Embed Size (px)
Citation preview
12th ESO Colorectal Cancer Observatory:Innovation and care in the next 12 months
Wednesday 1st July 2015, 18:45 – 20:15
Panellists:Nadir Arber, IL
Roberto Labianca, ITEric Van Cutsem, BEJosep Tabernero, ES
Bernard Nordlinger, FRNeil Howie, UK/RS
Chair: Mario Dicato, LUCo-Chair: Jola Gore-Booth, UK
12th ESO Colorectal Cancer Observatory:Innovation and care in the next 12 months
Nadir Arber
The Tel-Aviv Sourasky Medical Center
Tel Aviv, Israel
View of a Gastroenterologist
ESO Observatory:Screening of CRC
Retired American Major League Baseball
catcher, manager, and coach and
Integrated Cancer Prevention Center, Tel Aviv
It's tough to make predictions, especially about the future."
"Yogi" Berra and Nadir Arber

My Financial Disclosures:Bayer
GI ViewTakeda
Bio ViewCheck-Cap
Bio-ExplorerNawe-Pharma
Ideal CRC Screening Test• Organized program
• High Uptake
• Test accuracy (NPV, PPV, Spec, Sens)
• Quality (FIT, colonoscopy, polypectomy)
• Costs
• Adherence to surveillance
• Reduced incidence of CR neoplasia
• Reduced specific morbidity
• Reduced specific mortality
• Reduced overall mortality
Blood tests (Septin9, Medial, CD24)
Stool Tests (FOBT, FIT, Cologuard, M2-PK)
Sigmoidoscopy
Colonoscopy
CT-colonography
Capsule endoscopy (Covidian, Check-Cap)
Different ScreeningModalities
Any Screening Modality is Better
than NothingBut colonoscopy is the
best option….in 2016…..as well
In 2015
• Before (referral practices, consent, anticoagulants,
bowel prep quality)
• During (sedation, technique, difficult polyps,
safety issues, documentation)
• After (recovery, post-procedure questionnaire,
surveillance recommendations)
European Guidelines for Quality Assurance in CRC Screening
Ed. J. Patnick, N Segnan, L. Von Karsa
NordICC trial – Polish arm
Kaminski MF, Regula J et al.N Engl J Med, 2010; 362: 1795-803
Colonoscopy Quality Parameters
• Mean withdrawal time (> 6
minutes)
• Adenoma detection rate
• Cecal intubation rate
• Number of adenomas/colonoscopy
• Bowel prep quality
• Photodocumentation of the cecum
• Adverse events (24 hours – 30 days)
Optimizing Colonoscopy Efficacy:
New/Current Technologies• Endocuff
• G-Eye
• Full Spectrum Endoscopy
• Extra Wide Angle View Endoscope
• Third Eye Retroscope
• Third Eye Panoramic
• Aer-O-scope
• Colon Capsule
• Prepless Colonic Capsule (Check-Cap)
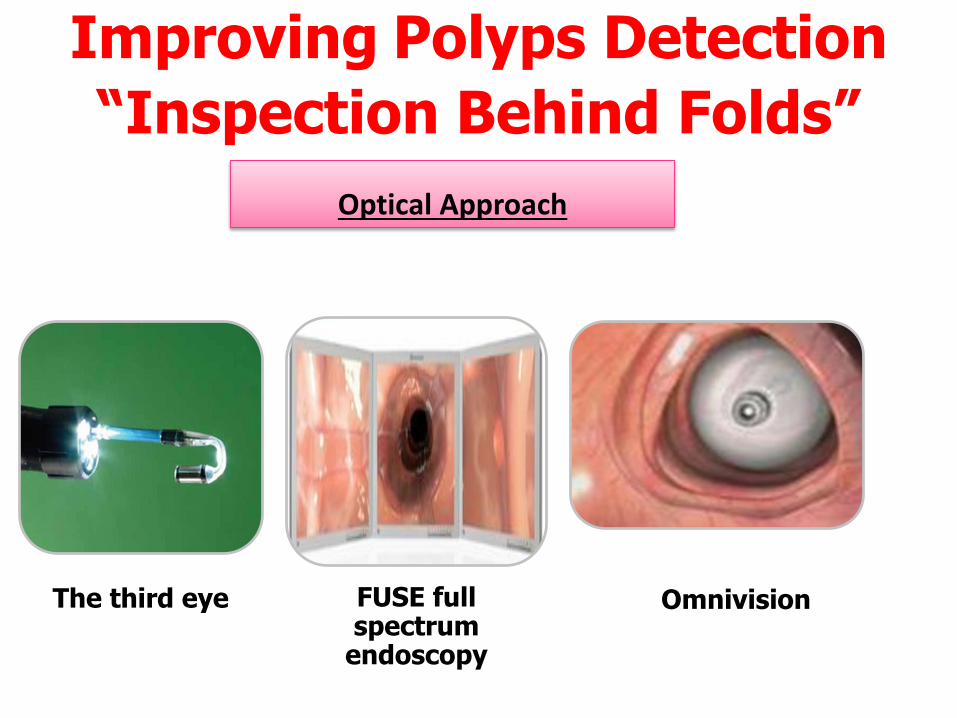
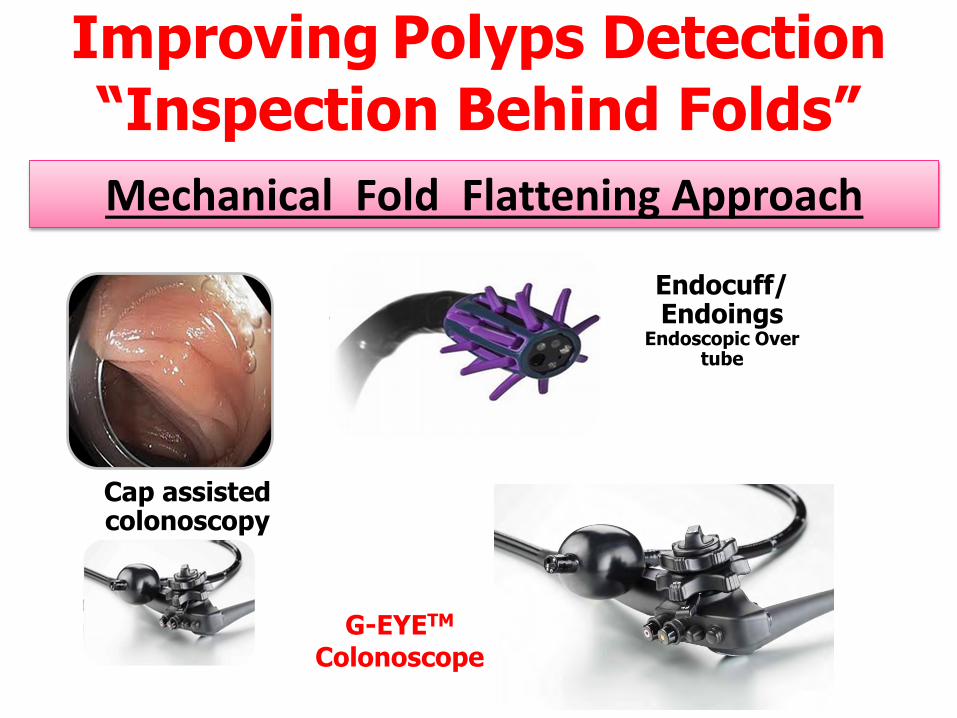
Improving Polyps Detection
“Inspection Behind Folds”
Optical Approach
The third eye FUSE full spectrum
endoscopy
Omnivision
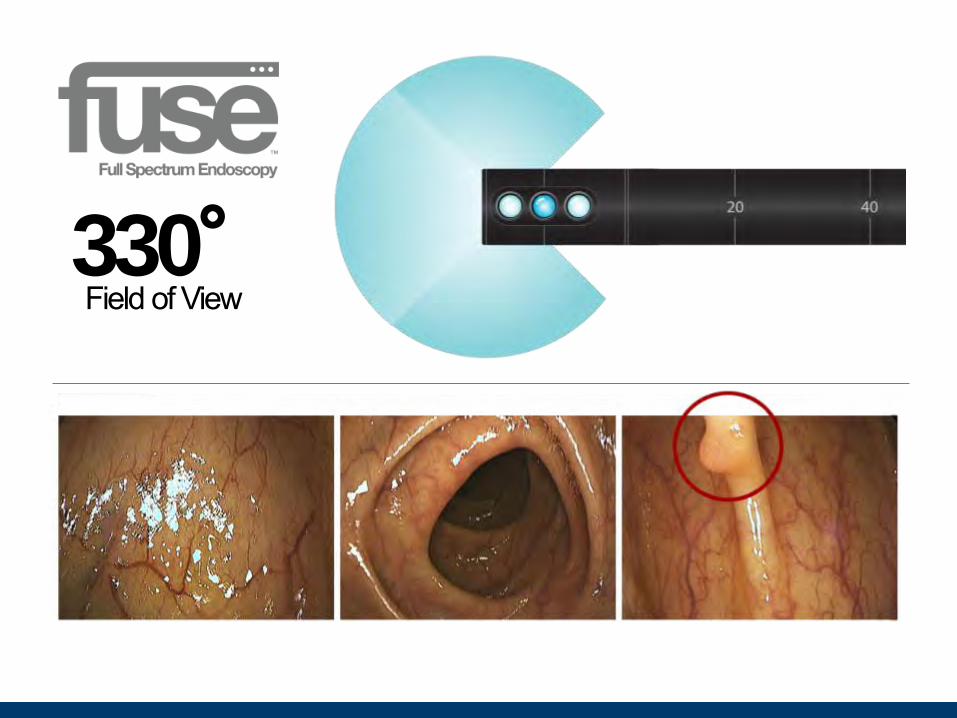
330°Field of View
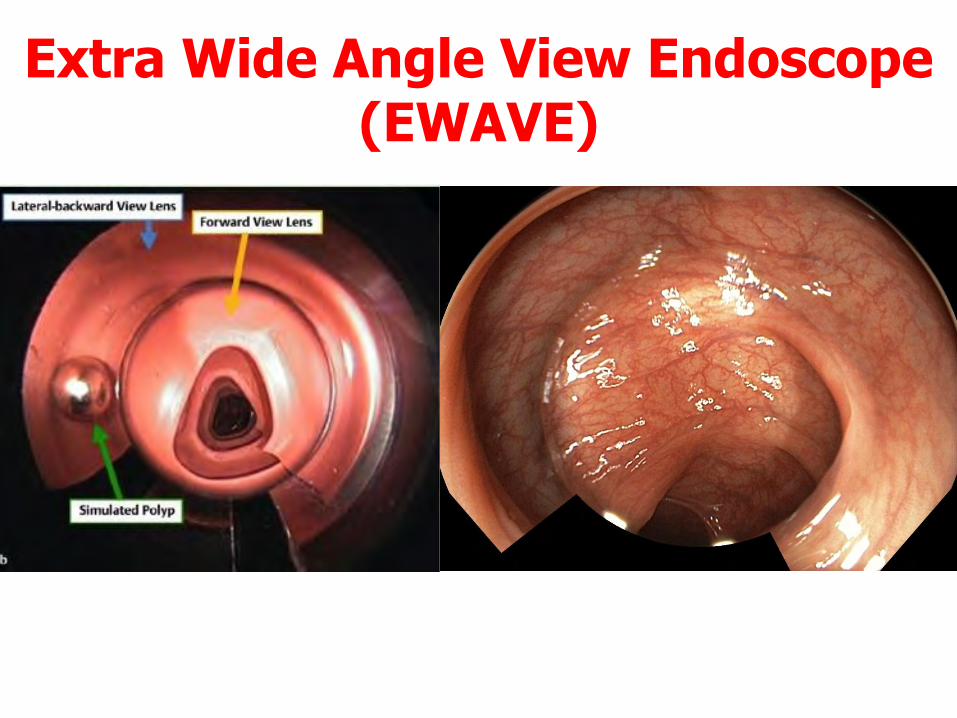
Extra Wide Angle View Endoscope(EWAVE)
Improving Polyps Detection
“Inspection Behind Folds”
Mechanical Fold Flattening Approach
Cap assisted colonoscopy
Endocuff/Endoings
Endoscopic Over tube
G-EYETM
Colonoscope
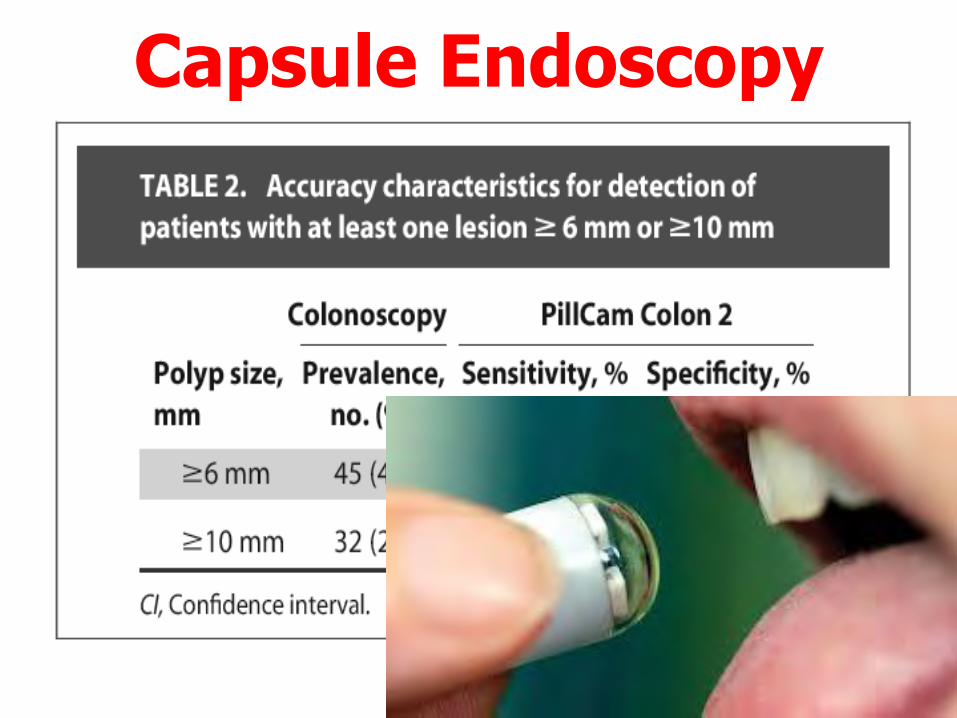
Capsule Endoscopy
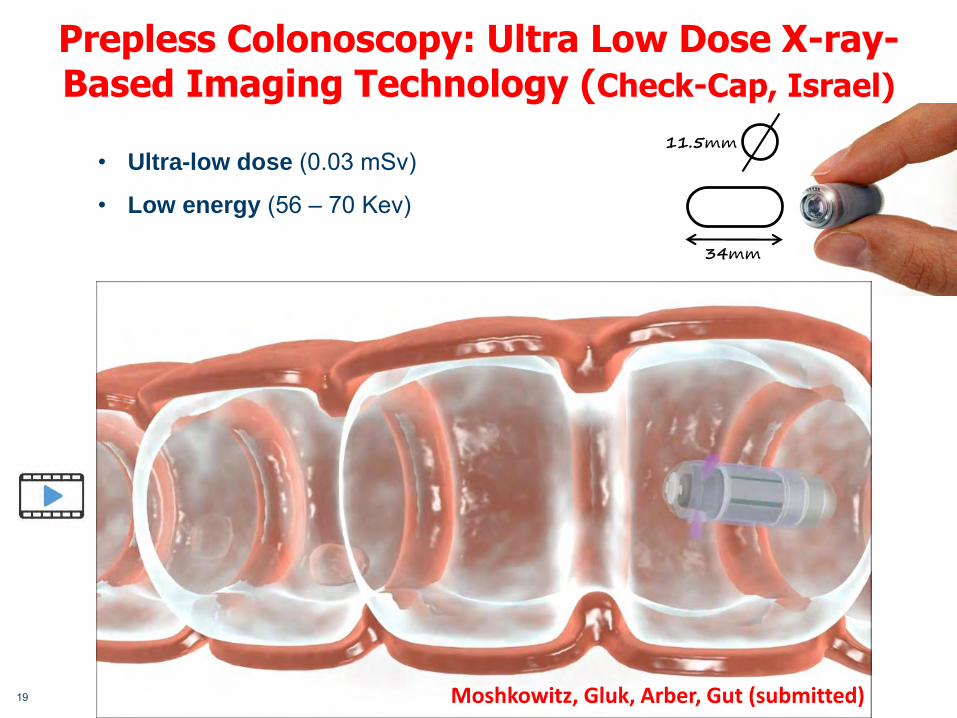
Prepless Colonoscopy: Ultra Low Dose X-ray-Based Imaging Technology (Check-Cap, Israel)
19
• Ultra-low dose (0.03 mSv)
• Low energy (56 – 70 Kev)
11.5mm
34mm
Moshkowitz, Gluk, Arber, Gut (submitted)

Single Use Colonoscope
20
Aeroscope (GI View, Israel):
Self Propelling Self Navigating
New Technologies – Improve Imaging
• Autofluorescence
• Chromoendoscopy
• HD
• NBI
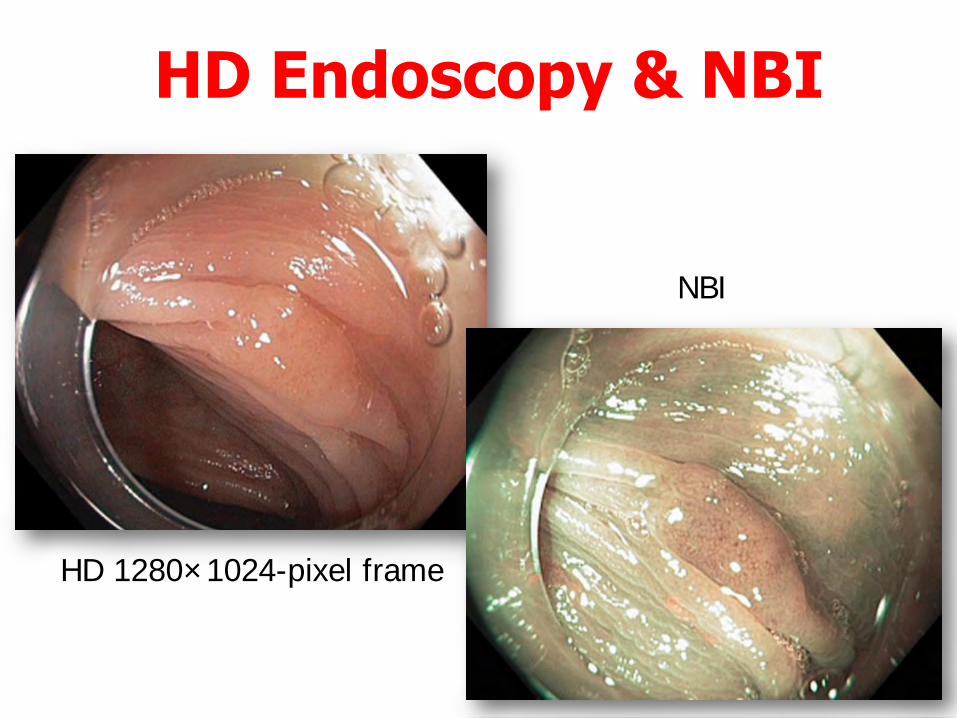
HD Endoscopy & NBI
HD 1280×1024-pixel frame
NBI
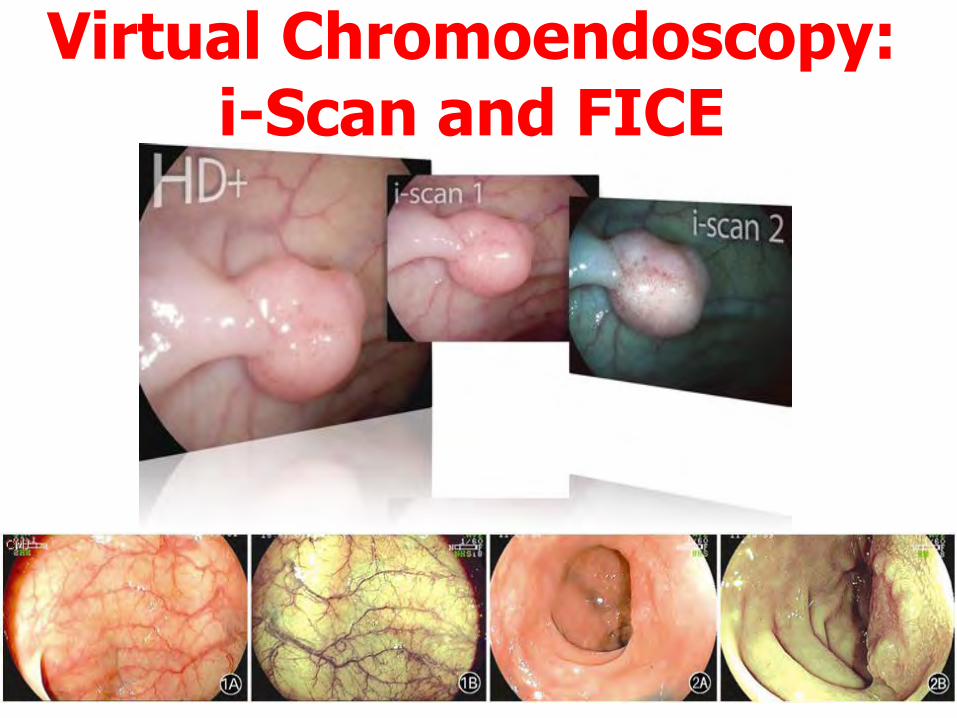
Virtual Chromoendoscopy:i-Scan and FICE
23

Does it look like anattractive screening test?
Stool Testing

• Methylated Septin 9, Church et al. Gut 2014 ;63:317-25
• CD24, Kraus and Arber. Disease Markers, 2015
• Meidal
Highest Compliance with Blood Tests
• MedialICS (Israel)
Approach
• Looking into
standard CBC
• Identifying trends
and variations
within the normal
ranges in millions
of CBC26
MeScore: Computed Indicator for CRC Findings
MeScore
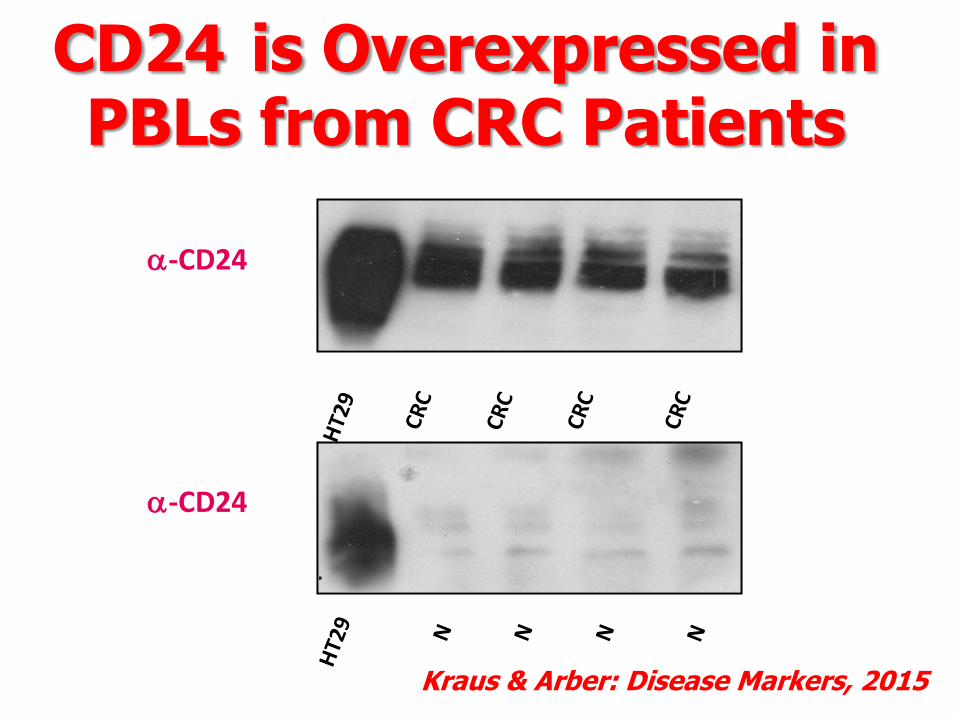
CD24 is Overexpressed in PBLs from CRC Patients
a-CD24
a-CD24
Kraus & Arber: Disease Markers, 2015
Conclusions
-Two stages approach
- Non invasive test as the initial step
Blood test
Stool test/capsule/virtual colonoscopy/prepless cap?
- Quality parameters for colonoscopy
ADR
Withdrawal time
“A test is better than none, and the best test is the one that is done”
Conclusions- Monitoring of quality (The big brother)
- Improvement in teaching methods
- Advanced technologies are available,
but are time and money consuming
- Public demands
- Legal issues

12th ESO Colorectal Cancer Observatory :Innovation and care in the next 12 months
Roberto Labianca
Hospital Giovanni XXIII
Bergamo, Italy
View of a Medical Oncologist
Adjuvant therapy of colorectal cancerColon Cancer
Colon cancer stage II patients will receive adjuvant CT only if“high-risk”, according to clinico-pathological criteria(biological criteria: still experimental)
Colon cancer stage III: FOLFOX or XELOX for 6 months willremain the standard treatment in patients up to 70 (75) years
In stage III elderly patient: fluoropyrimidine alone is still anacceptable choice
Duration could decrease to 3 months (Kumar, CCC 2015) ifthe ongoing IDEA collaboration will be positive (but dataexpected only in 2017-2018)
Avenues for progress
The interventions on lifestyle (diet, physical exercise,smoking habits…) will gain an increased roleNew independent studies will evaluate aspirin (or COX-2inhibitors) +/- chemotherapyAlso immunotherapy could be evaluated in this setting(e.g.: vaccine in Stage IV R0)Anti-PD1/PDL-1 in MSI patients???The opportunities for translational (BRAF, MSI…) orepidemiological (e.g.: BMI, metformin, L/N,thromboembolism…) research linked to adjuvant trialswill increase
Colon Cancer
Rectal Cancer
In preoperative setting: fluoropyrimidine alone(capecitabine or 5FU) will remain the standard, without arole for oxaliplatinIn postoperative setting: adjuvant chemotherapy(fluoropyrimidine + oxaliplatin) will be more frequentlyused in clinical practice (see also: EXPERT DISCUSSIONHERE TODAY)Through better neoadjuvant treatment: more sphinctersaving surgeryBiological/genomic characterization: not ready for use
12th ESO Colorectal Cancer Observatory :Innovation and care in the next 12 months
Eric Van Cutsem
University Hospital Gasthuisberg
Leuven, Belgium
View of a Medical Oncologist
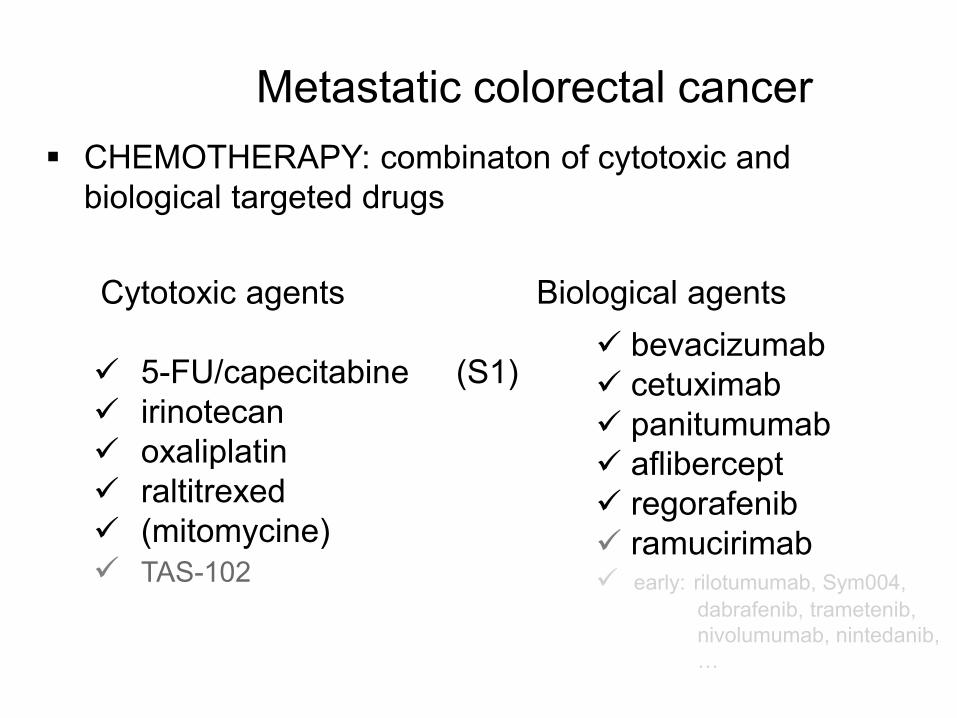
Metastatic colorectal cancer CHEMOTHERAPY: combinaton of cytotoxic and
biological targeted drugs
Cytotoxic agents Biological agents
5-FU/capecitabine (S1) irinotecan oxaliplatin raltitrexed (mitomycine) TAS-102
bevacizumab cetuximab panitumumab aflibercept regorafenib ramucirimab early: rilotumumab, Sym004,
dabrafenib, trametenib, nivolumumab, nintedanib, …
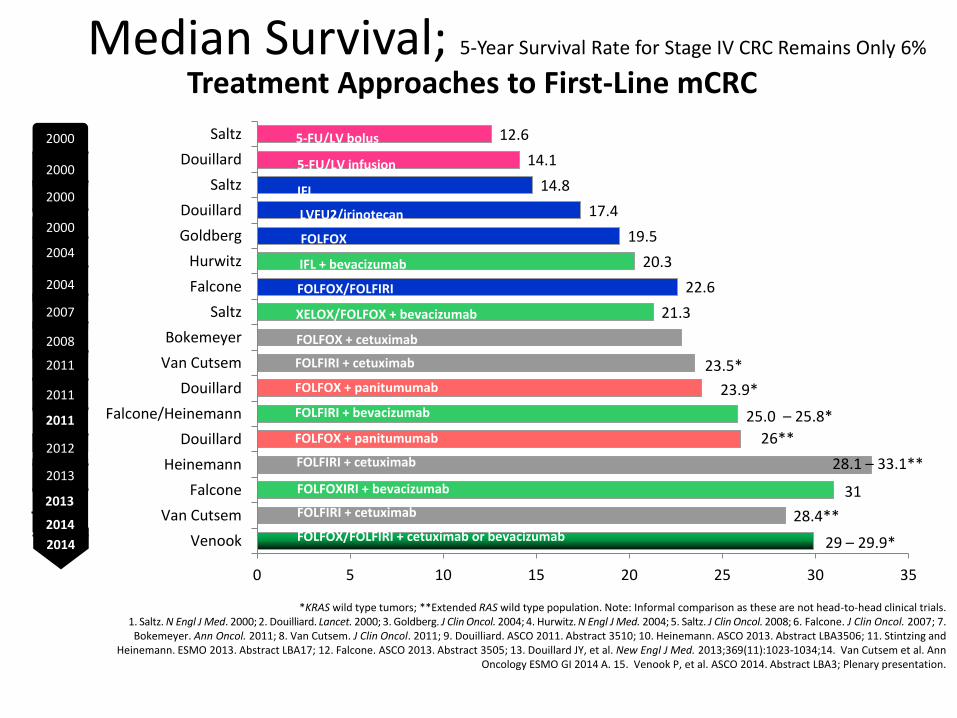
Median Survival; 5-Year Survival Rate for Stage IV CRC Remains Only 6%
*KRAS wild type tumors; **Extended RAS wild type population. Note: Informal comparison as these are not head-to-head clinical trials.1. Saltz. N Engl J Med. 2000; 2. Douilliard. Lancet. 2000; 3. Goldberg. J Clin Oncol. 2004; 4. Hurwitz. N Engl J Med. 2004; 5. Saltz. J Clin Oncol. 2008; 6. Falcone. J Clin Oncol. 2007; 7. Bokemeyer. Ann Oncol. 2011; 8. Van Cutsem. J Clin Oncol. 2011; 9. Douilliard. ASCO 2011. Abstract 3510; 10. Heinemann. ASCO 2013. Abstract LBA3506; 11. Stintzing and
Heinemann. ESMO 2013. Abstract LBA17; 12. Falcone. ASCO 2013. Abstract 3505; 13. Douillard JY, et al. New Engl J Med. 2013;369(11):1023-1034;14. Van Cutsem et al. Ann Oncology ESMO GI 2014 A. 15. Venook P, et al. ASCO 2014. Abstract LBA3; Plenary presentation.
29 – 29.9*
28.4**
31
28.1 – 33.1**
26**
25.0 – 25.8*
23.9*
23.5*
21.3
22.6
20.3
19.5
17.4
14.8
14.1
12.6
0 5 10 15 20 25 30 35
Venook
Van Cutsem
Falcone
Heinemann
Douillard
Falcone/Heinemann
Douillard
Van Cutsem
Bokemeyer
Saltz
Falcone
Hurwitz
Goldberg
Douillard
Saltz
Douillard
Saltz
Overall Survival (months)
5-FU/LV bolus
5-FU/LV infusion
IFL
LVFU2/irinotecan
FOLFOX
IFL + bevacizumab
FOLFOX/FOLFIRI
XELOX/FOLFOX + bevacizumab
FOLFOX + cetuximab
FOLFIRI + cetuximab
FOLFOX + panitumumab
Treatment Approaches to First-Line mCRC
FOLFIRI + bevacizumab
2013
2000
2012
2011
2011
2008
2007
2004
2004
2000
2000
2000
2011
2013
2014FOLFOX/FOLFIRI + cetuximab or bevacizumab
2013
22.8*
FOLFOXIRI + bevacizumab
FOLFIRI + cetuximab
FOLFOX + panitumumab
FOLFIRI + cetuximab
2014
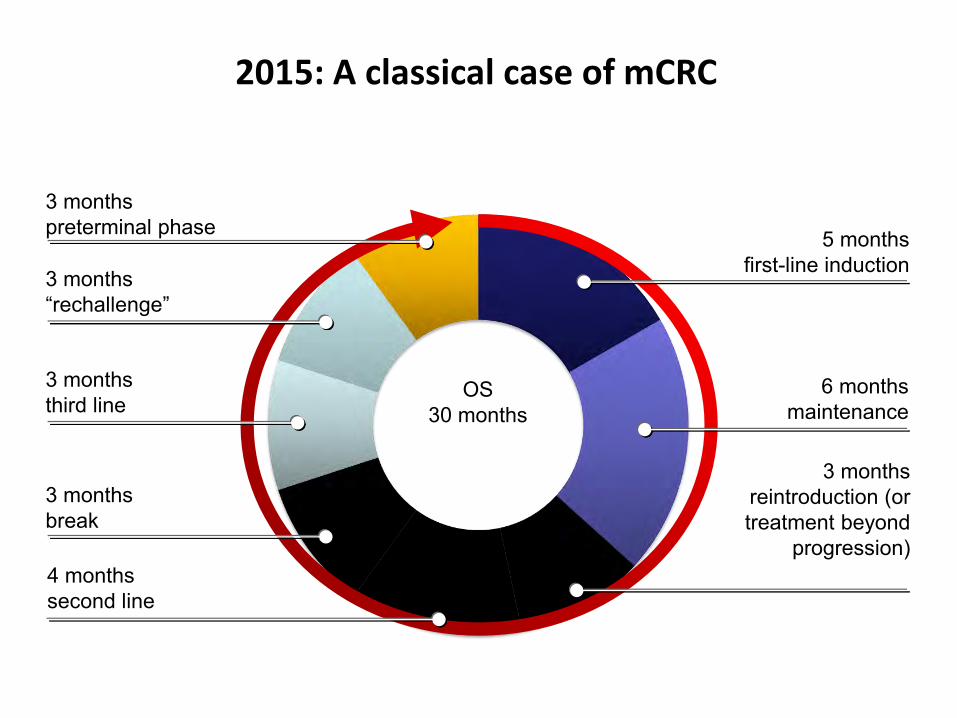
OS30 months
2015: A classical case of mCRC
5 monthsfirst-line induction
3 monthsreintroduction (or treatment beyond
progression)
3 months“rechallenge”
3 monthsbreak
6 monthsmaintenance
4 monthssecond line
3 monthsthird line
3 monthspreterminal phase
Metastatic colorectal cancer (mCRC) is not one disease
Patient and tumor characteristics vary widely
Tumor cell heterogeneity is what makes tumors challenging to treat:
– Multiple molecular alterations occur during tumor progression
– Various molecular signaling pathways are involved
Development of drugs which target and inhibit key molecular pathways is an essential step towards personalized cancer care
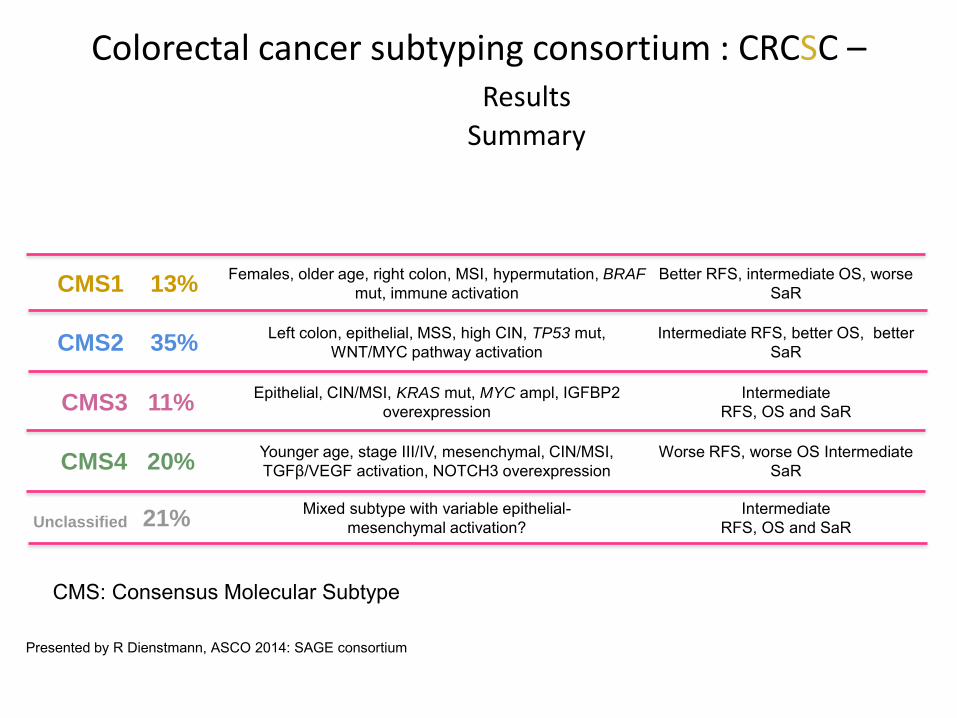
Colorectal cancer subtyping consortium : CRCSC –Results
Summary
CMS1 13%Females, older age, right colon, MSI, hypermutation, BRAF
mut, immune activationBetter RFS, intermediate OS, worse
SaR
CMS2 35% Left colon, epithelial, MSS, high CIN, TP53 mut,
WNT/MYC pathway activationIntermediate RFS, better OS, better
SaR
CMS3 11%Epithelial, CIN/MSI, KRAS mut, MYC ampl, IGFBP2
overexpressionIntermediate
RFS, OS and SaR
CMS4 20%Younger age, stage III/IV, mesenchymal, CIN/MSI, TGFβ/VEGF activation, NOTCH3 overexpression
Worse RFS, worse OS Intermediate SaR
Unclassified 21%Mixed subtype with variable epithelial-
mesenchymal activation?Intermediate
RFS, OS and SaR
CMS: Consensus Molecular Subtype
Presented by R Dienstmann, ASCO 2014: SAGE consortium
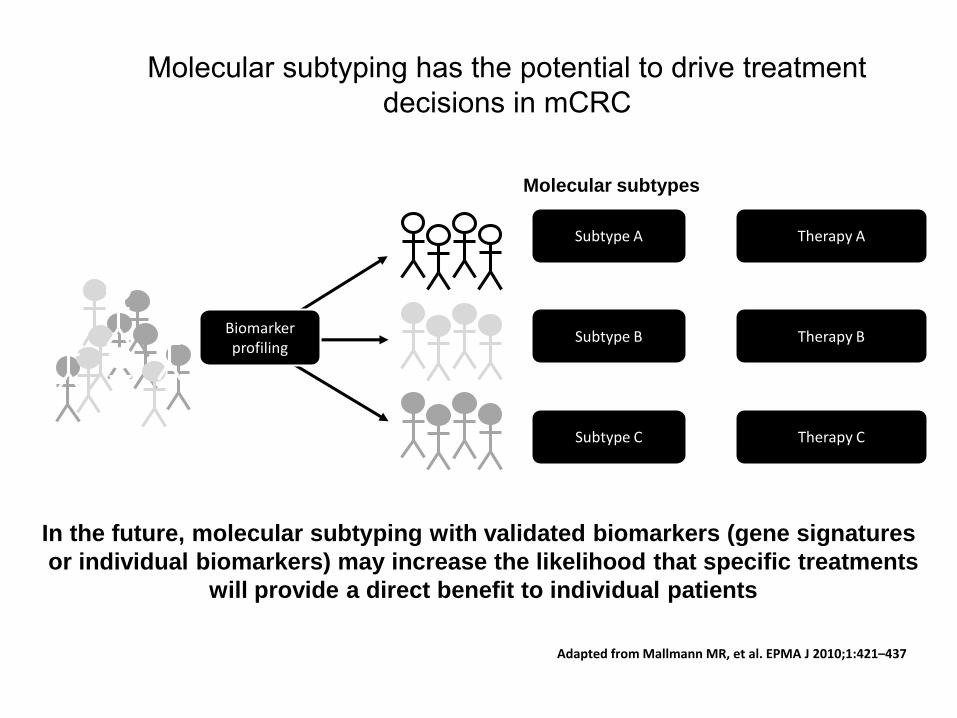
Molecular subtyping has the potential to drive treatment decisions in mCRC
Adapted from Mallmann MR, et al. EPMA J 2010;1:421–437
Molecular subtypes
Subtype A Therapy A
Subtype B Therapy B
Subtype C Therapy C
In the future, molecular subtyping with validated biomarkers (gene signatures
or individual biomarkers) may increase the likelihood that specific treatments
will provide a direct benefit to individual patients
Biomarkerprofiling
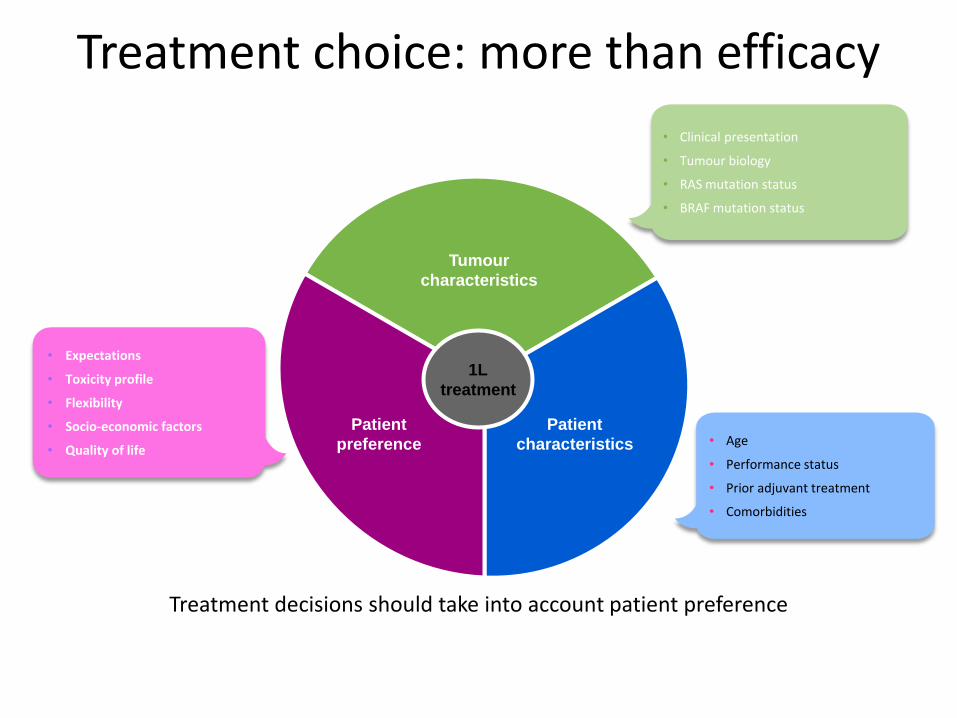
Treatment decisions should take into account patient preference
1L
treatment
• Expectations
• Toxicity profile
• Flexibility
• Socio-economic factors
• Quality of life• Age
• Performance status
• Prior adjuvant treatment
• Comorbidities
Tumour
characteristics
Patient
preference
Patient
characteristics
• Clinical presentation
• Tumour biology
• RAS mutation status
• BRAF mutation status
Treatment choice: more than efficacy
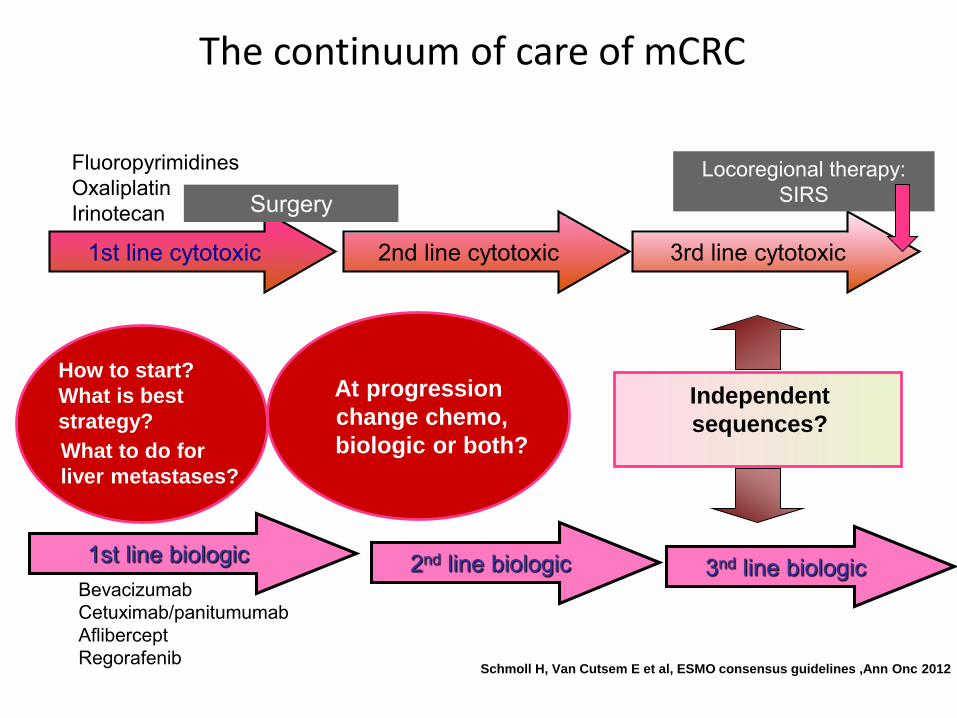
The continuum of care of mCRC
1st line cytotoxic 3rd line cytotoxic2nd line cytotoxic
1st line biologic 2nd line biologic
At progression
change chemo,
biologic or both?
Independent
sequences?
FluoropyrimidinesOxaliplatinIrinotecan
BevacizumabCetuximab/panitumumabAfliberceptRegorafenib
How to start?
What is best
strategy?
What to do for
liver metastases?
Locoregional therapy: SIRSSurgery
3nd line biologic
Schmoll H, Van Cutsem E et al, ESMO consensus guidelines ,Ann Onc 2012

Josep TaberneroVall d’Hebron University Hospital
Vall d’Hebron Institute of OncologyBarcelona
New Therapies
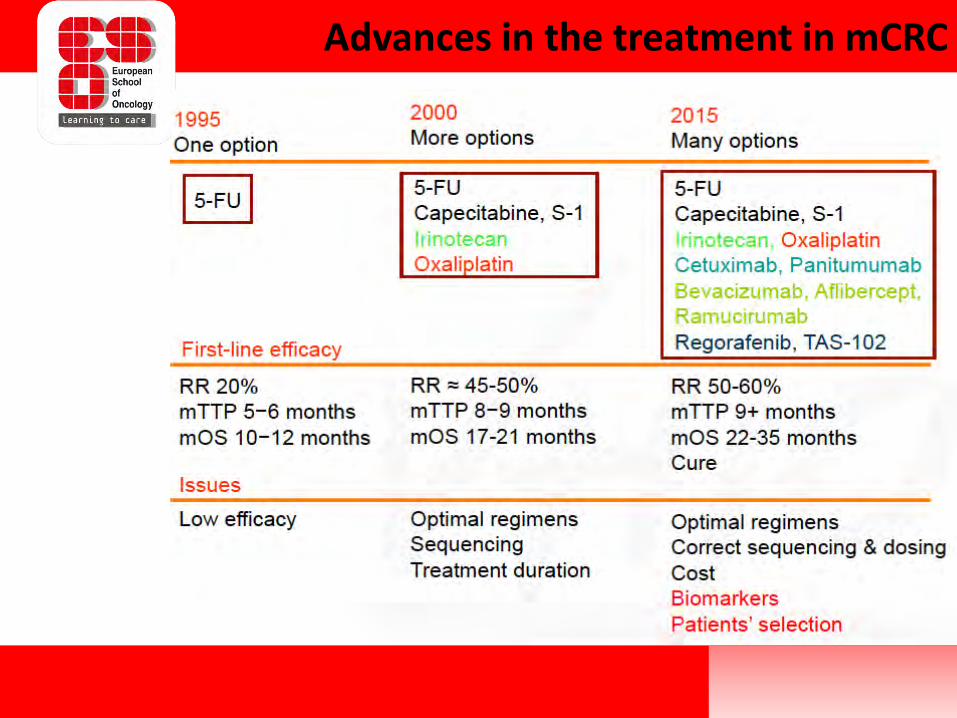
Advances in the treatment in mCRC
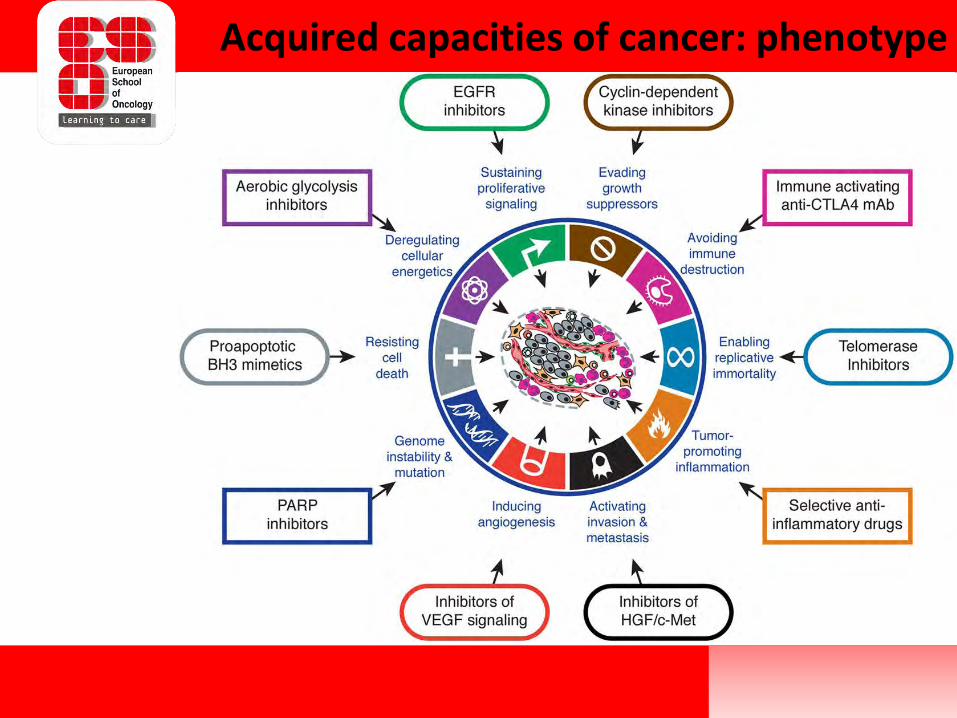
Acquired capacities of cancer: phenotype
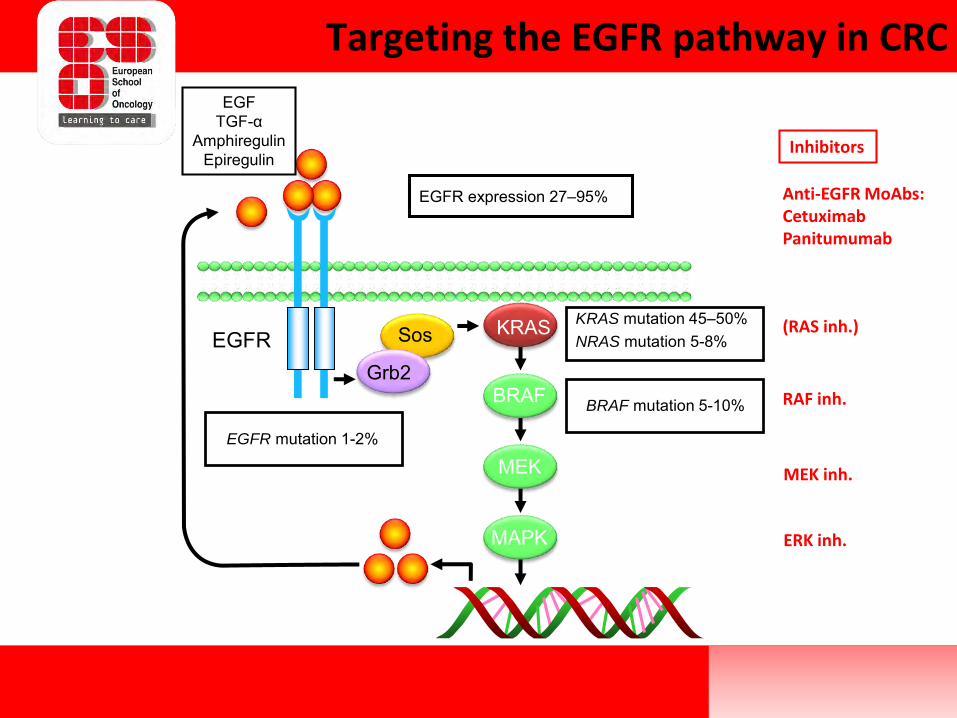
Targeting the EGFR pathway in CRC
BRAF mutation 5-10%
KRAS mutation 45–50%NRAS mutation 5-8%
EGFR expression 27–95%
EGFR mutation 1-2%
MAPK
MEK
BRAF
KRAS
EGFTGF-α
AmphiregulinEpiregulin
Grb2
SosEGFR
Anti-EGFR MoAbs:CetuximabPanitumumab
(RAS inh.)
RAF inh.
MEK inh.
ERK inh.
Inhibitors
• More efficient anti-EGFR MoAbs:
– Sym004, MM-151
• MoAbs directed to other members of the EGFR/HER family:
– HER-2: trastuzumab, trastuzumab + pertuzumab, trastuzumab + lapatinib
– HER-3: Duligotuzumab (MEHD7945A)
• MoAbs directed to other receptors:
– cMET: rilotumab, ficlatuzumab, omartuzumab
• Combination with downstream effector inhibitors:
– BRAF mt: Anti-EGFR MoAb + BRAFi / MEKi
Beyond EGFR inhibition
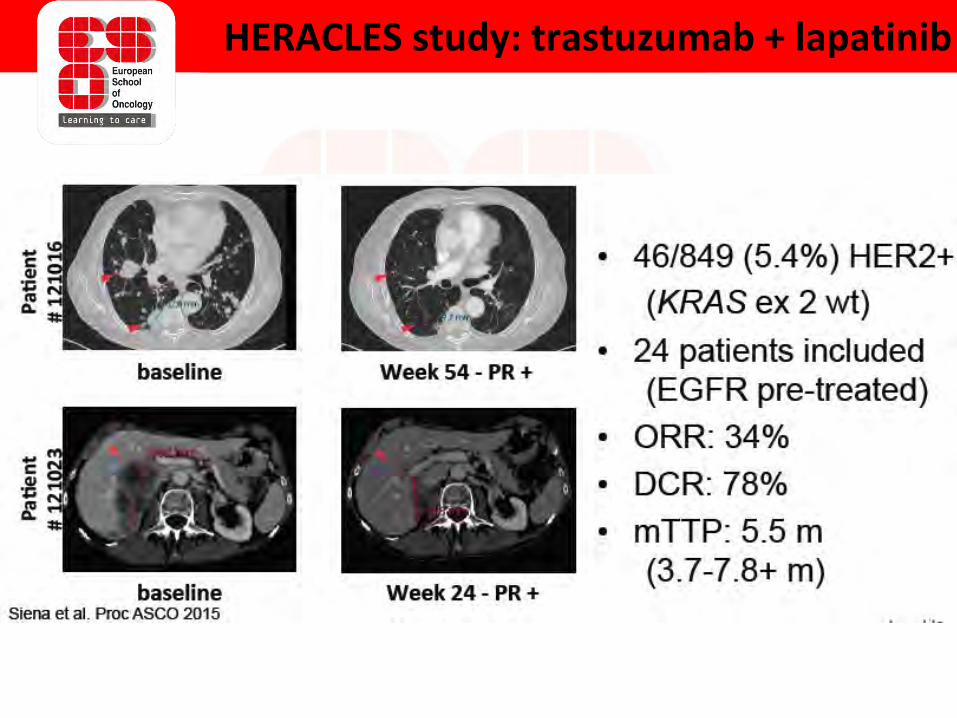
HERACLES study: trastuzumab + lapatinib
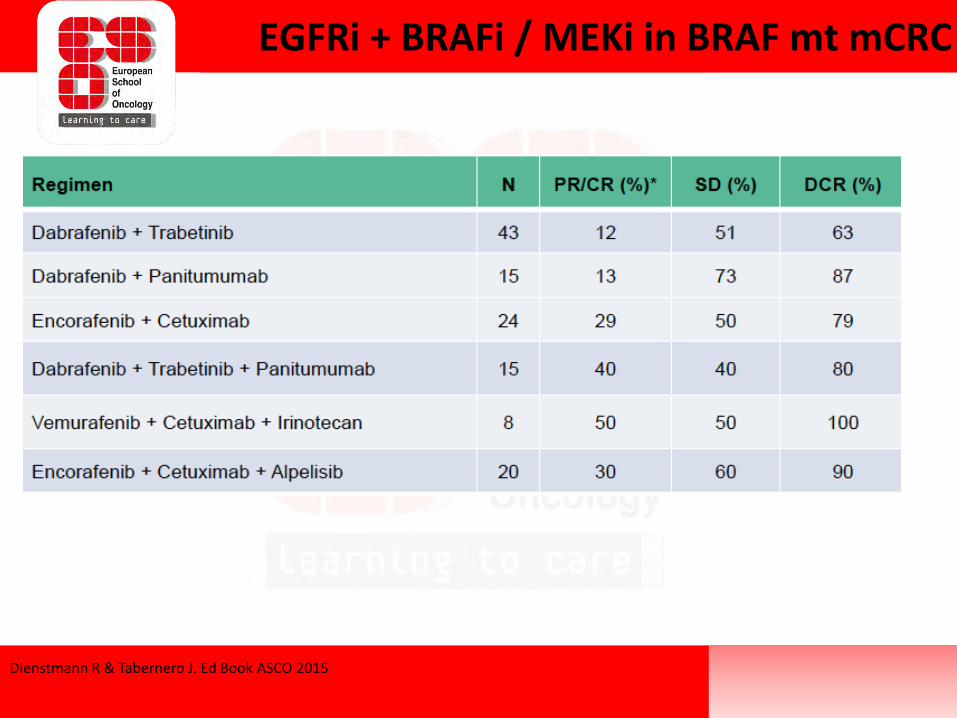
Dienstmann R & Tabernero J. Ed Book ASCO 2015
EGFRi + BRAFi / MEKi in BRAF mt mCRC
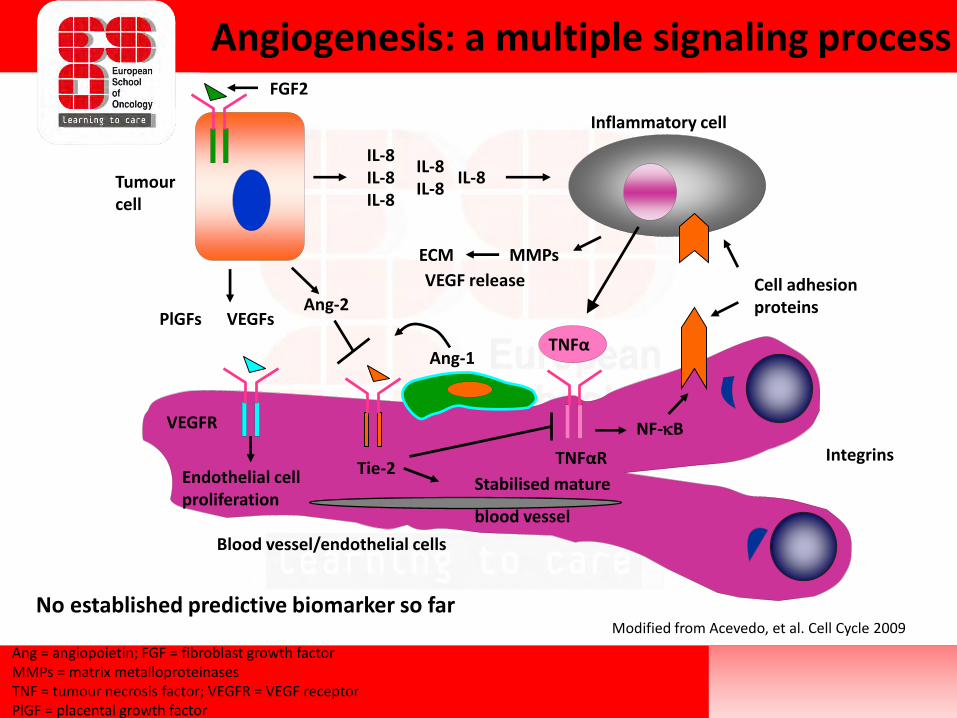
Modified from Acevedo, et al. Cell Cycle 2009
Ang = angiopoietin; FGF = fibroblast growth factor MMPs = matrix metalloproteinasesTNF = tumour necrosis factor; VEGFR = VEGF receptorPlGF = placental growth factor
Tumourcell
FGF2
IL-8IL-8IL-8
IL-8IL-8
IL-8
ECM MMPs
VEGF release
Inflammatory cell
Cell adhesionproteins
VEGFsAng-2
TNFα
TNFαR
NF-kB
Ang-1
Stabilised mature
blood vessel
Tie-2
VEGFR
Endothelial cellproliferation
Blood vessel/endothelial cells
PlGFs
Integrins
Angiogenesis: a multiple signaling process
No established predictive biomarker so far
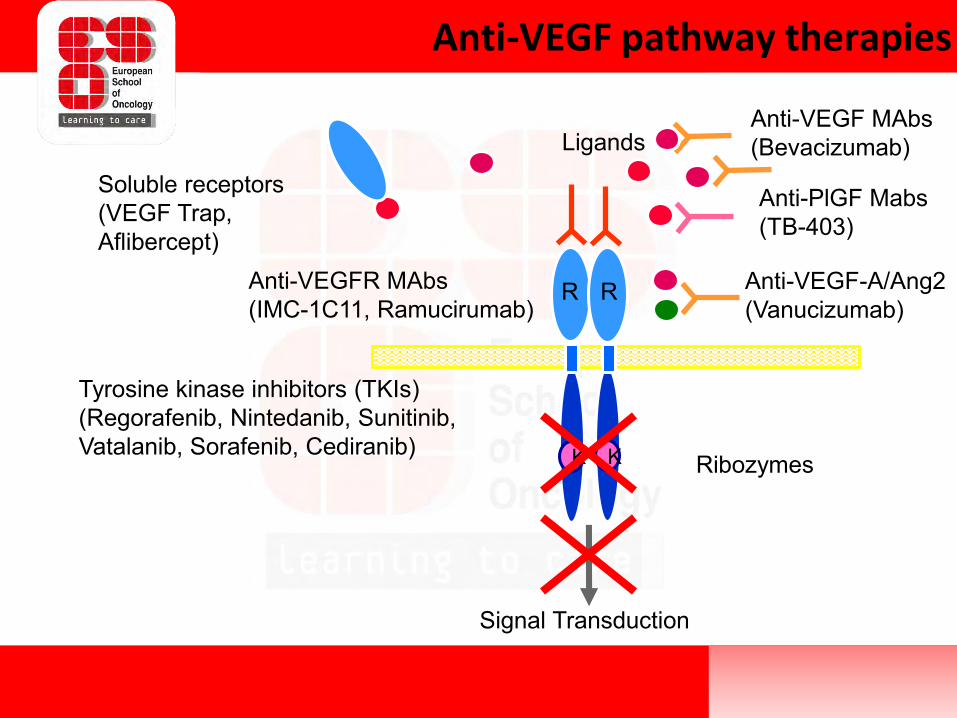
Tyrosine kinase inhibitors (TKIs)(Regorafenib, Nintedanib, Sunitinib, Vatalanib, Sorafenib, Cediranib)
Anti-VEGFR MAbs(IMC-1C11, Ramucirumab)
Signal Transduction
R R
K K
LigandsAnti-VEGF MAbs(Bevacizumab)
Soluble receptors(VEGF Trap, Aflibercept)
Ribozymes
Anti-PlGF Mabs(TB-403)
Anti-VEGF pathway therapies
Anti-VEGF-A/Ang2(Vanucizumab)
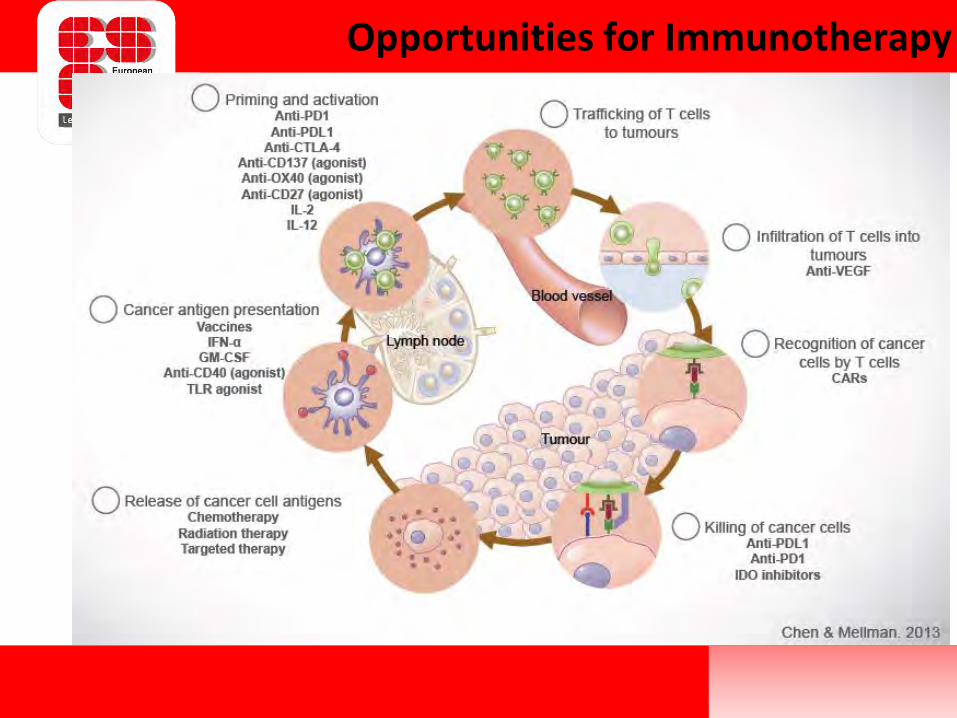
Opportunities for Immunotherapy
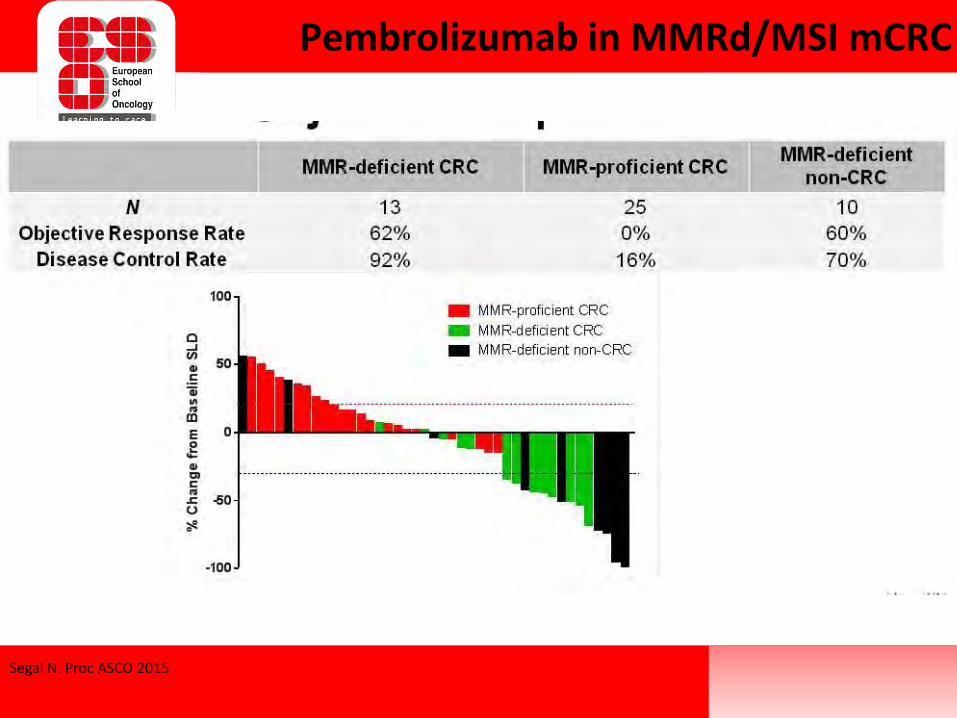
Segal N. Proc ASCO 2015
Pembrolizumab in MMRd/MSI mCRC
• Target discovery has resulted in numerous novel drugs in clinical development
• Median survival of patients with mCRC has reached a new benchmark of ≈30 months
• Different CRC subtypes: genomic signatures• Tumor heterogenity and clonal selection/evolution• Several examples of treatment benefit in small populations• Need for molecular profile and selection• Combinations: mechanistic interactions, rationale-based• Need to balance pricing/reimbursement for accesibility
Summary and challenges
12th ESO Colorectal Cancer Observatory:Innovation and care in the next 12 months
Bernard Nordlinger
Hôpital Amboise Paré
Boulogne-Billancourt, France
View of a Surgical Oncologist
Surgical progress in the treatment of rectal cancer
- Laparoscopic vs Open- One port: NOTES- Robot
COLOR II Study
• International trial in 30 hospitals,
• 1044 patients with adenocarcinoma of the rectum
• 15 cm of the anal verge, not invading adjacent tissues, no T4 and T3 with CRM less than 2mm and without distant metastases
• Non inferiority margin 5%
• laparoscopic n= 699
• open surgery n= 345, 2:1 ratio.
• End points: primary: 3y locoregional recurrence
secondary: DFS,OS.
COLOR II Study:Results
3 years:
- Locoregional recurrence: 5.0% in the 2 groups
- DFS :74.8% laparoscopic and 70.8% open.
- OS : 86.7% laparoscopic, 83.6% open.
COLOR II Study:Conclusions
• Laparoscopic surgery in patients with rectal cancer was associated with rates of
- locoregional recurrence
- disease-free
- overall survival
• Similar to those for open surgery
COREAN TRIAL• Open versus laparoscopic surgery for mid or low rectal
cancer cT3N0–2M0 after neoadjuvantchemoradiotherapy
• Randomised controlled trial; non inferiority, margin 15%
• From April 2006, to Aug 2009, 3 centers in Korea. 340 patients to receive either open surgery (n=170) or laparoscopic surgery (n=170).
• Stratification by sex and preoperative chemotherapy regimen.
• Primary endpoint: 3 y DFS, with a non-inferiority margin of 15%.
• 3 year disease-free survival was 72·5% (95% CI 65·0–78·6) for the open surgery group and 79·2% (72·3–84·6) for the laparoscopic surgery group
• Difference was lower than the prespecified non-inferiority margin (–6·7%,95% CI –15·8 to 2·4; p<0·0001).
• 25 (15%) patients died in the open group and 20 (12%) died in the laparoscopicgroup. No deaths were treatment related.
COREAN TRIAL: RESULTS

COREAN TRIAL: INTERPRETATION
• Laparoscopic resection for locally advanced rectal cancer after preoperative chemoradiotherapy provides similar outcomes for disease-free survival as open resection.
ENDOSCOPIC TRANSANAL PROCTECTOMY
• NOTES: natural orifice transluminal endoscopic surgery
• The aim of this study was to evaluate the technical feasibility of ENDOSCOPIC TRANSANAL PROCTECTOMY, with a particular focus on postoperative and oncological results and on functional outcomes.
• Hybrid technique
ENDOSCOPIC TRANSANAL PROCTECTOMY
• 56 consecutive patients (41 M/ 15 F) Feb 2010 to Jun 2012. • Median age was 65 years (39–83), median BMI was 27 (20-42). • No intraoperative complications; no postoperative mortality,• Postoperative morbidity rate was 26%. • Pathologic examination:
- intact mesorectum( 84%) or almost intact(16%).- median number of lymph nodes retrieved was 12 - median margins: CRM 8 mm (0–20), distal 10 mm (3–40),- R0 resection was achieved in 94.6%).
• Function: (28%)patients reported stool fragmentation and difficult evacuation.
CONCLUSIONS
• ENDOSCOPIC TRANSANAL PROCTECTOMY is feasible for rectal resection and may represent a step toward rectal natural orifice transluminal endoscopic surgery (NOTES).
ROBOTIC RESECTION OF RECTAL CANCER
• 217 patients; April 2006 to August 2011
• Rectal cancer with stage I–III disease
• Prospectively assigned to surgery either with robot ( n = 133) or laparoscopy ( n = 84).
• Median follow-up 58 months ( 4–80 )
• Evaluated for early outcome, morbidity,
5-y survival, prognostic factors, cost
ROBOTIC RESECTION OF RECTAL CANCER Results:
• Early outcome: no significant differences except higher conversion rate and longer hospital stay for robot.
• 5-year OS: 92.8% (robot), and 93.5% (laparoscopic) (ns)• The 5-year DFS 81.9% (robot)and 78.7%, (laparoscopic).• Local recurrence rates: 2.3% and 1.2% • Surgical approach was not a prognostic factor for long-
term survival. • The patient’s• Mean cost for patient was more than double for robotic
surgery
ROBOTIC RESECTION OF RECTAL CANCERConclusions
Robotic surgery for rectal cancer failed to offer any oncologic or clinical benefits as compared with laparoscopy despite at higher cost
LAPAROSCOPIC, TRANSANAL,ROBOTIC… RESECTION OF RECTAL CANCER
DO NOT FORGET
• TOTAL MESORECTUM EXCISION IS THE STANDARD
• THIS IS DIFFICULT SURGERY
• THE AIM IS TO CURE CANCER WITH ACCEPTABLE FUNCTION
Neil HowiePatient Advocate
Charity Runner Neil
”The patient’s perspective”
View of an Advocate Representative
12th ESO Colorectal Cancer Observatory:Innovation and care in the next 12 months
April 2014
On FOLOFOX4 asDiagnosed with T3N2aM0 Stage 3 cancer

April 2015
London Marathon

September 2015
Motivation
• Cancer is not JUST about the ACTUAL treatment
• Life goes on after cancer
• Treatment MUST also focus on the motivation to get through it
• Positive reinforcement of a goal/challenge can help– Can come via family / friends / health professionals
Drug guidance - Future
• What are the drugs
– Clear guidance on the differences
– Simplify the options
• E.g. Europacolon new guide “Colorectal Cancer Prevention and Screening: What YOU Need to Know”
– Clear guide on what is being recommended
– And why
Testing - Future
• Testing kits available– Where are they, and do people know
– For all those Over 50
– Plus for those with family history (http://www.knowyourrisk.org.au/)
• More encouragement to Over 50s to use– Through clearer, simple posters
– But related to all cancers to reduce information overload

Follow my challenge:
• https://facebook.com/neil4bc
• http://neil4bc.org.uk
• http://neil4bc.wordpress.org
• Donate via:– http://justgiving.com/neil4bc-rof