Embed Size (px)
Citation preview

Endocrine-RelatedCancer
ReviewC Durante et al. DTC follow-up 20 :4 R141–R154
Differentiated thyroid carcinoma:defining new paradigms forpostoperative management
Cosimo Durante, Giuseppe Costante1,2 and Sebastiano Filetti
Department of Internal Medicine and Medical Specialties, University of Rome ‘Sapienza’, Viale del Policlinico 155,
00161 Rome, Italy1Department of Internal Medicine, Institute Jules Bordet, 1000 Bruxelles, Belgium2Department of Health Sciences, University of Catanzaro ‘Magna Graecia’, 88100 Catanzaro, Italy
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
Published by Bioscientifica Ltd.
Downloa
Correspondence
should be addressed
to S Filetti
Abstract
The demography of differentiated thyroid cancers (DTCs) has changed considerably since the
1990s, when the vast majority of these tumors were clinically evident at the time of
diagnosis, and many were associated with regional lymph node involvement. Today’s DTCs
are more likely to be small, localized, asymptomatic papillary forms that are discovered
incidentally, during neck imaging procedure performed for other reasons or during
postoperative assessment of a gland removed for benign nodular goiter. The tools available
for diagnosing, treating, and monitoring DTCs have also changed and their diagnostic
capacities have increased. For these reasons, DTC treatment and follow-up paradigms are
being revised to ensure more appropriate, cost-effective management of the current
generation of DTCs. This review examines some of the key issues in this area, including the
assessment of risks for disease recurrence and thyroid cancer-related death, the indications
for postoperative ablation of the thyroid remnant with radioactive iodine and TSH-
suppressive doses of levothyroxine, the pros, cons, and rationales for the use of various
follow-up tools (serum thyroglobulin assays, neck ultrasound, 2-[18F]fluoro-2-deoxyglu-
cose–positron emission tomography, and whole-body 131I scintigraphy), and temporal
strategies for maximizing their efficacy. An algorithm is presented for individualized,
risk-tailored management of DTC patients.
Key Words
" differentiated thyroidcarcinoma
" radioiodine remnant ablation
" follow-up
" neck ultrasound
" thyroglobulin
" recurrence
ded
Endocrine-Related Cancer
(2013) 20, R141–R154
Introduction
The incidence of thyroid cancer has been increasing
steadily since the 1970s. Data from the Surveillance
Epidemiology and End Results Registries show an average
annual increase in the USA of 6.6% between 1997 and
2009. The estimated number of patients with thyroid
cancer on January 1, 2009, was almost half a million, and
roughly three out of four of these individuals were women
(http://seer.cancer.gov/statfacts/html/thyro.html; last
accessed 20 January 2013). These tumors are fifth on the
list of the most common incident cancers among women,
and they represent the most rapidly growing category of
cancer in both sexes (Eheman et al. 2012).
This trend is almost entirely the result of increases in
the diagnosis of differentiated thyroid cancers (DTCs), the
papillary type, in particular (Incidence rates of follicular
thyroid cancers – like those of the poorly differentiated
anaplastic and medullary forms – have remained relatively
stable over the past 20–30 years.). DTC treatment and
follow-up practices were developed on the basis of experi-
ence gained during the latter half of the 20th century.
from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R142
During those years, papillary thyroid cancers (PTCs) were
almost always clinically evident at the time of presen-
tation, and a substantial number were associated
with regional lymph node involvement (DeGroot 1994,
Mazzaferri & Jhiang 1994). Today, the vast majority of
newly detected PTCs are small, localized, asymptomatic
tumors that are discovered incidentally (e.g. during
imaging studies of the neck performed for other reasons
or postoperatively, after thyroid gland removal for benign
nodular goiter; Leenhardt et al. 2004, Davies & Welch
2006, Hall et al. 2009). The tools at our disposal for
diagnosing, treating, and monitoring PTCs have also
changed and evolved over the past two decades (Table 1;
Cooper et al. 2009). The challenge facing us today is the
need to revise treatment and follow-up paradigms in light
of more recent evidence to ensure more appropriate, cost-
effective management of the current generation of DTCs.
This review examines some of the key issues in this
area, including the accurate assessment of risks for disease
recurrence and thyroid-cancer-related death, the indi-
cations for postoperative ablation of the thyroid remnant
with radioactive iodine, the pros and cons of various
follow-up tools, and temporal strategies for maximizing
their efficacy. Finally, an algorithm is presented for
individualized, risk-tailored management of DTC patients.
Tailoring management to risk
Given the changes that have occurred in the demography
of DTC patients, accurate risk stratification of the current
patient population is an essential first step toward
improved treatment and follow-up protocols. For patients
with DTCs, risk assessment provides the foundation for
informed, evidence-based choices regarding subsequent
management, including the administration of radioactive
iodine after surgery, the use of TSH suppression, the
strategies and methods that will be used to detect the signs
of disease recurrence, and the frequency, intensity, and
duration of the follow-up. Tailoring management
strategies to individual risk can increase the cost-
effectiveness of care and in many cases improve the
patient’s quality of life, by reducing the burden of
adverse treatment effects and the stress and costs of
ongoing surveillance.
Reliable assessment of the risks faced by an individual
patient with DTC requires the use of the right tool at the
right time during follow-up. The initial evaluation occurs
when the cancer is diagnosed and, in all probability,
surgically removed. Staging at this point is conventionally
based on the clinicopathologic system elaborated by the
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
American Joint Cancer Committee/Union Internationale
Contre le Cancer (AJCC/UICC), which is widely used for
all types of cancers. It is based on four variables: patient
age, the size and extension of the primary tumor (pT),
lymph node involvement (N), and the presence of distant
metastases (M).
Both the American Thyroid Association (ATA)
Practice Guidelines (Cooper et al. 2009) and the European
Thyroid Association (ETA) Consensus Statement (Pacini
et al. 2006) endorse the AJCC/UICC staging system for use
in patients with DTCs. The main problem with this
approach is that the system was designed to predict
mortality (Brierley et al. 1997, Orlov et al. 2009), whereas
clinicians planning focused follow-ups also need infor-
mation on the probability of persistent or recurrent disease
after surgery. When the AJCC/UICC system was tested in
DTC patients to see how well it predicted structural disease
recurrence during follow-up, stage IV disease was clearly
associated with the highest risk (70%), but the increase
in risk across stages I, II, and III was anything but linear
(11, 34, and 14% respectively; Tuttle et al. 2010).
The solution proposed by the ATA in its 2009
guidelines was a new system, which classifies the
probability of recurrence as high, intermediate, or low
(Table 2; Cooper et al. 2009) on the basis of pTNM
parameters plus other types of information that are
generally available shortly after the initial treatment (i.e.
thyroidectomy or lobectomy, with or without radioiodine
therapy). The latter variables include tumor histotype,
evidence of vascular invasion, the completeness of the
surgical intervention, and the results of the post-treatment
whole-body radioiodine scan (RxWBS). As expected, the
ATA system has proved to be more effective in predicting
the follow-up findings of persistent or recurrent cancer. In
a cohort of 588 patients with DTC followed at the
Memorial Sloan-Kettering Cancer Center for a median of
7 years after primary treatment, the likelihood of detecting
structural disease during the surveillance period increased
progressively with the risk level: from w3% in low-risk
patients to 21% in those with an intermediate-risk and
68% for those assigned to the high-risk category (Tuttle
et al. 2010).
Even the ATA risk assessment system, however, has
some intrinsic limitations. Little distinction is made
between PTCs and follicular thyroid cancers (FTCs),
which usually demonstrate different biological behaviors.
For instance, for FTCs, the presence of vascular invasion
appears to be the major determinant of risk. Thus, the
so-called minimally invasive follicular thyroid cancers,
which are characterized histologically by tumor capsule
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Table 1 Paradigm shifts in the management of differentiated thyroid cancers.
Old paradigms Current paradigmsa Future paradigms
What is the appropriateoperation for DTCs?
Total thyroidectomyGnecklymph node dissection
Lobectomy (very low-riskpatients)
Depending on the preoperativeestimates of the risk
Total thyroidectomyGnecklymph node dissection
Which patients should undergoRAI remnant ablation?
All patients Selectedb intermediate-riskpatients
Patients with postoperativeevidence of disease (and ahigh risk of persistentdisease?)
High-risk patientsWhich patients should receive
TSH suppression therapy andhow much suppression isappropriate?
All patients (target TSH:!0.1 mU/l)
Early follow-upc Patients with postoperativeevidence of disease (and ahigh risk of persistentdisease?)
Low-risk patients (target TSH:0.1–0.5 mU/l)
Intermediate- and high-riskpatients (target TSH:!0.1 mU/l)
Long-term follow-upHigh-risk patients (target TSH:0.1–0.5 mU/l, for 5–10 years)
Patients with persistentdisease (target TSH:!0.1 mU/l)
Which diagnostic tools shouldbe used to monitor DTCpatients after the initialtreatment?
DxWBS Early follow-upc Early follow-upc
Assay of serum Tg levels(basal and during TSH stimu-lation achieved with thyroidhormone withdrawal)
Neck US (when available)
Patients treated with RRA Neck USNeck US Long-term follow-upSerum Tg measurement
(rhTSH-stimulated levels ora high-sensitivity assay ofbasal levels)
Serial highly sensitive serumTg assay (trend over time)
DxWBS (high-riskpatients only)
Patients not treated with RRANeck USHigh-sensitivity assay of basal
serum Tg levelsLong-term follow-upNeck USSerial measurements of basalTg with a high-sensitivityassay
How long should DTC patientsbe followed?
Until death Until death Duration determined by therisk of disease recurrence
DTC, differentiated thyroid cancer; DxWBS, diagnostic whole-body scintigraphy; RAI, radioactive iodine; RRA, radioactive iodine remnant ablation; rhTSH,recombinant human TSH; Tg, thyroglobulin; US, ultrasonography.aBased on the most recently published evidence-based international guidelines (Cooper et al. 2009).bThose with higher risk clinicopathological features, such as worrisome histologic subtypes (i.e. tall cell, columnar, insular, and solid variants, as well aspoorly differentiated thyroid cancer); invasion of intrathyroidal vasculature; multifocal disease (gross or microscopic); and non-papillary histology(i.e. follicular thyroid cancer and Hurthle cell cancer with vascular invasion).c1–2 years after the initial treatment.
Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R143
penetration without vascular invasion, are generally
regarded as lower risk tumors, irrespective of the tumor
size (van Heerden et al. 1992, Sanders & Silverman 1998,
D’Avanzo et al. 2004, Lo et al. 2005, Dralle et al. 2013).
Most importantly the ATA risk assessment system fails to
consider two factors that can significantly alter the odds of
recurrence and death over time: the clinical course of the
disease and its response to the initial therapy and any
interventions performed thereafter. To address this
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
shortcoming, the Sloan-Kettering group had previously
proposed a dynamic risk assessment strategy, which
provides for ongoing revision and refinement of the
risk estimate as new data emerge during follow-up
(Tuttle 2008). In the study cited above (Tuttle et al.
2010), the patients originally staged with the ATA
recurrence risk system were subsequently re-assessed on
the basis of treatment–response data obtained during the
first 2 years after the initial therapy (in this case, total
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Table 2 The American Thyroid Association staging system for predicting the risk of disease recurrence/persistence in patients with
differentiated thyroid cancer.
Low-risk Intermediate-risk High-risk
Meets all of the following criteria: Meets at least one of the following criteria: Meets at least one of the following criteria:No aggressive tumor histotype(e.g. tall cell, insular, and columnarcell cancers)
Aggressive tumor histotype or vascularinvasion
Macroscopic extrathyroidal extension ofthe tumor
No vascular invasion; completemacroscopic resection of the tumor
Microscopic extrathyroidal extension ofthe tumor neck lymph node metastasesor131I uptake outside the thyroid bed onthe first post-treatment RxWBS
Incomplete resection of the tumor
No extrathyroidal tumor extension Distant metastasesNo local or distant metastasesNo 131I uptake outside the thyroid bed onthe first RxWBS (when done)
RxWBS, post-treatment whole-body scan.
Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R144
thyroidectomy plus postoperative radioiodine ablation of
the normal thyroid remnant). Excellent responses
(absence of both structural and biochemical evidence of
disease) reduced the likelihood of finding persistent/re-
current structural disease in all three ATA risk groups
(from 3 to 2% in the low-risk category, from 21 to 2% in
the intermediate-risk groups, and from 68 to 14% in
those with high-risk disease). Similar findings later
emerged from a second retrospective, single-institution
study, in which risk was re-classified on the basis of the
disease status w1 year after the initial treatment
(Castagna et al. 2011a).
These studies showed that, regardless of the initial risk
estimate, the likelihood of recurrence in patients with no
evidence of disease at the 1–2-year follow-up is quite low
(4% in the earlier study and 3.4% in the later one; Tuttle
et al. 2010, Castagna et al. 2011a). Most importantly,
around 30% (Tuttle et al. 2010) to 50% (Castagna et al.
2011a) of the patients previously classified as ATA
intermediate–high-risk could be re-classified as low-risk
(no evidence of disease) within 1–2 years of follow-up.
With this approach, a substantial proportion of patients
with DTCs – including some whose initial staging
revealed a high risk of persistent disease – can at some
point be channeled into surveillance that is less intensive
than originally planned.
What are the current indications andcontraindications for postoperativeradioactive iodine therapy?
By the late 1990s, patients with DTCs were almost
invariably treated postoperatively with radioiodine (131I).
In the currently advocated risk- and response-based
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
management strategies, this approach is being used
much more selectively. Even the specific indications for
using radioiodine therapy in the early postoperative
management have been questioned over the past few
years. Current practice guidelines in Europe and the USA
(Pacini et al. 2006, Cooper et al. 2009) cite three rationales
for administering radioiodine after total thyroidectomy:
i) it eliminates any normal thyroid tissue left after surgery,
thereby simplifying subsequent detection of residual/
recurrent tumor tissue; ii) it destroys any occult micro-
scopic foci of neoplastic cells within the thyroid remnant
or elsewhere in the body, thus improving the long-term
outcome (adjuvant therapy); and iii) it can be used to treat
known tumor residual tissues. While the ATA and the ETA
have defined indications for using radioiodine, the
application of this treatment in clinical practice differs
between countries and even within them (Haymart et al.
2013). This variation is possibly due to several non-tumor-
related factors, such as different restrictions for adminis-
tering radioactive material, different cohorts of patients,
and, last but not the least, different acceptance of the
treatment strategy. The latter underlines the need for clear
recommendations for the management of DTCs and thus
for well-designed clinical trials addressing the gray areas
where evidence is ambivalent. Current indications for
postoperative radioactive iodine therapy are discussed in
more detail below.
Normal thyroid remnant ablation
Postoperative administration of radioiodine facilitates
subsequent follow-up by eliminating any normal thyroid
tissue left behind after surgery. It is widely accepted
that the presence of such tissue can diminish the
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R145
accuracy of two methods for detecting residual/recurrent
thyroid cancer.
The first is the serum thyroglobulin (Tg) assay. The
measurement of basal and stimulated Tg levels has been a
cornerstone of postoperative surveillance programs for
patients with DTCs since the 1980s (Pacini et al. 2006,
Cooper et al. 2009). Tg is produced exclusively by cells of
thyroid follicular origin, so if all normal thyroid tissues
have been eliminated by surgery and postoperative radio-
iodine remnant ablation (RRA), subsequent findings of
detectable Tg levels represent a highly specific marker of
tumor recurrence (Pacini et al. 2006, Cooper et al. 2009). If
RRA is omitted, the clinical significance of these findings
declines since the assay positivity may simply reflect Tg
production by residual nests of normal thyrocytes, and
there is no specific cutoff level that can reliably distinguish
the production of this type from that of persistent or
recurrent neoplastic thyroid tissue (Pacini et al. 2006,
Cooper et al. 2009). Consequently, the use of RRA is
advocated to preserve the diagnostic value of serum Tg
assays in the patient’s follow-up.
This is not, however, the only solution. As will be
discussed later in this article, while the predictive value of
a single serum Tg measurement is undeniably lower in
patients who have not undergone RRA, serial Tg measure-
ments can disclose changes over time that can be reliable
markers of recurrent disease. In a recent retrospective
study, the natural history of ‘benign’ Tg production by
unablated postoperative remnants of normal thyroid
tissue has been characterized in 290 patients with low-
risk PTCs (classified by the ATA system; Durante et al.
2012). Although none of these patients had undergone
RRA, around 60% had undetectable Tg levels (!0.2 ng/ml)
– without TSH suppression – within the first year of
thyroidectomy. In the other cases, Tg levels remained
detectable during the first year but declined spontaneously
and progressively thereafter. As a result, by the fifth year of
the follow-up, the proportion of patients with undetect-
able levels was close to 80%. In the other 20%, serum Tg
levels decreased to low but detectable ones and remained
stable for the duration of the follow-up. At the end of the
follow-up (median 5 years), all of these individuals were
disease-free. Only 1 of the 290 patients experienced
recurrence, and it was associated with a gradual increase
in previously stable levels of Tg. These data challenge the
notion that Tg assays are of little use in the follow-up of
patients with DTCs who have not undergone RRA. In some
cases, Tg levels will remain within a detectable range
during the early phase of the follow-up (the first 5 years),
and this will undeniably reduce the diagnostic value of
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
single Tg assay results. However, the temporal trend of
consecutive measurements of serum Tg can be a reliable
indicator of the presence (rising values) or absence
(declining values) of recurrent thyroid cancer in patients
undergoing total or near-total thyroidectomy. Short
postoperative serum Tg doubling-time (!1 year) has
been reported to be independently associated with
the likelihood of having loco-regional and distant
recurrence, irrespective of radioiodine administration
(Miyauchi et al. 2011).
The second follow-up tool the use of which is
complicated by the omission of RRA is 131I scintigraphy.
When there is an appreciable thyroid remnant, the normal
tissue 131I uptake can mask the uptake by microscopic foci
of neoplastic cells within or near the remnant. The
likelihood of detecting extrathyroidal tumor cells is also
reduced. In vivo studies in patients with metastatic DTCs
have shown that 131I uptake by the neoplastic foci is
consistently lower (and may even drop below the
detection level) in the presence of a normal thyroid
remnant, which is often much more efficient than the
metastatic lesions in incorporating the radioiodine
(Schlumberger et al. 2007a). By eliminating this compe-
tition, RRA can improve the sensitivity of the 131I scan
for identifying disease recurrence (Pacini et al. 2006,
Cooper et al. 2009).
It is important to recall, however, that w70% of
thyroid cancers are confined to the thyroid bed at
diagnosis, and in 85% of the remaining cases, the
extrathyroidal disease consists exclusively of regional
lymph node involvement (http://seer.cancer.gov/stat-
facts/html/thyro.html; last accessed 20 January 2013). In
these cases, 131I scintigraphy displays a low sensitivity in
the detection of persistent/recurrent disease, and enhan-
cing its specificity by ablating the normal thyroid remnant
is of considerably less use (Cailleux et al. 2000, Pacini et al.
2003, Torlontano et al. 2003, 2006). Adverse effects must
also be considered in these decisions. Exposure to radio-
iodine significantly increases the probability of second
primary malignancies, salivary gland dysfunction, and
other complications (Rubino et al. 2003, Brown et al. 2008,
Sawka et al. 2009, Van Nostrand 2009). Most of these can
have a negative effect on the patient’s quality of life. As for
the risk for second primaries, it is generally felt to be
radiation dose dependent (Rubino et al. 2003), but some
increase in the overall risk – which nonetheless remains
very low – has been reported even in patients treated
exclusively to ablate the normal remnant, presumably
with cumulative activities in the lower range (Iyer
et al. 2011).
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R146
In light of these considerations, the view that RRA is
necessary to facilitate initial staging and follow-up appears
somewhat less convincing, and postoperative radioiodine
therapy is being used with much more caution, especially
in low-risk cases (Cooper et al. 2009). If it is used, the ATA
guidelines advise using the lowest activity needed to
ensure successful remnant ablation (Cooper et al. 2009).
The validity of this approach has recently been confirmed
by the results of two prospective randomized clinical
trials conducted in low-to-intermediate-risk DTC patients
(Mallick et al. 2012, Schlumberger et al. 2012). In both
studies, low-dose (1.1 GBq (30 mCi)) and high-dose
(3.7 GBq (100 mCi)) radioiodine regimens displayed
similar efficacies in eliminating normal thyroid residual
tissue, regardless of whether the patients were prepared for
the procedure with thyroid hormone withdrawal or
recombinant human TSH (rhTSH) stimulation.
Destruction of occult foci of neoplastic cells
Postoperative 131I administration is also used as an
adjuvant procedure for destroying any residual micro-
scopic nests of thyroid cancer cells that may be present in
the thyroid remnant or elsewhere in the body (Cooper
et al. 2009). The elimination of these potential foci is
thought to reduce the risk of recurrence and improve the
long-term outcome. This rationale is supported largely by
data from retrospective studies conducted in the 1990s. In
the landmark study by Mazzaferri & Jhiang (1994), 1355
patients with DTC were followed for over 40 years (median
15.7 years). At 30 years, the rates of both recurrence and
cancer-related death were approximately threefold lower
in the patients who had undergone RRA. Similar con-
clusions emerged from other studies, which found that
RRA significantly reduced disease recurrence (Samaan et al.
1992, DeGroot 1994) and disease-specific mortality rates
(Samaan et al. 1992). The publication of these reports was
followed by dramatic increases in the use of postoperative131I administration, and by the late 1990s, it was being
performed in almost all patients.
Other large studies, however, have kindled debates on
the true effectiveness of this approach: they found that
radioiodine adjuvant therapy had no significant effect on
long-term outcomes in patients with DTCs (Hundahl et al.
1998, Hay et al. 2002). The conflicting results that emerged
from these efforts are largely a reflection of
the heterogeneity of the study populations in terms of
the risks of recurrence and disease-specific mortality. Even
the investigators who had reported benefits with RRA
acknowledged that these benefits seemed to be restricted
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
to patients with larger primary tumors (i.e. 1.5 cm or more;
DeGroot 1994, Mazzaferri & Jhiang 1994). More recent
studies have looked at the effectiveness of RRA as a
function of disease stage (Jonklaas et al. 2006, Sacks et al.
2010). The National Thyroid Cancer Treatment Coopera-
tive Study Group (NTCTCSG) has published its experience
with 2936 DTC patients who were prospectively followed
for a median period of 3 years (Jonklaas et al. 2006).
Benefits from radioiodine therapy were documented only
for patients with advanced-stage cancers (NTCTCSG stages
III and IV): in this setting, there were significant
improvements in the risk ratios for both disease-free
survival (1.32, 95% CI 1.02–1.68, PZ0.035) and disease-
specific survival (1.46, 95% CI 1.13–1.87, PZ0.0045). RRA
had no effect, however, on either of these outcomes in
patients with stage I or II DTCs.
In light of these findings, it is becoming increasingly
clear that radioiodine adjuvant therapy needs to be used
selectively, and this strategy shift is reflected in the 2009
ATA guidelines (Cooper et al. 2009), which recommend
tailoring case management to individual risk levels.
A recent multicenter study conducted in Italy (Durante
et al. 2010) has retrospectively examined the long-term
outcomes of 175 DTC patients with very-low-risk primary
tumors (intrathyroidal, unifocal, subcentimeter PTCs with
no known high-risk features) who had not received RRA.
In a median follow-up of 6.7 years (range 5–23), there were
no recurrences and no thyroid-cancer-related deaths.
Shortly thereafter, Vaisman et al. (2011) reported that
the omission of radioactive iodine therapy is compatible
with very low rates of recurrence, even in selected patients
with estimated risks classified as low to intermediate. In
120 non-ablated patients with primary tumors measuring
1–4 cm, little or no extrathyroidal extension, and minimal
or absent cervical lymph node involvement, the rate of
structural disease recurrence was only 4.1% (5 out of 120)
after a median follow-up of 5 years (range 0.5–34).
A similar approach has been advocated for FTC histotype,
for which the absence or the presence of histopathological
vascular invasion better discriminates between low-
and high-risk patients respectively. In particular, the
occurrence of vascular invasion (widely invasive FTCs)
should prompt RRA therapy (Cooper et al. 2009, Dralle
et al. 2013).
Accurate risk assessment thus appears to be the key to
identifying DTC patients who are likely to benefit from
postoperative radioiodine therapy. In this regard, prophy-
lactic central and/or lateral neck dissection has been
advocated to optimize staging (Hartl et al. 2012). However,
the prognostic significance of subclinical microscopic
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Table 3 Features predicting radioiodine-refractory disease.
Clinicopathological features Age O40 yearsPoorly differentiated thyroid
cancerLarge metastasesBone metastases
Functional imaging findings RAI scan: at least one lesionwithout RAI uptake
18FDG–PET scan: FDG-avidlesions, irrespective of their
Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R147
cervical lymph node metastases has been recently ques-
tioned (Randolph et al. 2012). Firm conclusions on this
issue will have to be based on data regarding the effects of
radioiodine not only on recurrence but also on disease-
specific survival. These aspects are being addressed in one
multicenter prospective randomized trial in low-risk
thyroid cancer patients, which is now underway in
Europe (http://clinicaltrials.gov/show/NCT01398085; last
accessed 31 January 2013).
RAI uptakeResponse to therapy At least one lesion that pro-gresses during the first yearafter RAI therapy
Persistent disease after treat-ment with cumulative RAIactivity of O22 GBq(600 mCi)
RAI, radioactive iodine; 18FDG–PET, 2-[18F]fluoro-2-deoxyglucose–positronemission tomography; GBq, gigabecquerel.
Elimination of documented residual disease foci
For DTC patients with gross residual disease that is
inoperable, radioiodine therapy is currently the most
effective treatment that we have to offer. Indeed, it is the
only approach that has been demonstrated to significantly
improve disease-free survival (Samaan et al. 1992) and,
most important, overall survival (Durante et al. 2006),
which represents the main outcome in clinical oncology.
For several reasons, however, the use of radioiodine for
this purpose is also becoming more selective (Tuttle et al.
2011), and clinicians are being encouraged to base their
decisions on a careful risk–benefit analysis.
Aside from the risk of long- and short-term adverse
effects, one of the main reasons for this shift is the growing
awareness that RAI is ineffective in some patients with
advanced disease. The selectivity of radioiodine therapy
for DTC cells depends on the functional integrity of the
complex network of specialized proteins (e.g. the sodium
iodide symporter and thyroperoxidase) involved in phys-
iological iodine metabolism and hormonogenesis
(Schlumberger et al. 2007a). These functions are usually
preserved to some extent in the cells of primary DTCs
(Arturi et al. 2001), although varying degrees of impair-
ment can be caused by genetic and epigenetic events
involved in the malignant transformation process
(Trapasso et al. 1999, Puppin et al. 2005, Durante et al.
2007, Russo et al. 2011). Complete loss of these functions
is characteristic of undifferentiated and anaplastic
primaries. Iodine uptake in some metastatic thyroid
cancer cells is also less efficient than that in their primary
tumor counterparts. This phenomenon, too, can be
attributed to dedifferentiation, although the iodine-
trapping capacity of metastatic thyrocytes may also vary
with the site of the lesion (i.e. lymph nodes, bone, lung,
and liver; Arturi et al. 2000). Table 3 presents some of the
clinical, pathlogical, and radiological findings associated
with radioiodine-refractory thyroid cancer. It is also
important to note that promising therapeutic alternatives
to radioiodine are finally becoming available. Several
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
novel, molecularly targeted drug therapies are already
being tested for this purpose in clinical trials, and others
will begin such testing soon (Schlumberger & Sherman
2012).
Which patients stand to benefit from TSHsuppression therapy and what degree ofsuppression is appropriate?
Thyroid cancer cells generally remain responsive to the
effects of circulating TSH, which stimulates a variety of
cellular processes including cell proliferation (Biondi et al.
2005). This is the rationale cited for the use of TSH-
suppressive doses of thyroid hormone therapy, which has
been reported to significantly decrease recurrence rates
and cancer-related mortality in DTC patients (Mazzaferri
& Kloos 2001, McGriff et al. 2002). However, the degree of
suppression required to achieve these goals is uncertain.
The reduction of TSH levels to !0.1 mU/l has been
associated with better clinical outcomes in high-risk
thyroid cancer patients (Cooper et al. 1998), but the
possibility that milder reductions (0.1–0.5 mU/l) might
offer the same benefits has never been explored. Further-
more, TSH suppression produces a state of subclinical
hyperthyroidism, which can have negative effects on the
bone and heart (Cooper & Biondi 2012). The 2009 ATA
guidelines stress the importance of striking a
balance between the potential risks and benefits of TSH
suppression (Cooper et al. 2009). At the beginning of the
follow-up, the degree of TSH suppression should be chosen
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R148
on the basis of the individual patient’s risk for persistent
or recurrent disease. Later on, suppression might be
discontinued if there is no documented evidence of
disease (Table 1).
What are the best diagnostic methods fordetecting persistent/recurrent disease and foridentifying patients who are cured and howshould these tools be used?
The early phase of the postoperative follow-up of patients
with DTCs (i.e. the first year or 2 years after the initial
treatment) has a twofold purpose: to detect persistent
disease, which may require additional therapy or at least
more active surveillance, and to identify probable cures.
As has been discussed previously, most patients will
belong to the latter group, and in some the likelihood of
recurrence will be low enough to justify less intensive
surveillance than that planned on the basis of the initial
ATA- or ETA-based risk estimate (Tuttle et al. 2010,
Castagna et al. 2011a,b). For the patients who appear to
be disease free, the main goal of the successive, long-term
phase of the follow-up is the prompt detection of
possible recurrence.
Reliable detection of persistent or recurrent disease
requires diagnostic tools with a high positive predictive
value; those with high negative predictive values are
suitable for identifying cases that have been cured. The
ATA (Cooper et al. 2009) and the ETA (Pacini et al. 2006)
concur that serum Tg assays and neck ultrasonography
(US) are the essential tools for monitoring patients with
DTCs, but neither association offers any details on the
merits or shortcomings of these tools or on how and when
should they be used.
Serum Tg assays
As has been discussed above, the serum Tg level is a highly
specific marker of persistent or recurrent disease in a
patient treated with total thyroidectomy and RRA. In
patients whose surgery consisted of sub-total thyroid-
ectomy or lobectomy or those who had a total thyroid-
ectomy without RRA, the specificity of a positive Tg assay
plummets, since the Tg detected may well be coming from
the normal thyroid remnant (Pacini et al. 2006, Cooper
et al. 2009). The importance of this shortcoming is highest
during the initial postoperative evaluation/phase of the
follow-up: as the follow-up continues, the value of the
Tg assay increases. Recent studies have shown, in fact,
that Tg production by the normal remnant declines
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
spontaneously and sometimes becomes undetectable
within the first year of the follow-up. After 5 years, levels
are likely to be undetectable in the vast majority of cases
(almost 80%) – just as they are in patients who have
undergone total thyroidectomies plus RRA (see the
previous section for details; Durante et al. 2012). In
addition, although benign Tg production in some non-
ablated patients never ceases completely, it does stabilize.
In contrast, ‘malignant’ Tg production tends to increase
over time, and this trend is highly predictive of persistent
or progressive neoplastic disease, regardless of whether or
not nests of normal thyrocytes are still present (Baudin
et al. 2003, Torlontano et al. 2004, Miyauchi et al. 2011). In
short, in non-ablated patients – who represent an
increasingly large proportion of the individuals with
DTCs – the initial postoperative serum Tg measurement
is per se an unreliable marker of persistent disease, but its
specificity increases when it is examined with subsequent
measurements: increasing Tg production documented
with serial determinations over the course of the follow-
up is associated with a positive predictive value for
persistent/recurrent disease of roughly 100%. In particu-
lar, a Tg doubling-time of !1 year appears to be the
strongest correlate of recurrence and cancer-specific
survival (Miyauchi et al. 2011).
The sensitivity of a serum Tg measurement varies
depending on the patient’s TSH level at the time of the
assay. Small foci of neoplastic tissue may not be detected if
the Tg assay is done while the patient is on levothyroxine
(especially at TSH-suppressive doses) (Mazzaferri et al.
2003, Bachelot et al. 2005). To maximize sensitivity, Tg
production must be measured during endogenous or
exogenous TSH stimulation (the former elicited by
levothyroxine withdrawal and the latter by the adminis-
tration of rhTSH; Eustatia-Rutten et al. 2004, Schlumberger
et al. 2007b). The latter approach, however, is generally
reserved for patients who have undergone RRA (Pacini
et al. 2006, Cooper et al. 2009). In these cases, one can be
reasonably certain that normal thyroid cells are no longer
present, and TSH stimulation will be targeting only
residual cancerous cells (if any are present).
The need to measure TSH-stimulated Tg is expected to
decline as the availability of high-sensitivity Tg assays
increases inclinical settings (Smallridge et al. 2007, Castagna
et al. 2011a,b, Malandrino et al. 2011). These assays, which
have functional sensitivities of !0.2 ng/ml, may allow
earlier detection of ‘malignant’ Tg production even while
patients are still taking levothyroxine. A study conducted in
2007 has compared the diagnostic values of seven pro-
gressively sensitive Tg assays (Schlumberger et al. 2007b).
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R149
A detection limit of 0.9 ng/ml was associated with a low
sensitivity in identifying persistent disease (40%). Sensi-
tivity doubled (almost 80%) when the assays with the
lowest detection limits (0.11 and 0.02 ng/ml) were tested,
but the cost of this improvement was a considerable loss in
specificity. Based on their data, the authors concluded that
the best trade-off was a functional assay sensitivity
between 0.2 and 0.3 ng/ml, which offers an improved
diagnostic sensitivity (about 65%) without significantly
diminishing the specificity (Schlumberger et al. 2007b).
However, the true diagnostic accuracies of the high-
sensitivity Tg assays still need to be validated in larger
prospective studies. At present, they can be exploited to
study the trend of serial serum Tg determinations, which
still offers the highest negative (decreasing levels) and
positive (rising levels) predictive values (Baudin et al. 2003,
Torlontano et al. 2004).
In the presence of serum Tg antibodies, both
conventional measurements of TSH-stimulated Tg levels
and high-sensitivity assays of basal Tg production may fail
to identify patients with clinically significant tumor foci
(Spencer et al. 1999). In these cases, serial serum anti-Tg
antibody quantification using the same methodology may
serve as an imprecise surrogate marker of residual normal
thyroid tissue or tumor (Spencer et al. 1998, Chiovato et al.
2003). In a large series of patients with DTC who
underwent RRA, those showing a more than 50% decrease
in serum anti-Tg antibodies within 6–12 months of
ablation had a significantly lower recurrence rate than
patients with lower reduction or increasing levels of the
antibodies (Kim et al. 2008).
Neck US
Aside from the safety and relatively low cost of ultrasound
imaging in general, one of the main reasons neck
sonography is so valuable in the postoperative follow-up
of PTC patients (Durante & Filetti 2011) is that disease
spread or recurrence is almost always associated first with
cervical lymphadenopathy. In addition, unlike serum Tg
assays and 131I WBS, it performs equally well in patients
who have not undergone RRA, it requires no hormone
withdrawal or administration of rhTSH, and it provides
valuable information for surgeons on the location and
preoperative tattooing of the involved nodes.
Neck US has been widely used in patients with DTCs
since the 1990s, and the sonographic criteria for identify-
ing cervical lymph node metastases are well established
(Leboulleux et al. 2007). In terms of sensitivity, it has
repeatedly proved to be superior to stimulated Tg assays
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
and diagnostic WBS in detecting cervical node involve-
ment (Antonelli et al. 1995, Pacini et al. 2003, Torlontano
et al. 2003, 2004). In 335 PTC patients whose Tg levels
remained undetectable after TSH stimulation at the 1-year
postoperative follow-up, neck US disclosed cervical
metastases in 7 (2%) cases (Torlontano et al. 2004).
Another important advantage of neck US over Tg assays
is its high negative predictive value, which approaches
100% in cases of very low-risk DTCs. In a large, long-term
study of 312 patients with this type of PTC, those with
negative findings on the first postoperative US study (3–12
months after surgery) were all disease free at the end of the
follow-up (Durante et al. 2010). To improve the specificity
of the examination, nodules that appear suspicious can be
biopsied immediately under US guidance (Pacini et al.
2006, Cooper et al. 2009) and the sample submitted for
cytologic analysis and/or measurement of Tg levels in the
needle-washout fluid (Uruno et al. 2005).
Neck US is thus becoming the mainstay of the
postoperative follow-up of DTCs, especially during the
early months, when, in the increasingly large proportion
of patients with low- or very-low-risk tumors who have not
undergone RRA, Tg assay results are difficult to interpret.
When the initial postoperative scan is negative, the
probability of a favorable long-term outcome is quite
high, regardless of serum Tg levels. Even in low-risk
patients, however, metastatic disease can still be discov-
ered, sometimes several years after the initial treatment
(Ross et al. 2009), so surveillance must be continued. As
has been discussed above, the value of serum Tg assays
increases with time, as consecutive measurements
accumulate and allow increasingly reliable assessments
of production trends. In the later phases of the follow-up,
greater reliance might be placed on basal Tg assays, which
are less expensive and easier to schedule than neck US
(Fig. 1). Additional research is needed, of course, to assess
the sensitivity of this approach.
All the above-mentioned arguments apply mainly to
PTC histotype. As for FTCs, while lymph node metastases
involve almost 20% of patients with widely invasive
forms, distant metastases are present in as many as one-
third of the patients, often in the absence of nodal
involvement (Dralle et al. 2013). Thus, staging FTCs
requires further complementary imaging modalities
(Table 4). Finally, it is important to recall that one of the
inherent features of sonographic imaging is inter-operator
variability. To reduce the effect of this potential limitation,
neck US, as an integral part of thyroid cancer follow-up
protocols, should be performed using standardized proto-
cols and in strict compliance with guidelines and criteria
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Yes No
Diseasefree
Diseasefree
Evidence ofdisease
Postoperative RAI therapy
Stimulated Tg orbasal Tg assay
Neck US
Cross sectional/functional studies(high-risk patients, FTC)
Basal Tg assay
Neck US
Earlyfollow-up
1–2 years afterinitial surgery
Therapy oractive
surveillance
Latefollow-up
>2 years afterinitial surgery
Serial serum Tg determination (trend)
Neck US
Figure 1
Diagnostic tools in the early and long-term follow-up of DTC patients. RAI, radioactive iodine; Tg, thyroglobulin; US, ultrasound;
FTC, follicular thyroid cancer.
Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R150
recommended by the scientific societies. Uniform quality
may also be more likely when the examinations are done
by specially trained physicians with close and continuous
involvement in the overall care of the patient with DTC.
Other tools
Whenever US and/or Tg data are suggestive of persistent/
recurrent disease, additional imaging studies may be
warranted. These include both cross-sectional modalities
such as computed tomography or magnetic resonance
imaging and nuclear medicine procedures, such as WBS
and 2-[18F]fluoro-2-deoxyglucose–positron emission
tomography (18FDG–PET;Table 4; Pacini et al. 2006, Cooper
et al. 2009). In addition to detecting neoplastic foci, 18FDG–
PET also has important prognostic and treatment impli-
cations. Several studies have shown, in fact, that FDG-avid
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
lesions are unresponsive to high-dose radioiodine therapy,
and this type of disease carries the highest risk for thyroid
cancer-related mortality (Robbins et al. 2006).
How long should the patients who areapparently disease free be followed?
Life-long follow-up is still the rule for patients with DTCs.
Once again, however, this practice is rooted largely in data
on the outcomes of cases treated at least 20 or 30 years ago
(DeGroot 1994, Mazzaferri & Jhiang 1994). Today, in light
of the numbers of PTCs being diagnosed, the changing
profile of the PTC patient population, and improvements
in the methods available for detecting postoperative
recurrence, the cost-effectiveness of protracted surveil-
lance is being questioned. In 1994, Mazzaferri & Jhiang
analyzed 1077 PTC patients treated during the last four
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Table 4 Second-line imaging studies for the work-up of
persistent/recurrent disease in patients with DTCs.
Imaging procedures Clinical applications
Contrast-enhanced computedtomography
To detect lesions in the brain,neck, chest, and abdomen(triple-phase scanning isrequired for liver studies)
Magnetic resonance imaging To detect brain, liver, and bonelesions
Diagnostic 131I whole-bodyscan
To identify the source ofpersistent Tg production inintermediate-/high-riskpatients
To stage patients at a higherrisk of persistent/recurrentdisease, including individ-uals with widely invasive FTC
Bone scintigraphy To detect skeletal lesions18FDG–PET To identify occult metastases in
patients with elevated Tglevels and negative whole-body scans
To stage patients with poorlydifferentiated thyroid canceror Hurthle cell carcinoma
To identify patients with dis-tant metastases at a highestrisk for cancer-relatedmortality
To identify patients unlikely torespond to RAI therapy
To evaluate responses tosystemic or local treatment
DTC, differentiated thyroid cancer; RAI, radioactive iodine; Tg, thyro-globulin; FTC, follicular thyroid cancer; 18FDG–PET, 2-[18F]fluoro-2-deoxyglucose–positron emission tomography.
Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R151
decades of the 20th century and found a recurrence rate of
more than 20%. After O5 years of follow-up, 40% of the
recurrences were identified, and around 20% were
detected after the tenth year. In 2013, Durante et al.
(2013) conducted a similar analysis of 1020 patients
treated between 1990 and 2008. The recurrence rate was
markedly lower (1.4%); over 75% of the recurrences were
discovered within 5 years of the initial treatment, and
none were detected after the eighth year of the follow-up.
The demography of DTC patients seen in general
thyroid disease practices has clearly changed. Roughly
three out of four of the patients in the 2013 study had
stage I tumors. This is approximately five times higher
than the percentage reported by Mazzaferri & Jhiang
(even allowing for the fact that the staging criteria used in
the two studies were slightly different). In addition, almost
half the cases analyzed in the 1994 study were charac-
terized by regional lymph node involvement at the time of
the initial therapy – almost twice the rate reported in the
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
2013 study. Finally, the past 30 years have witnessed a
progressive decline in the use of 131I WBS during
the follow-up of DTC patients and greater reliance on
high-resolution neck US and increasingly sensitive serum
Tg assays.
Concluding remarks
Figure 1 shows an algorithm for individualized, risk-
tailored management of the DTC patients being seen by
today’s endocrinologists. This approach reflects current
recommendations made by the ATA and ETA, and it is
clearly different from the approaches that had been used
5–10 years ago (Table 1). As our knowledge of the biology
and natural history of these tumors expands, the manage-
ment strategies that we use will continue to evolve. In all
probability, the trend will be toward increasingly indivi-
dualized treatment aimed at optimizing treatment – in
terms of efficacy, cost, and quality of life benefits – for all
patients with DTCs (right column, Table 1).
Declaration of interest
The authors declare that there is no conflict of interest that could be
perceived as prejudicing the impartiality of the review reported.
Funding
This review did not receive any specific grant from any funding agency in
the public, commercial or not-for-profit sector.
Acknowledgements
The authors acknowledge the following funding sources: The Umberto Di
Mario Foundation and the ‘Banca d’Italia’. The authors thank Marian
Everett Kent, BSN, for editing the manuscript.
References
Antonelli A, Miccoli P, Ferdeghini M, Di Coscio G, Alberti B, Iacconi P,
Baldi V, Fallahi P & Baschieri L 1995 Role of neck ultrasonography in
the follow-up of patients operated on for thyroid cancer. Thyroid 5
25–28. (doi:10.1089/thy.1995.5.25)
Arturi F, Russo D, Giuffrida D, Schlumberger M & Filetti S 2000 Sodium–
iodide symporter (NIS) gene expression in lymph-node metastases of
papillary thyroid carcinomas. European Journal of Endocrinology 143
623–627. (doi:10.1530/eje.0.1430623)
Arturi F, Russo D, Bidart JM, Scarpelli D, Schlumberger M & Filetti S 2001
Expression pattern of the pendrin and sodium/iodide symporter genes
in human thyroid carcinoma cell lines and human thyroid tumors.
European Journal of Endocrinology 145 129–135. (doi:10.1530/eje.0.
1450129)
Bachelot A, Leboulleux S, Baudin E, Hartl DM, Caillou B, Travagli JP &
Schlumberger M 2005 Neck recurrence from thyroid carcinoma: serum
thyroglobulin and high-dose total body scan are not reliable criteria for
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R152
cure after radioiodine treatment. Clinical Endocrinology 62 376–379.
(doi:10.1111/j.1365-2265.2005.02228.x)
Baudin E, Do Cao C, Cailleux AF, Leboulleux S, Travagli JP &
Schlumberger M 2003 Positive predictive value of serum thyroglobulin
levels, measured during the first year of follow-up after thyroid
hormone withdrawal, in thyroid cancer patients. Journal of Clinical
Endocrinology and Metabolism 88 1107–1111. (doi:10.1210/jc.2002-
021365)
Biondi B, Filetti S & Schlumberger M 2005 Thyroid-hormone therapy and
thyroid cancer: a reassessment. Nature Clinical Practice. Endocrinology &
Metabolism 1 32–40. (doi:10.1038/ncpendmet0020)
Brierley JD, Panzarella T, Tsang RW, Gospodarowicz MK & O’Sullivan B
1997 A comparison of different staging systems predictability of patient
outcome. Thyroid carcinoma as an example. Cancer 79 2414–2423.
(doi:10.1002/(SICI)1097-0142(19970615)79:12!2414::AID-CNCR18O3.
0.CO;2-U)
Brown AP, Chen J, Hitchcock YJ, Szabo A, Shrieve DC & Tward JD 2008 The
risk of second primary malignancies up to three decades after the
treatment of differentiated thyroid cancer. Journal of Clinical Endo-
crinology and Metabolism 93 504–515. (doi:10.1210/jc.2007-1154)
Cailleux AF, Baudin E, Travagli JP, Ricard M & Schlumberger M 2000 Is
diagnostic iodine-131 scanning useful after total thyroid ablation for
differentiated thyroid cancer? Journal of Clinical Endocrinology and
Metabolism 85 175–178. (doi:10.1210/jc.85.1.175)
Castagna MG, Maino F, Cipri C, Belardini V, Theodoropoulou A,
Cevenini G & Pacini F 2011a Delayed risk stratification, to include
the response to initial treatment (surgery and radioiodine ablation),
has better outcome predictivity in differentiated thyroid cancer
patients. European Journal of Endocrinology 165 441–446. (doi:10.1530/
EJE-11-0466)
Castagna MG, Tala Jury HP, Cipri C, Belardini V, Fioravanti C, Pasqui L,
Sestini F, Theodoropoulou A & Pacini F 2011b The use of ultrasensitive
thyroglobulin assays reduces but not abolishes the need for TSH
stimulation in patients with differentiated thyroid carcinoma. Journal of
Endocrinological Investigation 34 e219–e223. (doi:10.3275/7571)
Chiovato L, Latrofa F, Braverman LE, Pacini F, Capezzone M, Masserini L,
Grasso L & Pinchera A 2003 Disappearance of humoral thyroid
autoimmunity after complete removal of thyroid antigens. Annals of
Internal Medicine 139 346–351. (doi:10.7326/0003-4819-139-5_Part_1-
200309020-00010)
Cooper DS & Biondi B 2012 Subclinical thyroid disease. Lancet 379
1142–1154. (doi:10.1016/S0140-6736(11)60276-6)
Cooper DS, Specker B, Ho M, Sperling M, Ladenson PW, Ross DS, Ain KB,
Bigos ST, Brierley JD, Haugen BR et al. 1998 Thyrotropin suppression
and disease progression in patients with differentiated thyroid cancer:
results from the National Thyroid Cancer Treatment Cooperative
Registry. Thyroid 8 737–744. (doi:10.1089/thy.1998.8.737)
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ,
Mazzaferri EL, McIver B, Pacini F, Schlumberger M et al. 2009 Revised
American Thyroid Association management guidelines for patients
with thyroid nodules and differentiated thyroid cancer. Thyroid 19
1167–1214. (doi:10.1089/thy.2009.0110)
D’Avanzo A, Treseler P, Ituarte PH, Wong M, Streja L, Greenspan FS,
Siperstein AE, Duh QY & Clark OH 2004 Follicular thyroid carcinoma:
histology and prognosis. Cancer 100 1123–1129. (doi:10.1002/
cncr.20081)
Davies L & Welch HG 2006 Increasing incidence of thyroid cancer in the
United States, 1973–2002. Journal of the American Medical Association
295 2164–2167. (doi:10.1001/jama.295.18.2164)
DeGroot LJ 1994 Long-term impact of initial and surgical therapy on
papillary and follicular thyroid cancer. American Journal of Medicine 97
499–500. (doi:10.1016/0002-9343(94)90342-5)
Dralle H, Musholt TJ, Schabram J, Steinmuller T, Frilling A, Simon D,
Goretzki PE, Niederle B, Scheuba C, Clerici T et al. 2013 German
Association of Endocrine Surgeons practice guideline for the surgical
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
management of malignant thyroid tumors. Langenbeck’s Archives of
Surgery 398 347–375. (doi:10.1007/s00423-013-1057-6)
Durante C & Filetti S 2011 Management of papillary thyroid cancer
patients in absence of postoperative radioiodine remnant ablation:
tailoring follow-up by neck sonography. Journal of Clinical Endocrinology
and Metabolism 96 3059–3061. (doi:10.1210/jc.2011-1379)
Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B,
Ricard M, Lumbroso JD, De Vathaire F et al. 2006 Long-term outcome of
444 patients with distant metastases from papillary and follicular
thyroid carcinoma: benefits and limits of radioiodine therapy. Journal of
Clinical Endocrinology and Metabolism 91 2892–2899. (doi:10.1210/
jc.2005-2838)
Durante C, Puxeddu E, Ferretti E, Morisi R, Moretti S, Bruno R, Barbi F,
Avenia N, Scipioni A, Verrienti A et al. 2007 BRAF mutations in
papillary thyroid carcinomas inhibit genes involved in iodine
metabolism. Journal of Clinical Endocrinology and Metabolism 92
2840–2843. (doi:10.1210/jc.2006-2707)
Durante C, Attard M, Torlontano M, Ronga G, Monzani F, Costante G,
Ferdeghini M, Tumino S, Meringolo D, Bruno R et al. 2010
Identification and optimal postsurgical follow-up of patients with very
low-risk papillary thyroid microcarcinomas. Journal of Clinical Endo-
crinology and Metabolism 95 4882–4888. (doi:10.1210/jc.2010-0762)
Durante C, Montesano T, Attard M, Torlontano M, Monzani F, Costante G,
Meringolo D, Ferdeghini M, Tumino S, Lamartina L et al. 2012 Long-
term surveillance of papillary thyroid cancer patients who do not
undergo postoperative radioiodine remnant ablation: is there a role for
serum thyroglobulin measurement? Journal of Clinical Endocrinology and
Metabolism 97 2748–2753. (doi:10.1210/jc.2012-1123)
Durante C, Montesano T, Torlontano M, Attard M, Monzani F, Tumino S,
Costante G, Meringolo D, Bruno R, Trulli F et al. 2013 Papillary thyroid
cancer: time course of recurrences during postsurgery surveillance.
Journal of Clinical Endocrinology and Metabolism 98 636–642.
(doi:10.1210/jc.2012-3401)
Eheman C, Henley SJ, Ballard-Barbash R, Jacobs EJ, Schymura MJ,
Noone AM, Pan L, Anderson RN, Fulton JE, Kohler BA et al. 2012
Annual Report to the Nation on the status of cancer, 1975–2008,
featuring cancers associated with excess weight and lack of sufficient
physical activity. Cancer 118 2338–2366. (doi:10.1002/cncr.27514)
Eustatia-Rutten CF, Smit JW, Romijn JA, van der Kleij-Corssmit EP,
Pereira AM, Stokkel MP & Kievit J 2004 Diagnostic value of serum
thyroglobulin measurements in the follow-up of differentiated thyroid
carcinoma, a structured meta-analysis. Clinical Endocrinology 61 61–74.
(doi:10.1111/j.1365-2265.2004.02060.x)
Hall SF, Walker H, Siemens R & Schneeberg A 2009 Increasing detection
and increasing incidence in thyroid cancer. World Journal of Surgery 33
2567–2571. (doi:10.1007/s00268-009-0226-9)
Hartl DM, Leboulleux S, Al Ghuzlan A, Baudin E, Chami L, Schlumberger M
& Travagli JP 2012 Optimization of staging of the neck with
prophylactic central and lateral neck dissection for papillary thyroid
carcinoma. Annals of Surgery 255 777–783. (doi:10.1097/SLA.
0b013e31824b7b68)
Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA,
Maurer MS, McIver B, Mullan BP, Oberg AL et al. 2002 Papillary thyroid
carcinoma managed at the Mayo Clinic during six decades (1940–
1999): temporal trends in initial therapy and long-term outcome in
2444 consecutively treated patients. World Journal of Surgery 26
879–885. (doi:10.1007/s00268-002-6612-1)
Haymart MR, Muenz DG, Stewart AK, Griggs JJ & Banerjee M 2013 Disease
severity and radioactive iodine use for thyroid cancer. Journal of Clinical
Endocrinology and Metabolism 98 678–686. (doi:10.1210/jc.2012-3160)
van Heerden JA, Hay ID, Goellner JR, Salomao D, Ebersold JR, Bergstralh EJ
& Grant CS 1992 Follicular thyroid carcinoma with capsular invasion
alone: a nonthreatening malignancy. Surgery 112 1130–1136.
Hundahl SA, Fleming ID, Fremgen AM & Menck HRA 1998 National Cancer
Data Base report on 53,856 cases of thyroid carcinoma treated in the
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R153
U.S, 1985–1995. Cancer 83 2638–2648. (doi:10.1002/(SICI)1097-
0142(19981215)83:12!2638::AID-CNCR31O3.0.CO;2-1)
Iyer NG, Morris LG, Tuttle RM, Shaha AR & Ganly I 2011 Rising incidence
of second cancers in patients with low-risk (T1N0) thyroid cancer who
receive radioactive iodine therapy. Cancer 117 4439–4446.
(doi:10.1002/cncr.26070)
Jonklaas J, Sarlis NJ, Litofsky D, Ain KB, Bigos ST, Brierley JD, Cooper DS,
Haugen BR, Ladenson PW, Magner J et al. 2006 Outcomes of patients
with differentiated thyroid carcinoma following initial therapy. Thyroid
16 1229–1242. (doi:10.1089/thy.2006.16.1229)
Kim WG, Yoon JH, Kim WB, Kim TY, Kim EY, Kim JM, Ryu JS, Gong G,
Hong SJ & Shong YK 2008 Change of serum antithyroglobulin antibody
levels is useful for prediction of clinical recurrence in thyroglobulin-
negative patients with differentiated thyroid carcinoma. Journal of
Clinical Endocrinology and Metabolism 93 4683–4689. (doi:10.1210/
jc.2008-0962)
Leboulleux S, Girard E, Rose M, Travagli JP, Sabbah N, Caillou B, Hartl DM,
Lassau N, Baudin E & Schlumberger M 2007 Ultrasound criteria of
malignancy for cervical lymph nodes in patients followed up for
differentiated thyroid cancer. Journal of Clinical Endocrinology and
Metabolism 92 3590–3594. (doi:10.1210/jc.2007-0444)
Leenhardt L, Grosclaude P & Cherie-Challine L 2004 Increased incidence of
thyroid carcinoma in France: a true epidemic or thyroid nodule
management effects? Report from the French Thyroid Cancer
Committee Thyroid 14 1056–1060. (doi:10.1089/thy.2004.14.1056)
Lo CY, Chan WF, Lam KY & Wan KY 2005 Follicular thyroid carcinoma: the
role of histology and staging systems in predicting survival. Annals of
Surgery 242 708–715. (doi:10.1097/01.sla.0000186421.30982.d2)
Malandrino P, Latina A, Marescalco S, Spadaro A, Regalbuto C, Fulco RA,
Scollo C, Vigneri R & Pellegriti G 2011 Risk-adapted management of
differentiated thyroid cancer assessed by a sensitive measurement of
basal serum thyroglobulin. Journal of Clinical Endocrinology and
Metabolism 96 1703–1709. (doi:10.1210/jc.2010-2695)
Mallick U, Harmer C, Yap B, Wadsley J, Clarke S, Moss L, Nicol A, Clark PM,
Farnell K, McCready R et al. 2012 Ablation with low-dose radioiodine
and thyrotropin alfa in thyroid cancer. New England Journal of Medicine
366 1674–1685. (doi:10.1056/NEJMoa1109589)
Mazzaferri EL & Jhiang SM 1994 Long-term impact of initial surgical and
medical therapy on papillary and follicular thyroid cancer. American
Journal of Medicine 97 418–428. (doi:10.1016/0002-9343(94)90321-2)
Mazzaferri EL & Kloos RT 2001 Clinical review 128: current approaches to
primary therapy for papillary and follicular thyroid cancer. Journal of
Clinical Endocrinology and Metabolism 86 1447–1463. (doi:10.1210/
jc.86.4.1447)
Mazzaferri EL, Robbins RJ, Braverman LE, Pacini F, Haugen B, Wartofsky L,
Haugen BR, Sherman SI, Cooper DS, Braunstein GD et al. 2003 Authors’
response: a consensus report of the role of serum thyroglobulin as a
monitoring method for low-risk patients with papillary thyroid
carcinoma. Journal of Clinical Endocrinology and Metabolism 88
4508–4509. (doi:10.1210/jc.2003-031041)
McGriff NJ, Csako G, Gourgiotis L, Lori CG, Pucino F & Sarlis NJ 2002
Effects of thyroid hormone suppression therapy on adverse clinical
outcomes in thyroid cancer. Annals of Medicine 34 554–564.
(doi:10.1080/078538902321117760)
Miyauchi A, Kudo T, Miya A, Kobayashi K, Ito Y, Takamura Y, Higashiyama T,
Fukushima M, Kihara M, Inoue H et al. 2011 Prognostic impact of serum
thyroglobulin doubling-time under thyrotropin suppression in patients
with papillary thyroid carcinoma who underwent total thyroidectomy.
Thyroid 21 707–716. (doi:10.1089/thy.2010.0355)
Orlov S, Orlov D, Shaytzag M, Dowar M, Tabatabaie V, Dwek P, Yip J, Hu C,
Freeman JL & Walfish PG 2009 Influence of age and primary tumor size
on the risk for residual/recurrent well-differentiated thyroid carcinoma.
Head & Neck 31 782–788. (doi:10.1002/hed.21020)
Pacini F, Molinaro E, Castagna MG, Agate L, Elisei R, Ceccarelli C, Lippi F,
Taddei D, Grasso L & Pinchera A 2003 Recombinant human
thyrotropin-stimulated serum thyroglobulin combined with neck
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
ultrasonography has the highest sensitivity in monitoring differen-
tiated thyroid carcinoma. Journal of Clinical Endocrinology and
Metabolism 88 3668–3673. (doi:10.1210/jc.2002-021925)
Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW & Wiersinga W 2006
European consensus for the management of patients with differen-
tiated thyroid carcinoma of the follicular epithelium. European
Journal of Endocrinology 154 787–803. (doi:10.1530/eje.1.02158)
Puppin C, D’Aurizio F, D’Elia AV, Cesaratto L, Tell G, Russo D, Filetti S,
Ferretti E, Tosi E, Mattei T et al. 2005 Effects of histone acetylation on
sodium iodide symporter promoter and expression of thyroid-specific
transcription factors. Endocrinology 146 3967–3974. (doi:10.1210/
en.2005-0128)
Randolph GW, Duh QY, Heller KS, LiVolsi VA, Mandel SJ, Steward DL,
Tufano RP, Tuttle RM & American Thyroid Association Surgical Affairs
Committee’s Taskforce on Thyroid Cancer Nodal Surgery 2012 The
prognostic significance of nodal metastases from papillary thyroid
carcinoma can be stratified based on the size and number of metastatic
lymph nodes, as well as the presence of extranodal extension. Thyroid
22 1144–1152. (doi:10.1089/thy.2012.0043)
Robbins RJ, Wan Q, Grewal RK, Reibke R, Gonen M, Strauss HW, Tuttle RM,
Drucker W & Larson SM 2006 Real-time prognosis for metastatic
thyroid carcinoma based on 2-[18F]fluoro-2-deoxy-D-glucose–positron
emission tomography scanning. Journal of Clinical Endocrinology and
Metabolism 91 498–505. (doi:10.1210/jc.2005-1534)
Ross DS, Litofsky D, Ain KB, Bigos T, Brierley JD, Cooper DS, Haugen BR,
Jonklaas J, Ladenson PW, Magner J et al. 2009 Recurrence after
treatment of micropapillary thyroid cancer. Thyroid 19 1043–1048.
(doi:10.1089/thy.2008.0407)
Rubino C, de Vathaire F, Dottorini ME, Hall P, Schvartz C, Couette JE,
Dondon MG, Abbas MT, Langlois C & Schlumberger M 2003 Second
primary malignancies in thyroid cancer patients. British Journal of
Cancer 89 1638–1644. (doi:10.1038/sj.bjc.6601319)
Russo D, Damante G, Puxeddu E, Durante C & Filetti S 2011 Epigenetics of
thyroid cancer and novel therapeutic targets. Journal of Molecular
Endocrinology 46 R73–R81. (doi:10.1530/JME-10-0150)
Sacks W, Fung CH, Chang JT, Waxman A & Braunstein GD 2010 The
effectiveness of radioactive iodine for treatment of low-risk thyroid
cancer: a systematic analysis of the peer-reviewed literature from 1966
to April 2008. Thyroid 20 1235–1245. (doi:10.1089/thy.2009.0455)
Samaan NA, Schultz PN, Hickey RC, Goepfert H, Haynie TP, Johnston DA &
Ordonez NG 1992 The results of various modalities of treatment of well
differentiated thyroid carcinomas: a retrospective review of 1599
patients. Journal of Clinical Endocrinology and Metabolism 75 714–720.
(doi:10.1210/jc.75.3.714)
Sanders LE & Silverman M 1998 Follicular and Hurthle cell carcinoma:
predicting outcome and directing therapy. Surgery 124 967–974.
(doi:10.1016/S0039-6060(98)70036-4)
Sawka AM, Thabane L, Parlea L, Ibrahim-Zada I, Tsang RW, Brierley JD,
Straus S, Ezzat S & Goldstein DP 2009 Second primary malignancy risk
after radioactive iodine treatment for thyroid cancer: a systematic
review and meta-analysis. Thyroid 19 451–457. (doi:10.1089/
thy.2008.0392)
Schlumberger M & Sherman SI 2012 Approach to the patient with
advanced differentiated thyroid cancer. European Journal of
Endocrinology 166 5–11. (doi:10.1530/EJE-11-0631)
Schlumberger M, Lacroix L, Russo D, Filetti S & Bidart JM 2007a Defects in
iodide metabolism in thyroid cancer and implications for the follow-up
and treatment of patients. Nature Clinical Practice. Endocrinology &
Metabolism 3 260–269. (doi:10.1038/ncpendmet0449)
Schlumberger M, Hitzel A, Toubert ME, Corone C, Troalen F, Schlageter
MH, Claustrat F, Koscielny S, Taieb D, Toubeau M et al. 2007b
Comparison of seven serum thyroglobulin assays in the follow-up of
papillary and follicular thyroid cancer patients. Journal of Clinical
Endocrinology and Metabolism 92 2487–2495. (doi:10.1210/
jc.2006-0723)
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access

Endocrine-RelatedCancer
Review C Durante et al. DTC follow-up 20 :4 R154
Schlumberger M, Catargi B, Borget I, Deandreis D, Zerdoud S, Bridji B,
Bardet S, Leenhardt L, Bastie D, Schvartz C et al. 2012 Strategies of
radioiodine ablation in patients with low-risk thyroid cancer. New
England Journal of Medicine 366 1663–1673. (doi:10.1056/
NEJMoa1108586)
Smallridge RC, Meek SE, Morgan MA, Gates GS, Fox TP, Grebe S &
Fatourechi V 2007 Monitoring thyroglobulin in a sensitive
immunoassay has comparable sensitivity to recombinant human
TSH-stimulated thyroglobulin in follow-up of thyroid cancer patients.
Journal of Clinical Endocrinology and Metabolism 92 82–87. (doi:10.1210/
jc.2006-0993)
Spencer CA, Takeuchi M, Kazarosyan M, Wang CC, Guttler RB, Singer PA,
Fatemi S, LoPresti JS & Nicoloff JT 1998 Serum thyroglobulin
autoantibodies: prevalence, influence on serum thyroglobulin
measurement, and prognostic significance in patients with differen-
tiated thyroid carcinoma. Journal of Clinical Endocrinology and
Metabolism 83 1121–1127. (doi:10.1210/jc.83.4.1121)
Spencer CA, LoPresti JS, Fatemi S & Nicoloff JT 1999 Detection of residual
and recurrent differentiated thyroid carcinoma by serum thyroglobulin
measurement. Thyroid 9 435–441. (doi:10.1089/thy.1999.9.435)
Torlontano M, Crocetti U, D’Aloiso L, Bonfitto N, Di Giorgio A, Modoni S,
Valle G, Frusciante V, Bisceglia M, Filetti S et al. 2003 Serum
thyroglobulin and 131I whole body scan after recombinant human TSH
stimulation in the follow-up of low-risk patients with differentiated
thyroid cancer. European Journal of Endocrinology 148 19–24.
(doi:10.1530/eje.0.1480019)
Torlontano M, Attard M, Crocetti U, Tumino S, Bruno R, Costante G,
D’Azzo G, Meringolo D, Ferretti E, Sacco R et al. 2004 Follow-up of low
risk patients with papillary thyroid cancer: role of neck ultrasono-
graphy in detecting lymph node metastases. Journal of Clinical
Endocrinology and Metabolism 89 3402–3407. (doi:10.1210/jc.
2003-031521)
Torlontano M, Crocetti U, Augello G, D’Aloiso L, Bonfitto N, Varraso A,
Dicembrino F, Modoni S, Frusciante V, Di Giorgio A et al. 2006
Comparative evaluation of recombinant human thyrotropin-
stimulated thyroglobulin levels, 131I whole-body scintigraphy, and
http://erc.endocrinology-journals.org q 2013 Society for EndocrinologyDOI: 10.1530/ERC-13-0066 Printed in Great Britain
neck ultrasonography in the follow-up of patients with papillary
thyroid microcarcinoma who have not undergone radioiodine therapy.
Journal of Clinical Endocrinology and Metabolism 91 60–63. (doi:10.1210/
jc.2005-1185)
Trapasso F, Iuliano R, Chiefari E, Arturi F, Stella A, Filetti S, Fusco A &
Russo D 1999 Iodide symporter gene expression in normal and
transformed rat thyroid cells. European Journal of Endocrinology 140
447–451. (doi:10.1530/eje.0.1400447)
Tuttle RM 2008 Risk-adapted management of thyroid cancer. Endocrine
Practice 14 764–774. (doi:10.4158/EP.14.6.764)
Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M, Brokhin M,
Omry G, Fagin JA & Shaha A 2010 Estimating risk of recurrence in
differentiated thyroid cancer after total thyroidectomy and radioactive
iodine remnant ablation: using response to therapy variables to modify
the initial risk estimates predicted by the new American Thyroid
Association staging system. Thyroid 20 1341–1349. (doi:10.1089/thy.
2010.0178)
Tuttle RM, Rondeau G & Lee NY 2011 A risk-adapted approach to the use of
radioactive iodine and external beam radiation in the treatment of
well-differentiated thyroid cancer. Cancer Control 18 89–95.
Uruno T, Miyauchi A, Shimizu K, Tomoda C, Takamura Y, Ito Y, Miya A,
Kobayashi K, Matsuzuka F, Amino N et al. 2005 Usefulness of
thyroglobulin measurement in fine-needle aspiration biopsy specimens
for diagnosing cervical lymph node metastasis in patients with
papillary thyroid cancer. World Journal of Surgery 29 483–485.
(doi:10.1007/s00268-004-7701-0)
Vaisman F, Shaha A, Fish S & Tuttle R 2011 Initial therapy with either
thyroid lobectomy or total thyroidectomy without radioactive iodine
remnant ablation is associated with very low rates of structural disease
recurrence in properly selected patients with differentiated thyroid
cancer. Clinical Endocrinology 75 112–119. (doi:10.1111/j.1365-2265.
2011.04002.x)
Van Nostrand D 2009 The benefits and risks of I-131 therapy in patients
with well-differentiated thyroid cancer. Thyroid 19 1381–1391.
(doi:10.1089/thy.2009.1611)
Received in final form 31 March 2013Accepted 9 April 2013Made available online as an Accepted Preprint9 April 2013
Published by Bioscientifica Ltd.
Downloaded from Bioscientifica.com at 11/01/2018 06:19:20AMvia free access






















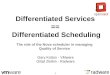


![[re]defining age - LeadingAge New Jersey](https://img.pdfslide.us/doc/110x75/5868e06a1a28ab5e1d8b8feb/redening-age-leadingage-new-jersey.jpg)