Embed Size (px)
Citation preview
38
tive, or even beneficial, changes were more frequent among pa-tients in this group.
Fears that laparoscopic electrocoagulation leads to disruptedmenstrual patterns are thus not warranted. Problems such asbowel burns and the prognosis for later re-anastomosis are ofmuch greater concern, and it is for these reasons that minila-parotomy or the application of mechanical occlusion devicesvia laparoscopy should replace laparoscopic electro-
coagulation in interval female sterilisation.International Fertility
Research Program,North Carolina 27709, U.S.A.
MARGARET F. McCANNELTON KESSEL
DIFFERENT SEROTYPES OF HUMANROTAVIRUSES
SiR,-We have been detecting rotaviruses in stools with asensitive micro complement-fixation (c.F.) technique for morethan two years.’ This method is as sensitive and specific aselectronmicroscopy (E.M.), and use of a simple absorptionmethod has avoided difficulties with anticomplementary fac-tors. The only problem is the need for a high-titre humanserum, 128 on c.F.; convalescent calf serum is not sensitiveenough for the detection of human reovirus-like particles(H.R.V.L.). We have tried to produce guineapig antiserum as analternative, and this led us, quite by chance, to considerwhether different serotypes OfH.R.V.L. might exist.
In the first attempt to produce high-titre guineapig serum aguineapig was immunised according to the technique ofMcLure et a1.2 A fxcal suspension (about 30%, w/v) of stoolno. 7 (table I) was twice centrifuged for 10 min, and the super-natant (crude H.R.v.L. antigen) was then sedimented througha 60/45/30% sucrose gradient at 100 000 g for 2t h. Completerotavirus particles (purified H.R.V.L. antigen), banding at adensity of 1.22, were then used as antigen for immunisation.
1. Zissis, G., Lambert, J. P., Dekegel, D. J. clin. Path. (in the press).2. McLure, A. R., MacFarlane, D. E., Somerville, R. G. Arch. ges. Virusforsch.
1972, 37, 6.
TABLE !——C.F. REACTIVITY OF 12 CRUDE FACAL ROTAVIRUSSUSPENSIONS OF HUMAN ORIGIN WITH THREE DIFFERENT IMMUNE
SERA
(R)=residual red bloodcells (>95% hxmolysis).TABLE 11-C.F. REACTIVITY OF TWO PURIFIED ROTAVIRUS
SUSPENSIONS OF HUMAN ORIGIN WITH THREE DIFFERENT IMMUNE
SERA
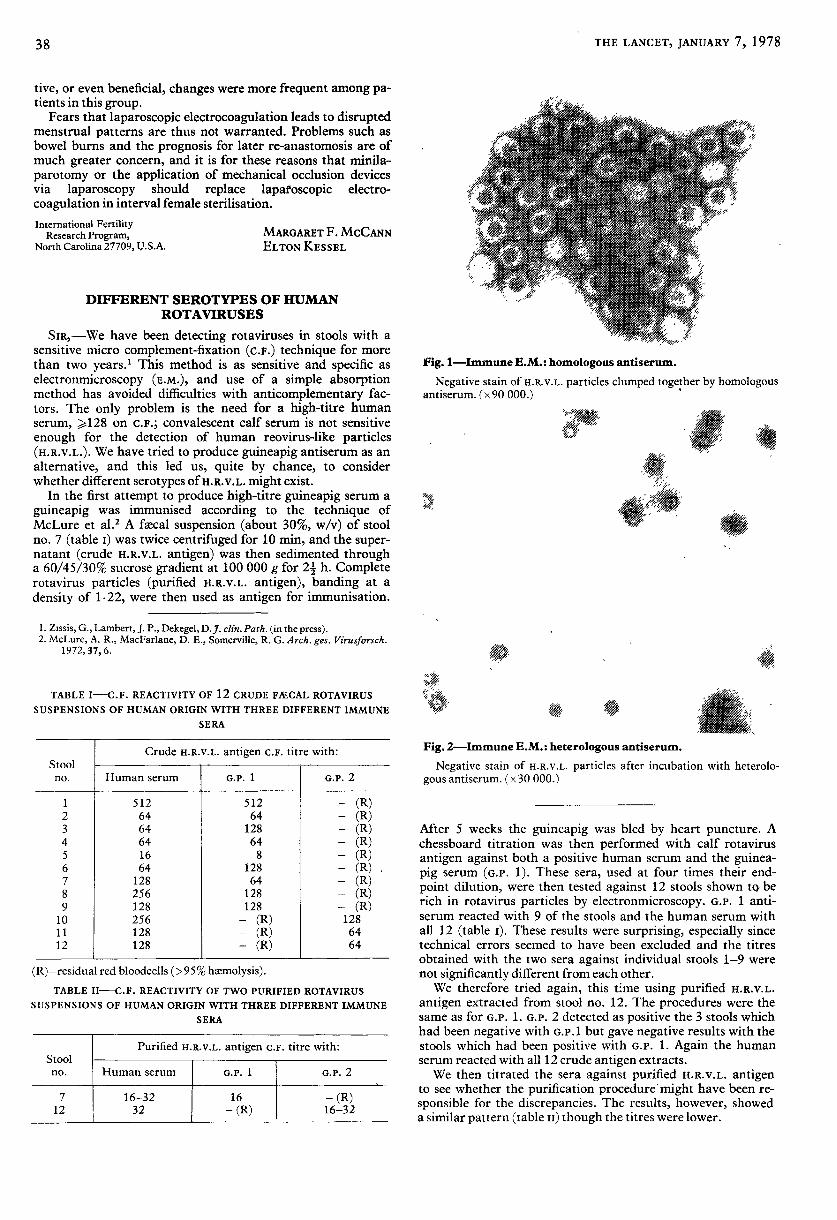
Fig. I-Immune E.M. : homologous antiserum.
Negative stain of H.R.V.L. particles clumped together by homologousantiserum. (x 90 000.)
"
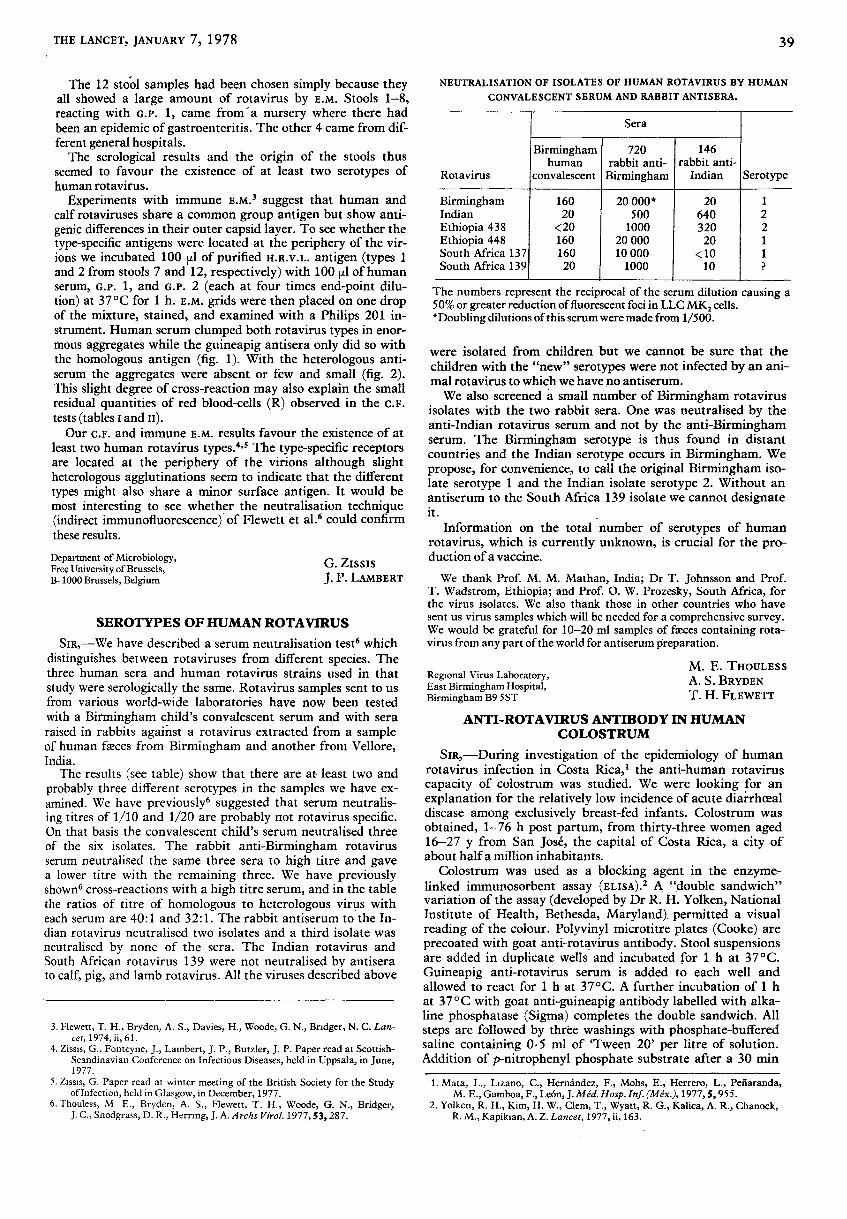
Fig. 2-Immune E.M. : heterologous antiserum.
Negative stain of H.R.V.L. particles after incubation with heterolo-gous antiserum. (x 30 000.)
After 5 weeks the guineapig was bled by heart puncture. Achessboard titration was then performed with calf rotavirusantigen against both a positive human serum and the guinea-pig serum (G.P. 1). These sera, used at four times their end-point dilution, were then tested against 12 stools shown tct berich in rotavirus particles by electronmicroscopy. G.P. 1 anti-serum reacted with 9 of the stools and the human serum withall 12 (table i). These results were surprising, especially sincetechnical errors seemed to have been excluded and the titresobtained with the two sera against individual stools 1-9 werenot significantly different from each other.We therefore tried again, this time using purified H.R.V.L.
antigen extracted from stool no. 12. The procedures were thesame as for G.P. 1. G.P. 2 detected as positive the 3 stools whichhad been negative with G.p.l but gave negative results with thestools which had been positive with G.P. 1. Again the humanserum reacted with all 12 crude antigen extracts.We then titrated the sera against purified H.R.v.L. antigen
to see whether the purification procedure might have been re-sponsible for the discrepancies. The results, however, showeda similar pattern (table 11) though the titres were lower.
39
The 12 stool samples had been chosen simply because theyall showed a large amount of rotavirus by E.M. Stools 1-8,reacting with G.P. 1, came from a nursery where there hadbeen an epidemic of gastroenteritis. The other 4 came from dif-ferent general hospitals.The serological results and the origin of the stools thus
seemed to favour the existence of at least two serotypes ofhuman rotavirus.
Experiments with immune E.M.3 suggest that human andcalf rotaviruses share a common group antigen but show anti-genic differences in their outer capsid layer. To see whether thetype-specific antigens were located at the periphery of the vir-ions we incubated 100 1 of purified H.R.V.L. antigen (types 1and 2 from stools 7 and 12, respectively) with 100 pi of humanserum, G.P. 1, and G.P. 2 (each at four times end-point dilu-tion) at 37°C for 1 h. E.M. grids were then placed on one dropof the mixture, stained, and examined with a Philips 201 in-strument. Human serum clumped both rotavirus types in enor-mous aggregates while the guineapig antisera only did so withthe homologous antigen (fig. 1). With the heterologous anti-serum the aggregates were absent or few and small (fig. 2).This slight degree of cross-reaction may also explain the smallresidual quantities of red blood-cells (R) observed in the c.F.tests (tables i and n).Our c.F. and immune E.M. results favour the existence of at
least two human rotavirus types.4,s The type-specific receptorsare located at the periphery of the virions although slightheterologous agglutinations seem to indicate that the differenttypes might also share a minor surface antigen. It would bemost interesting to see whether the neutralisation technique(indirect immunofluorescence) of Flewett et al.6 could confirmthese results.
Department of Microbiology,Free University of Brussels,B-1000 Brussels, Belgium
G. Zissis
J. P. LAMBERT
SEROTYPES OF HUMAN ROTAVIRUS
SiR,-We have described a serum neutralisation test6 whichdistinguishes between rotaviruses from different species. Thethree human sera and human rotavirus strains used in that
study were serologically the same. Rotavirus samples sent to usfrom various world-wide laboratories have now been testedwith a Birmingham child’s convalescent serum and with seraraised in rabbits against a rotavirus extracted from a sampleof human faeces from Birmingham and another from Vellore,India.
The results (see table) show that there are at least two andprobably three different serotypes in the samples we have ex-amined. We have previously6 suggested that serum neutralis-ing titres of 1/10 and 1/20 are probably not rotavirus specific.On that basis the convalescent child’s serum neutralised threeof the six isolates. The rabbit anti-Birmingham rotavirusserum neutralised the same three sera to high titre and gavea lower titre with the remaining three. We have previouslyshown6 cross-reactions with a high titre serum, and in the tablethe ratios of titre of homologous to heterologous virus witheach serum are 40:1 and 32:1. The rabbit antiserum to the In-dian rotavirus neutralised two isolates and a third isolate wasneutralised by none of the sera. The Indian rotavirus andSouth African rotavirus 139 were not neutralised by antiserato calf, pig, and lamb rotavirus. All the viruses described above
3. Flewett, T. H., Bryden, A. S., Davies, H., Woode, G. N., Bndger, N. C. Lan-cet, 1974, ii, 61.
4. Zissis, G., Fonteyne, J., Lambert, J. P., Butzler, J. P. Paper read at Scottish-Scandinavian Conference on Infectious Diseases, held in Uppsala, in June,1977.
5. Zissis, G. Paper read at winter meeting of the British Society for the Studyof Infection, held in Glasgow, in December, 1977.
6. Thouless, M E., Bryden, A. S., Flewett, T. H., Woode, G. N., Bridger,J. C., Snodgrass, D. R., Herring, J. A. Archs Virol. 1977, 53, 287.
NEUTRALISATION OF ISOLATES OF HUMAN ROTAVIRUS BY HUMAN
CONVALESCENT SERUM AND RABBIT ANTISERA.
I I I I
The numbers represent the reciprocal of the serum dilution causing a50% or greater reduction of fluorescent foci in LLC MK2 cells.*Doubling dilutions of this serum were made from 1/500.
were isolated from children but we cannot be sure that thechildren with the "new" serotypes were not infected by an ani-mal rotavirus to which we have no antiserum.We also screened a small number of Birmingham rotavirus
isolates with the two rabbit sera. One was neutralised by theanti-Indian rotavirus serum and not by the anti-Birminghamserum. The Birmingham serotype is thus found in distantcountries and the Indian serotype occurs in Birmingham. Wepropose, for convenience, to call the original Birmingham iso-late serotype 1 and the Indian isolate serotype 2. Without anantiserum to the South Africa 139 isolate we cannot designateit.
Information on the total number of serotypes of humanrotavirus, which is currently unknown, is crucial for the pro-duction of a vaccine.
We thank Prof. M. M. Mathan, India; Dr T. Johnsson and Prof.T. Wadstrom, Ethiopia; and Prof. O. W. Prozesky, South Africa, forthe virus isolates. We also thank those in other countries who havesent us virus samples which will be needed for a comprehensive survey.We would be grateful for 10-20 ml samples of faeces containing rota-virus from any part of the world for antiserum preparation.
Regional Virus Laboratory,East Birmingham Hospital,Birmingham B9 5ST
M. E. THOULESSA. S. BRYDENT. H. FLEWETT
ANTI-ROTAVIRUS ANTIBODY IN HUMANCOLOSTRUM
SiR,-During investigation of the epidemiology of humanrotavirus infection in Costa Rica,’ the anti-human rotaviruscapacity of colostrum was studied. We were looking for anexplanation for the relatively low incidence of acute diarrhoea!disease among exclusively breast-fed infants. Colostrum wasobtained, 1-76 h post partum, from thirty-three women aged16-27 y from San Jose, the capital of Costa Rica, a city ofabout half a million inhabitants.
Colostrum was used as a blocking agent in the enzyme-linked immunosorbent assay (ELISA).2 A "double sandwich"variation of the assay (developed by Dr R. H. Yolken, NationalInstitute of Health, Bethesda, Maryland) permitted a visualreading of the colour. Polyvinyl microtitre plates (Cooke) areprecoated with goat anti-rotavirus antibody. Stool suspensionsare added in duplicate wells and incubated for 1 h at 37 °C.
Guineapig anti-rotavirus serum is added to each well andallowed to react for 1 h at 37° C. A further incubation of 1 hat 370C with goat anti-guineapig antibody labelled with alka-line phosphatase (Sigma) completes the double sandwich. Allsteps are followed by three washings with phosphate-bufferedsaline containing 0.5 ml of ’Tween 20’ per litre of solution.Addition of p-nitrophenyl phosphate substrate after a 30 min
1. Mata, L., Lizano, C., Hernández, F., Mohs, E., Herrero, L., Peñaranda,M. E., Gamboa, F., Le6n, J. Med. Hosp. Inf. (Méx.), 1977, 5, 955.
2. Yolken, R. H., Kim, H. W., Clem, T., Wyatt, R. G., Kalica, A. R., Chanock,R. M., Kapikian, A. Z. Lancet, 1977, ii, 163.










![Emergence of Unusual G6P[6] Rotaviruses in Children ...Emergence of Unusual G6P[6] Rotaviruses in Children, Burkina Faso, 2009–2010 Technical Appendix Technical Appendix Table 1](https://img.pdfslide.us/doc/110x75/5f0ac8c87e708231d42d537a/emergence-of-unusual-g6p6-rotaviruses-in-children-emergence-of-unusual-g6p6.jpg)


















