocket creation
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
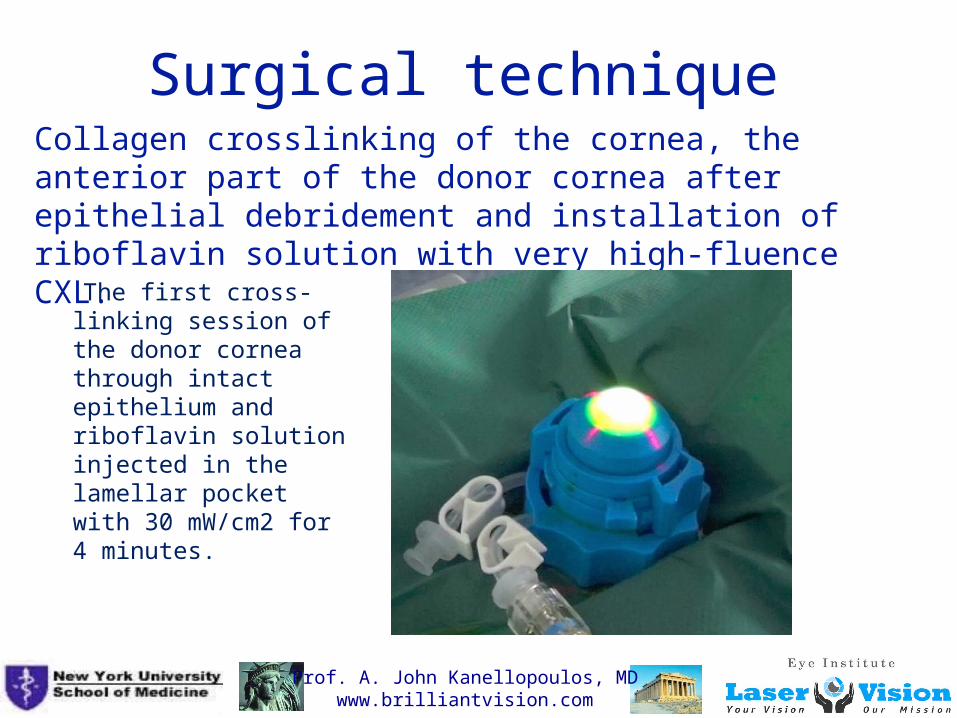
Surgical techniqueCollagen crosslinking of the cornea, the anterior part of the donor cornea after epithelial debridement and installation of riboflavin solution with very high-fluence CXL.
The first cross-linking session of the donor cornea through intact epithelium and riboflavin solution injected in the lamellar pocket with 30 mW/cm2 for 4 minutes.
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
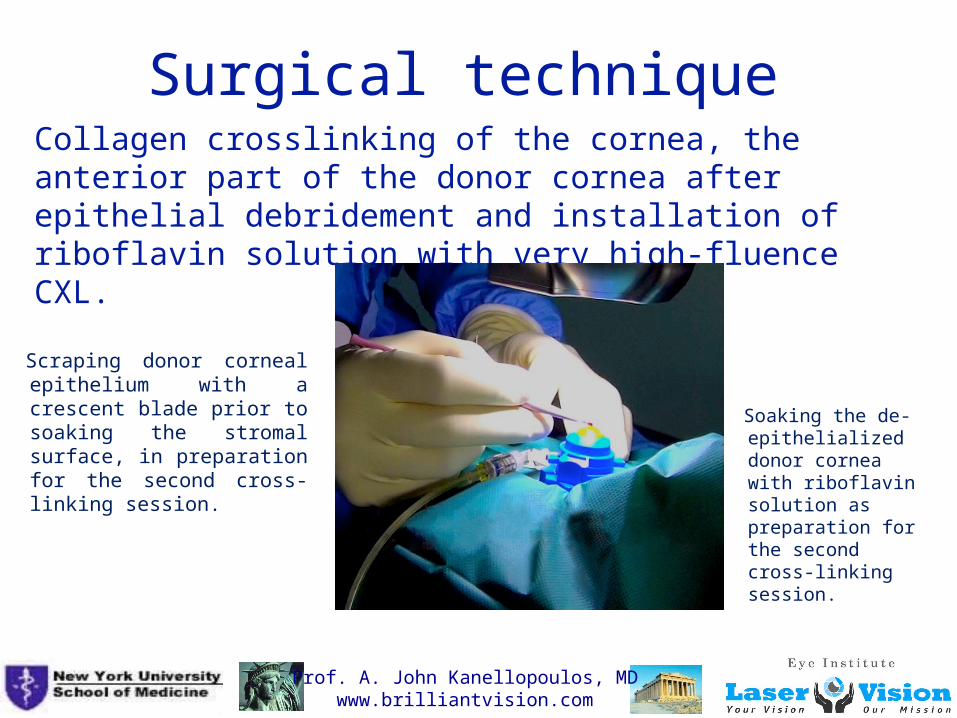
Surgical techniqueCollagen crosslinking of the cornea, the anterior part of the donor cornea after epithelial debridement and installation of riboflavin solution with very high-fluence CXL.
Soaking the de-epithelialized donor cornea with riboflavin solution as preparation for the second cross-linking session.
Scraping donor corneal epithelium with a crescent blade prior to soaking the stromal surface, in preparation for the second cross-linking session.
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
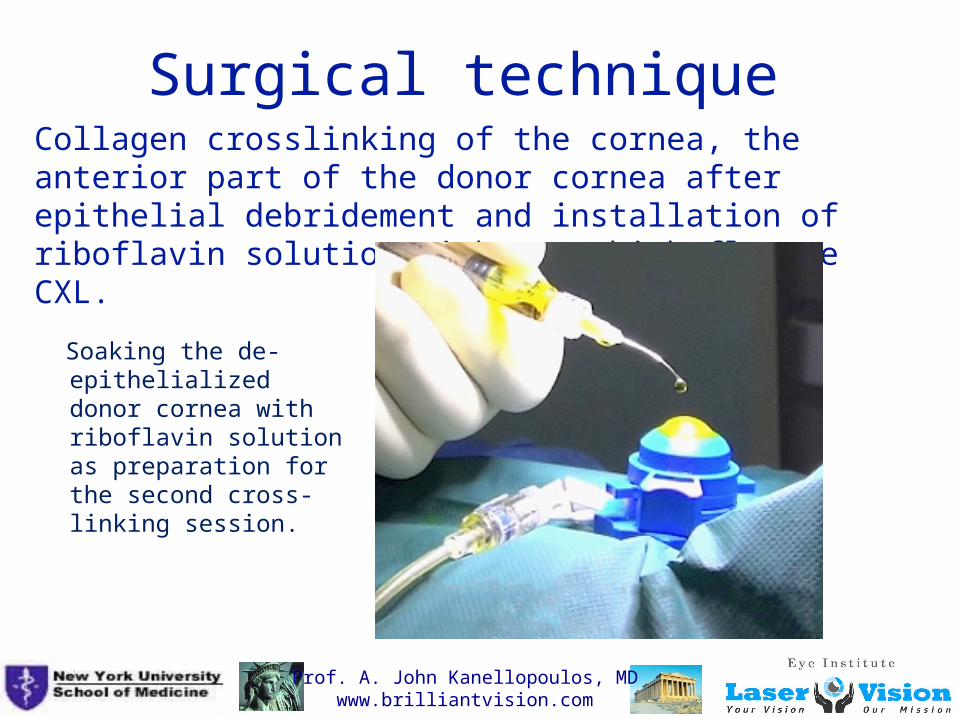
Surgical techniqueCollagen crosslinking of the cornea, the anterior part of the donor cornea after epithelial debridement and installation of riboflavin solution with very high-fluence CXL.
Soaking the de-epithelialized donor cornea with riboflavin solution as preparation for the second cross-linking session.
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
Results
We evaluated visual acuity, corneal surface and donor vehicle cornea stability. Mean follow-up was 7.5(1 to 9) years.
Mean uncorrected visual acuity improved from light-perception to 20/60.
One case needed follow-up surgery, due to significant melt in the host cornea.
None of the eyes developed melts and/or infection, especially on the vehicle cornea on which the keratoprosthesis was fitted.
Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
DiscussionThe main obstacles of prosthesis and visual rehabilitation stability which we have encountered and reported (Peralta RJ, Kanellopoulos AJ. Boston Keratoprosthesis: A long-term prospective clinical study A Long-Term Prospective Clinical Study. Poster Presentation, ARVO Meeting, May 6-10, 2007, Fort Lauderdale, Florida, USA), have been intraocular pressure (IOP) control, infection (which was attributed partly on cornea melt around the prosthesis), and intraocular inflammation.
One of the two major difficulties in managing these patients has been antibiotic prophylaxis, because these eyes are especially susceptible to microbial infections, which, following the keratoprosthesis surgery, almost invariably become endophthalmitis in a unichamber eye with very poor prognosis.
The second significant post-operative management problem is donor vehicle cornea and/or host cornea melts, especially near the graft-host interface.

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
DiscussionThe decision to incorporate this adjunct prophylactic treatment in these very challenging cases was based on significant experience with collagen crosslinking techniques.
The long-term safety and efficacy results of this technique as noted above suggest that there may exist a very significant advantage to the long-term prognosis of Boston keratoprosthesis.
This work presents 11 cases treated with adjuvant crosslinking.
The relative rarity of the parameters that led to the decision for inclusion in this study leads us to believe our cases represent one of the largest groups in the literature.
Among the reasons for cross-linking was our observation that up to 50% of these patients suffer from cornea melting which may increase their likelihood for infections

Prof. A. John Kanellopoulos, MDwww.brilliantvision.com
Conclusions
Pre-treatment with intrastromal and superficial very high-fluence collagen crosslinking in conjunction with Boston Type 1 keratoprosthesis appears to be a safe and effective adjunctive treatment aiming to increase vehicle donor cornea rigidity and potentially increased resistance to enzymatic degradation.
This application may serve to enhance the biomechanical stability and external disease susceptibility of the donor vehicle cornea in these advanced external disease cases.





























