Embed Size (px)
Citation preview
{InsIde thIs Issue}
STAMPEDE Study: A Surgical Perspective p.3
Service Spotlight: Swallowing Center p.4
Pancreatic Cyst Registry Helps Avoid Unneeded Surgery p.6
Digestive Disease institute | Fall | 2012
Digestthis
Fecal Incontinence Therapy: Raising the Bar p.1
in their genes – p.8
DIgESTIvE DISEASE InSTITUTE CHAIR John Fung, MD, PhD
MAnAgIng EDIToR glenn Campbell
ART DIRECToR Mike viars
MARkETIng MAnAgERS Priya Barra Matthew Chaney
ConTRIBUTIng PHoTogRAPHERS Russell Lee Cleveland Clinic Center for Medical Art & Photography
dear Colleagues,genetics-related research is the focus of our cover story in this issue of Digest This.
For clinician researchers, success in unraveling the genetic underpinnings of disease
has at least two key ingredients: a large volume of patients with (or at risk of) a given
disease, and a supportive scientific infrastructure.
As our cover story profiles the recent genetic research achievements of three clini-
cian investigators from across Cleveland Clinic’s Digestive Disease Institute, a pattern
emerges. Each investigator has drawn on specimens and experience from a formidable
base of patients with complex and challenging diseases, and each has deployed clini-
cal insight and scientific know-how to make more sense of these diseases at the popu-
lation level — and, in some cases, even at the patient level. They have been assisted
in their efforts by the size and multidisciplinary expertise of Cleveland Clinic as well as
through collaborations with partners beyond Cleveland Clinic.
The result has been significant steps along the path toward more personalized medicine,
whether in more tailored and effective methods of detecting cancer, enhanced ability to
predict disease recurrence, or insights that may lead to more targeted therapies.
other articles in this issue continue the theme of personalized medicine outside the
context of genetic research. For instance, Dr. R. Matthew Walsh (p. 6) explains how
we have used our extensive pancreatic cyst registry to develop a protocol for pancreatic
cyst management that recognizes that some patients with these cysts do not require
resection and can be safely observed. And Drs. Steven D. Wexner and Brooke gurland
(p. 1) draw on our substantial experience in sacral nerve stimulation for fecal inconti-
nence to give advice on which patients are the best candidates for this highly effective
new intervention.
The personalized medicine promised by genetic research and other investigations is
one more form — albeit an especially potent one — of valuing the individual patient
experience. Putting a premium on patient experience has been a guiding principle
for Cleveland Clinic, as reflected by our reorganization under the patient-oriented
institute model several years ago. Under this model, the Digestive Disease Institute
comprises a breadth of services related to digestive health. I’m delighted that this
issue spotlights clinical and research insights from a wide sampling of those services.
Take a moment to review our diverse activities within these pages, and let me know
if you see opportunities to partner in improving the experience of all our patients.
Respectfully,
John Fung, Md, Phd Chairman, Cleveland Clinic Digestive Disease Institute
Director, Cleveland Clinic Transplant Center Professor of Surgery, Lerner College of Medicine [email protected]
Cleveland Clinic #2 in the U.S. – Gastroenterology

clevelandclinic.org/digestive 855.REFER.123 {1}
Digestive Disease Institute
95 – 100%of Cleveland Clinic patients
have been able to move
on to implantation of a
permanent stimulator.
sacral nerve stimulation: Raising the Bar in Fecal Incontinence Therapy
special Feature
sacral nerve stimulation (sns) offers patients with chronic fecal incontinence an
opportunity to achieve improved or even complete control of their symptoms. the procedure,
used to treat urinary incontinence in the united states since 1997, received FDa approval for
use in fecal incontinence in 2011. clinical trials of sns for fecal incontinence were completed
at cleveland clinic’s main campus and cleveland clinic Florida, and colorectal surgeons at
both locations now offer the procedure for fecal incontinence.
‘PACEMAkER FoR THE AnAL SPHInCTER’
SnS is like a cardiac pacemaker for the anal sphinc-
ter. Surgeons first implant temporary subcutaneous
stimulators into the sacral nerve. For patients who
experience improvement of more than 50 percent in
the number of fecal incontinence episodes during a
two-week trial, surgeons go on to implant a perma-
nent stimulator in a second procedure.
The procedure requires only local anesthesia and
intravenous sedation and does not have a long
recovery period.
CoMPARES WELL WITH ALTERnATIvES
Steven D. Wexner, MD, Chairman of Colorectal Sur-
gery and Chief Academic Officer at Cleveland Clinic
Florida, was lead international investigator on the SnS
fecal incontinence trials that led to FDA approval. He
presented results at the 2010 meeting of the Ameri-
can Society of Colon and Rectal Surgeons, of which he
is now president, and was lead author of the full study
report published in Annals of Surgery in 2010. He
also was lead author of another key study, examining
infection rates in SnS, published in Journal of Gastro-
intestinal Surgery (see Suggested Reading, p. 2).
Dr. Wexner’s experience with SnS is among the broad-
est in the country. He has performed more than 50 of
the procedures and reports having achieved excellent
outcomes in most patients.
“I have a lot I can compare with SnS, as I have been
lead investigator in numerous trials for several other
predicate devices,” he says. “SnS achieves vastly bet-
ter outcomes with far less frequent and significantly
less severe complications.”
About 95 percent of Dr. Wexner’s patients move on
to the second-stage procedure. Advancement to the
second-stage procedure has been possible for all seven
of the patients treated by Brooke gurland, MD, and as-
sociates in the Colorectal Center for Functional Bowel
Disorders at Cleveland Clinic’s main campus.
BEST CAnDIDATES
Drs. Wexner and gurland both say there is no “ideal
candidate” for this procedure. For example, age (young
vs. old) does not seem to affect outcomes.
“More patients are turning out to be very good
candidates than we expected,” Dr. Wexner says.
Dr. gurland says the best candidates are often those
with the worst control. These are patients who have
tried other treatments, such as bulking agents and
antidiarrheal medications, and perhaps even unsuc-
cessful prior surgical procedures. “We are finding that
patients with loose stools who are poor candidates for
sphincteroplasty may have improvements with SnS,”
she notes.
oTHER InDICATIonS LIkELy
Dr. Wexner expects that, with time, approved indica-
tions for SnS will include chronic constipation and ir-
ritable bowel syndrome. Additionally, success with the
procedure has been reported anecdotally from outside
the United States in patients with rectal pain, sphincter
injuries and anal fissures.
“SnS is not replacing or augmenting the anal sphincter,
but rather creating a neuromodulation that enhances
sensation, alerting patients earlier when they need to
go to the bathroom, which is an entirely different
approach to treating these problems,” he says.
steven d. Wexner, Md
Brooke Gurland, Md
{2} digest this Fall | 2012
Cleveland Clinic
PATIEnTS ARE PLEASED
Patients are delighted with the outcomes, both surgeons report. “I get more positive
comments about SnS than about any other treatment we offer for fecal incontinence,”
Dr. Wexner says. “Patients are very happy, not just mildly happy.”
Many other treatments achieve therapeutic success — a 50 percent or greater reduction in
symptoms — in about 35 to 65 percent of patients, he says. In the Annals of Surgery study, at
12 months, 83 percent of subjects achieved therapeutic success and 41 percent achieved 100
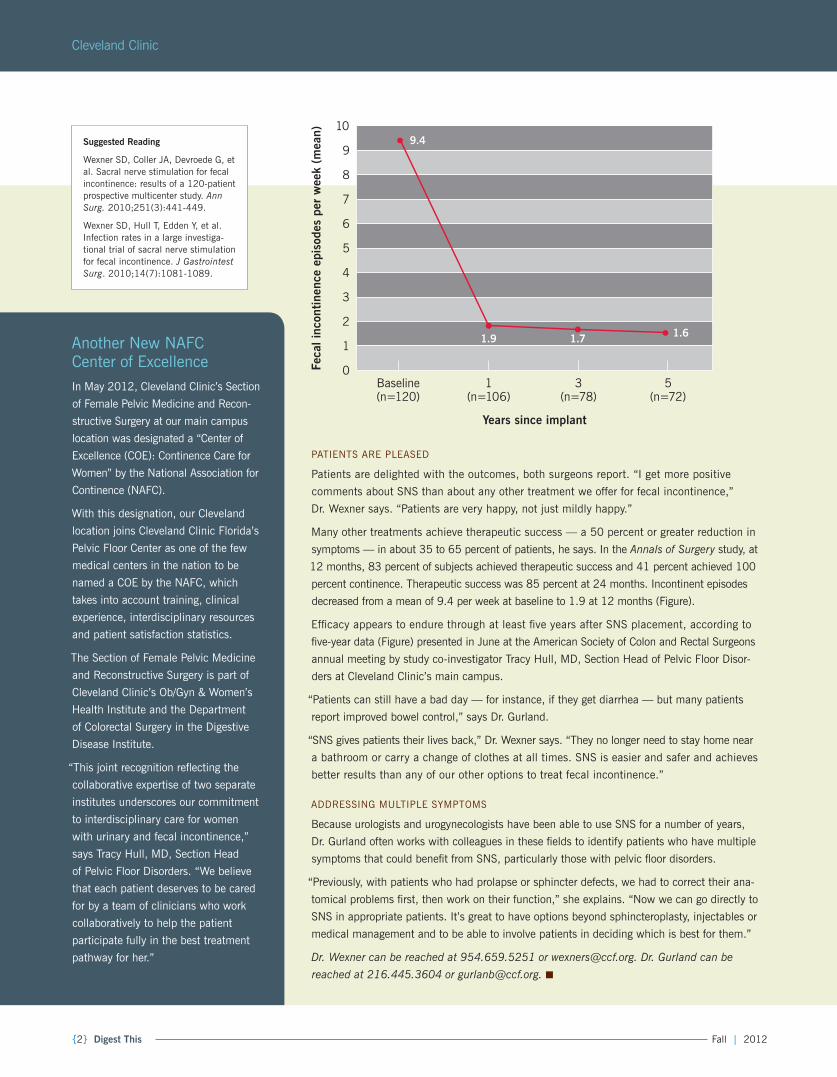
percent continence. Therapeutic success was 85 percent at 24 months. Incontinent episodes
decreased from a mean of 9.4 per week at baseline to 1.9 at 12 months (Figure).
Efficacy appears to endure through at least five years after SNS placement, according to
five-year data (Figure) presented in June at the American Society of Colon and Rectal Surgeons
annual meeting by study co-investigator Tracy Hull, MD, Section Head of Pelvic Floor Disor-
ders at Cleveland Clinic’s main campus.
“Patients can still have a bad day — for instance, if they get diarrhea — but many patients
report improved bowel control,” says Dr. gurland.
“SnS gives patients their lives back,” Dr. Wexner says. “They no longer need to stay home near
a bathroom or carry a change of clothes at all times. SnS is easier and safer and achieves
better results than any of our other options to treat fecal incontinence.”
ADDRESSIng MULTIPLE SyMPToMS
Because urologists and urogynecologists have been able to use SnS for a number of years,
Dr. Gurland often works with colleagues in these fields to identify patients who have multiple
symptoms that could benefit from SNS, particularly those with pelvic floor disorders.
“Previously, with patients who had prolapse or sphincter defects, we had to correct their ana-
tomical problems first, then work on their function,” she explains. “Now we can go directly to
SnS in appropriate patients. It’s great to have options beyond sphincteroplasty, injectables or
medical management and to be able to involve patients in deciding which is best for them.”
Dr. Wexner can be reached at 954.659.5251 or [email protected]. Dr. Gurland can be
reached at 216.445.3604 or [email protected]. ■
Feca
l inc
ontine
nce
epis
odes
per
wee
k (m
ean)
Years since implant
109.4
1.9 1.7 1.6
9
8
7
6
5
4
3
2
1
0Baseline (n=120)
1 (n=106)
3 (n=78)
5 (n=72)
suggested Reading
Wexner SD, Coller JA, Devroede g, et al. Sacral nerve stimulation for fecal incontinence: results of a 120-patient prospective multicenter study. Ann Surg. 2010;251(3):441-449.
Wexner SD, Hull T, Edden y, et al. Infection rates in a large investiga-tional trial of sacral nerve stimulation for fecal incontinence. J Gastrointest Surg. 2010;14(7):1081-1089.
Another new nAFC Center of ExcellenceIn May 2012, Cleveland Clinic’s Section
of Female Pelvic Medicine and Recon-
structive Surgery at our main campus
location was designated a “Center of
Excellence (CoE): Continence Care for
Women” by the national Association for
Continence (nAFC).
With this designation, our Cleveland
location joins Cleveland Clinic Florida’s
Pelvic Floor Center as one of the few
medical centers in the nation to be
named a CoE by the nAFC, which
takes into account training, clinical
experience, interdisciplinary resources
and patient satisfaction statistics.
The Section of Female Pelvic Medicine
and Reconstructive Surgery is part of
Cleveland Clinic’s ob/gyn & Women’s
Health Institute and the Department
of Colorectal Surgery in the Digestive
Disease Institute.
“This joint recognition reflecting the
collaborative expertise of two separate
institutes underscores our commitment
to interdisciplinary care for women
with urinary and fecal incontinence,”
says Tracy Hull, MD, Section Head
of Pelvic Floor Disorders. “We believe
that each patient deserves to be cared
for by a team of clinicians who work
collaboratively to help the patient
participate fully in the best treatment
pathway for her.”
clevelandclinic.org/digestive 855.REFER.123 {3}
Digestive Disease Institute
the staMpeDe study – a surgical perspective
cleveland clinic’s staMpeDe trial has been making headlines since March (see sidebar
for study details), but much of the buzz has been in diabetes circles. We asked Matthew
D. Kroh, MD, a minimally invasive surgeon in our Digestive Disease institute who performs
many bariatric procedures (but who was not involved in staMpeDe), for his take on the
study’s likely implications for bariatric surgery.
Q: In light of stAMPede, will bariatric surgery
be considered earlier in the management of obese
patients with uncontrolled type 2 diabetes?
dr. Kroh: I believe it will. For years retrospective studies
have shown that bariatric surgery is effective for treat-
ment of type 2 diabetes. now STAMPEDE has demon-
strated that prospectively, using a randomized design
with excellent follow-up and with a control arm of best
medical management. I think this will lead to greater
consideration of bariatric surgery as an earlier interven-
tion as opposed to an end-stage intervention for these
patients, and I certainly believe that is appropriate.
Q: how important were surgical skill and surgical
volume to the results achieved in stAMPede?
dr. Kroh: Cleveland Clinic has been designated a
Center of Excellence by the American Society for Meta-
bolic and Bariatric Surgery (ASMBS), so it would be
inappropriate for these findings to be broadly applied
to every general or bariatric surgeon performing bar-
iatric surgery. But the findings are probably applicable
to the more than 400 ASMBS-designated Centers of
Excellence, which all meet certain criteria for volume,
outcomes and ancillary services.
Q: Which factors should guide patient selection
to optimize the risk-benefit calculation?
dr. Kroh: Historically there has been a misperception
that bariatric surgery has a very high complication
rate. With the advent of ASMBS Centers of Excellence,
complications have been significantly reduced and bar-
iatric surgery is now on par with many other commonly
performed operations. The STAMPEDE results further
confirm this. So the calculation now is whether to in-
tervene earlier to prevent the end-stage manifestations
of diabetes, and I think we should. So any patient with
type 2 diabetes who meets the nIH criteria for bariatric
surgery — BMI of 35 or greater with weight-related
medical conditions, or BMI of 40 or greater — should
be considered, to prevent the progression of what is a
severely disabling chronic disease.
Q: As longer-term results emerge from stAMPede,
what should surgeons pay particular attention to?
dr. Kroh: We know that weight loss after gastric
bypass and sleeve gastrectomy continues beyond 12
months — up to 24 months in some patients. I’ll be
looking to see if the STAMPEDE patients’ glycemic
control improves beyond the initial 12 months as well,
and by how much. The corollary is that at around five
or 10 years, some proportion of patients regain some
weight, although it’s usually insignificant compared
with their initial weight loss. We’ll need to see what ef-
fect that may have on long-term resolution or remission
of diabetes. So looking at the durability of the effects of
surgery on glycemic control over two years, five years
and beyond is going to be very important.
Q: Any last thoughts?
dr. Kroh: I hope this high-quality data will start to
change practice patterns in diabetes management.
In view of these findings, morbidly obese patients
should be given an option to consider bariatric
surgery for potential remission of diabetes earlier
in their treatment course as opposed to prolonged
therapy with antihyperglycemic regimens.
Dr. Kroh has appointments in the Digestive Disease
Institute’s Department of General Surgery and in
the Bariatric & Metabolic Institute. Contact him
at 216.445.9966 or [email protected]. ■
Matthew d. Kroh, Md
STAMPEDE at a glancedesign: Randomized,
nonblinded, single-center
(Cleveland Clinic) comparison
of intensive medical therapy
alone with medical therapy
plus either Roux-en-y gastric
bypass or sleeve gastrectomy
Population: 150 obese
patients with uncontrolled
type 2 diabetes being
followed for five years
Primary endpoint:
Percentage of patients with
an HbA1c ≤ 6.0 percent
Results: At 12 months
(first planned analysis),
significantly more patients
in the gastric bypass group
(42 percent) and the sleeve
gastrectomy group (37
percent) achieved the primary
endpoint compared with the
medical therapy group (12
percent). Weight loss was
also significantly greater in
both bariatric surgery groups
vs. the medical therapy arm.
Schauer PR, kashyap SR, Wolski D, et al. N Engl J Med. 2012;366(17):1567-1576.

{4} digest this Fall | 2012
Cleveland Clinic
service spotlight: Center for Swallowing and Esophageal Disorders
One of the nation’s few dedicated swallowing centers has a new leader. sigurbjorn
Birgisson, MD, Ma, joined cleveland clinic’s Digestive Disease institute in February 2012
as Director of the center for swallowing and esophageal Disorders (swallowing center).
The appointment marks a homecoming of sorts
for Dr. Birgisson, who trained at Cleveland Clinic in
the mid-1990s and 2000. “Some of the best esoph-
agologists in the nation have practiced and taught
at Cleveland Clinic over the years,” he says. “I am
honored to lead a program with such a rich history
of excellence in swallowing disorder practice
and research.”
Dr. Birgisson, who previously directed the endoscopy
and motility unit at the national University Hospital of
Iceland, rounds out a team of four specialist physicians
in the Swallowing Center. The others are Steven Shay,
MD; Prashanthi Thota, MD; and Monica Ray, MD. Two
full-time nurses perform all the center’s motility, pH
and breath-test studies.
A FoCUS on CoMPLEx CASES
The Swallowing Center team collaborates with mul-
tidisciplinary specialists from across Cleveland Clinic
— radiologists, otolaryngologists, thoracic and general
surgeons, pathologists, speech pathologists and oth-
ers — to manage some 2,500 patients a year. Their
patients fall into two main groups: those with dyspha-
gia from a variety of causes, and those with difficult-
to-manage gERD with typical and atypical symptoms.
The program’s particular strengths lie in dealing with
several complex conditions:
Achalasia. “We see more than 150 new achalasia
patients a year,” says Dr. Birgisson. “Many are referred
from out of state.” Most often they are treated surgically,
mainly by Cleveland Clinic thoracic surgeons such as
Thomas Rice, MD, with whom the Swallowing Center’s
esophagologists closely consult. “Dr. Rice probably has
more experience treating achalasia patients surgically
than anyone in the country,” Dr. Birgisson notes.
Reflux management in lung transplant patients. Reflux
is common in lung transplant recipients and can lead
to organ rejection. Because Cleveland Clinic has one
of the nation’s largest lung transplant programs, there
is great demand for the Swallowing Center’s expertise.
“These patients often have troublesome reflux before
or after surgery, as well as problems with swallowing
or gastroparesis,” explains Dr. Birgisson. “We evaluate
many of them before or after transplant and consult on
reflux management strategies.”
Extraesophageal reflux syndromes, such as chronic
laryngitis, chronic cough and asthma. “It can be very
difficult to establish or exclude the association between
reflux and these symptoms and disorders,” Dr. Birgis-
son says. “A multidisciplinary approach with consider-
able testing is typically needed.” Similarly, the Swal-
lowing Center sees many patients referred to Cleveland
Clinic following failed reflux surgery — another group
that can pose big management challenges.
sigurbjorn Birgisson, Md
“It can be difficult to establish or exclude the association between
reflux and symptoms of extraesophageal reflux syndromes such as
chronic laryngitis, chronic cough and asthma. A multidisciplinary
approach is typically needed.” – Sigurbjorn Birgisson, MD
clevelandclinic.org/digestive 855.REFER.123 {5}
Digestive Disease Institute
RESEARCH PRIoRITIES
Dr. Birgisson sees many of the above conditions as the
Swallowing Center’s priority research areas, largely by
virtue of the volume of patients seen. “We have a great
opportunity to study a variety of motility and reflux prob-
lems in lung transplant recipients,” he says. Likewise,
the center is exploring research initiatives to leverage its
nearly matchless volume of achalasia cases.
Further research opportunities stem from the center’s
registry of approximately 2,000 Barrett’s esophagus
patients — one of the largest such registries in the
nation. About one-third of the registry’s patients have
dysplasia, which drives the center’s use of the registry
to ensure regular follow-up and to monitor patient
progress following ablation therapy, endoscopic muco-
sal resection or other treatments.
CUSToMIzED EMR-InTEgRATED QUESTIonnAIRE
An early priority for Dr. Birgisson has been developing
an electronic patient questionnaire specific to esopha-
geal disease. The questionnaire is being created within
the framework of Cleveland Clinic’s knowledge Pro-
gram, an interactive database that helps quantitatively
measure the effectiveness of medical decisions for
patients with specific diseases. The aim is for patients
to complete the questionnaires on touch-screen tablets
before each clinical visit to allow good longitudinal
tracking and to automatically update the electronic
medical record (EMR) in real time, prior to the visit.
“our questionnaire will cover patients with symptoms
of dysphagia and gERD, and the aim is to correlate
symptoms with findings on tests such as endoscopy,
manometry and pH studies,” explains Dr. Birgisson.
He expects it will enhance treatment monitoring and
promote better-targeted testing. Implementation is
planned for later this year.
RETURn oF ‘SWALLoW THIS’
One smaller but personally significant initiative
Dr. Birgisson has championed is the reintroduction
of the Swallowing Center’s monthly multidisciplinary
“Swallow This” meetings he remembers fondly from his
motility fellowship at Cleveland Clinic in the mid-1990s.
These monthly meetings gather the center’s staff with
colleagues from other relevant specialties to discuss the
management of complex cases. “The sessions are stimu-
lating,” he says, “and underscore the broad expertise
and resources we can bring to bear for patients with the
most challenging swallowing and esophageal disorders.”
Contact Dr. Birgisson at 216.444.0780
or [email protected]. ■
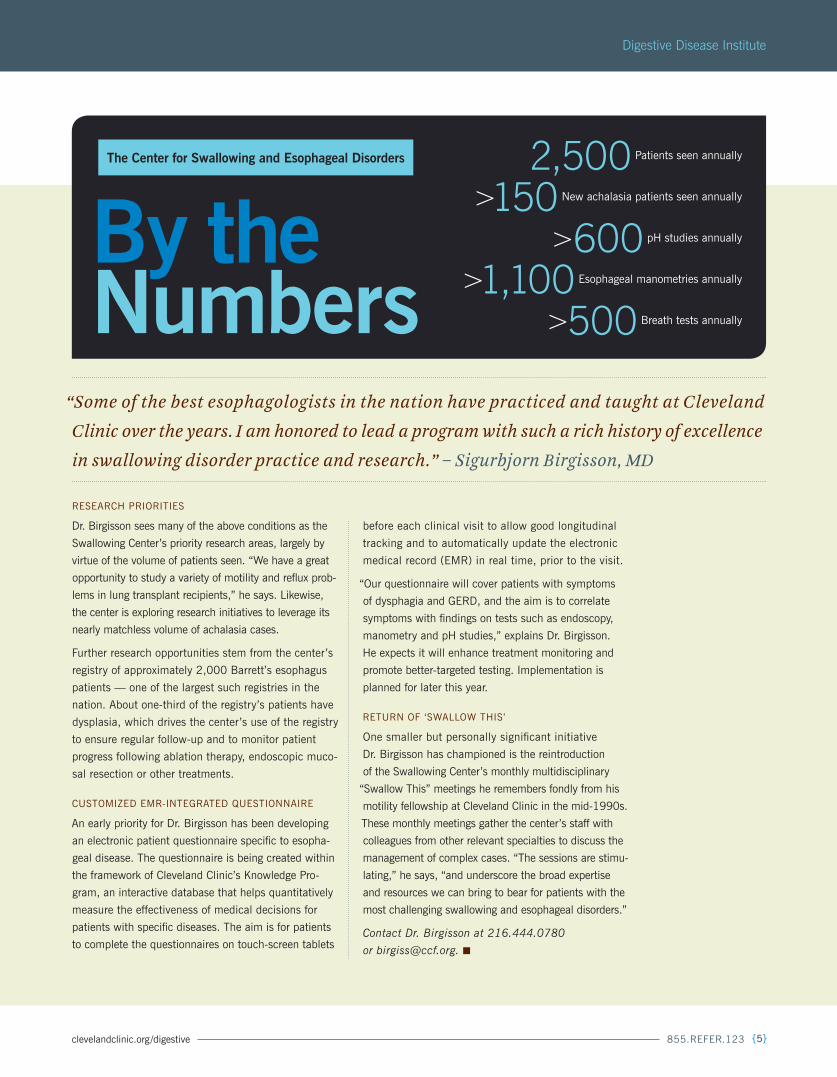
2,500 Patients seen annually
>150 new achalasia patients seen annually
>600 pH studies annually
>1,100 Esophageal manometries annually
>500 Breath tests annually
the Center for swallowing and esophageal disorders
By the numbers
“Some of the best esophagologists in the nation have practiced and taught at Cleveland
Clinic over the years. I am honored to lead a program with such a rich history of excellence
in swallowing disorder practice and research.” – Sigurbjorn Birgisson, MD
{6} digest this Fall | 2012
Cleveland Clinic
pancreatic cyst registry Helps patients avoid surgeryRegistry-based protocol guides cyst management when there is no initial indication of cancer.
r. Matthew Walsh, MD, Department chair of general surgery, began compiling a registry
of pancreatic cysts 12 years ago to help differentiate patients with cancer risk from those
with no indications of risk. today, the registry contains more than 1,500 cases, making it
one of the largest such registries in the world.
“Pancreatic cysts have become a major clinical issue,”
says Dr. Walsh, who has a special interest in biliary,
pancreatic and gastrointestinal surgery. “There has
been a huge explosion in their detection, largely due
to improved imaging. About 15 to 20 percent of the
population could develop these cysts at some point,
often later in life.”
A MoRE SELECTIvE APPRoACH To RESECTIon
Cleveland Clinic was the first institution to study these
patients in detail, and its findings have helped change
the way pancreatic cysts are managed worldwide.
“Previously, the perception was that all cysts had to be
removed due to the presumed high likelihood that they
would eventually lead to pancreatic cancer,” Dr. Walsh says.
However, because surgery has about a 2 percent
mortality rate and a 40 percent morbidity rate, iden-
tifying patients who don’t need surgery is important,
especially because patients with cysts often have no
symptoms and should not be subjected to the risks
of surgery, he says.
“By accurately identifying the type of cyst at an early
stage, we can determine which patients require resec-
tion and which can be safely observed,” he explains.
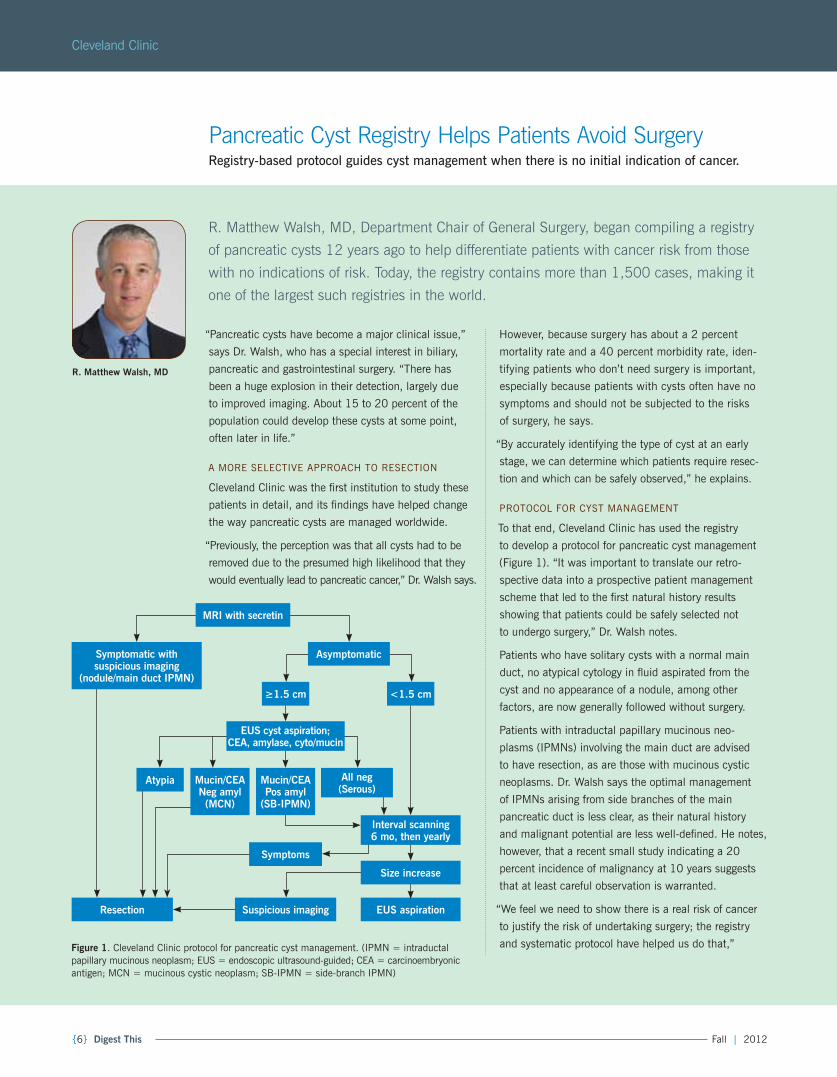
PRoToCoL FoR CyST MAnAgEMEnT
To that end, Cleveland Clinic has used the registry
to develop a protocol for pancreatic cyst management
(Figure 1). “It was important to translate our retro-
spective data into a prospective patient management
scheme that led to the first natural history results
showing that patients could be safely selected not
to undergo surgery,” Dr. Walsh notes.
Patients who have solitary cysts with a normal main
duct, no atypical cytology in fluid aspirated from the
cyst and no appearance of a nodule, among other
factors, are now generally followed without surgery.
Patients with intraductal papillary mucinous neo-
plasms (IPMns) involving the main duct are advised
to have resection, as are those with mucinous cystic
neoplasms. Dr. Walsh says the optimal management
of IPMns arising from side branches of the main
pancreatic duct is less clear, as their natural history
and malignant potential are less well-defined. He notes,
however, that a recent small study indicating a 20
percent incidence of malignancy at 10 years suggests
that at least careful observation is warranted.
“We feel we need to show there is a real risk of cancer
to justify the risk of undertaking surgery; the registry
and systematic protocol have helped us do that,”
R. Matthew Walsh, Md
symptoms
Resection eus aspiration
MRI with secretin
Asymptomatic
≥1.5 cm <1.5 cm
eus cyst aspiration; CeA, amylase, cyto/mucin
symptomatic with suspicious imaging
(nodule/main duct IPMn)
Atypia All neg (serous)
Mucin/CeA Pos amyl
(sB-IPMn)
Mucin/CeA neg amyl
(MCn)
Interval scanning 6 mo, then yearly
size increase
suspicious imaging
Figure 1. Cleveland Clinic protocol for pancreatic cyst management. (IPMn = intraductal papillary mucinous neoplasm; EUS = endoscopic ultrasound-guided; CEA = carcinoembryonic antigen; MCn = mucinous cystic neoplasm; SB-IPMn = side-branch IPMn)
clevelandclinic.org/digestive 855.REFER.123 {7}
Digestive Disease Institute
he explains. “Too many patients had surgery in the
past because they erroneously thought they were at
high risk for cancer.”
Dr. Walsh acknowledges that the protocol is subject
to constant revision, but he notes it has held up well
over time. of the patients
identified for observation,
only about 10 percent
have eventually gone on
to need surgery.
Prior to the registry-based
protocol, almost all pa-
tients with pancreatic cysts
would have been advised
to undergo surgery. Today,
using cyst size as one vari-
able, only 16 percent of
cysts smaller than 3 cm are recommended for
resection. That proportion rises to 50 percent
for cysts larger than 3 cm.
PATIEnTS CRAvE gUIDAnCE
The protocol has been developed in conjunction with
Cleveland Clinic gastroenterologists, who obtain the
fluid samples in these patients (Figure 2). Patients
travel from all over the country to be seen in the
pancreatic clinic held weekly by Dr. Walsh and
gastroenterologist Tyler Stevens, MD.
“Patients often don’t know what to do when they learn
they have a pancreatic cyst, and clearly many are
concerned that they harbor
a diagnosis of pancreatic
cancer,” Dr. Walsh says. “It
is a high-referral diagnosis.”
Some will still want sur-
gery, even if their risk signs
indicate otherwise. Family
history of pancreatic cancer
is often a motivating factor.
“We talk with them about
all the risks, and sometimes
we agree with them,” Dr. Walsh says. “Education is
very important with these patients.”
Moving forward, Dr. Walsh hopes to preserve more
cystic fluid obtained from patients for evaluation
as more sophisticated testing technology emerges,
including proteomics-based assessment.
Dr. Walsh can be contacted at 216.445.7576
or [email protected]. ■
Figure 2. Ultrasound image of a pancreatic cyst being aspirated.
“We need to show there is a
real risk of cancer to justify the
risk of undertaking surgery; the
registry and systematic protocol
have helped us do that.”
– R. Matthew Walsh, MD
16% The proportion of pancre-
atic cysts smaller than 3 cm
recommended for resection
under the Cleveland Clinic
registry-based protocol

{8} digest this Fall | 2012
Genetics-related investigations increasingly figure at the center of the research
enterprise in cleveland clinic’s Digestive Disease institute. these studies are using
genetic information for everything from understanding causes of disease risk to earlier
disease detection to predicting recurrence and individual response to therapies.
We checked in with three clinician researchers from
across the Institute with significant genetic research
initiatives under way or recently published. Their
stories illustrate how our genetics-related studies
are contributing to the understanding of a range of
digestive diseases — and how they are starting to
change clinical practice.
In PURSUIT oF PERSonALIzED MEDICInE
In CoLoRECTAL CAnCER
A hotbed of genetics research within the Institute is
the Colorectal Cancer Translational Science Research
Laboratory, directed by colorectal surgeon Matthew
kalady, MD.
Colon and rectal cancers are a natural for genetic re-
search, says Dr. kalady, in view of their clinical hetero-
geneity and the fact that their prognosis and outcomes
are determined by underlying molecular and genetic
changes. “our lab uses advanced high-throughput tech-
nology and analysis to develop gene signature profiles
to predict colorectal cancer recurrence and response to
therapies,” he notes. “These types of studies are steps
on the path toward personalized medicine.”
one recent contribution along that path came in a
national Cancer Institute-supported multicenter study
published in Science (2012;336[6082]:736-739) in
May. Dr. kalady collaborated with colleagues from other
institutions for this study that identified variant enhancer
loci (vELs), or “master switches” that control key genes
whose altered expression is defining for colon cancer.
“vELs seem to distinguish colon cancer from normal
colon,” Dr. kalady explains. “They are unique, previ-
ously unidentified factors.” The study’s broad findings
suggest that individual differences within vELs may
exert important influences on individuals’ differing
susceptibilities to colon cancer.
cOver Feature

clevelandclinic.org/digestive 855.REFER.123 {9}
This recent vELs work dovetails with other gene signa-
ture profiling projects from Dr. Kalady’s lab, some with
more near-term clinical implications:
Prediction of recurrent rectal cancer. Dr. kalady’s
lab recently identified a particular gene signature as-
sociated with recurrence of early-stage rectal cancer
(J Am Coll Surg. 2010;211[2]:187-195). now his
team is working to validate its finding in a larger
set of patients so that the signature can be applied
to practice and tested in clinical trials. “About 20
percent of patients with stage I or II rectal cancer are
at risk for recurrent disease,” he says. “We hope to
use this tumor gene expression profile to identify and
target these patients with additional therapy after
surgery to reduce their risk of recurrence.”
Linking mutations with outcomes. Earlier this year the
kalady lab showed that mutations in the BRAF onco-
gene are associated with distinct clinical characteris-
tics and with significantly worse survival in colorectal
cancer (Dis Colon Rectum. 2012;55[2]:128-133).
“This gene has been known to be mutated in colorectal
cancer,” Dr. kalady says. “We examined the impact of
the mutation in a large series of patients and demon-
strated a difference in clinical outcome.”
enhanced cancer staging accuracy. In June the lab
published results showing that distinct gene expres-
sion signatures from primary rectal cancers can help
determine the presence or absence of lymph node
metastasis (Dis Colon Rectum. 2012;55[6]:628-
639). “We’ve identified a signature that seems to
have fairly high accuracy in predicting lymph node
involvement by analyzing tissue from the primary
tumor,” Dr. kalady says. “Lymph node involvement
is one of the most important determinants that guide
preoperative therapy, a decision that must be made
before we have definitive pathologic staging. Tradi-
tional means of preoperative staging are only about
70 to 80 percent accurate in predicting node positivity.
This more objective staging tool can help inform the
management approach to the tumor.”
Predicting response to chemoradiation. Drawing on
the Department of Colorectal Surgery’s large tumor
bank, the lab is using total genome sequencing to
evaluate factors associated with complete response
to preoperative chemoradiation for rectal cancer. “By
isolating RnA from tumor samples collected before
chemoradiation treatment, we are working to identify
key pathways that promote tumor killing or tumor
resistance,” Dr. kalady explains. Statistical evaluation
of these results may help identify which patients will
benefit most from chemoradiation, as 15 to 20 per-
cent of patients have complete tumor regression after
chemoradiation. This work may also ultimately guide
Clinician Investigators Share How Their Genetic Studies Are Already Shaping Digestive Disease Practice
in their genes:
“Using our genetic studies, we have uncovered unique interactions between colorectal
cancer cells and surrounding cells, and we’ve identified novel targets for intervention
that may inhibit cancer cell growth.” — Matthew Kalady, MD
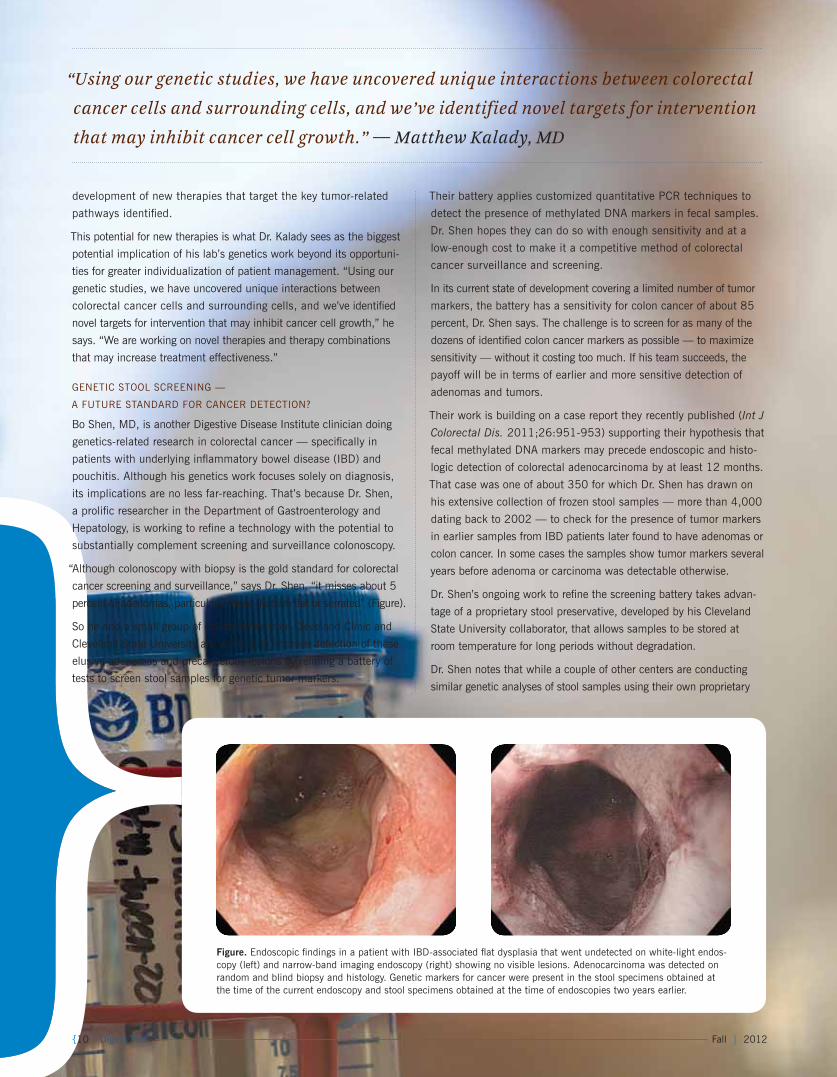
Figure. Endoscopic findings in a patient with IBD-associated flat dysplasia that went undetected on white-light endos-copy (left) and narrow-band imaging endoscopy (right) showing no visible lesions. Adenocarcinoma was detected on random and blind biopsy and histology. genetic markers for cancer were present in the stool specimens obtained at the time of the current endoscopy and stool specimens obtained at the time of endoscopies two years earlier.
development of new therapies that target the key tumor-related
pathways identified.
This potential for new therapies is what Dr. kalady sees as the biggest
potential implication of his lab’s genetics work beyond its opportuni-
ties for greater individualization of patient management. “Using our
genetic studies, we have uncovered unique interactions between
colorectal cancer cells and surrounding cells, and we’ve identified
novel targets for intervention that may inhibit cancer cell growth,” he
says. “We are working on novel therapies and therapy combinations
that may increase treatment effectiveness.”
gEnETIC STooL SCREEnIng —
A FUTURE STAnDARD FoR CAnCER DETECTIon?
Bo Shen, MD, is another Digestive Disease Institute clinician doing
genetics-related research in colorectal cancer — specifically in
patients with underlying inflammatory bowel disease (IBD) and
pouchitis. Although his genetics work focuses solely on diagnosis,
its implications are no less far-reaching. That’s because Dr. Shen,
a prolific researcher in the Department of Gastroenterology and
Hepatology, is working to refine a technology with the potential to
substantially complement screening and surveillance colonoscopy.
“Although colonoscopy with biopsy is the gold standard for colorectal
cancer screening and surveillance,” says Dr. Shen, “it misses about 5
percent of adenomas, particularly those that are flat or serrated” (Figure).
So he and a small group of collaborators from Cleveland Clinic and
Cleveland State University are working to improve detection of these
elusive adenomas and precancerous lesions by refining a battery of
tests to screen stool samples for genetic tumor markers.
Their battery applies customized quantitative PCR techniques to
detect the presence of methylated DnA markers in fecal samples.
Dr. Shen hopes they can do so with enough sensitivity and at a
low-enough cost to make it a competitive method of colorectal
cancer surveillance and screening.
In its current state of development covering a limited number of tumor
markers, the battery has a sensitivity for colon cancer of about 85
percent, Dr. Shen says. The challenge is to screen for as many of the
dozens of identified colon cancer markers as possible — to maximize
sensitivity — without it costing too much. If his team succeeds, the
payoff will be in terms of earlier and more sensitive detection of
adenomas and tumors.
Their work is building on a case report they recently published (Int J
Colorectal Dis. 2011;26:951-953) supporting their hypothesis that
fecal methylated DnA markers may precede endoscopic and histo-
logic detection of colorectal adenocarcinoma by at least 12 months.
That case was one of about 350 for which Dr. Shen has drawn on
his extensive collection of frozen stool samples — more than 4,000
dating back to 2002 — to check for the presence of tumor markers
in earlier samples from IBD patients later found to have adenomas or
colon cancer. In some cases the samples show tumor markers several
years before adenoma or carcinoma was detectable otherwise.
Dr. Shen’s ongoing work to refine the screening battery takes advan-
tage of a proprietary stool preservative, developed by his Cleveland
State University collaborator, that allows samples to be stored at
room temperature for long periods without degradation.
Dr. Shen notes that while a couple of other centers are conducting
similar genetic analyses of stool samples using their own proprietary
{10} digest this Fall | 2012
preservatives, his team’s quantitative PCR technique has achieved
the greatest sensitivity for cancer detection to date. He also believes
his team’s technique has cost advantages. “We are at the forefront in
sensitivity, and our technique is considered to be cost-effective, which
is key to being competitive with colonoscopy,” he says.
Indeed, he sees this screening of stool samples for genetic markers as
a serious competitor to colonoscopy within the next five to 10 years,
especially in populations at risk for inflammation-induced colorectal
cancer, like the IBD patients he often manages. He says that while some
gastroenterologists may not initially welcome the threat to colonoscopy
fees, patient benefits (earlier detection and avoiding the discomforts of
colonoscopy) will ultimately prevail, especially because they align with
the imperative for healthcare cost control.
Meanwhile, Dr. Shen’s team continues to perfect its stool-screening
battery while it applies for nIH grant funding as well as venture capi-
tal investment to conduct a large clinical trial of the battery.
LoCATIng A kEy PIECE oF THE ULCERATIvE CoLITIS PUzzLE
While Dr. Shen pursues his work to genetically detect a potential
complication of IBD — colon cancer — one of his Department of
gastroenterology and Hepatology colleagues, Jean-Paul Achkar, MD,
who holds the kenneth Rainin Endowed Chair in IBD Research, is
working to unravel key genetic risks that predispose patients to the
development of IBD.
“When genetic studies in IBD began over 20 years ago, it was pre-
dicted that there would be only a small number of genes implicated
in causing IBD,” says Dr. Achkar. “However, to date, 163 genes have
been associated with IBD — some only with ulcerative colitis, some
only with Crohn’s disease and some common to both diseases. So
what’s been found has far exceeded what was expected. That un-
derscores the complexity of the genetics of IBD and has led to some
uncertainty about where to go from here with all these genes.”
one point that was clear amid the uncertainty was that the HLA
locus on chromosome 6 was likely to be important in the genetics
of IBD and other inflammatory conditions, as it contains multiple
immune-related genes. “But it has been extremely difficult to pinpoint
a specific gene, let alone a specific abnormality within it, to explain
some of the association with that locus, due to the multiple, closely
positioned genes in that region,” Dr. Achkar says.
So he and the head of the IBD group in Cleveland Clinic’s Lerner Re-
search Institute, Claudio Fiocchi, MD, recently teamed with researchers
from the University of Pittsburgh, led by Richard Duerr, MD, to better
define where the signal for association with IBD was coming from.
They performed genotyping of DnA samples collected at Cleveland
Clinic and the University of Pittsburgh from more than 500 patients
with ulcerative colitis, 600 patients with Crohn’s disease and 1,400
controls and analyzed over 10,000 single nucleotide polymorphisms
across the HLA region. Then, in collaboration with researchers from
Brigham and Women’s Hospital, Carnegie Mellon University and the
University of Pittsburgh, they applied sophisticated imputation and
association techniques to test further genetic and amino acid variants
across the HLA locus. In a paper published online in December 2011
(Genes Immun. 2012;13[3]:245-252), they confirmed the suspicion
that variation in the HLA-DRβ1 gene was strongly related to ulcer-
ative colitis. More notably, they identified a very specific defect in this
gene — a variation at amino acid position 11 — as being strongly
associated with the risk of developing ulcerative colitis. This position
is in a crucial binding pocket likely to have significant influence on
immune response to antigens.
“There are certainly other genes and defects involved in ulcerative
colitis, but this one appears to be one of the big players in driving risk
for the disease,” says Dr. Duerr.
Dr. Achkar adds that the finding is significant for two reasons: “First,
it ties in nicely with theories of abnormal immune response being
triggered by responses to certain antigens. Second, since it opens the
potential to better understand how the body responds to antigens, it
could certainly help lead to different approaches to treatment or to
altering the immune system.”
After this paper was published, another study implicated the exact
same amino acid position as an important cause of rheumatoid ar-
thritis (Nat Genet. 2012;44[3]:291-298). “This independent finding
in another immune-mediated disease is a nice validation of our study,”
Dr. Achkar says. “It confirms that something important is going on at
this position.”
Dr. Kalady can be contacted at 216.445.2655 or [email protected];
Dr. Shen at 216.444.9252 or [email protected]; and Dr. Achkar at
216.444.6513 or [email protected]. ■
Matthew Kalady, Md: Profiling gene signatures to personalize colorectal cancer management.
Bo shen, Md: Refining a screening battery for cancer markers in stool samples.
Jean-Paul Achkar, Md (front), with colleague Claudio Fiocchi, Md: Working to unravel the genetics of IBD.
clevelandclinic.org/digestive 855.REFER.123 {11}
{12} digest this Fall | 2012
Cleveland Clinic
laparoscopic right Hepatectomy eases patient recoveryMultidisciplinary surgical oncology approach offers best chance for cure with smooth recovery.
case stuDy
DECEMBER 2011
A 51-year-old man is referred to Eren Berber, MD, at
Cleveland Clinic for management of liver metastases
from colorectal cancer. He had been diagnosed with co-
lon cancer with synchronous liver and pulmonary metas-
tases and had resection of his colonic primary in october
2010. He was started on the FoLFox chemotherapy
regimen and bevacizumab until September 2011, with
resolution of pulmonary metastases. This was followed
by the FoLFIRI chemotherapy regimen and cetuximab.
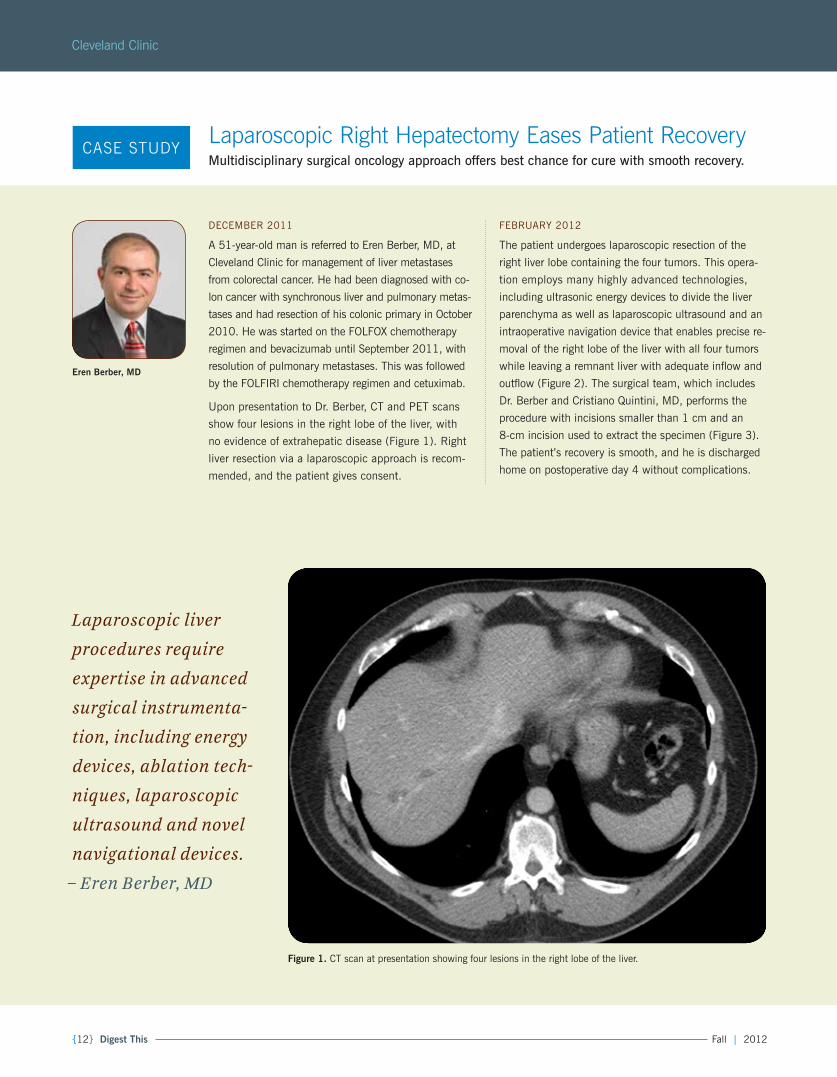
Upon presentation to Dr. Berber, CT and PET scans
show four lesions in the right lobe of the liver, with
no evidence of extrahepatic disease (Figure 1). Right
liver resection via a laparoscopic approach is recom-
mended, and the patient gives consent.
FEBRUARy 2012
The patient undergoes laparoscopic resection of the
right liver lobe containing the four tumors. This opera-
tion employs many highly advanced technologies,
including ultrasonic energy devices to divide the liver
parenchyma as well as laparoscopic ultrasound and an
intraoperative navigation device that enables precise re-
moval of the right lobe of the liver with all four tumors
while leaving a remnant liver with adequate inflow and
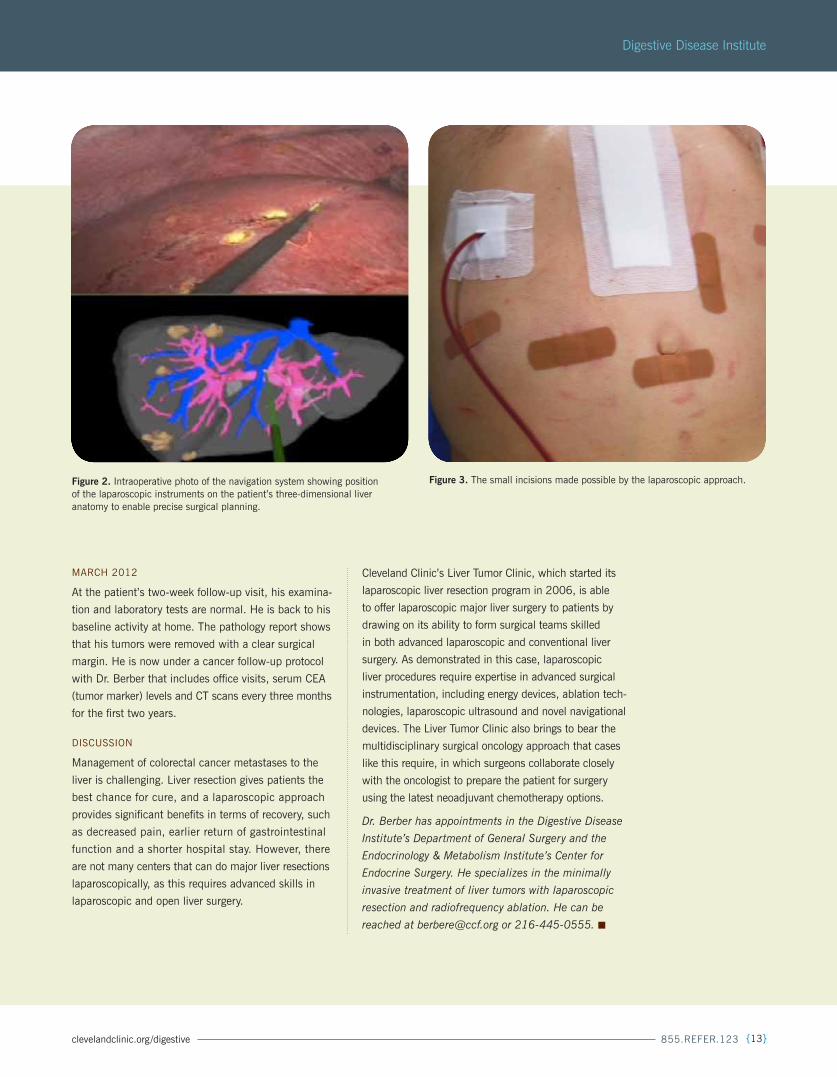
outflow (Figure 2). The surgical team, which includes
Dr. Berber and Cristiano Quintini, MD, performs the
procedure with incisions smaller than 1 cm and an
8-cm incision used to extract the specimen (Figure 3).
The patient’s recovery is smooth, and he is discharged
home on postoperative day 4 without complications.
eren Berber, Md
Figure 1. CT scan at presentation showing four lesions in the right lobe of the liver.
Laparoscopic liver
procedures require
expertise in advanced
surgical instrumenta-
tion, including energy
devices, ablation tech-
niques, laparoscopic
ultrasound and novel
navigational devices.
– Eren Berber, MD
clevelandclinic.org/digestive 855.REFER.123 {13}
Digestive Disease institute
Figure 3. The small incisions made possible by the laparoscopic approach.
MARCH 2012
At the patient’s two-week follow-up visit, his examina-
tion and laboratory tests are normal. He is back to his
baseline activity at home. The pathology report shows
that his tumors were removed with a clear surgical
margin. He is now under a cancer follow-up protocol
with Dr. Berber that includes office visits, serum CEA
(tumor marker) levels and CT scans every three months
for the first two years.
DISCUSSIon
Management of colorectal cancer metastases to the
liver is challenging. Liver resection gives patients the
best chance for cure, and a laparoscopic approach
provides significant benefits in terms of recovery, such
as decreased pain, earlier return of gastrointestinal
function and a shorter hospital stay. However, there
are not many centers that can do major liver resections
laparoscopically, as this requires advanced skills in
laparoscopic and open liver surgery.
Cleveland Clinic’s Liver Tumor Clinic, which started its
laparoscopic liver resection program in 2006, is able
to offer laparoscopic major liver surgery to patients by
drawing on its ability to form surgical teams skilled
in both advanced laparoscopic and conventional liver
surgery. As demonstrated in this case, laparoscopic
liver procedures require expertise in advanced surgical
instrumentation, including energy devices, ablation tech-
nologies, laparoscopic ultrasound and novel navigational
devices. The Liver Tumor Clinic also brings to bear the
multidisciplinary surgical oncology approach that cases
like this require, in which surgeons collaborate closely
with the oncologist to prepare the patient for surgery
using the latest neoadjuvant chemotherapy options.
Dr. Berber has appointments in the Digestive Disease
Institute’s Department of General Surgery and the
Endocrinology & Metabolism Institute’s Center for
Endocrine Surgery. He specializes in the minimally
invasive treatment of liver tumors with laparoscopic
resection and radiofrequency ablation. He can be
reached at [email protected] or 216-445-0555. ■
Figure 2. Intraoperative photo of the navigation system showing position of the laparoscopic instruments on the patient’s three-dimensional liver anatomy to enable precise surgical planning.

{14} digest this Fall | 2012
Cleveland Clinic
cirrhosis-related sarcopenia:Cleveland Clinic Researcher Advances Management of a Major but Neglected Complication
A hepatologist in Cleveland Clinic’s Digestive Disease Institute is the recipient of the first
u.s. research grant for studying the molecular mechanisms of malnutrition and muscle
loss in cirrhosis, but he’s not preoccupied with that distinction. in fact, he wishes he
had more fellow grant awardees in this field. “Allocation of more resources to examine
malnutrition in cirrhosis is critically needed,” explains Srinivasan Dasarathy, MD.
That’s because malnutrition in cirrhosis results in
sarcopenia, or loss of skeletal muscle mass, the most
common complication of cirrhosis. Because cirrhosis
is widespread, affecting an estimated 2.5 million U.S.
residents, cirrhosis-related sarcopenia confers a large
clinical burden. Sarcopenia reduces both survival and
quality of life in cirrhotic patients, and it is a major
contributor to other complications of cirrhosis, such
as encephalopathy, ascites and portal hypertension.
It also worsens outcomes after liver transplantation.
“Sarcopenia affects every phase of liver disease,” says
Dr. Dasarathy, a clinician-researcher in the Depart-
ment of gastroenterology and Hepatology with joint
appointments in the Transplant Center and the De-
partment of Pathobiology.
Despite these impacts, there are no effective thera-
pies for sarcopenia of cirrhosis, largely because its
mechanisms are not yet known. This is the result of
a lack of recognition of the condition, scarce research
funding and the dominance of research interest in
aging-related sarcopenia, which is likely to have dif-
ferent mechanisms.
Dr. Dasarathy has been working for more than a
decade to increase understanding of cirrhosis-related
sarcopenia, and his lab has made important advances
in the last few years in both animal and human studies.
THE RoLE oF MyoSTATIn
Dr. Dasarathy’s grant referred to above is a five-year
nIH award to examine the mechanisms of sarcopenia
of cirrhosis using a combination of tracer methodol-
ogy and molecular biology tools both in vivo and with
in vitro cell systems. This work will build on his lab’s
considerable animal research in this field to date,
which includes the first demonstration of the causal
role of the protein myostatin in the reduced skeletal
muscle mass that accompanies cirrhosis (J Hepatol.
2011;54[5]:915-921).
Those animal studies prompted Dr. Dasarathy’s team
to generate a compound called follistatin that blocks
myostatin and its effects on muscle. They used an ani-
mal model to show that follistatin was able to reverse
cirrhosis-related muscle loss without affecting the liver.
Enthusiasm for follistatin is tempered, however, by the
compound’s proliferative effect on cells, which raises
the specter of carcinogenicity.
But Dr. Dasarathy remains undaunted. “There are
certainly ways to generate small-molecule products
that can block myostatin quite specifically, without
follistatin’s effect on other tissues,” he says.
TRAnSLATIon To HUMAnS WELL UnDER WAy
Meanwhile, Dr. Dasarathy’s research team at Cleveland
Clinic is forging ahead with the first human studies
to explore whether large doses of amino acids will
improve muscle mass in cirrhotics.
“We have an ongoing protocol in which we are giving
cirrhotics as well as healthy controls a large dose of
leucine along with other amino acids that cirrhotics
are deficient in,” he says. “We view these amino acids
not as nutrients but rather as signaling molecules, like
drugs that have very specific effects on the down-
stream consequences of myostatin.” Participants un-
dergo muscle biopsy, blood studies, and measurements
of strength and muscle mass before and after the treat-
ment. “The aim is to see if the molecular defects we’ve
identified in human cirrhotic muscle are reversible or
not,” he explains.
srinivasan dasarathy, Md
clevelandclinic.org/digestive 855.REFER.123 {15}
Digestive Disease institute
cirrhosis-related sarcopenia:Cleveland Clinic Researcher Advances Management of a Major but Neglected Complication
So far six cirrhotics and six controls have been evalu-
ated, and preliminary results are “very encouraging,”
says Dr. Dasarathy. His goal is to study 20 cirrhotics
and 20 controls for more definitive results.
Based on its preliminary findings, his lab has been
awarded a grant from the Japanese government to
study precisely how the combination of leucine and
other amino acids is able to prevent and potentially
reverse muscle loss in cirrhosis.
QUESTIonIng ASSUMPTIonS In LIvER TRAnSPLAnT
In a separate human study, Dr. Dasarathy’s team is
doing muscle biopsies in cirrhotic patients before and
after liver transplantation to determine why muscle
mass does not improve — and even declines — follow-
ing transplant. “Transplantation used to be considered
a cure for all cirrhotic complications, but that’s been
found not to be the case for the nutritional complica-
tions,” he notes. “We think sarcopenia may contribute
to impaired quality of life after transplant, and we’d
like to see if we can fix that.”
Fixing or avoiding the effects of sarcopenia — whether
through amino acids or compounds that block the
effects of myostatin overexpression — is the ultimate
goal of Dr. Dasarathy’s research in all cirrhotic patients,
regardless of whether they undergo liver transplant.
“Because loss of muscle mass is nearly universal in
cirrhotics and affects survival, quality of life, other
complications and post-transplant outcomes,” he says,
“reversing sarcopenia has the potential to improve the
life of patients at any stage of liver disease.”
Dr. Dasarathy can be reached at 216.444.2980 or
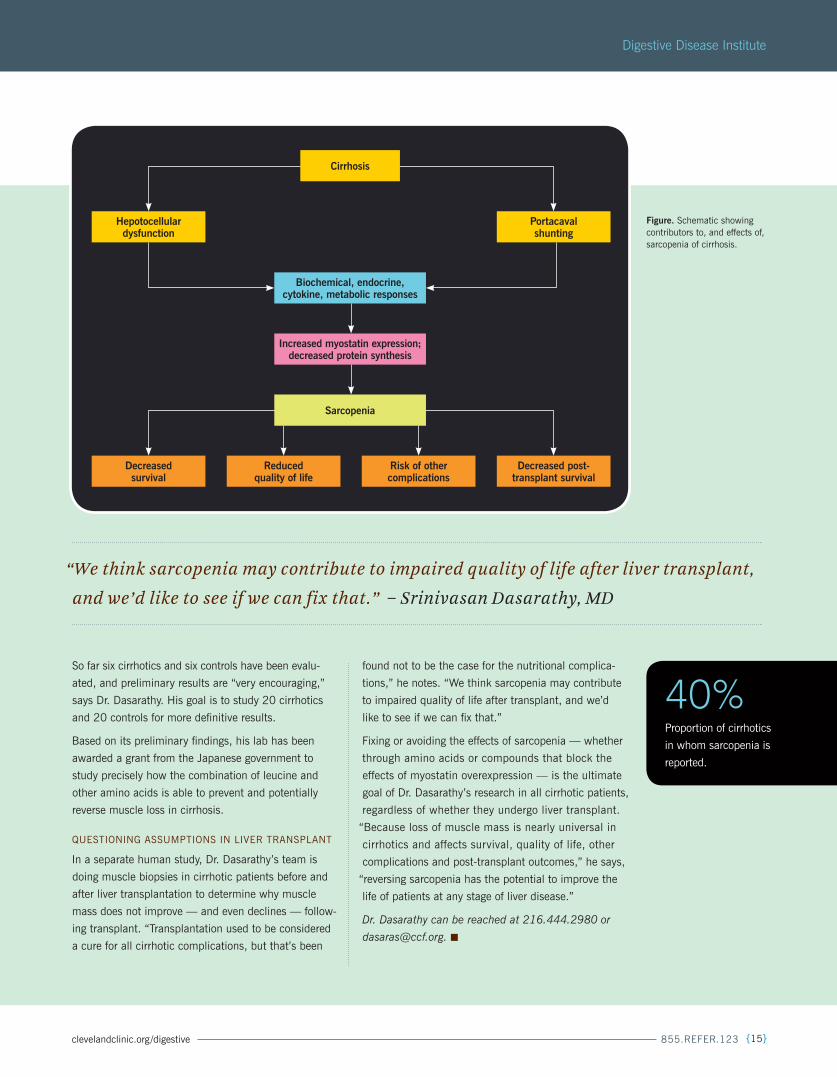
“We think sarcopenia may contribute to impaired quality of life after liver transplant,
and we’d like to see if we can fix that.” – Srinivasan Dasarathy, MD
Biochemical, endocrine, cytokine, metabolic responses
Increased myostatin expression; decreased protein synthesis
decreased survival
Reduced quality of life
Risk of other complications
decreased post- transplant survival
hepotocellular dysfunction
Portacaval shunting
Cirrhosis
sarcopenia
Figure. Schematic showing contributors to, and effects of, sarcopenia of cirrhosis.
40%Proportion of cirrhotics
in whom sarcopenia is
reported.

{16} digest this Fall | 2012
Cleveland Clinic
newstaff}CoLoRECTAL SURgERy
John P. Cullen, Md
Specialty interests: Minimally invasive colorectal surgery, robotic-assisted colorectal surgery, inflammatory bowel disease, Crohn’s disease, ulcerative colitis, colonoscopy, colon and rectal cancer, anal cancer, diverticular disease
Locations: Hillcrest Hospital, Twinsburg Family Health and Surgery Center, Willoughby Hills Family Health Center Office: 440.312.7111
Giovanna da silva, Md
Specialty interests: Laparoscopic surgery, colorectal cancer, ulcerative colitis, Crohn’s disease, diverticulitis, fecal incontinence, benign anorectal diseases
Location: Weston, Fla. Office: 954.659.5278
gASTRoEnTERoLogy AnD HEPAToLogy
Brian Baggott, Md
Specialty interests: Inflammatory bowel disease, gastroenteritis, Barrett’s epithelium, endoscopic mucosal resection
Location: Wooster Milltown Specialty and Surgery Center Office: 330.287.4500
sigurbjorn Birgisson, Md
Specialty interests: Achalasia, Barrett’s esophagus, caustic ingestion, eosinophilic esophagitis, esophageal cancer, esophageal disorders, esophageal varices, esophagitis
Location: Main campus Office: 216.444.0780
Jessica Philpott, Md, Phd
Specialty interest: general gastroenterology
Locations: Main campus, Richard E. Jacobs Health Center (Avon) Office: 216.445.7692
Abdullah shatnawei, Md
Specialty interests: Celiac disease, constipation and fecal incontinence, eosinophilic esophagitis, esophageal motility disorders, GI endoscopy, gastroesophageal reflux disease, gI motility disorders, H. pylori infection, inflammatory bow-el disease, intestinal transplantation, insulin resistance, malabsorption, enteral and parenteral nutrition, medical education and education of fellows/residents, metabolic syndrome, motility disorders, nutritional problems, obesity, peptic ulcer disease, short bowel syndrome, therapeutic endoscopy including difficult colonoscopy and polypectomy
Location: Main campus Office: 216.445.2301
gEnERAL SURgERy
Kareem Abu-elmagd, Md, Phd
Specialty interests: gut rehabilitation and autologous bowel reconstruction, intestinal and multivisceral trans-plantation, surgery for portomesenteric venous thrombosis, portal hypertensive surgery, complex abdominal surgery, solitary pancreas transplant, islet cell transplant, pediatric abdominal organ transplantation
Location: Main campus Office: 216.444.8292
Kalman Bencsath, Md
Specialty interests: Advanced laparoscopic surgery, hiatal hernia repair, nissen fundoplication, gastric surgery, splenectomy, pancreatic surgery, biliary surgery, hernia repair, general surgery
Locations: Hillcrest Hospital, Twinsburg Family Health and Surgery Center Office: 440.449.1101
Jeffrey s. ustin, Md
Specialty interests: Acute care surgery, trauma, surgical critical care
Locations: Main campus, Hillcrest Hospital Office: 216.445.1977
Jane Wey, Md
Specialty interests: Surgical oncology, hepatobiliary and pancreatic surgery, laparoscopic surgery, metastasectomy, gastrointestinal surgery, gastric cancer, retroperitoneal sar-comas, neuroendocrine tumors, HIPEC (tumor debulking/intraperitoneal chemoperfusion), melanoma, breast cancer
Location: Main campus Office: 216.445.6469
WE WELCoME THE FoLLoWIng SPECIALISTS To THE DIgESTIvE DISEASE InSTITUTE
For a complete listing of Digestive Disease Institute staff, visit clevelandclinic.org /digestive.

CMe Calendar: Medical professionals are invited to attend the following continuing education programs
7th Annual Obesity summit oct. 4-5, 2012 Cleveland Clinic, Cleveland, ohio
Multidisciplinary Breast Cancer summit (including sessions on breast surgery) oct. 11-13, 2012 Cleveland, ohio
16th Annual Meeting of the Collaborative Group of the Americas on Inherited Colorectal Cancer (CGA-ICC) (in joint sponsorship with Cleveland Clinic) oct. 27-29, 2012 Boston, Mass.
47th Annual Gastroenterology update: the next Generation in diagnosis and treatment nov. 8-9, 2012 Cleveland Clinic, Cleveland, ohio
Visit ccfcme.org for more information about the above events and more Cleveland Clinic CMe offerings in digestive disease and other clinical areas.
digestive disease Institute’s International Interdisciplinary education Week
24th Annual Jagelman International Colorectal disease symposium and 34th Annual turnbull symposium Feb. 12-17, 2013 Fort Lauderdale, Fla.
2nd Annual Gastroenterology and hepatology symposium Feb. 14-16, 2013 Fort Lauderdale, Fla.
12th Annual surgery of the Foregut symposium Feb. 17-20, 2013 (with live surgery Feb. 20) Coral gables, Fla.
Visit ClevelandClinicFloridaCMe.org for more information about the above events and more CMe offerings from Cleveland Clinic Florida.
855.REFER.123 for 24/7 referrals and
service assistance from cleveland clinic
The Power of Today: Referring Your Patient to Cleveland Clinic
Cleveland Clinic’s Referring Physician Center has established
a 24/7 hotline for referring physicians and their office staff to
streamline access to our array of medical services. our goal is to
make it as easy as possible for you and your patients when you
entrust us with their care.
you can contact the Referring Physi-
cian Hotline — 855.REFER.123
(855.733.3712) — for informa-
tion on our clinical specialties and
services, to schedule and confirm
patient appointments, for assistance
in resolving service-related issues
and to connect with Cleveland
Clinic specialists.
“We have made physician referrals
a priority,” says James Merlino, MD, Chief Experience Officer.
“We looked at what worked and what didn’t. We collaborated
with referring physicians to develop a one-stop shop for all
their needs. The result is the Referring Physician Center and its
hotline. Today, we’re here 24/7 to give quick service and rapid
resolution of any issues.”
Cleveland Clinic will work with your patient to complete our
registration process and to schedule
an appointment at his or her conve-
nience. You will be notified once the
appointment is scheduled.
“Patients honor and respect their per-
sonal physician,” says Dr. Merlino,
who is also a surgeon in the Diges-
tive Disease Institute’s Department
of Colorectal Surgery. “We realized
that if our referring physicians are
not happy, their patients won’t be
happy. our Referring Physician Center will do whatever it takes
to give all referring physicians and their patients the best out-
come and experience.”
The Referring Physician Hotline can be reached 24 hours a day, 7 days a week, at 855.REFER.123 (855.733.3712).
Digestive Disease InstituteThe Cleveland Clinic Foundation9500 Euclid Avenue/AC311Cleveland, oH 44195
24/7 referralsreferring physician Hotline 855.REFER.123 (855.733.3712)
Hospital transfers 800.553.5056
On the Web at: clevelandclinic.org/refer123
stay connected with us on…
Referring Physician Center and hotlineCleveland Clinic’s Referring Physician Center has established a 24/7 hotline — 855.REFER.123 (855.733.3712) — to streamline access to our array of medical services. Contact the Referring Physician Hotline for information on our clini-cal specialties and services, to schedule and confirm patient appointments, for assistance in resolving service-related issues, and to connect with Cleveland Clinic specialists.
Physician directoryview all Cleveland Clinic staff online at clevelandclinic.org/staff.
track Your Patient’s Care OnlineDrConnect is a secure online service providing real-time information about the treatment your patient receives at Cleveland Clinic. Establish a DrConnect account at clevelandclinic.org/drconnect.
Critical Care transport WorldwideCleveland Clinic’s critical care transport teams and fleet of vehicles are available to serve patients across the globe.
• To arrange for a critical care transfer, call 216.448.7000 or 866.547.1467 (see clevelandclinic.org/criticalcaretransport).
• For STEMI (ST elevated myocardial infarction), acute stroke, ICH (intracerebral hemorrhage), SAH (subarachnoid hemorrhage) or aortic syndrome transfers, call 877.379.COde (2633).
Outcomes dataview clinical outcomes Books from all Cleveland Clinic institutes at clevelandclinic.org/outcomes.
Clinical trialsWe offer thousands of clinical trials for qualifying patients. visit clevelandclinic.org/clinicaltrials.
CMe Opportunities: Live and OnlineThe Cleveland Clinic Center for Continuing Education’s website offers convenient, complimentary learning oppor-tunities. visit ccfcme.org to learn more, and use Cleveland Clinic’s myCME portal (available on the site) to manage your CME credits.
executive educationCleveland Clinic has two education programs for healthcare executive leaders — the Executive visitors’ Program and the two-week Samson global Leadership Academy immer-sion program. visit clevelandclinic.org/executiveeducation.
about cleveland clinicCleveland Clinic is an integrated healthcare delivery system with local, national and international reach. At Cleveland Clinic, 2,800 physicians represent 120 medical special-ties and subspecialties. We are a main campus, 18 family health centers, eight community hospitals, Cleveland Clinic Florida, the Cleveland Clinic Lou Ruvo Center for Brain Health in Las vegas, Cleveland Clinic Canada, Sheikh khalifa Medical City, and Cleveland Clinic Abu Dhabi.
In 2012, Cleveland Clinic was ranked one of America’s top 4 hospitals in U.S. News & World Report’s annual “Amer-ica’s Best Hospitals” survey. The survey ranks Cleveland Clinic among the nation’s top 10 hospitals in 14 specialty areas, and the top hospital in three of those areas.
RESoURCES FoR PHyS IC IAnS
CLEvELAnD CLInIC #2 In THE U.S. – GAstROenteROLOGY