Embed Size (px)
Citation preview

Epidemiologic ReviewsCopyright © 2001 by the Johns Hopkins University Bloomberg School of Public HealthAll rights reserved
Vol. 23, No. 2Printed in U.S.A.
Diet and Obstructive Lung Diseases
Isabelle Romieu1 and Carol Trenga2
INTRODUCTION
In recent studies, dietary factors have been implicated inthe cause and prevention of important diseases. Nutritionalfactors could significantly modify host response to environ-mental toxicants. An adequate diet may be able to inhibit,arrest, or even reverse the chain of events in toxicity (1),while a deficient diet could increase a person's susceptibil-ity to adverse environmental exposures, such as allergens,environmental tobacco smoke, infectious agents, and airpollution (2). Several dietary factors have been implicated inthe genesis of obstructive lung diseases, mainly because ofthe potential role of dietary factors in inflammatory reac-tions (1) and in the activities of airway smooth muscle andenzymatic reactions that affect neuromuscular transmission(3). These factors include a deficiency of antioxidant vita-mins, a lower consumption of <w-3 fatty acids, and a higherconsumption of <w-6 oils, processed foods, and salt (4).
In this paper, we examine the relation between dietaryfactors and most prevalent obstructive lung diseases, includ-ing asthma and chronic obstructive pulmonary disease(COPD). We limit our review to nutrients that have recentlybeen implicated in the genesis or severity of obstructivelung diseases; we do not address the issues of food allergy,breastfeeding, or body mass index (a combination of caloricintake and energy expenditure). First, we review the mech-anisms by which specific dietary factors may affect respira-tory health. Second, we review the epidemiologic evidencefor a link between diet and obstructive lung diseases.
Epidemiologic studies were identified through a MED-LINE search (US National Library of Medicine) on dietaryfactors and obstructive lung diseases. Studies were classi-fied by health outcome, nutrient, and study design. Theevidence is discussed in light of some of the criteria pro-posed by Hill (5) for evaluating causal relations, including
Received for publication October 6, 1999, and accepted for pub-lication July 18, 2000.
Abbreviations: Cl, confidence interval; COPD, chronic obstructivepulmonary disease; FEV,, forced expiratory volume in 1 second;NHANES, National Health and Nutrition Examination Survey; PUFA,polyunsatu rated fatty acids.
Pan American Health Organization and National Institute ofPublic Health, Center for Population Studies, Cuernavaca, Morelos,Mexico.
2 Department of Environmental Health, University of Washington,Seattle, WA.
Reprint requests to Dr. Isabelle Romieu, Instituto Nacional deSalud Publica, Avenida Universidad 655, Col. Santa MariaAhuacatitlan, 62508 Cuernavaca, Morelos, Mexico (e-mail:[email protected]).
biologic plausibility, temporality, and consistency of theassociation.
MECHANISM OF ACTION
Role of oxidants and antioxidants
Normally, the lung exists in an oxygen-rich environmentbalanced between the toxicity of oxidants (generatedthrough normal cellular function or exposure to prooxi-dants) and the protective activities of several intracellularand extracellular antioxidant defense systems. A tight con-trol of redox balance is critically important for the mainte-nance of normal pulmonary cellular function (6).Disequilibrium, either through an increase in oxidant stressor a compromise of antioxidant resources, can initiate aseries of pathophysiologic events in the lung that culminatesin cellular death and pulmonary dysfunction (7). A shift ofthe oxidant/antioxidant balance in favor of oxidants hasbeen termed "oxidative stress" (8). Researchers havehypothesized that a diet low in antioxidants such as |3-carotene and vitamins C and E may reduce natural defensesand increase susceptibility to oxidant attack and airwayinflammation (7).
Cigarette smoke and atmospheric pollutants such asozone and nitrogen oxide are rich in free radicals, and expo-sure to them can induce oxidant-mediated lung injury bydirect tissue oxidation, as well as through endogenous oxi-dizing agents and proteolytic enzymes released after recruit-ment and activation of neutrophils during the inflammatoryresponse (9). Inhaled oxidants also amplify the effect ofneutrophil proteases by oxidative deactivation of a-1-proteinase inhibitor (6, 10).
The antioxidant defenses of the lung have recently beenreviewed (7, 10-13). Antioxidants are the first line of defenseagainst oxygen free radicals, which are capable of damagingcellular components and contributing to inflammation.Briefly, the major antioxidant system available to cells dur-ing oxidative stress is that of free-radical-scavenging agents.These agents are present to varying degrees in the intracellu-lar and extracellular spaces, and they function by either elim-inating oxidants or preventing their conversion to more toxiccompounds (8). Antioxidants may act at different levels inthe oxidation process—for example, by scavenging initiatingradicals, binding metal ions; by scavenging peroxyl radicals;or by removing oxidatively damaged biomolecules (8).Antioxidant defenses in the lung are provided by endogenousenzyme systems and nonenzymatic antioxidant compounds.The major enzymatic antioxidants are superoxide dismutase,
268
Diet and Obstructive Lung Diseases 269
which degrades superoxide anion, and catalase and the glu-tathione redox system, which inactivates hydrogen peroxide(11). Nonenzymatic antioxidants such as vitamin E (a-tocopherol), vitamin C (ascorbic acid), and p-carotene (a pre-cursor of vitamin A), ubiquinone, flavonoids, and seleniumare present in foods and are considered dietary antioxidants(8).
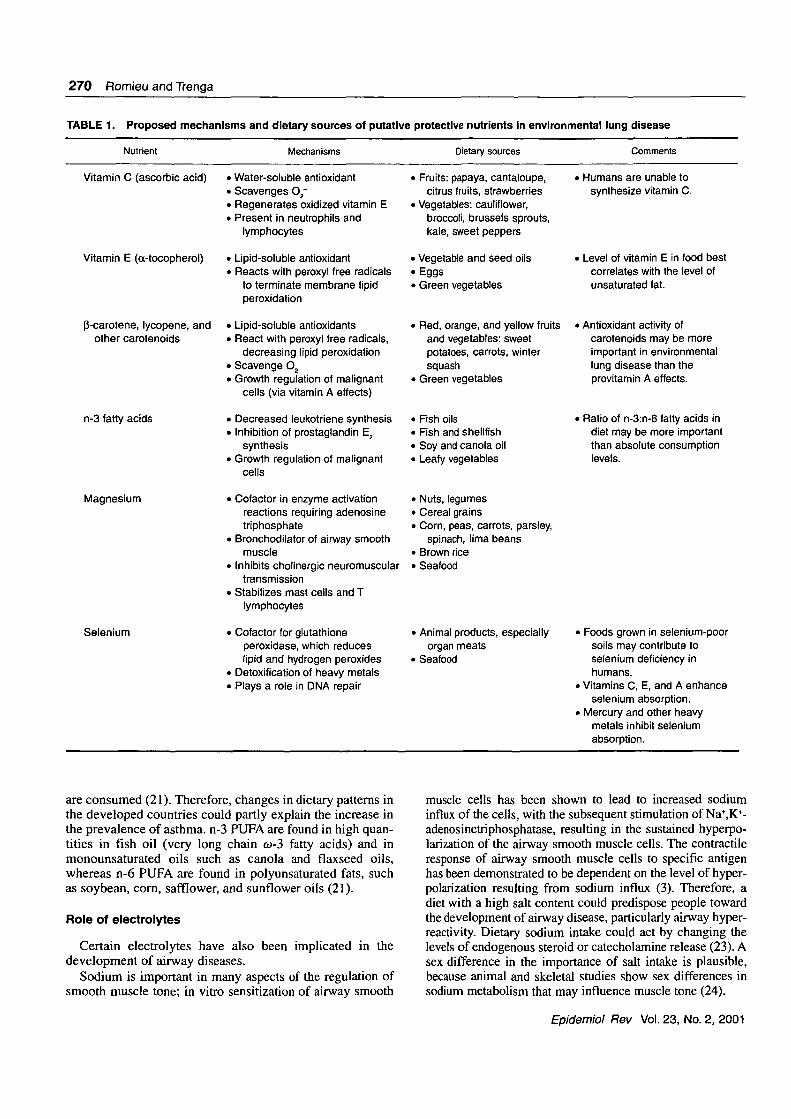
Vitamin E, a lipid-soluble vitamin, represents the body'sprincipal defense against oxidant-induced membrane injuryin human tissue, via its role in breaking the lipid peroxidationchain reaction (14). Vitamin C, a water-soluble vitamin, con-tributes to antioxidant activity through several mechanisms,including scavenging the superoxide radical O2~. Vitamin Cacts on airways by affecting arachidonic acid metabolites,particularly prostaglandins. An antagonist effect of vitamin Con prostaglandin F2a-induced bronchoconstriction has beenshown in animals (3). Vitamin C appears to be the mostabundant antioxidant substance in the extracellular fluid lin-ing of the lung (15), and it also contributes to the regenera-tion of membrane-bound oxidized vitamin E, allowing it tofunction again as a chain-breaking antioxidant (16). In addi-tion, vitamin C plays a role in immune function and is trans-ported into neutrophils and lymphocytes (12). P-Carotene, aprecursor to vitamin A, accumulates in tissue membranes,scavenges superoxide anion, and reacts directly with peroxylfree radicals, thereby serving as a lipid-soluble antioxidant(8). Thus, dietary intake of these vitamins may play a role inhost defense against oxidative lung damage. Flavonoids suchas quercetin are scavengers of superoxide anion; they exhibitsinglet oxygen-quenching proprieties, scavenge lipid peroxylradicals, and can act as chelators of iron ions (8). Selenium isincorporated into the antioxidant enzyme glutathione perox-idase, which reduces hydrogen peroxide and other organicperoxides, thereby preventing lipid peroxidation and subse-quent instability of cell membranes (3). Selenium also has anoverlapping function with vitamin E (17) (see table 1).
Antioxidant intake may act primarily on the evolution ofasthma, modulating the impact of oxidants on the lung,decreasing inflammation of the airway. Infection andinhaled pollutants activate leukocytes to produce oxidants.Eosinophils, alveolar macrophages, and neutrophils fromasthmatic patients produce more reactive oxygen speciesthan do those from normal subjects. Reactive oxygenspecies directly contract airway smooth muscle preparation(18) and can stimulate histamine release from mast cells(15). A number of antioxidant disturbances have also beenobserved in COPD patients, and the involvement of oxida-tive stress in COPD has been indicated through higherhydrogen peroxide exhalation, an increase in lipid peroxida-tion products, and DNA damage. Cigarette smoke, a majorrisk factor for COPD, is a significant source of oxidants;smokers have been found to have decreased levels of plasmaascorbate, p-carotene, and vitamin E (11). In addition, thecoexistence of airway inflammation and parenchymalinflammation is observed in most patients with COPD.Therefore, antioxidant intake could modulate the lung dam-age induced by oxidative stress (11).
Fresh fruits and vegetables contain considerable amountsof vitamin C (e.g., broccoli, spinach, tomatoes, and citrus
fruits) and carotenoids (e.g., carrots, tomatoes, grapefruit,beans, broccoli, oranges, and mangos) (19). The maincarotenoids serving as provitamin A, a- and P-carotene andcryptoxanthin, may be transformed into vitamin A. The rich-est sources of vitamin E in the human diet are oil productssuch as mayonnaise, vegetable and seed oils (corn, safflower,and soybean), butter, and eggs. Flavonoids are mainly foundin fruits and vegetables (apples, lemons, oranges, potatoes,and cauliflower) and tea (8). Selenium is found in grain,meat, seafood, and certain vegetables. The currentRecommended Dietary Allowance requirements are 60mg/day for vitamin C (100 mg/day for smokers), 800-1,000retinol equivalents per day (1 retinol equivalent = 6 (ig of P-carotene) for vitamin A, 8—10 mg/day for a-tocopherol, and55-70 u.g/day for selenium (20).
Role of co-3 and «-6 fatty acids
Patterns of consumption of <o-3 and <D-6 fatty acids havebeen related to the development of airway inflammation. Inbrief, w-3 polyunsaturated fatty acids (n-3 PUFA), which arestored in cell membranes, have an important role in control-ling inflammation (4) but are easily replaced by co-6 polyun-saturated fatty acids (n-6 PUFA), which facilitate the devel-opment of inflammation. The most abundant n-6 PUFA inthe Western diet, linoleic acid (18:2n-6), is converted toarachidonic acid, a progenitor of both prostaglandin E2 andleukotriene B4 via cyclooxygenase and 5-lipoxygenaseenzymatic pathways, respectively. Both prostaglandin E2
and leukotriene B4 have proinflammatory biologic actions.In contrast, oc-linolenic acid (18:3n-3) n-3 PUFA is con-
verted to eicosapentaenoic acid (20:5n-3), which can inhibitarachidonic acid metabolism competitively via the enzy-matic pathways and thereby suppress production of the n-6eicosanoid inflammatory mediators. Eicosapentaenoic acidis a potential cyclooxygenase substrate for the synthesis ofprostaglandin E3 and a 5-lipooxygenase substrate for thesynthesis of leukotriene B5. Both prostaglandin E3 andleukotriene B5 have little inflammatory activity in compari-son with prostaglandin E2 and leukotriene B4. Thus, increas-ing dietary n-3 PUFA can shift the balance of theeicosanoids produced to a less inflammatory mixture (21).Prostaglandin E2 acts on T lymphocytes to reduce the for-mation of interferon-y without affecting the formation ofinterleukin-4. This may lead to the development of allergicsensitization, since interleukin-4 promotes the synthesis ofimmunoglobulin E, whereas interferon-y has the oppositeeffect (22). Leukotriene B4 increases postcapillary vascularpermeability, is a potent stimulator of airway smooth mus-cle cells, and mediates pulmonary asthma through involve-ment in vasoconstriction and mucus secretion, n-3 PUFAmay also suppress the production of tumor necrosis factor-aand interleukin-lp; however, the mechanism for this sup-pression remains unknown (21).
The competitive interactions between n-6 PUFA and n-3PUFA determine the cellular content of arachidonic acid andeicosapentaenoic acid. A higher concentration of eicosapen-taenoic acid occurs in diets low in linoleic acid. In theWestern diet, 20- to 25-fold more n-6 PUFA than n-3 PUFA
Epidemiol Rev Vol. 23, No. 2, 2001
270
TABLE
Romieu and Trenga
1. Proposed mechanisms and dietary sources of putative
Nutrient Mechanisms
protective nutrients in
Dietary sources
environmental lung disease
Comments
Vitamin C (ascorbic acid)
Vitamin E (a-tocopherol)
P-carotene, lycopene, andother carotenoids
n-3 fatty acids
Magnesium
Selenium
• Water-soluble antioxidant• Scavenges O2'• Regenerates oxidized vitamin E• Present in neutrophils and
lymphocytes
• Lipid-soluble antioxidant• Reacts with peroxyl free radicals
to terminate membrane lipidperoxidation
• Lipid-soluble antioxidants• React with peroxyl free radicals,
decreasing lipid peroxidation• Scavenge O2~• Growth regulation of malignant
cells (via vitamin A effects)
• Decreased leukotriene synthesis• Inhibition of prostaglandin E2
synthesis• Growth regulation of malignant
cells
• Cofactor in enzyme activationreactions requiring adenosinetriphosphate
• Bronchodilator of airway smoothmuscle
• Inhibits cholinergic neuromusculartransmission
• Stabilizes mast cells and Tlymphocytes
• Cofactor for glutathioneperoxidase, which reduceslipid and hydrogen peroxides
• Detoxification of heavy metals• Plays a role in DNA repair
> Fruits: papaya, cantaloupe,citrus fruits, strawberries
> Vegetables: cauliflower,broccoli, brussels sprouts,kale, sweet peppers
> Vegetable and seed oils-Eggs> Green vegetables
• Red, orange, and yellow fruitsand vegetables: sweetpotatoes, carrots, wintersquash
• Green vegetables
• Fish oils• Fish and shellfish• Soy and canola oil• Leafy vegetables
' Nuts, legumes> Cereal grains> Corn, peas, carrots, parsley,
spinach, lima beans• Brown rice' Seafood
> Animal products, especiallyorgan meats
• Seafood
i Humans are unable tosynthesize vitamin C.
• Level of vitamin E in food bestcorrelates with the level ofunsaturated fat.
> Antioxidant activity ofcarotenoids may be moreimportant in environmentallung disease than theprovitamin A effects.
> Ratio of n-3:n-6 fatty acids indiet may be more importantthan absolute consumptionlevels.
> Foods grown in selenium-poorsoils may contribute toselenium deficiency inhumans.
> Vitamins C, E, and A enhanceselenium absorption.
> Mercury and other heavymetals inhibit seleniumabsorption.
are consumed (21). Therefore, changes in dietary patterns inthe developed countries could partly explain the increase inthe prevalence of asthma, n-3 PUFA are found in high quan-tities in fish oil (very long chain eo-3 fatty acids) and inmonounsaturated oils such as canola and flaxseed oils,whereas n-6 PUFA are found in polyunsaturated fats, suchas soybean, corn, safflower, and sunflower oils (21).
Role of electrolytes
Certain electrolytes have also been implicated in thedevelopment of airway diseases.
Sodium is important in many aspects of the regulation ofsmooth muscle tone; in vitro sensitization of airway smooth
muscle cells has been shown to lead to increased sodiuminflux of the cells, with the subsequent stimulation of Na+,K+-adenosinetriphosphatase, resulting in the sustained hyperpo-larization of the airway smooth muscle cells. The contractileresponse of airway smooth muscle cells to specific antigenhas been demonstrated to be dependent on the level of hyper-polarization resulting from sodium influx (3). Therefore, adiet with a high salt content could predispose people towardthe development of airway disease, particularly airway hyper-reactivity. Dietary sodium intake could act by changing thelevels of endogenous steroid or catecholamine release (23). Asex difference in the importance of salt intake is plausible,because animal and skeletal studies show sex differences insodium metabolism that may influence muscle tone (24).
Epidemiol Rev Vol. 23, No. 2, 2001

Diet and Obstructive Lung Diseases 271
Magnesium may also influence airway disease, because itis involved in maintaining electric potential across cellmembranes and may therefore have a direct action onbronchial smooth muscle, producing airway dilatation (3).Magnesium is an essential cofactor for enzymes that requireadenosine triphosphate, and it is involved in the synthesisand replication of RNA and DNA. Magnesium has beenshown to relax airway smooth muscle in vitro, to bron-chodilate asthmatic airways in vivo, to inhibit cholinergicneuromuscular transmission, to stabilize mast cells and Tlymphocytes, and to stimulate the generation of nitric oxideand prostacyclin (25). A diet low in magnesium could there-fore be a risk factor for airway diseases. Magnesium in thediet is obtained principally from cereals, nuts, green vegeta-bles, and dairy products (17).
EPIDEMIOLOGIC STUDIES
Methodological issues
Study design. Two major types of studies have been usedto investigate the impact of diet on obstructive lung diseases:experimental studies, in which patients were randomlyassigned to receive diet supplement or placebo, and cross-sectional studies, in which dietary intake was assessedsimultaneously with airway responsiveness, change in lungfunctions, or respiratory symptoms. Although the experimen-tal study design is more likely to provide information on atrue causal relation, the existing studies were conducted inclinical settings on small numbers of patients, which limitsthe application of the results to larger populations. They usu-ally focused on acute outcomes such as bronchoconstrictionand were aimed at determining the potential for nutritionaltherapy in the management of obstructive lung disease, par-ticularly asthma. In contrast, most of the epidemiologic datafrom free-living populations are based on cross-sectionalstudies of adults or children that evaluated dietary factorsamong people with and without disease at a single point intime. These studies aimed at determining risk factors forprevalent obstructive lung diseases; however, because of theircross-sectional nature, they cannot provide information on thetemporal relation between dietary intake and lung diseases.For instance, there is a possibility that subjects with prevalentsymptoms may alter their diet as a result of their symptoms,thus altering the nature of the association. In addition, there isuncertainty about the biologically relevant exposure win-dow^), and dietary agents might plausibly act at differentstages of the disease process. It is likely that, as in otherchronic diseases, nutrient intake several years prior to diag-nosis may be the most relevant in relation to the developmentof obstructive lung diseases. In addition, the difficulty ofreconstructing past dietary intake renders difficult the inter-pretation of cross-sectional data.
There have been few cohort studies that have enrolledpersons initially free of disease and evaluated the incidenceof lung disease over time. Because the estimation of dietaryintake precedes the diagnosis of obstructive lung disease,results from these studies provide a correct temporal rela-tion. However, a cohort study is costly and time-consumingto carry out. It is also difficult to assess long-term dietary
intake in these studies because of changes in nutrient statusduring the long follow-up periods needed, particularly forCOPD; and lack of knowledge on the relevant window ofsusceptibility may lead to misclassification of the exposureof interest. However, the cohort design is the only observa-tional design that provides the elements needed to establisha causal relation between diet and obstructive lung diseases.
Assessment of dietary intake. Different methods havebeen used for dietary assessment across studies, includingmeasurement of biomarkers of intake and administration ofdietary questionnaires such as 24-hour recalls, food fre-quency questionnaires, and diet histories. Biochemical indi-cators of dietary intake include serum vitamin C levels andurinary sodium and potassium excretion. These biomarkersreflect recent intake (26) and therefore will not provide ade-quate information on long-term intake, the most relevantrisk factor for chronic disease. In addition, some factors,such as exposure to tobacco smoke, will decrease serum lev-els of vitamin C (11, 19) and therefore provide erroneousinformation on dietary intake. Similarly, assessment ofnutrient intake based on 24-hour dietary recalls provides apoor measurement of usual intake because of potentiallywide variation from day to day, particularly for micronutri-ents such as electrolytes and vitamins, and it has been notedto be more variable than use of semiquantitative food fre-quency questionnaires, which gather data on average dietaryintake over a period of several months or years (27). Whilethe use of a food frequency questionnaire provides betterassessment of food intake, it still results in random error inthe measurement of dietary intakes and thus may lead tounderestimation of the relation between dietary factors andlung disease (28).
For some nutrients, such as vitamin E and selenium, rely-ing on dietary assessment methods to classify individuals isproblematic, since accurate data on food content are limited.Selenium content will vary according to the origin of thefood. Additionally, intake of fats from oils, which are rich invitamin E, is difficult to discern in quantity (29). Finally,because few studies consider more than one nutrient in theiranalyses, a protective or adverse effect attributed to onenutrient or micronutrient, such as vitamin C, may actuallyreflect the effect of another, correlated dietary constituent oran interaction between dietary constituents. It is particularlydifficult to exclude the possibility that another component ofcertain fruits or vegetables may have a true protective effect(27). These issues are particularly relevant when consideringthe endpoints used in different studies. While the use of anindicator of short-term intake may be adequate for an acuteoutcome such as bronchoconstriction, it is not adequate for achronic outcome such as decrement in lung function.
Epidemiologic studies of diet and airflow limitation
Obstructive lung diseases such as asthma and COPD havein common airway narrowing, with a consequent increase inthe work of breathing. Intraluminal airway obstruction hasmultiple causes. Airway smooth muscle contraction, a clas-sic mechanism in asthma, is the most commonly consideredcause of airway narrowing. Infiltration with inflammatory
Epidemiol Rev Vol. 23, No. 2, 2001
272 Romieu and Trenga
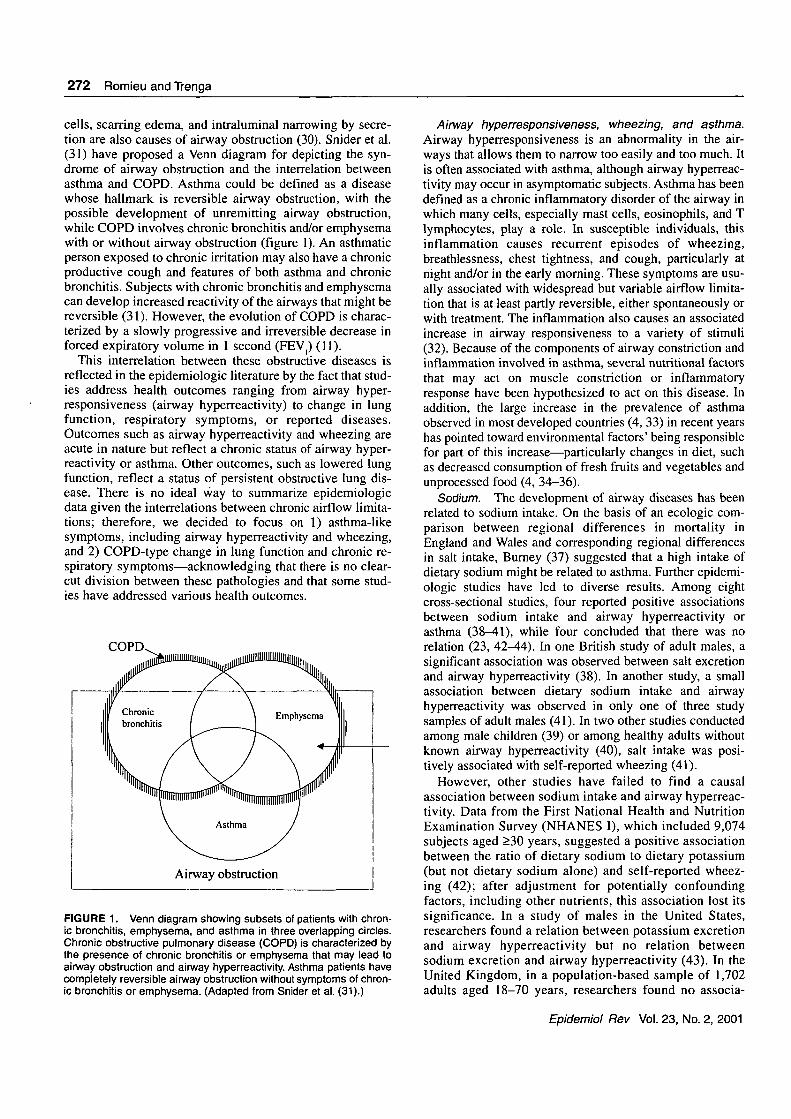
cells, scarring edema, and intraluminal narrowing by secre-tion are also causes of airway obstruction (30). Snider et al.(31) have proposed a Venn diagram for depicting the syn-drome of airway obstruction and the interrelation betweenasthma and COPD. Asthma could be defined as a diseasewhose hallmark is reversible airway obstruction, with thepossible development of unremitting airway obstruction,while COPD involves chronic bronchitis and/or emphysemawith or without airway obstruction (figure 1). An asthmaticperson exposed to chronic irritation may also have a chronicproductive cough and features of both asthma and chronicbronchitis. Subjects with chronic bronchitis and emphysemacan develop increased reactivity of the airways that might bereversible (31). However, the evolution of COPD is charac-terized by a slowly progressive and irreversible decrease inforced expiratory volume in 1 second (FEV,) (11).
This interrelation between these obstructive diseases isreflected in the epidemiologic literature by the fact that stud-ies address health outcomes ranging from airway hyper-responsiveness (airway hyperreactivity) to change in lungfunction, respiratory symptoms, or reported diseases.Outcomes such as airway hyperreactivity and wheezing areacute in nature but reflect a chronic status of airway hyper-reactivity or asthma. Other outcomes, such as lowered lungfunction, reflect a status of persistent obstructive lung dis-ease. There is no ideal way to summarize epidemiologicdata given the interrelations between chronic airflow limita-tions; therefore, we decided to focus on 1) asthma-likesymptoms, including airway hyperreactivity and wheezing,and 2) COPD-type change in lung function and chronic re-spiratory symptoms—acknowledging that there is no clear-cut division between these pathologies and that some stud-ies have addressed various health outcomes.
COPD
FIGURE 1. Venn diagram showing subsets of patients with chron-ic bronchitis, emphysema, and asthma in three overlapping circles.Chronic obstructive pulmonary disease (COPD) is characterized bythe presence of chronic bronchitis or emphysema that may lead toairway obstruction and airway hyperreactivity. Asthma patients havecompletely reversible airway obstruction without symptoms of chron-ic bronchitis or emphysema. (Adapted from Snider et al. (31).)
Airway hyperresponsiveness, wheezing, and asthma.Airway hyperresponsiveness is an abnormality in the air-ways that allows them to narrow too easily and too much. Itis often associated with asthma, although airway hyperreac-tivity may occur in asymptomatic subjects. Asthma has beendefined as a chronic inflammatory disorder of the airway inwhich many cells, especially mast cells, eosinophils, and Tlymphocytes, play a role. In susceptible individuals, thisinflammation causes recurrent episodes of wheezing,breathlessness, chest tightness, and cough, particularly atnight and/or in the early morning. These symptoms are usu-ally associated with widespread but variable airflow limita-tion that is at least partly reversible, either spontaneously orwith treatment. The inflammation also causes an associatedincrease in airway responsiveness to a variety of stimuli(32). Because of the components of airway constriction andinflammation involved in asthma, several nutritional factorsthat may act on muscle constriction or inflammatoryresponse have been hypothesized to act on this disease. Inaddition, the large increase in the prevalence of asthmaobserved in most developed countries (4, 33) in recent yearshas pointed toward environmental factors' being responsiblefor part of this increase—particularly changes in diet, suchas decreased consumption of fresh fruits and vegetables andunprocessed food (4, 34-36).
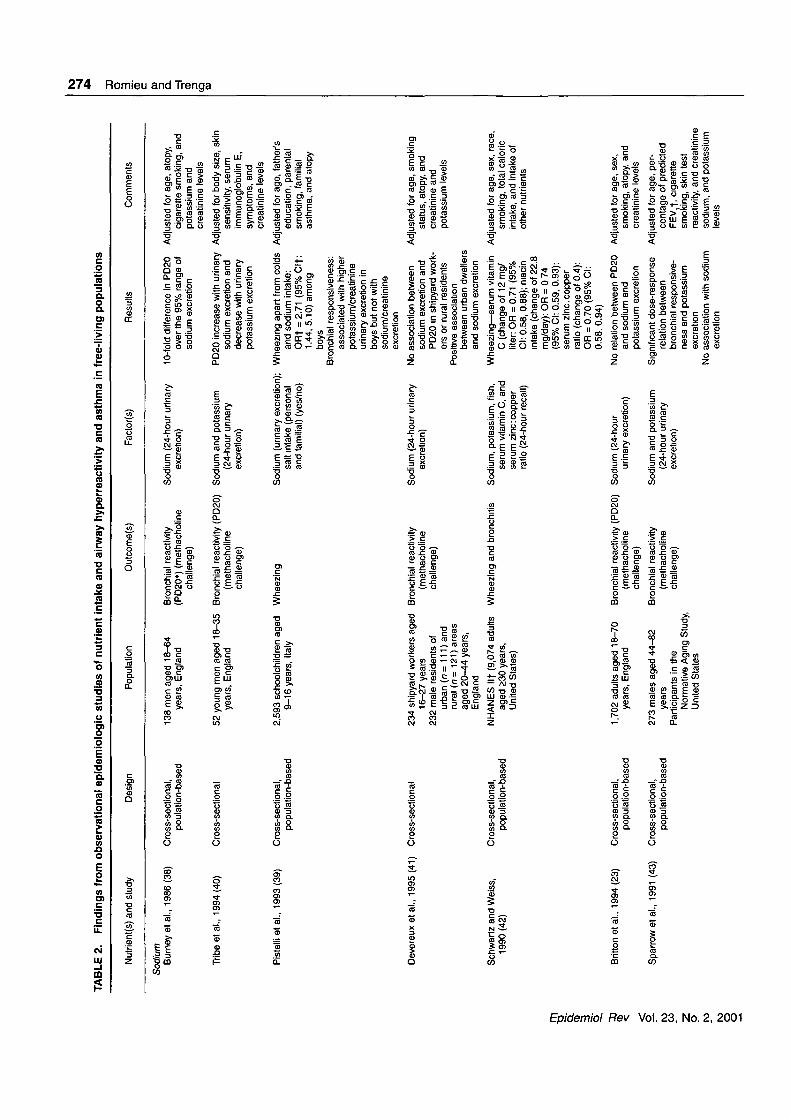
Sodium. The development of airway diseases has beenrelated to sodium intake. On the basis of an ecologic com-parison between regional differences in mortality inEngland and Wales and corresponding regional differencesin salt intake, Burney (37) suggested that a high intake ofdietary sodium might be related to asthma. Further epidemi-ologic studies have led to diverse results. Among eightcross-sectional studies, four reported positive associationsbetween sodium intake and airway hyperreactivity orasthma (38-41), while four concluded that there was norelation (23, 42^44). In one British study of adult males, asignificant association was observed between salt excretionand airway hyperreactivity (38). In another study, a smallassociation between dietary sodium intake and airwayhyperreactivity was observed in only one of three studysamples of adult males (41). In two other studies conductedamong male children (39) or among healthy adults withoutknown airway hyperreactivity (40), salt intake was posi-tively associated with self-reported wheezing (41).
However, other studies have failed to find a causalassociation between sodium intake and airway hyperreac-tivity. Data from the First National Health and NutritionExamination Survey (NHANES I), which included 9,074subjects aged >30 years, suggested a positive associationbetween the ratio of dietary sodium to dietary potassium(but not dietary sodium alone) and self-reported wheez-ing (42); after adjustment for potentially confoundingfactors, including other nutrients, this association lost itssignificance. In a study of males in the United States,researchers found a relation between potassium excretionand airway hyperreactivity but no relation betweensodium excretion and airway hyperreactivity (43). In theUnited Kingdom, in a population-based sample of 1,702adults aged 18-70 years, researchers found no associa-
Epidemiol Rev Vol. 23, No. 2, 2001
Diet and Obstructive Lung Diseases 273
tion between 24-hour urinary sodium excretion and air-way hyperreactivity (23).
All of the studies noted above were cross-sectional indesign and evaluated the relation between airway hyper-reactivity and sodium intake as assessed through 24-hoururinary excretion (23, 38, 41, 43) or dietary questionnaires(39, 42, 44) (table 2). The discrepancies in results betweenstudies have been attributed to a number of factors: the lowstatistical power of small studies; a lack of control for thepotentially confounding effect of smoking (38, 39); misclas-sification due to the fact that dietary intakes are variable andinherently difficult to quantify; and the inadequacy of saltexcretion as a marker for total dietary intake over a pro-longed period (4). Some authors have also suggested that theassociation between airway hyperreactivity and sodiumintake may be confounded by other dietary factors corre-lated with sodium intake, such as intake of magnesium (25)or vitamin C (42). A high salt intake is generally associatedwith a diet that is poor in fresh fruits and vegetables. Onlyone study adjusted for intake of other nutrients, and resultsdid not confirm an association between dietary salt intakeand wheezing (42).
Experimental studies have also produced conflictingresults. Burney et al. (45) reported a greater bronchialresponse to histamine among asthma patients taking asodium supplement as compared with those taking a placebo.These results were observed only among men, and no signif-icant change in FEV, was seen in either group during thestudy. Similarly, Carey et al. (46) reported an increase in air-way hyperreactivity and respiratory symptoms among asth-matic patients receiving a sodium supplement as comparedwith those receiving placebo. In addition, a decrease in FEV,was observed in the supplement-taking group. Medici et al.(47) observed a decrease in FEV, and peak expiratory flowrate among asthmatic patients receiving sodium supplementsbut no change in airway hyperreactivity. Another experimen-tal study (48) failed to find an effect of dietary sodium levelson bronchial responsiveness. Although these studies sug-gested that increased sodium intake may adversely affect thebronchopulmonary system in small groups of asthmaticpatients, the fact that the increase in airway hyperreactivitywas found only among males raises some concern about thepathogenesis of this effect, which may or may not involve theairway smooth muscles. In addition, these studies providedlittle support for the adoption of a low-salt diet by patientswith asthma (3). On the basis of experimental data, anincrease in salt consumption could be associated with anincrease in airway hyperreactivity among asthmatic individ-uals, but there is no evidence of an impact of sodium intakeon the increase in asthma incidence.
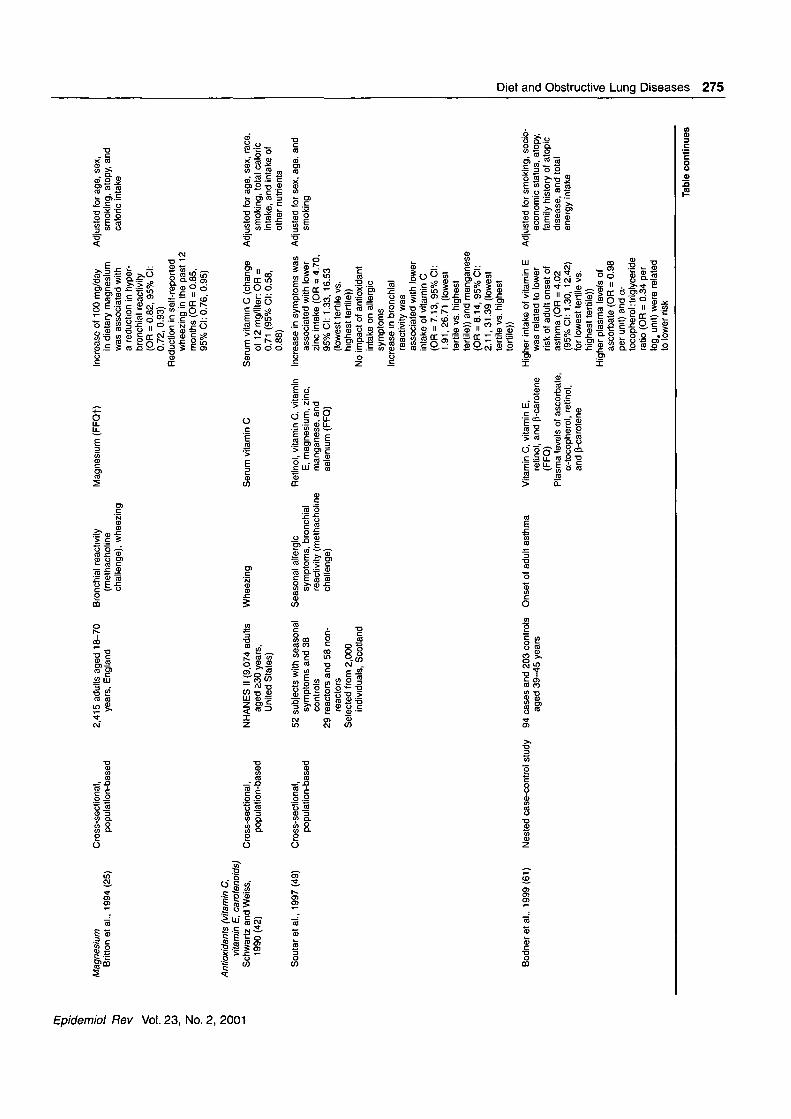
Magnesium. Few epidemiologic studies have investi-gated the impact of magnesium intake on airway reactivity(table 2). In a cross-sectional UK study of 2,633 adults aged18-70 years, Britton et al. (25) reported that a 100-mg/dayhigher magnesium intake (assessed by semiquantitative foodfrequency questionnaire) was associated with both a reduc-tion in airway hyperreactivity (odds ratio = 0.82, 95 percentconfidence interval (CI): 0.72, 0.93) and a higher FEV,.They also observed a reduction in self-reported wheezing in
the previous months (odds ratio = 0.85, 95 percent CI: 0.76,0.95). Data were adjusted for potential confounders such asage, sex, height, atopy, smoking, caloric intake, and vitaminC intake. The dose-response characteristics of this associa-tion suggest that FEV, increases in approximately linear rela-tion to magnesium intake up to the level of 400 mg/day.Britton et al. suggested that, in previous studies, magnesiumcould have confounded the association between sodium orpotassium and airway hyperreactivity and asthma. In a case-control study conducted in Scotland, decreasing intake ofmagnesium was also related to an increased risk of airwayhyperreactivity (49).
Experimental studies have not confirmed the associationbetween magnesium intake and airway hyperreactivity andpulmonary functions. Magnesium infusion among patientswith acute asthma exacerbation has produced either a tran-sient improvement in FEV, (50) or no improvement (51). Ina randomized trial among 17 stable asthmatic patients, Hillet al. (52) reported no significant improvement in airwayhyperreactivity or FEV, during a 3-week magnesium sup-plementation period, although high magnesium intake wasassociated with improvement in symptom scores. Someauthors have also measured serum and intracellular magne-sium levels (erythrocytes and mononuclear leukocytes).Because magnesium is largely intracellular, it is thought thatmagnesium levels in erythrocytes and leukocytes are moreaccurate measures of magnesium status than serum levels.In a study by De Valk et al. (53), no significant differencewas found between asthmatic patients and nonasthmaticcontrols in either extracellular or intracellular magnesiumlevels.
On the basis of experimental data, there is no clear evi-dence that magnesium intake may have an impact on thegenesis or evolution of chronic asthma. Although magne-sium intake was found to have a beneficial effect on the lungin two studies conducted in free-living populations (25, 49),diet was evaluated retrospectively in those studies. In addi-tion, the association between magnesium and respiratoryoutcomes might be confounded by intake of other micronu-trients that may be correlated with magnesium intake, suchas calcium, potassium, or selenium.
Antioxidants. Some researchers have hypothesized thata deficiency in dietary antioxidants could contribute toasthma, because 1) the US diet has grown deficient in foodscontaining antioxidants (34) while the asthma rate hasincreased and 2) there is increasing evidence for a role ofantioxidants in lung defense mechanisms. In a recentreview, Hatch (15) suggested that oxidant exposure, partic-ularly in infancy, could be a causative factor for asthma.Oxidants could increase susceptibility to infections that inturn cause lung injury. This injury or inflammation couldfurther be an underlying cause of asthma (15).
Exposure to oxidants from different sources, includingcigarette smoke, air pollutants, and endogenous sources, hasbeen related to asthma incidence or severity (54, 55).Cigarette smoke is one of the most potent oxidants, and ithas been shown to result in oxidation of plasma vitamin Cand vitamin E (56). Smoking during pregnancy and expo-sure to environmental tobacco smoke have been related to
Epidemiol Rev Vol. 23, No. 2, 2001
3§;3D
<
2.-oj3
zO
ro, POO
TABLE 2. Findings from observational epidemiologic studies of nutrient intake and airway hyperreactivity and asthma in
Nutrient(s) and study Design
SodiumBurney et al., 1986 (38) Cross-sectional,
poulation-based
Tribe et al., 1994 (40) Cross-sectional
Pistelli et al., 1993 (39) Cross-sectional,population-based
Devereux et al., 1995 (41) Cross-sectional
Schwartz and Weiss, Cross-sectional,1990(42) population-based
Britton et al., 1994 (23) Cross-sectional,population-based
Sparrow et al., 1991 (43) Cross-sectional,population-based
Population
138 men aged 18-64years, England
52 young men aged 18-35years, England
2,593 schoolchildren aged9-16 years, Italy
234 shipyard workers aged16-27 years
232 male residents ofurban (n = 111) andrural (n= 121) areasaged 20-44 years,England
NHANES l i t (9,074 adultsaged 230 years,United States)
1,702 adults aged 18-70years, England
273 males aged 44-82years
Participants in theNormative Aging Study,United States
Outcome(s)
Bronchial reactivity(PD20*) (methacholine
challenge)
Bronchial reactivity (PD20)(methacholinechallenge)
Wheezing
Bronchial reactivity(methacholinechallenge)
Wheezing and bronchitis
Bronchial reactivity (PD20)(methacholinechallenge)
Bronchial reactivity(methacholinechallenge)
Factor(s)
Sodium (24-hour urinaryexcretion)
Sodium and potassium(24-hour urinaryexcretion)
Sodium (urinary excretion);salt intake (personaland familial) (yes/no)
Sodium (24-hour urinaryexcretion)
Sodium, potassium, fish,serum vitamin C, andserum zinc:copperratio (24-hour recall)
Sodium (24-hoururinary excretion)
Sodium and potassium(24-hour urinaryexcretion)
free-living populations
Results
10-fold difference in PD20over the 95% range ofsodium excretion
PD20 increase with urinarysodium excretion anddecrease with urinarypotassium excretion
Wheezing apart from coldsand sodium intake:ORt = 2.71 (95%Clt:1.44, 5.10) amongboys
Bronchial responsiveness:associated with higherpotassium/creatinineurinary excretion inboys but not withsodium/creatinineexcretion
No association betweensodium excretion andPD20 in shipyard work-ers or rural residents
Positive associationbetween urban dwellersand sodium excretion
Wheezing—serum vitaminC (change of 12 mg/liter: OR = 0.71 (95%Cl: 0.58, 0.88); niacinintake (change of 22.8mg/day): OR = 0 74(95% Cl: 0.59, 0.93);serum zinc.copperratio (change of 0.4):OR = 0.70 (95% Cl:0.58, 0.94)
No relation between PD20and sodium andpotassium excretion
Significant dose-responserelation betweenbronchial responsive-ness and potassiumexcretion
No association with sodiumexcretion
Comments
Adjusted for age, atopy,cigarette smoking, andpotassium andcreatinine levels
Adjusted for body size, skinsensitivity, serumimmunoglobulin E,symptoms, andcreatinine levels
Adjusted for age, father'seducation, parentalsmoking, familialasthma, and atopy
Adjusted for age, smokingstatus, atopy, andcreatinine andpotassium levels
Adjusted for age, sex, race,smoking, total caloricintake, and intake ofother nutrients
Adjusted for age, sex,smoking, atopy, andcreatinine levels
Adjusted for age, per-centage of predictedFEV,f, cigarettesmoking, skin testreactivity, and creatininesodium, and potassiumlevels
274 Ftom
iei
Q.—iCD
<QW
I
CO
MagnesiumBritton et al., 1994 (25)
Cross-sectional,population-based
2,415 adults aged 18-70years, England
Bronchial reactivity(methacholinechallenge), wheezing
Magnesium (FFQf) Increase of 100 mg/dayin dietary magnesiumwas associated witha reduction in hyper-bronchial reactivity(OR = 0.82, 95% Cl:0.72, 0.93)
Reduction in self-reportedwheezing in the past 12months (OR = 0.85,95% Cl: 0.76, 0.95)
Adjusted for age, sex,smoking, atopy, andcaloric intake
ooAntioxidants (vitamin C,
vitamin E, carotenoids)Schwartz and Weiss,
1990(42)
Soutaretal., 1997(49)
Cross-sectional,population-based
Cross-sectional,population-based
NHANES II (9,074 adultsaged £30 years,United States)
52 subjects with seasonalsymptoms and 38controls
29 reactors and 58 non-reactors
Selected from 2,000individuals, Scotland
Wheezing Serum vitamin C
Seasonal allergicsymptoms, bronchialreactivity (methacholinechallenge)
Retinol, vitamin C, vitaminE, magnesium, zinc,manganese, andselenium (FFQ)
Bodneretal., 1999(61) Nested case-control study 94 cases and 203 controls Onset of adult asthmaaged 39-45 years
Adjusted for age, sex, race,smoking, total caloricintake, and intake ofother nutrients
Adjusted for sex, age, andsmoking
Vitamin C, vitamin E,retinol, and p-carotene(FFQ)
Plasma levels of ascorbate,oc-tocopherol, retinol,and p-carotene
Serum vitamin C (changeof 12 mg/liter: OR =0.71 (95% Cl: 0.58,0.88)
Increase in symptoms wasassociated with lowerzinc intake (OR = 4.70,95% Cl: 1.33, 16.53(lowest fertile vs.highest fertile))
No impact of antioxidantintake on allergicsymptoms
Increase in bronchialreactivity wasassociated with lowerintake of vitamin C(OR = 7.13, 95% Cl:1.91, 26.71 (lowestfertile vs. highestfertile)) and manganese(OR = 8.14, 95% Cl:2.11, 31.39 (lowestfertile vs. highestfertile))
Higher intake of vitamin E Adjusted for smoking, socio-was related to lowerrisk of adult onset ofasthma (OR = 4.02(95% Cl: 1.30, 12.42)for lowest fertile vs.highest fertile))
Higher plasma levels ofascorbate (OR = 0.98per unit) and ot-tocopherol: triglycerideratio (OR = 0.34 perlog. unit) were relatedto lower risk
economic status, atopy,family history of atopicdisease, and totalenergy intake
O2.01
a.O<ao
ic
inCDID
sTable continues
3in
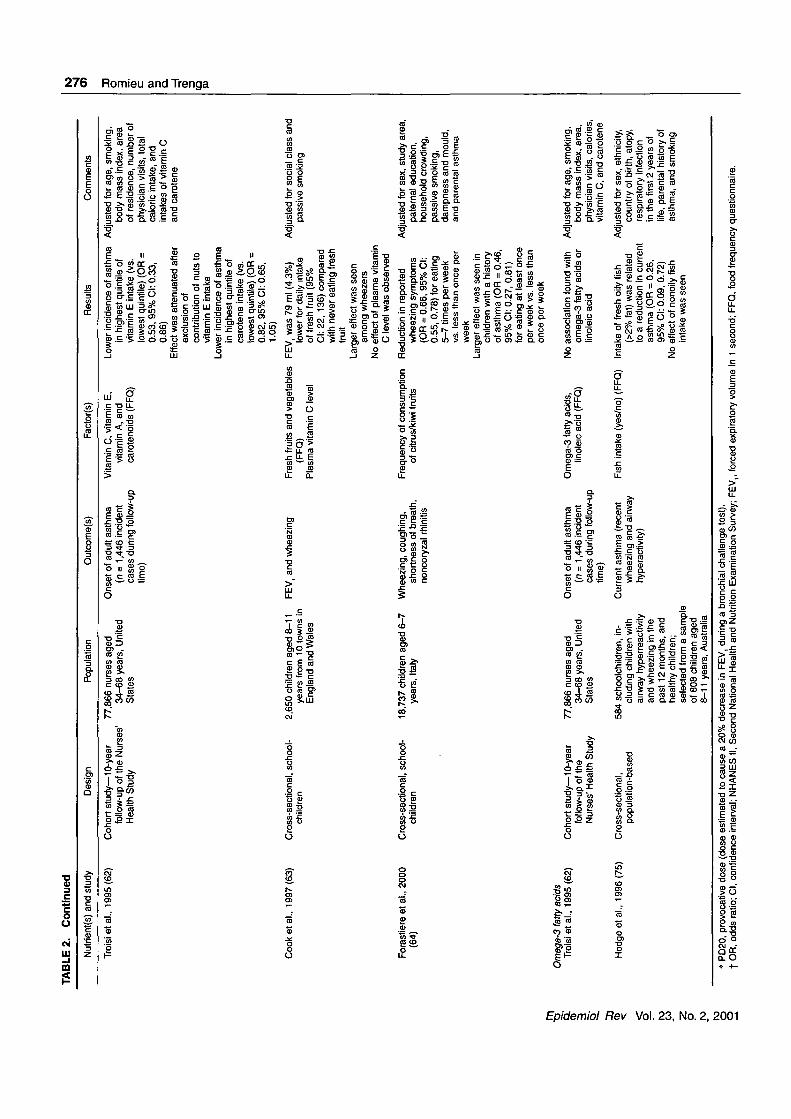
TABLE 2. Continued
1"—§:ofO
wzpro
Nutrient(s) and study
Troisi et al., 1995 (62)
Cooketal., 1997(63)
Forastiere et al., 2000(64)
Omega-3 fatty acidsTroisi etal., 1995(62)
Hodge et al., 1996(75)
Design Population
Cohort study—10-year 77,866 nurses agedfollow-up of the Nurses' 34-68 years, UnitedHealth Study States
Cross-sectional, school- 2,650 children aged 8-11children years from 10 towns in
England and Wales
Cross-sectional, school- 18,737 children aged 6-7children years, Italy
Cohort study—10-year 77,866 nurses agedfollow-up of the 34-68 years, UnitedNurses' Health Study States
Cross-sectional, 584 schoolchildren, in-population-based eluding children with
airway hyperreactivityand wheezing in thepast 12 months, andhealthy children;selected from a sampleof 808 children aged8-11 years, Australia
Outcome(s)
Onset of adult asthma(n = 1,446 incidentcases during follow-uptime)
FEV, and wheezing
Wheezing, coughing,shortness of breath,noncoryzal rhinitis
Onset of adult asthma(n = 1,446 incidentcases during follow-uptime)
Current asthma (recentwheezing and airwayhyperactivity)
Factor(s) Results
Vitamin C, vitamin E, Lower incidence of asthmavitamin A, and in highest quintile ofcarotenoids (FFQ) vitamin E intake (vs.
lowest quintile) (OR =0.53, 95% Cl: 0.33,0.86)
Effect was attenuated afterexclusion ofcontribution of nuts tovitamin E intake
Lower incidence of asthmain highest quintile ofcarotene intake (vs.lowest quintile) (OR =0.82, 95% Cl: 0.65,1.05)
Fresh fruits and vegetables FEV, was 79 ml (4.3%)(FFQ) lower for daily intake
Plasma vitamin C level of fresh fruit (95%Cl: 22, 136) comparedwith never eating freshfrl litTIUII
Larger effect was seenamong wheezers
No effect of plasma vitaminC level was observed
Frequency of consumption Reduction in reportedof citrus/kiwi fruits wheezing symptoms
(OR = 0.66, 95% Cl:0.55, 0.78) for eating5-7 times per weekvs. less than once perweek
Larger effect was seen inchildren with a historyof asthma (OR = 0.46,95% Cl: 0.27, 0.81)for eating at least onceper week vs. less thanonce per week
Omega-3 fatty acids, No association found withlinoleic acid (FFQ) omega-3 fatty acids or
linoleic acid
Fish intake (yes/no) (FFQ) Intake of fresh oily fish(>2% fat) was relatedto a reduction in currentasthma (OR = 0.26,95% Cl: 0.09, 0.72)
No effect of nonoily fishintake was seen
Comments
Adjusted for age, smoking,body mass index, areaof residence, number ofphysician visits, totalcaloric intake, andintakes of vitamin Cand carotene
Adjusted for social class andpassive smoking
Adjusted for sex, study area,paternal education,household crowding,passive smoking,dampness and mould,and parental asthma
Adjusted for age, smoking,body mass index, area,physician visits, calories,vitamin C, and carotene
Adjusted for sex, ethnicity,country of birth, atopy,respiratory infectionin the first 2 years oflife, parental history ofasthma, and smoking
* PD20, provocative dose (dose estimated to cause a 20% decrease in FEV, during a bronchial challenge test).t OR, odds ratio; Cl, confidence interval; NHANES II, Second National Health and Nutrition Examination Survey; FEV,, forced expiratory volume in 1 second; FFQ, food frequency questionnaire.

Diet and Obstructive Lung Diseases 277
children's risk of respiratory infection, which in turn is a riskfactor for the later development of asthma (4, 54).Children's exposure to environmental tobacco smoke hasalso been related to higher immunoglobulin E levels andhigher eosinophil counts and elevated skin-prick sensitivity(56), as well as increased airway hyperreactivity and anincrease in respiratory symptoms (54). Similarly, severalepidemiologic studies have shown that, among differentpopulations of asthmatic children or adults, exposure to pho-tooxidant gases (ozone or nitrogen dioxide) increases thefrequency of respiratory symptoms and bronchial respon-siveness (57). In addition, both experimental and epidemio-logic studies have suggested that antioxidant supplementationcould modulate the acute changes in lung function observedamong people exposed to photooxidants (58-60). It is there-fore reasonable to suggest that antioxidants could play animportant role in asthma.
Six epidemiologic studies, four in adults and two in chil-dren, have investigated the association between antioxidantintake and airway hyperreactivity or asthma-like symptoms(table 2). In these studies, diet was assessed through admin-istration of dietary questionnaires (24-hour recall) (42) orfood frequency questionnaires including different numbersof foods (49, 61-64), or by measuring serum levels ofantioxidant vitamins (42, 63). Analyses of the cross-sectional data of the Second National Health and NutritionExamination Survey (NHANES II) have shown an associ-ation between vitamin C and respiratory health. Lowserum vitamin C levels were associated with increasedwheezing in the previous 12 months (42). After adjustmentfor age, sex, race, smoking, socioeconomic status, and totalcaloric intake, an increase of 12 mg/liter in serum vita-min C was related to a 41 percent decreased risk (oddsratio = 0.71, 95 percent CI: 0.58, 0.88) for wheezing in theprevious 12 months. In a case-control study conductedamong 29 persons who reacted to methacholine and 58persons who did not react to it, Soutar et al. (49) reportedthat the lowest intake of vitamin C and manganese wasassociated with a fivefold increased risk for bronchialreactivity. Studies on adult onset of asthma have producedconflicting results. In a nested case-control study, Bodneret al. (61) reported a protective effect of vitamin E intake(lowest tertile vs. highest: odds ratio = 4.02, 95 percentCI: 1.30, 12.42), as well as higher plasma levels of ascor-bate and a higher oc-tocopherol:triglyceride ratio. Theeffects appeared to be stronger among participants oflower social class, who are likely to have a lower intake ofantioxidants, and among smokers (61). However, in thisstudy, information on dietary intake was obtained after theidentification of cases and controls. In contrast with previ-ous results, a prospective study conducted in a large cohortof nurses aged 34-68 years over a 10-year period (62) didnot find an association between dietary intakes of vitaminC and carotene and onset of adult asthma, but women inthe highest quintile of vitamin E intake (from diet, notfrom supplements) had a relative risk of 0.53 (95 percentCI: 0.33, 0.86) for asthma compared with women in thelowest quintile. The authors concluded that some of theeffect noted was probably due to asthma patients' avoiding
nuts and peanut butter (foods with a high vitamin E con-tent) as possible allergens.
Two recent cross-sectional studies conducted in childrenhave suggested a beneficial impact of fresh fruit consump-tion on respiratory health. In a cross-sectional study of 2,650schoolchildren aged 8-11 years from England and Wales,Cook et al. (63) reported that children who never ate anyfruit had an FEV, 79 ml (4.3 percent) lower than that of chil-dren who ate fruit more than once per day (95 percent CI:22,136). This association was stronger among children withwheezing, although wheezing itself was not associated withfresh fruit consumption. Plasma vitamin C levels were unre-lated to FEV[ or to wheezing, and they correlated poorlywith fresh fruit consumption (63). Forastiere et al. (64) eval-uated dietary intake of citrus and kiwi fruits in a largesample of children aged 6-7 years residing in northern andcentral Italy and recorded the occurrence of wheezing andother respiratory symptoms. After adjustment for potentiallyconfounding factors, intake of citrus/kiwi fruits was protec-tive against wheezing in the previous 12 months (oddsratio = 0.66, 95 percent CI: 0.55, 0.78) among children whoate such fruits 5-7 times per week as compared with lessthan once per week. Similar results were observed whenrespiratory symptoms were recorded 1 year after the assess-ment of citrus/kiwi fruit consumption. No clear doseresponse was observed, and the protective effect was evi-dent even among children who ate such fruits only once ortwice per week. A stronger effect was observed among chil-dren with a history of asthma.
Asthma patients have been reported to have lower-than-normal concentrations of vitamin C in their plasma and bloodleukocytes (3), which suggests that asthma could be associ-ated with a chronically lower concentration of vitamin C.However, providing asthmatic patients with vitamin C sup-plements has yielded conflicting results (15). Supplementstudies have generally been conducted in a small number ofasthma patients with doses of vitamin C ranging from 500mg to 2 g, administered a few hours before bronchoconstric-tor challenge or other assessments of pulmonary function.Results suggest that supplementation with large amounts ofvitamin C may reverse airway hyperreactivity and othersymptoms of asthma (15). In one study, this protective effectwas abolished by indomethacin, which suggests thatleukotriene production is modulated by vitamin C (65).Anderson et al. conducted two supplementation studies (66,67) to evaluate the impact of vitamin C supplementation onpulmonary function and immune response in asthmatic chil-dren over a 6-month period. Vitamin C supplementation wasdemonstrated to improve neutrophil motility and decreaseanti-streptolysin O levels; no clear effect on lung functionwas observed. Studies conducted among asthmatic adultsand healthy controls have suggested that patients withasthma have a lower concentration of selenium in plasma(68) and whole blood (68, 69) and/or reduced glutathioneperoxidase activity (69, 70). Results are inconsistent, andthere is no clear mechanism for low selenium levels in thepathogenesis of asthma.
Cross-sectional and case-control studies suggest a protec-tive effect of vitamin C on airway hyperreactivity and
Epidemiol Rev Vol. 23, No. 2, 2001

278 Romieu and Trenga
wheezing; however, results should be interpreted with cau-tion, and it is premature to conclude that vitamin C is thecritical nutrient. Fresh fruits, a main source of vitamin C, arealso a source of other nutrients such as flavonoids, and vita-min C intake is highly correlated with intakes of carotene,vitamin A, and vitamin E, which may also have a beneficialeffect on pulmonary health (29). In addition, consumptionof fresh fruit is a marker of a healthy lifestyle, which mayhave a positive effect on respiratory health. A lack of adjust-ment for other dietary factors and body mass index mayhave confounded the associations. Additionally, because ofthe nature of these study designs (cross-sectional or case-control), a temporal relation between diet and pulmonaryhealth could not be established. The negative resultobserved in the only prospective study (62) could be due toseveral factors: 1) that study focused on adult onset ofasthma, which may differ substantially from childhood inci-dence because of differences in the immune system, expo-sure patterns, and other factors between children and adults;and 2) intake of vitamin C by nurses in that study wasgreater than average, with few having a low intake, and thismay have masked an effect of vitamin C intake.Supplementation studies suggest a potential impact on acuteairway hyperreactivity response (15). However, none ofthese studies provided evidence that consistent use of vita-min C has a positive effect on objective measures ofpulmonary function or that vitamin C is beneficial in thetreatment of chronic asthma. Vitamin E intake could berelated to the risk of adult-onset asthma. However, furtherstudies are needed to evaluate this association.
co-3 and co-6 fatty acids. The hypothesis that dietary fishintake may reduce people's susceptibility to chronic airwaydiseases originated from the observation that Inuit (Eskimo)populations had a very low prevalence of asthma (71),whereas in most other populations, asthma rates had beenincreasing in parallel with an increase in dietary intake ofpolyunsaturated fat, particularly linoleic acid (co-6 fattyacid) (72). While there are clearly many factors that distin-guish traditional Inuit populations from a society with aWestern lifestyle, the effect of dietary fish intake, particu-larly intake of oily fish with a high co-3 fatty acid content,has attracted much interest. Data from NHANES II sug-gested that a high fish intake was associated with a loweroccurrence of self-reported wheezing; however, this relationdid not persist after adjustment for other factors, includingserum vitamin C levels (42). In a cross-sectional study, noassociations were found between fish consumption andwheezing, chest tightness, or asthma attacks among youngNorwegian adults with a high overall fish intake (73).Similarly, no association was observed between adult onsetof asthma and dietary intake of co-3 fatty acids or dark fishmeat in a large prospective study of US nurses (62).
In contrast, studies carried out among children have founda protective effect of fish intake on asthma incidence. In across-sectional study of Australian children, Peat et al. (74)observed that consumption of one serving of fish per weekwas associated with a reduced risk of asthma. Following thisobservation, in another cross-sectional study of 574Australian children aged 8-11 years, Hodge et al. (75)
reported that children who ate fresh oily fish (>2 percent fat)had a significantly reduced risk for current asthma (oddsratio = 0.29, 95 percent CI: 0.13, 0.67). A test for trend wasnot presented. Similar results were observed after adjust-ment for potentially confounding factors, including atopy,parental history of asthma, parental smoking, ethnicity,country of birth, early respiratory illness, and sex. There wasno difference in consumption of nonoily fish between asth-matic children and nonasthmatic children, which suggeststhat parents of asthmatic children do not selectively preventthem from eating fish.
The central role played by airway inflammation in thepathogenesis of asthma and the recognition that leukotrienesare potent mediators of bronchoconstriction have led toinvestigations of the effect of co-3 fatty acid supplementationamong patients with asthma (71). Studies supplementing thediets of asthmatic patients with co-3 fatty acids or fish oilhave yielded varied results (76-79). Some researchers havesuggested that the ratio of co-3 fatty acid to co-6 fatty acidmay be important. Three recent studies evaluated the impactof increased co-3 fatty acid and reduced w-6 fatty acid in thediets of asthmatics. Broughton et al. (80) reported that asth-matic adults with a high ratio of co-3 fatty acid intake toco-6 fatty acid intake (0.5:1) had a lower rate of metha-choline-induced respiratory distress than those consumingthese fats in a low ratio (0.1:1), as well as lower 4-seriesleukotriene urinary excretion and higher 5-series leukotrieneexcretion. No significant effect on baseline spirometry wasfound. Villani et al. (81) reported that supplementation with3 g/day of to-3 fatty acids during a 30-day period decreasedairway hyperreactivity, but no long-lasting effect wasobserved. Hodge et al. (82) observed no clinical differencein the severity of asthma between asthmatic children receiv-ing co-3 fatty acid dietary supplementation (1.2 g/day) for 6months (a high co-3:co-6 ratio) and those receiving a diet richin w-6 fatty acids. In the group receiving co-3 fatty acids,plasma levels of these fatty acids increased and the produc-tion of stimulated tumor necrosis factor-a, which has beenimplicated in asthma pathogenesis, decreased (82). Thesestudies did not show clinical improvement in asthmapatients using fish oil supplementation, despite somechanges in inflammatory cell functions (3).
Black and Sharpe (72) have suggested that the decrease inthe consumption ratio of co-3:co-6 fatty acids in the devel-oped world could be related to an increase in allergic dis-eases. Fish oil may exert its beneficial effect by reducingconsumers' risk for allergic sensitization rather than bydirectly affecting their asthma (72). This could explain theinconsistency between the results of epidemiologic and sup-plementation studies and fish oil's apparent lack of effect onthe onset of asthma among adults, many of whom are notatopic. It is also important to mention that most of the non-experimental studies (42, 73-75) used fish intake as amarker of co-3 fatty acid consumption and did not accountfor other dietary sources of co-3 fatty acid, such as canolaand flaxseed oils. This, in addition to the fact that fish maybe a source of potentially important nutrients other than co-3fatty acids, should be considered in interpreting the results.
Epidemiol Rev Vol. 23, No. 2, 2001
Diet and Obstructive Lung Diseases 279
Chronic obstructive pulmonary disease
Chronic obstructive airway disease can be defined as aprocess characterized by the presence of chronic bronchitisor emphysema that may lead to the development of airwayobstruction. It is a major cause of death and disabilityamong adults in the United States and throughout the world(83). Cigarette smoking is a major risk factor for chronic air-way disease; however, differences in tobacco consumptiondo not fully account for the variations in population rates ofthis disease. Factors such as dietary intake could play a rolein modulating the impact of environmental exposures on thelung. To assess the association between COPD and diet,most studies have focused on lung functions.
Sodium. Data from NHANES I suggested a positiveassociation between the ratio of dietary sodium to dietarypotassium and the prevalence of self-reported bronchitisamong adults. This association persisted after adjustment forintake of other nutrients, including serum vitamin C (42).
Magnesium. In a study conducted among 2,633 adultsaged 18-70 years, Britton et al. (25) reported that a 100-mg/day higher magnesium intake was associated with ahigher FEV, (27.7 ml; 95 percent CI: 11.9,43.5). This resultcorresponded to an increase of approximately 124 ml over a95 percent range of magnesium intake (156.5-603 ml) or a3.9 percent increase in the population mean FEV,.Adjustment for potentially confounding factors, includingage, sex, height, atopy, calcium, vitamin C, and total caloricintake, did not modify this result substantially. This resultwas not confirmed by Butland et al. (84).
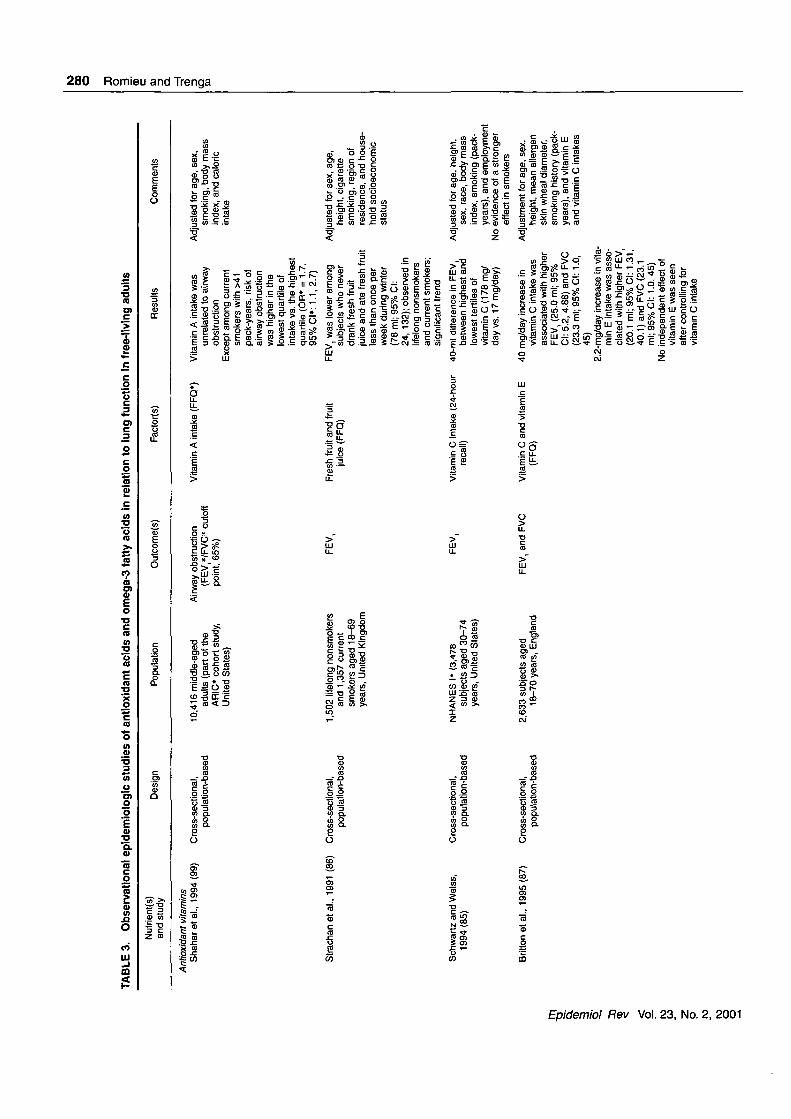
Antioxidants. Lung function among adults has beenrelated to intake of antioxidants, particularly vitamin C.Numerous studies have estimated consumption of fresh fruitor juice (85) and consumption of antioxidants using dietaryquestionnaires (42, 49, 85-94), dietary interviews (95), orblood levels of antioxidants (88, 93, 96, 97) (table 3).
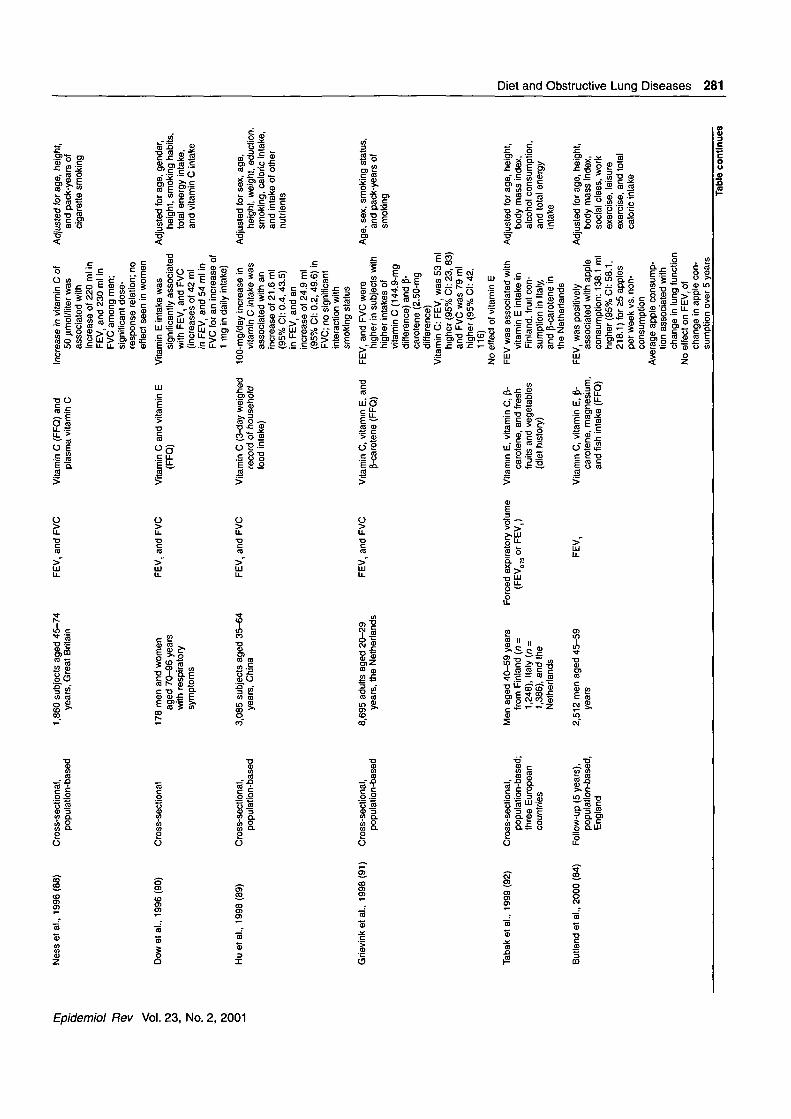
Ten cross-sectional studies conducted in adults reportedthat vitamin C intake had a protective effect against declinein lung function (85-93, 96). In a study of 1,502 lifelongsmokers and 1,357 current smokers aged 18-69 years, FEV,was 78 ml lower among subjects who drank no fruit juice orwho ate fresh fruit less than once per week during the win-ter (86). However, total vitamin C intake was not assessed inthat study. Britton et al. (87) observed in 2,633 adults thatboth FEV, and forced vital capacity were significantlyrelated to subjects' mean daily intakes of vitamin C and vi-tamin E. An increased vitamin C intake of 40 mg/day wasrelated to a 25-ml higher FEV1 and a 23.3-ml higher forcedvital capacity. For vitamin E, an increase in intake of 2.2mg/day was associated with a 20.1-ml higher FEV, and a23.1-ml higher forced vital capacity. These results persistedafter adjustment for age, sex, height, mean allergen skinwheal diameter, and pack-years of smoking. However, afteradjustment for vitamin C intake, the authors found no inde-pendent effect of vitamin E. The effect of vitamin C intakeon lung functions was slightly higher among current smok-ers and ex-smokers (87). In a cross-sectional population-based study that included 1,860 adults aged 45-75 years,higher plasma vitamin C levels were associated with higher
pulmonary function: A 50-u.mol/liter increase in plasma vi-tamin C was associated with an increase of 0.22 liter inFEV, (89). In NHANES I, FEV, was related to dietary vita-min C intake as estimated by 24-hour dietary recall; subjectsin the lowest tertile of vitamin C intake (17 mg/day) had anaverage FEV, 40 ml lower than that of subjects in the high-est tertile (170 mg/day). This difference corresponds to theeffect of 10 pack-years of smoking or 1 year of aging (85).
More recently, in a study carried out among 3,085 sub-jects from 69 counties in China, researchers reported a pos-itive association between vitamin C intake and lung func-tion. An increase in vitamin C intake of 100 mg/day wasassociated with increases of 21.6 ml (95 percent CI: -0.4,43.5) in FEV, and 24.9 ml (95 percent CI: 0.2, 49.6) inforced vital capacity (89). In a study of 178 elderly personsaged 76-90 years in England, FEV, and forced vital capac-ity were significantly related to vitamin E intake but not tovitamin C intake. After adjustment for age, sex, height,smoking habits, total energy intake, and vitamin C intake,researchers found that an increase of 1 mg/day in vitamin Eintake was related to increases of 42 ml in FEV, and 54 mlin forced vital capacity (90). Data from the MORGENStudy, conducted in Dutch adults, have shown higher FEV,and forced vital capacity among subjects with higher intakesof vitamin C and p-carotene (91). When investigators com-pared subjects in the 10th and 90th percentiles of vitamin Cconsumption (a 144.4-mg/day difference), FEV, was 53 mlhigher (95 percent CI: 23, 83) and forced vital capacity was79 ml higher (95 percent CI: 42, 116) in the higher con-sumption group. With regard to P-carotene consumption, thesame comparison (a 2.50-mg/day difference) showedincreases of 60 ml (95 percent CI: 31, 89) for FEV, and 75ml (95 percent CI: 40, 110) for forced vital capacity. Noeffect of vitamin E consumption was observed. Tabak et al.(92) studied the impact of fruit and vegetable consumptionon FEV, among adults in three European countries. FEV,was higher in men with a combined fruit and vegetableintake above the median as compared with those whoseintake of both types of food was below the median, but thefinding did not reach statistical significance after adjustmentfor total caloric intake (92). The association of the individ-ual dietary factors with pulmonary function was not consis-tent across countries. Two recent studies confirmed the pos-itive association between FEV, and antioxidant nutrients,particularly vitamin E, vitamin C, and some carotenoids (93,96).
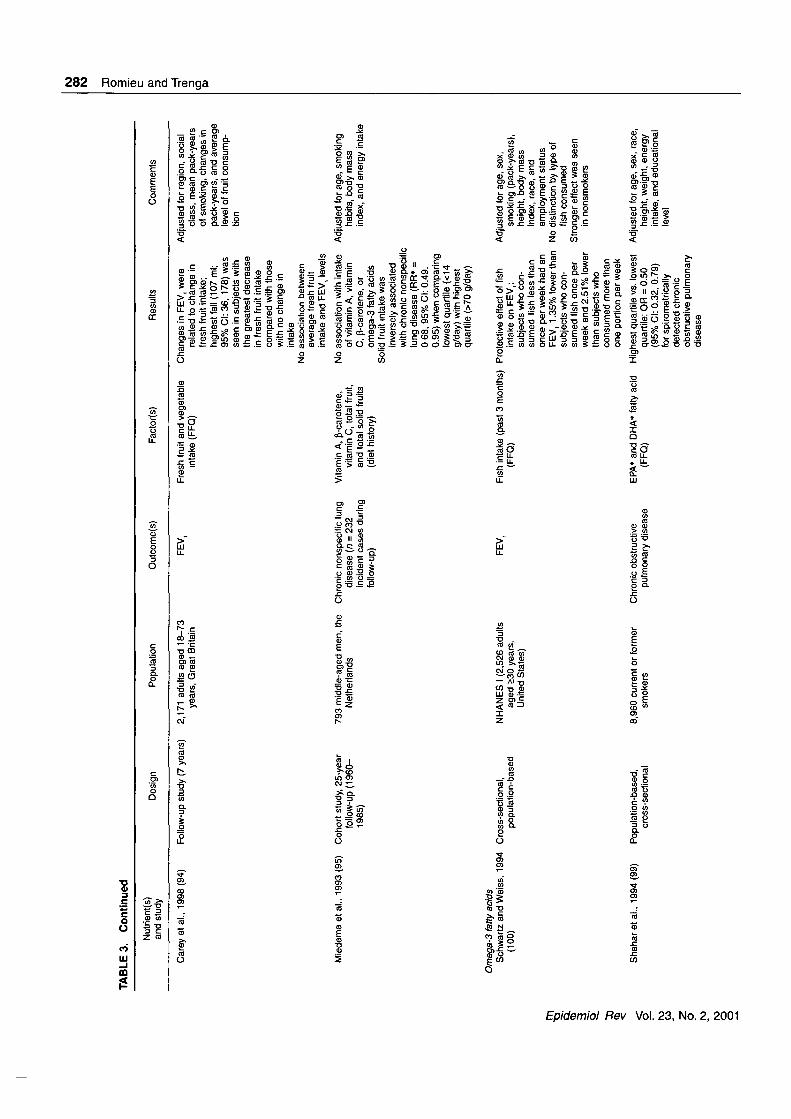
Three longitudinal studies have evaluated the impact ofantioxidant intake on chronic lung diseases (95-97). In a 25-year prospective study carried out among 793 middle-agedmen in Zutphen, the Netherlands, Miedema et al. (95) com-pared subjects who consumed more than 70 g of solid fruitper day with those who consumed 14 g or less. After adjust-ing for age, body mass index, smoking, and total energyintake and other dietary factors, they observed that con-sumption of solid fruits was inversely related to the inci-dence of chronic nonspecific lung disease (a classificationthat grouped self-reported chronic respiratory symptomswith a diagnosis of emphysema, chronic bronchitis, orasthma). The incidence of chronic nonspecific lung disease
Epidemiol Rev Vol. 23, No. 2, 2001
IS)»o
TABLE 3. Observational epidemiologic studies of antioxidant acids and omega-3 fatty acids in relation to lung function in free-living adults
Nutrient(s)and study D e s i g n Population Outcome(s) Factor(s) Results Comments
33o
<b"a>Q.
CD
(Q01
Antioxidant vitaminsShahar et al., 1994(99) Cross-sectional,
population-based10,416 middle-aged
adults (part of theARIC* cohort study,United States)
Airway obstruction(FEV//FVC* cutoffpoint, 65%)
Vitamin A intake (FFQ*)
Strachan et al., 1991 (86) Cross-sectional,population-based
1,502 lifelong nonsmokersand 1,357 currentsmokers aged 18-69years, United Kingdom
FEV, Fresh fruit and fruitjuice (FFQ)
Schwartz and Weiss,1994 (85)
Cross-sectional,population-based
Britton et al., 1995 (87) Cross-sectional,population-based
NHANES I* (3,478subjects aged 30-74years, United States)
2,633 subjects aged18-70 years, England
FEV,
FEV, and FVC
Vitamin C intake (24-hourrecall)
Vitamin C and vitamin E(FFQ)
3
CO
OJOIOOO
Vitamin A intake wasunrelated to airwayobstruction
Except among currentsmokers with >41pack-years, risk ofairway obstructionwas higher in thelowest quartile ofintake vs. the highestquartile (OR* = 1.7,95% Cl*: 1.1, 2.7)
FEV, was lower amongsubjects who neverdrank fresh fruitjuice and ate fresh fruitless than once perweek during winter(78 ml; 95% Cl:24, 132); observed inlifelong nonsmokersand current smokers;significant trend
40-ml difference in FEV,between highest andlowest tertiles ofvitamin C (178 mg/day vs. 17 mg/day)
40 mg/day increase invitamin C intake wasassociated with higherFEV, (25.0 ml; 95%Cl: 5.2, 4.88) and FVC(23.3 ml; 95% Cl: 1.0,45)
2.2-mg/day increase in vita-min E intake was asso-ciated with higher FEV,(20.1 ml; 95% Cl: 1.31,40.1) and FVC (23.1ml;95%CI: 1.0,45)
No independent effect ofvitamin E was seenafter controlling forvitamin C intake
Adjusted for age, sex,smoking, body massindex, and caloricintake
Adjusted for sex, age,height, cigarettesmoking, region ofresidence, and house-hold socioeconomicstatus
Adjusted for age, height,sex, race, body massindex, smoking (pack-years), and employment
No evidence of a strongereffect in smokers
Adjustment for age, sex,height, mean allergenskin wheal diameter,smoking history (pack-years), and vitamin Eand vitamin C intakes
!6'
ro_co
zpro
8o
Ness el al., 1996(88) Cross-sectional,population-based
Dowetal., 1996(90) Cross-sectional
Huelal. , 1998(89) Cross-sectional,population-based
Grievink el al., 1998(91) Cross-sectional,population-based
Tabaketal., 1999(92)
Butland et al., 2000 (84)
Cross-sectional,population-based;three Europeancountries
Follow-up (5 years),population-based,England
1,860 subjects aged 45-74years, Great Britain
FEV, and FVC Vitamin C (FFQ) andplasma vitamin C
178 men and womenaged 70-96 yearswith respiratorysymptoms
3,085 subjects aged 35-64years, China
FEV, and FVC
FEV, and FVC
Vitamin C and vitamin E(FFQ)
Vitamin C (3-day weighedrecord of householdfood intake)
8,695 adults aged 20-29years, the Netherlands
FEV, and FVC Vitamin C, vitamin E, andP-carotene (FFQ)
Men aged 40-59 yearsfrom Finland (n =1,248), Italy (n =1,386), and theNetherlands
2,512 men aged 45-59years
Forced expiratory volume(FEV075orFEV,)
FEV,
Vitamin E, vitamin C, p-carotene, and freshfruits and vegetables(diet history)
Vitamin C, vitamin E, p-carotene, magnesium,and fish intake (FFQ)
Increase in vitamin C of50 ixmol/liter wasassociated withincrease of 220 ml inFEV, and 230 ml inFVC among men;significant dose-response relation; noeffect seen in women
Vitamin E intake wassignificantly associatedwith FEV, and FVC(increases of 42 mlin FEV, and 54 ml inFVC for an increase of1 mg in daily intake)
100-mg/day increase invitamin C intake wasassociated with anincrease of 21.6 ml(95% Cl: 0.4, 43.5)in FEV, and anincrease of 24.9 ml(95% Cl: 0.2, 49.6) inFVC; no significantinteraction withsmoking status
FEV, and FVC werehigher in subjects withhigher intakes ofvitamin C (144.9-mgdifference) and p-carotene (2.50-mgdifference)
Vitamin C: FEV, was 53 mlhigher (95% Cl: 23, 83)and FVC was 79 mlhigher (95% Cl: 42,116)
No effect of vitamin E
FEV was associated withvitamin E intake inFinland, fruit con-sumption in Italy,and p-carotene inthe Netherlands
FEV, was positivelyassociated with appleconsumption: 138.1 mlhigher (95% Cl: 58.1,218.1) for £5 applesper week vs. non-consumption
Average apple consump-tion associated withchange in lung function
No effect on FEV, ofchange in apple con-sumption over 5 years
Adjusted for age, height,and pack-years ofcigarette smoking
Adjusted for age, gender,height, smoking habits,total energy intake,and vitamin C intake
Adjusted for sex, age,height, weight, eduction,smoking, caloric intake,and intake of othernutrients
Age, sex, smoking status,and pack-years ofsmoking
Adjusted for age, height,body mass index,alcohol consumption,and total energyintake
Adjusted for age, height,body mass index,social class, workexercise, leisureexercise, and totalcaloric intake
£
Q.
oorS2.
ac3
CO
ooTable continues
to00ro
TABLE 3. Continuedo
5'c01Q.
01
Nutrient(s)and study
Design Population Outcome(s) Factor(s) Results Comments
Carey et al., 1998 (94) Follow-up study (7 years) 2,171 adults aged 18-73years, Great Britain
FEV. Fresh fruit and vegetableintake (FFQ)
Miedema et al., 1993(95) Cohort study, 25-yearfollow-up (1960-1985)
793 middle-aged men, theNetherlands
Chronic nonspecific lungdisease (n = 232incident cases duringfollow-up)
Vitamin A, p-carotene,vitamin C, total fruit,and total solid fruits(diet history)
Adjusted for region, socialclass, mean pack-yearsof smoking, changes inpack-years, and averagelevel of fruit consump-tion
Changes in FEV, wererelated to change infresh fruit intake;highest fall (107 ml;95%CI:36, 178) wasseen in subjects withthe greatest decreasein fresh fruit intakecompared with thosewith no change inintake
No association betweenaverage fresh fruitintake and FEV, levels
No association with intake Adjusted for age, smokingof vitamin A, vitaminC, P-carotene, oromega-3 fatty acids
Solid fruit intake wasinversely associatedwith chronic nonspecificlung disease (RR* =0 68, 95% Cl: 0.49,0.95) when comparinglowest quartile (<14g/day) with highestquartile (>70 g/day)
habits, body massindex, and energy intake
S1
!
IroCO
prorooo
Omega-3 fatty acidsSchwartz and Weiss, 1994
(100)Cross-sectional,
population-basedNHANES I (2,526 adults
aged >30 years,United States)
FEV, Fish intake (past 3 months) Protective effect of fish(FFQ) intake on FEV,;
subjects who con-sumed fish less thanonce per week had anFEV, 1.35% lower thansubjects who con-sumed fish once perweek and 2.51% lowerthan subjects whoconsumed more thanone portion per week
Shaharetal., 1994(99) Population-based,cross-sectional
8,960 current or formersmokers
Chronic obstructivepulmonary disease
EPA* and DHA* fatty acid(FFQ)
Highest quartile vs. lowestquartile: OR = 0.50(95% Cl: 0.32, 0.79)for spirometricallydetected chronicobstructive pulmonarydisease
Adjusted for age, sex,smoking (pack-years),height, body massindex, race, andemployment status
No distinction by type offish consumed
Stronger effect was seenin nonsmokers
Adjusted for age, sex, race,height, weight, energyintake, and educationallevel
Diet and Obstructive Lung Diseases 283
111
Iff I
o > o £ o<D S - « "S S
ff§§3sfO <D Q 2
I" I\%%
J i ScMO ~ CO V
• CM -C <p 1 ^ (j) > i
C D § — - SO = 5 o o
11*1Q "O CO ~
<
I
HiII
oen<
855so
CO
• 3
Q.
CO. cc/3
2L
U. o
TJ <CD X
*.§
2 fjo
PE l
1̂
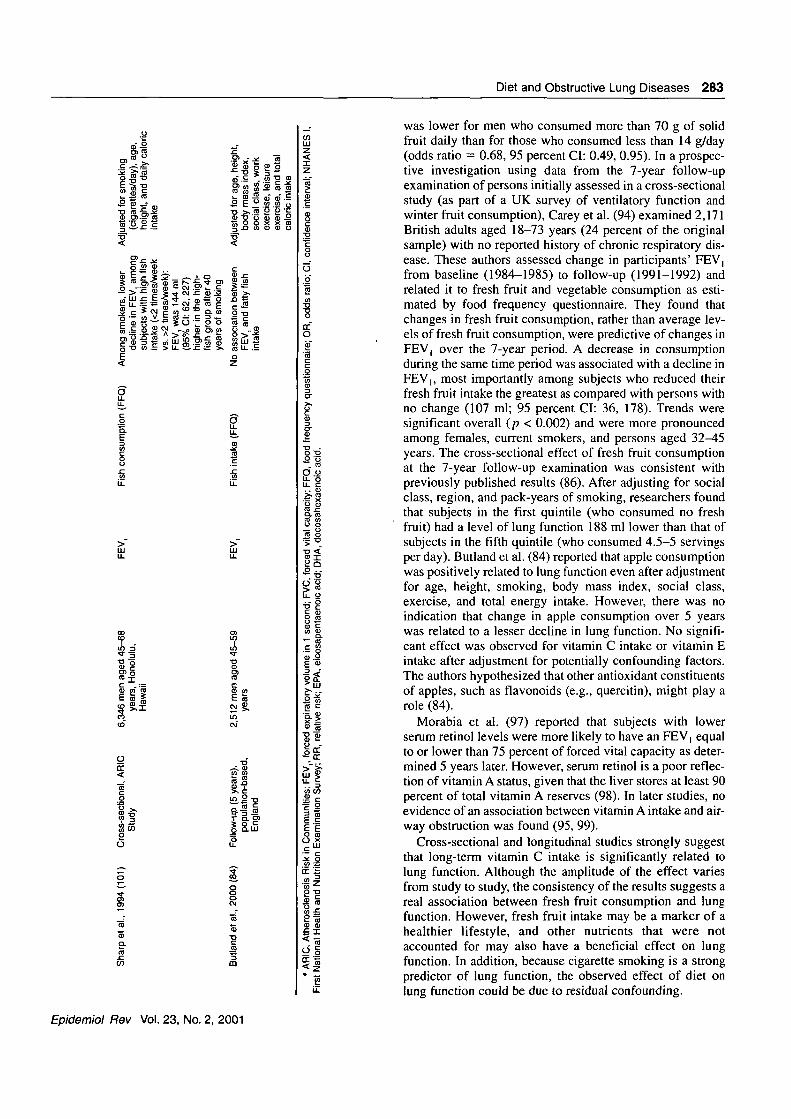
was lower for men who consumed more than 70 g of solidfruit daily than for those who consumed less than 14 g/day(odds ratio = 0.68, 95 percent CI: 0.49, 0.95). In a prospec-tive investigation using data from the 7-year follow-upexamination of persons initially assessed in a cross-sectionalstudy (as part of a UK survey of ventilatory function andwinter fruit consumption), Carey et al. (94) examined 2,171British adults aged 18-73 years (24 percent of the originalsample) with no reported history of chronic respiratory dis-ease. These authors assessed change in participants' FEV,from baseline (1984-1985) to follow-up (1991-1992) andrelated it to fresh fruit and vegetable consumption as esti-mated by food frequency questionnaire. They found thatchanges in fresh fruit consumption, rather than average lev-els of fresh fruit consumption, were predictive of changes inFEV, over the 7-year period. A decrease in consumptionduring the same time period was associated with a decline inFEV], most importantly among subjects who reduced theirfresh fruit intake the greatest as compared with persons withno change (107 ml; 95 percent CI: 36, 178). Trends weresignificant overall (p < 0.002) and were more pronouncedamong females, current smokers, and persons aged 32^15years. The cross-sectional effect of fresh fruit consumptionat the 7-year follow-up examination was consistent withpreviously published results (86). After adjusting for socialclass, region, and pack-years of smoking, researchers foundthat subjects in the first quintile (who consumed no freshfruit) had a level of lung function 188 ml lower than that ofsubjects in the fifth quintile (who consumed 4.5-5 servingsper day). Butland et al. (84) reported that apple consumptionwas positively related to lung function even after adjustmentfor age, height, smoking, body mass index, social class,exercise, and total energy intake. However, there was noindication that change in apple consumption over 5 yearswas related to a lesser decline in lung function. No signifi-cant effect was observed for vitamin C intake or vitamin Eintake after adjustment for potentially confounding factors.The authors hypothesized that other antioxidant constituentsof apples, such as flavonoids (e.g., quercitin), might play arole (84).
Morabia et al. (97) reported that subjects with lowerserum retinol levels were more likely to have an FEV, equalto or lower than 75 percent of forced vital capacity as deter-mined 5 years later. However, serum retinol is a poor reflec-tion of vitamin A status, given that the liver stores at least 90percent of total vitamin A reserves (98). In later studies, noevidence of an association between vitamin A intake and air-way obstruction was found (95, 99).
Cross-sectional and longitudinal studies strongly suggestthat long-term vitamin C intake is significantly related tolung function. Although the amplitude of the effect variesfrom study to study, the consistency of the results suggests areal association between fresh fruit consumption and lungfunction. However, fresh fruit intake may be a marker of ahealthier lifestyle, and other nutrients that were notaccounted for may also have a beneficial effect on lungfunction. In addition, because cigarette smoking is a strongpredictor of lung function, the observed effect of diet onlung function could be due to residual confounding.
Epidemiol Rev Vol. 23, No. 2, 2001
284 Romieu and Trenga
a>-3 and co-6 fatty acids. Three studies conducted in theUnited States have suggested that increased consumption offish, as estimated by dietary questionnaire, could decreasethe development of airway narrowing (99-101) (table 3).Schwartz and Weiss (100) reported a protective effect offish intake on FEV, in a subsample {n = 2,526) ofNHANES I participants aged >30 years. After controllingfor height, age, cigarette smoking, and sex, they found thatsubjects who consumed fish less than once per week had anFEV, 1.35 percent lower than that of subjects who con-sumed fish once per week and an FEV, 2.51 percent lowerthan that of subjects who consumed fish more than once perweek. The test for trend across categories was significant,and the effect was stronger among nonsmokers. However,the authors did not distinguish between different types offish or adjust for intake of other nutrients. In a cross-sectional analysis of data from the Atherosclerosis Risk inCommunities (ARIC) Study, which was conducted among9,000 male smokers aged 45-64 years, results suggestedthat dietary fish intake had a protective effect on COPDrisk. After adjustment for smoking, age, race, sex, educa-tion, height, and weight, the relative risk of COPD was0.3-0.6 for persons in the highest quartile of fish oil intakeas compared with those in the lowest quartile (99).However, results pertaining to lung functions were incon-sistent. In an assessment of data from the Honolulu HeartProgram, Sharp et al. (101) analyzed the relation betweenFEV, and self-reported frequency offish consumption, cat-egorized as less than twice per week and two or more timesper week. Among 6,346 male smokers aged 45-68 years,after adjustment for cigarettes per day, age, height, anddaily caloric intake, these authors found FEV, to be higheramong subjects with a high dietary fish intake than amongthose with a low fish intake. From the difference observed,Sharp et al. predicted an FEV, 144 ml higher (95 percentCI: 62, 227) in the high-fish group at >40 years of smoking(101). The effect was larger among smokers of 30 or fewercigarettes per day, which suggests a saturation effect. Incontrast, fish intake showed no clear association with pul-monary function in other studies (84, 92). However, inthose studies, no stratified analysis by smoking status wasconducted.
To our knowledge, only one study has addressed the w-3hypothesis in a prospective data set (95). Results suggestedthat intake of linoleic acid (co-6 fatty acid) was positivelyrelated to the incidence of chronic nonspecific lung disease(defined as chronic productive cough, diagnosed chronicbronchitis, emphysema, and asthma); however, over the 25-year study period, no association between n-3 fatty acid intakeand the incidence of chronic nonspecific lung disease wasfound.
Cross-sectional data suggest that w-3 fatty acids mayhave a protective effect against COPD and decreases in lungfunction; however, study results are inconsistent in identify-ing the subgroups in which fish oil appears to have the great-est effect (71). None of these studies controlled for intake ofother nutrients, such as antioxidant vitamins, which may becorrelated with w-3 fatty acid intake. Researchers who con-ducted the only known prospective study observed no pro-
tective effect for &>-3 fatty acids after adjusting for othernutrients (95); however, they did find that intake of solidfruit had a strong protective effect against chronic nonspe-cific lung disease.
SUMMARY
The results presented in this review suggest that theimpact of nutrition on obstructive lung disease is most evi-dent for antioxidant vitamins, particularly vitamin C and,to a lesser extent, vitamin E. By decreasing oxidant insultsto the lung, antioxidants could modulate the developmentof chronic lung diseases and lung function decrement.Antioxidant vitamins could also play an important role ingene-environment interactions in complex lung diseasessuch as childhood asthma. Data also suggest that co-3 fattyacids may have a potentially protective effect against air-way hyperreactivity and lung function decrements; how-ever, relevant data are still sparse. Although epidemiologicdata suggest that consumption of fresh fruit may reducerisk of noncarcinogenic airway limitation, there are noclear data on which nutrients might be most relevant.While some studies evaluate daily intake of vitamin C,other studies use fruit consumption as a surrogate forantioxidant intake. Given the dietary intercorrelationsamong antioxidant vitamins, particularly vitamin C, P-carotene, and flavonoids, as well as other micronutrients, itmay be difficult to isolate a specific effect. Some popula-tion subgroups with higher levels of oxidative stress, suchas cigarette smokers, may be more likely to benefit fromdietary supplementation, since some studies have sug-gested that antioxidant intake may have a greater impact inthis group.
Studies of lung function decrement and COPD in adultssuggest that daily intake of vitamin C at levels slightlyexceeding the current Recommended Dietary Allowance (60mg/day among nonsmokers and 100 mg/day among smok-ers) may have a protective effect (20). In the Schwartz andWeiss (85) and Britton et al. (87) studies, an increase of 40mg/day in vitamin C intake led to an approximate 20-mlincrease in FEV,. Daily mean vitamin C intakes in thesestudies were 66 mg and 99.2 mg, respectively, and the high-est intake level (178 mg/day) was approximately three timesthe Recommended Dietary Allowance. Although the ampli-tude of the effect was modest, if these effects accumulateover 20-30 years, they could have a meaningful impact onthe rate at which pulmonary function declines, particularlyin symptomatic subjects (85). Longitudinal data support thehypothesis that fresh fruit consumption has a beneficialimpact on the lung (95). Among children, consumption offresh fruit, particularly fruit high in vitamin C, has beenrelated to a lower prevalence of asthma symptoms andhigher lung function (64). This effect was observed even atlow levels of fruit consumption (one or two servings perweek vs. less than one serving per week), which suggeststhat a small increase in dietary intake could have a benefi-cial effect. Consumption of fish has also been related tolower airway hyperreactivity among children (75) andhigher lung function in adults (100); however, longitudinal
Epidemiol Rev Vol. 23, No. 2, 2001

Diet and Obstructive Lung Diseases 285
data do not provide evidence that increased co-3 fatty acidintake protects against lung disease (101).
Experimental studies of persons with asthma suggest thatmagnesium infusion may have a place in the acute treatmentof asthma, but it does not seem to have long-term benefits.The studies of sodium, selenium, and fish oils do not showconvincing evidence of clinical benefits. Studies of vitaminC supplementation suggest a short-term protective effect onairway responsiveness and pulmonary function. It remains tobe proven whether consistent use of vitamin C would have aprotective effect on the evolution of chronic asthma. Resultsfrom supplementation studies conducted among subjectsexposed to high levels of oxidants (57-60) suggest that dailyintake of antioxidant vitamins exceeding the RecommendedDietary Allowance may have a beneficial effect on lung air-ways and that intake higher than the Recommended DietaryAllowance should be recommended for populations chroni-cally exposed to photooxidant air pollutants (such as ozone),cigarette smoking, or vigorous exercise. It is difficult todetermine the amounts of antioxidant vitamins that peopleshould consume. In particular, although vitamin C wasshown to have maximum bioavailability when given in a sin-gle dose of 200 mg (102), experiments on which this findingwas based were conducted under normal conditions.Guidelines from the US National Cancer Institute (103) rec-ommend consumption of five servings of fruit and vegeta-bles daily, corresponding to a vitamin C intake exceeding200 mg. Dietary surveys carried out in the US populationindicate that less than 12 percent of US children and adultsmeet this recommended level of intake (104).
Diet appears to be an important cofactor in the develop-ment of obstructive lung disease, although data are stillsparse. There is a need for further research in experimen-tal and epidemiologic settings to better understand thephysiologic effects of antioxidant vitamins, w-3 fattyacids, and other nutrients on lung tissues. The impact ofdiet on the incidence and evolution of asthma and COPDshould be investigated using a cohort design that accountsfor known risk factors. This will allow researchers to eval-uate the exposure-disease relation over an adequate timeframe and obtain insight into the causality of the relation.Some of these studies should enroll infants and youngchildren to determine the impact of early diet on respira-tory health. Research should also focus on the equallychallenging policy issues—namely, finding effectivemethods of convincing people to increase their daily con-sumption of fresh fruits and vegetables, to stop smokingcigarettes, and to minimize their environmental and occu-pational exposure to pollutants and other agents that causerespiratory disease.
ACKNOWLEDGMENTS
This work was supported by the Pan American HealthOrganization and the US Centers for Disease Control andPrevention.
REFERENCES
1. Hu H, Kotha S, Brennan T. The role of nutrition in mitigat-ing environmental insults: policy and ethical issues. EnvironHealth Perspect 1995;103(suppl 106):185-90.
2. Willett WC. Diet, nutrition and avoidable cancer. EnvironHealth Perspect 1995; 103:165-70.
3. Monteleone CA, Sherman AR. Nutrition and asthma. ArchIntern Med 1997;157:23-34.
4. Peat JK. Prevention of asthma. Eur Respir J 1996;9:1545-55.5. Hill AB. The environment and disease: association or causa-
tion? Proc R Soc Med 1965;58:295-300.6. Rahman I, MacNee W. Role of oxidants/antioxidants in
smoking-induced lung diseases. Free Radic Biol Med 1996;21:669-81.
7. Heffner JE, Repine JE. Pulmonary strategies of antioxidantdefense. Am Rev Respir Dis 1989;140:531-54.
8. Sies H. Oxidative stress: introduction. In: Sies H, ed.Oxidative stress: oxidants and antioxidants. San Diego, CA:Academic Press, Inc, 1991:xv-xxii.
9. McGowan SE, Hunninghake GW. Neutrophils and emphy-sema. N Engl J Med 1989;321:968-70.
10. Sibille Y, Reynolds HY. Macrophages and polymorphonu-clear neutrophils in lung defense and injury. Am Rev RespirDis 1990;141:471-501.
11. Repine JE, Bast A, Lankhorst I. Oxidative stress in chronicobstructive pulmonary disease. The Oxidative Stress StudyGroup. Am J Respir Crit Care Med 1997; 156:341-57.
12. Bast A, Haenen GR, Doelman CJ. Oxidants and antioxidants:state of the art. Am J Med (suppl) 1991 ;91:2-13S.
13. Cantin A, Crystal RG. Oxidants, antioxidants and the patho-genesis of emphysema. Eur J Respir Dis 1985;66:7-17.
14. Burton GW, Ingold KU. Autooxidation of biological mol-ecules. 1. The antioxidant activity of vitamin E and relatedchain-breaking phenolic antioxidants in vitro. J Am ChemSoc 1981;103:6472-7.
15. Hatch GE. Asthma, inhaled oxidants and dietary antioxi-dants. Am J Clin Nutr 1995;61(suppl):625-30S.
16. McCay PB. Vitamin E: interaction with free radicals andascorbate. Annu Rev Nutr 1985;5:323-40.
17. Linder MC. Nutrition and metabolism of trace elements. In:Linder MC, ed. Nutrition biochemistry and metabolism withclinical application. Norwalk, CT: Appleton and Lange,1991:213-76.
18. Barnes PJ. Reactive oxygen species and airway inflamma-tion. Free Radic Biol Med 1990;9:235^*3.
19. Romieu I, Stampfer MJ, Stryker WS, et al. Food predictorsof plasma beta-carotene and alpha-tocopherol: validation ofa food frequency questionnaire. Am J Epidemiol 1990;131:864-76.
20. National Research Council. Recommended dietaryallowances. 10th ed. Washington, DC: National AcademyPress, 1989.
21. James MJ, Gibson RA, Cleland LG. Dietary polyunsaturatedfatty acids and inflammatory mediator production. Am J ClinNutr 2000;71(suppl):343S-8S.
22. Rossi AG, Haslett C. Inflammation, cell injury, and apopto-sis. In: Said SE, ed. Proinflammatory and antiinflammatorypeptides. (Lung biology in health and disease, vol 112). NewYork, NY: Marcel Dekker, Inc, 1998; 112:9-24.
23. Britton J, Pavord I, Richards R, et al. Dietary sodium intakeand the risk of airway hyperreactivity in a random adult pop-ulation. Thorax 1994;49:875-80.
24. Knox AJ. Salt and asthma. (Editorial). BMJ 1993,307:1159-60.
25. Britton J, Pavord I, Richards K, et al. Dietary magnesium,lung function, wheezing, and airway hyper-reactivity in arandom adult population sample. Lancet 1994;344:357-62.
26. Hunter D. Biochemical indicators of dietary intake. In:Willett W, ed. Nutritional epidemiology. 2nd ed. New York,NY: Oxford University Press, 1998:174-243.
Epidemiol Rev Vol. 23, No. 2, 2001
286 Romieu and Trenga
27. Buzzard M. 24-hour dietary recall and food record methods.In: Willett W, ed. Nutritional epidemiology. 2nd ed. NewYork, NY: Oxford University Press, 1998:50-73.
28. Willett W, Lenart E. Reproducibility and validity of food-frequency questionnaire. In: Willett W, ed. Nutritional epi-demiology. 2nd ed. New York, NY: Oxford University Press,1998:101-47.
29. Ziegler RC, Mayne ST, Swanson CA. Nutrition and lungcancer. Cancer Causes Control 1996;7:157-77.
30. Nadel J. General principles and diagnostic approach. In:Murray JF, Nadel JA, eds. Respiratory medicine. 2nd ed.Philadelphia, PA: WB Saunders Company, 1994:1245-58.
31. Snider GL, Faling LJ, Rennard SI. Chronic bronchitis andemphysema. In: Murray JF, Nadel JA, eds. Respiratory med-icine. 2nd ed. Philadelphia, PA: WB Saunders Company,1994:1331-97.
32. National Heart, Lung, and Blood Institute, National Institutesof Health. Global initiative on asthma. Bethesda, MD:National Heart, Lung, and Blood Institute, 1995:95-3659.(NHLBI publication no. 95-3659).
33. Mannino DM, Homa DM, Pertowski CA, et al. Surveillancefor asthma—United States, 1960-1995. Mor Mortal WklyRep CDC Surveill Summ 1998;47(no. SS-l):l-27.
34. Patterson BH, Block G, Rosenberg WF, et al. Fruit and veg-etables in the American diet: data from the NHANES II sur-vey. Am J Public Health 1990;80:1443-9.
35. Seaton A, Godden DJ, Brown K. Increase in asthma: a moretoxic environment or a more susceptible population? Thorax1994;49:171-4.
36. US Public Health Service, Department of Health and HumanServices. Healthy People 2000: national health promotionand disease prevention objectives. Washington, DC: USPublic Health Service, 1991:32. (DHHS publication no.(PHS) 91-50212.)
37. Burney PG. The causes of asthma: does salt potentiatebronchial activity? J R Soc Med 1987;80:364-7.
38. Burney PG, Britton JR, Chinn S, et al. Response to inhaledhistamine and 24 hour sodium excretion. Br Med J (Clin ResEd) 1986;292:1483-6.
39. Pistelli R, Forastiere F, Corbo GM, et al. Respiratory symp-toms and bronchial responsiveness are related to dietary saltintake and urinary potassium excretion in male children. EurRespirJ 1993;6:517-22.
40. Tribe RM, Barton JR, Poston L, et al. Dietary sodium intake,airway responsiveness, and cellular sodium transport. Am JRespir Crit Care Med 1994; 149:1426-33.
41. Devereux G, Beach JR, Bromly C, et al. Effect of dietarysodium on airways responsiveness and its importance in theepidemiology of asthma: an evaluation in three areas ofnorthern England. Thorax 1995;50:941-7.
42. Schwartz J, Weiss ST. Dietary factors and their relation torespiratory symptoms. Am J Epidemiol 199O;132:67-76.
43. Sparrow D, O'Connor GT, Rosner B, et al. Methacholine air-way responsiveness and 24-hr urine excretion of sodium andpotassium: The Normative Aging Study. Am Rev Respir Dis1991;144:722-5.
44. Cerveri I, Bruschi C, Zoja MC, et al. Chronic respiratorysymptoms, bronchial responsiveness and dietary sodium andpotassium: a population-based study. (Abstract). Am RevRespir Dis 1993;147:A376.
45. Burney PG, Neild JE, Twort CH, et al. Effects of changingdietary sodium on airway response to histamine. Thorax1989,44:36-41.
46. Carey OJ, Locke C, Cookson JB. Effect of alterations ofdietary sodium on the severity of asthma in men. Thorax1993;48:714-18.
47. Medici TC, Schmid AZ, Hacki M, et al. Are asthmatics salt-sensitive? A preliminary controlled study. Chest 1993;104:1138^3.
48. Lieberman D, Heimer D. Effect of dietary sodium on theseverity of bronchial asthma. Thorax 1992;47:360-2.
49. Soutar A, Seaton A, Brown K. Bronchial reactivity anddietary antioxidants. Thorax 1997;52:166-70.
50. Noppen M, Vanmaele L, Impens N, et al. Bronchodilatingeffect of intravenous magnesium sulfate in acute severebronchial asthma. Chest 1990;97:373-6.
51. Tiffany BR, Berk WA, Todd IK, et al. Magnesium bolus orinfusion fails to improve expiratory flow in acute asthmaexacerbations. Chest 1993; 104:831^1.
52. Hill J, Micklewright A, Lewis S, et al. Investigation of theeffect of short-term change in dietary magnesium intake inasthma. Eur Respir J 1997; 10:2225-9.
53. De Valk HW, Kok PT, Struyvenberg A, et al. Extracellularand intracellular magnesium concentrations in asthmaticpatients. Eur Respir J 1993;6:1122-5.
54. Environmental Protection Agency, Office of Research andDevelopment, Office of Air and Radiation. Respiratoryhealth effects of passive smoking: lung cancer and other dis-orders. Washington, DC: Environmental Protection Agency,1992. (Publication no. EPA/600/6-90/006F).
55. Committee of the Environmental and Occupational HealthAssembly of the American Thoracic Society. Health effectsof outdoor air pollution. Part I of II. Am J Respir Crit CareMed 1996; 153:3-50.
56. Frei B, Foret M, Ames BN, et al. Gas phase oxidants of cig-arette smoke induce lipid peroxidation and changes inlipoprotein properties in human blood plasma: protectiveeffects of ascorbic acid. Biochem J 1991;277:133-8.
57. Pryor WA. Can vitamin E protect humans against the patho-logical effects of ozone in smog? Am J Clin Nutr 1991;53:702-22.
58. Trenga CA, Koenig JQ, Williams PV. Dietary antioxidantsand ozone-induced bronchial hyperresponsiveness in adultswith asthma. Arch Environ Health 2001;56:242-9.
59. Grievink L, Zijlstra AG, Ke X, et al. Double-blind interven-tion trial on modulation of ozone effects on pulmonary func-tion by antioxidant supplements. Am J Epidemiol 1999;149:306-14.
60. Romieu I, Meneses F, Ramirez M, et al. Antioxidant supple-mentation and respiratory functions among workers exposedto high levels of ozone. Am J Respir Crit Care Med 1998;158:226-32.
61. Bodner C, Godden D, Brown K, et al. Antioxidant intake andadult-onset wheeze: a case-control study. Eur Respir J 1999;13:22-30.
62. Troisi RJ, Willett WC, Weiss ST, et al. A prospective study ofdiet and adult-onset asthma. Am J Respir Crit Care Med1995;151:1401-8.
63. Cook DG, Carey I, Whincup PH, et al. Effect of fresh fruitconsumption on lung function and wheeze in children.Thorax 1997;52:628-33.
64. Forastiere F, Pistelli R, Sestini P, et al. Consumption of freshfruit in vitamin C and wheezing symptoms in children.Thorax 2000;55:283-8.
65. Mohsenin V, Dubois AB. Vitamin C and airways. Ann N YAcad Sci 1987;498:259-68.
66. Anderson R, Hay I, Van Wyk H, et al. The effect of ascorbateon cellular humoral immunity in asthmatic children. S AfrMedJ 1980;58:974-7.
67. Anderson R, Hay I, Van Wyk HA, et al. Ascorbic acid inbronchial asthma. S Afr Med J 1983;63:649-52.
68. Stone J, Hinks LJ, Beasley R, et al. Reduced selenium statusof patients with asthma. Clin Sci 1989;77:495-500.
69. Flatt A, Pearce N, Thomson CD, et al. Reduced selenium inasthmatic subjects in New Zealand. Thorax 1990;45:95-9.
70. Powell CV, Nash AA, Powers HJ, et al. Antioxidant status inasthma. Pediatr Pulmonol 1994; 18:34-8.
71. Britton J. Dietary fish oil and airways obstruction. Thorax1995,50:511-15.
72. Black PN, Sharpe S. Dietary fat and asthma: is there a con-nection? Eur Respir J 1997; 10:6-12.
73. Fluge O, Omenaas E, Eide GE, et al. Fish consumption andrespiratory symptoms among young adults in a Norwegiancommunity. Eur Respir J 1998; 12:336-40.
74. Peat J, Salome CM, Woolcock AJ. Factors associated withbronchial hyperresponsiveness in Australian adults and chil-
Epidemiol Rev Vol. 23, No. 2, 2001
Diet and Obstructive Lung Diseases 287
dren. Eur Respir J 1992;5:921-9.75. Hodge L, Salome CM, Peat JK, et al. Consumption of oily
fish and childhood asthma risk. Med J Aust 1996; 164:137^tO.76. Arm JP, Horton CE, Spur BW, et al. The effects of dietary
supplementation with fish oil lipids on the airways: responseto inhaled allergen in bronchial asthma. Am Rev Respir Dis1989; 139:1395^00.
77. Dry J, Vincent D. Effects of a fish oil diet on asthma: resultsof a 1-year double blind study. Int Arch Allergy ApplImmunol 1991 ;95:156-7.
78. Kirsch CM, Payan DG, Wong MY. The effect of eicosapen-taenoic acid in asthma. Clin Allergy 1988;18:177-87.
79. Knapp HR. Omega-3 fatty acids in respiratory diseases: areview. J Am Coll Nutr 1995;14:18-23.
80. Broughton KS, Johnson CS, Pace BK, et al. Reduced asthmasymptoms with n-3 fatty acid ingestion are related to 5-seriesleukotriene production. Am J Clin Nutr 1997;65:1011-17.
81. Villani F, Comazzi R, De Maria P, et al. Effects of dietarysupplementation with polyunsaturated fatty acids onbronchial hyperreactivity in subjects with seasonal asthma.Respiration 1998;65:265-9.
82. Hodge L, Salome CM, Hughes JM, et al. Effects of dietaryintake of omega-3 and omega-6 fatty acids on severity ofasthma in children. Eur Respir J 1998; 11:361-5.
83. Feinleib M, Rosenberg HM, Collins JG, et al. Trends inCOPD morbidity and mortality in the United States. Am RevRespir Dis 1989;140(suppl):S9-18.
84. Butland BK, Fehily AM, Elwood PC. Diet, lung function,and lung function decline in a cohort of 2512 middle agedmen. Thorax 2000;55:102-8.
85. Schwartz J, Weiss ST. Relationship between dietary vitaminC intake and pulmonary function in the First National Healthand Nutrition Examination Survey (NHANES I). Am J ClinNutr 1994;59:110-14.
86. Strachan DP, Cox BD, Erzinclioglu SW, et al. Ventilatoryfunction and winter fresh fruit consumption in a randomsample of British adults. Thorax 1991;46:624-9.
87. Britton JR, Pavord ID, Richards A, et al. Dietary antioxidantvitamin intake and lung function in the general population.Am J Respir Crit Care Med 1995;151:1383-7.
88. Ness AR, Khaw KT, Bingham S, et al. Vitamin C status andrespiratory function. Eur J Clin Nutr 1996;50:573-9.
89. Hu G, Zhang X, Chen J, et al. Dietary vitamin C intake andlung function in rural China. Am J Epidemiol 1998;148:594-9.
90. Dow L, Tracey M, Villar A, et al. Does dietary intake of vi-tamins C and E influence lung function in older people? AmJ Respir Crit Care Med 1996;154:1401-4.
91. Grievink L, Smit HA, Ocke C, et al. Dietary intake of antiox-idant (pro)-vitamins, respiratory symptoms and pulmonaryfunction: The MORGEN Study. Thorax 1998;53:166-71.
92. Tabak C, Smit HA, Rasanen L, et al. Dietary factors and pul-monary function: a cross sectional study in middle aged menfrom three European countries. Thorax 1999;54:1021-6.
93. Hu G, Cassano P. Antioxidant nutrients and pulmonary func-tion: The Third National Health and Nutrition ExaminationSurvey (NHANES JJI). Am J Epidemiol 2000; 151:975-81.
94. Carey IM, Strachan DP, Cook DG. Effects of changes infresh fruit consumption on ventilatory function in healthyBritish adults. Am J Respir Crit Care Med 1998;158:728-33.
95. Miedema I, Feskens EJ, Heederik D, et al. Dietary determi-nants of long-term incidence of chronic nonspecific lungdisease: The Zutphen Study. Am J Epidemiol 1993;138:37^5 .
96. Schunemann HJ, Grant BJ, Freudenheim JL, et al. The rela-tion of serum levels of antioxidant vitamins C and E, retinoland carotenoids with pulmonary function in the general pop-ulation. Am J Respir Crit Care Med 2001; 163:1246-55.
97. Morabia A, Menkes MJ, Comstock GW, et al. Serum retinoland airway obstruction. Am J Epidemiol 1990;132:77-82.
98. Willett W, Colditz G. Vitamin A and lung cancer. In: WillettW, ed. Nutritional epidemiology. 2nd ed. New York, NY:Oxford University Press, 1998:357-76.
99. Shahar E, Folsom AR, Melnick SL, et al. Does dietaryvitamin A protect against airway obstruction? TheAtherosclerosis Risk in Communities (ARIC) StudyInvestigators. Am J Respir Crit Care Med 1994; 150:978-82.
100. Schwartz J, Weiss ST. The relationship of dietary fish intaketo level of pulmonary function in the First National Healthand Nutrition Examination Survey (NHANES I). Eur RespirJ 1994;7:1821-4.
101. Sharp DS, Rodriguez BL, Shahar E. Fish consumption maylimit the damage of smoking on the lung. Am J Respir CritCare Med 1994;150:983-7.
102. Levine M, Conry-Cantilena C, Wang Y, et al. Vitamin Cpharmacokinetics in healthy volunteers: evidence for a rec-ommended dietary allowance. Proc Natl Acad Sci U S A1996;93:3704-9.
103. Potter JD, Finnegan JR, Guinard JX, et al. 5 A Day for BetterHealth Program evaluation report. (NIH publication no. 01-4904). Bethesda, MD: National Cancer Institute, 2000.(www.cancercontrol.cancer.gov/5ad_exec.html).
104. Krebs-Smith SM, Cook A, Subar AF, et al. US adults' fruitand vegetable intake, 1989 to 1991: a revised baseline forthe Healthy People 2000 objective. Am J Public Health1995;85:1609-11.
Epidemiol Rev Vol. 23, No. 2, 2001





























