Signs & Symptoms of Approaching Death The dying process is variable depending on individual and family characteristics There are predictable physical, physiologic, and emotional changes During this important phase, the nurse serves as a consultant, collaborator, coach, or guide to assist the patient to achieve symptom relief Knowing what to expect is vital The dying process is variable depending on individual and family characteristics but there are predictable physical, physiologic and emotional changes that occur during the final days and hours of life. During this important phase of end-of-life care, the nurse serves as a consultant, collaborator, coach or guide to assist the patient to achieve symptom relief. Also the nurse helps the patient and family to prepare for the approaching death. Knowing what to expect is vital for the nurse to meet patient and family needs before, at, and after the death.
Diana J. Wilkie, PhD, RN, FAAN
To the Instructor: This Power Point presentation is a suggested
slide presentation that can be used for lecture.It is made from the
information on Instruction Material/ Content from TNEEL CD-ROM.The
presentation might includes some audio sound and video clips. Click
the red button to play the sound or video if any. For some sets of
slides, there will be suggestions and detail descriptions
throughout this Power Point presentation in the Notes Page.These
notes are for instructors use only, and are not intended for
distribution to the students. Thank you for using TNEEL.We welcome
any suggestions. Diana J. Wilkie, PhD, RN, FAAN Signs &
Symptoms of Approaching Death
The dying process is variable depending on individual and family
characteristics There are predictable physical, physiologic, and
emotional changes During this important phase, the nurse serves as
a consultant, collaborator, coach, or guide to assist the patient
to achieve symptom relief Knowing what to expect is vital The dying
process is variable depending on individual and family
characteristics but there are predictable physical, physiologic and
emotional changes that occur during the final days and hours of
life. During this important phase of end-of-life care, the nurse
serves as a consultant, collaborator, coach or guide to assist the
patient to achieve symptom relief. Also the nurse helps the patient
and family to prepare for the approaching death. Knowing what to
expect is vital for the nurse to meet patient and family needs
before, at, and after the death. 1 Cardiovascular disease 2 Cancer
3 Cerebrovacular diseases
Causes of Death The three leading causes of death in adult
Americans: 1 Cardiovascular disease 2Cancer 3Cerebrovacular
diseases The three leading causes of death in adult Americans
continue to be cardiovascular disease, cancer, and cerebrovascular
disease. Signs & Symptoms of Imminent Death
System Circulatory Pulmonary Etiology of Failure Myocardial
infarction, arrhythmias, blood loss Pneumonia, thromboembolism,
pleural effusion, pulmonary edema, pulmonary or tracheal
obstruction, depression of medullary respiratory centers Signs
Reduced tissue perfusion (decreasing blood pressure, tachycardia,
irregular pulse, reduced mentation, cooling and cyanosis of the
extremeties, reduced urinary output, pulmonary and peripheral
edema) Hypoxia with hypercapnia (slowed mentation, confusion,
restlessness, coma) Orthopnea, irregular or rapid breathing,
tachycardia, use of accessory muscles to breathe, excessive
secretions Symptoms Chest pain, dyspnea Apprehension, dyspnea,
cough, fear of choking or drowning Irreversible failure of body
systems leads to death but the cause of death is always
cardiopulmonary failure. Death occurs when the heart or the lungs
fail to perfuse and oxygenate vital tissues. Circulatory failure or
pulmonary failure precedes death. This table lists the best
indicators of imminent death, which are the signs or symptoms of
cardiovascular and respiratory failure. Physical, Physiological
& Emotional
Anticipating the changes and symptoms and preparing the patient and
family to expect and deal with them decrease the uncertainty that
often plagues this time of life Death In the final days and hours
before death, a number of signs and symptoms occur in a predictable
pattern. Changes in daily habits and bodily functions and decline
in functional status are observable and often distressing to the
patient and family. Anticipating the changes and symptoms and
preparing the patient and family to expect and deal with them
decrease the uncertainty that often plagues this time of life.
Eating A few people continue their dietary habits until they die.
The typical dying person, however, stops eating all but a few bites
of favorite foods. Family members often attempt to force the person
to eat, creating conflict and turmoil. An important role for the
nurse is to help the family to recognize that the disease results
in swallowing difficulties, food digestion problems, or lack of
energy or desire to eat. Instead of focusing feeding the dying
person, the family can focus on providing comfort give ice chips,
frequent sips of fluids, cleanse the mouth and moisten lips.These
comfort care actions can replace the giving of food when the dying
person refuses food or is unable to eat. Drinking and hydration -
The typical dying person also stops drinking all but a few sips of
water or a favorite beverage. Thirst is not usually a problem, but
a dry mouth is extremely uncomfortable. Oliguria Renal failure is a
common sign of impending death. Low urinary output less than 30
cc/day or concentrated urine is a sign of renal shutdown.
Incontinence may also occur. Difficulty breathing Dyspnea,
productive cough, and rattling breathing are examples of changes in
breathing that predict the last days of life. Cooling and cyanosis
of extremities Circulatory collapse is indicated by cooling of the
extremities and subsequently by cyanosis.The usual pattern is for
the feet to be cold and to have a purple-blue mottled
appearance.The cooling and discoloration spreads up the legs and
the hands become cold and cyanotic. Decreased consciousness
Alertness is difficult to maintain as body systems function at less
than optimal.The balance of oxygen and carbon dioxide, both of
which are altered with cardiopulmonary compromise, affects the
level of consciousness. Sleepiness, indifference and possible
disorientation lead to decreased level of consciousness. Other
signs Disorientation, restlessness and changes in vital signs are
other indicators of impending death. Patterns in vital signs that
reflect the imminent death include subnormal temperature; decreased
then increased irregular and then absent pulse rate; decreased and
then absent blood pressure, and increased, irregular and then
decreased with apnea respiratory rates. Less Uncertainty
Anticipating Signs of Approaching Death: The Last 48 Hours
1. Reduced level of consciousness 2. Taking no fluids or only sips
6. Bubbling sounds in throat and chest (death rattle) 3. No urine
output or small amount of very dark urine (anuria or olgiuria) In
the last days and hours before death, the nurse learns to predict
imminent death based on assessments that include astute
observations of the patients physical condition as well as the
behavioral and emotional responses. The signs of approaching death
in the last 48 hours include: Reduced level of consciousness Taking
no fluids or only sips No urine output or small amount of very dark
urine (anuria or olgiuria) Progressing coldness and purple
discoloration in legs and arms Laborious breathing; periods of no
breath (Cheyne-Stokes breathing) Bubbling sounds in throat and
chest (death rattle). 5. Progressing coldness and purple
discoloration in legs and arms 4. Progressing coldness and purple
discoloration in legs and arms (Blues & Zerwekh, 1984) Uncommon
Uncontrollable Events Prior to Death
Uncontrollable pain (when thepain was controlled prior to death)
Human Senses: Pain Fatal Hemorrhage Seizures Fatal Seizure The
uncommon but distressing events prior to death include
Uncontrollable Pain when the pain was well controlled prior to
death Fatal hemorrhage Seizures Dying Persons Bill of Rights
I have the right to be treated as a living human being until I die.
I have the right to maintain a sense of hopefulness, however,
changing its focus may be. I have the right to be cared for by
those who can maintain a sense of hopefulness, however challenging
this might be. I have the right to express my feelings and emotions
about my approaching death, in my own way. The Dying Persons Bill
of Rights inlcude: I have the right to be treated as a living human
being until I die. I have the right to maintain a sense of
hopefulness, however, changing its focus may be. I have the right
to be cared for by those who can maintain a sense of hopefulness,
however challenging this might be. I have the right to express my
feelings and emotions about my approaching death,in my own way. I
have the right to participate in decisions concerning my care. I
have a right to expect continuing medical and nursing attention
even though cure goals must be changed to comfort goals. I have the
right to participate in decisions concerning my care. I have a
right to expect continuing medical and nursing attention even
though cure goals must be changed to comfort goals. Dying Persons
Bill of Rights II
I have a right not to die alone. I have a right to be free from
pain. I have a right to have help from and for my family accepting
my death. I have the right to die in peace and dignity. I have the
right to retain my individuality and not be judged for my
decisions, which may be contrary to the beliefs of others. I have
the right to discuss and enlarge my religious and/or spiritual
experiences regardless of what they may mean to others. I have the
right to expect that the sanctity of the human body will be
respected after death. I have a right not to die alone. I have a
right to be free from pain. I have a right to have my questions
answered honestly. I have a right not to be deceived. I have a
right to have help from and for my family accepting my death. I
have the right to die in peace and dignity. I have the right to
retain my individuality and not be judged for my decisions, which
may be contrary to the beliefs of others. I have the right to
discuss and enlarge my religious and/or spiritual experiences
regardless of what they may mean to others. I have the right to
expect that the sanctity of the human body will be respected after
death. I have a right to be cared for by caring, sensitive,
knowledgeable people who will attempt to understand my needs and
will be able to gain some satisfaction in helping me face my death.
I have a right to be cared for by caring, sensitive, knowledgeable
people who will attempt to understand my needs and will be able to
gain some satisfaction in helping me face my death. Signs of Death
Cessation of heart beat and respiration
Pupils fixed and dilated No response to stimuli Eyelids open
without blinking Decreasing body temperature Jaw relaxed and
slightly open Body color is a waxen pallor The signs of death are
listed in this slide. (Note to instructor: Read the list.) After
Death Care: Various Cultural & Religious Groups
Cultural and religious beliefs and practices are important to
nursing care at the end-of-life and immediately after death The
following tables offer a common rituals and customs for the
following cultural and religious groups: American Indians, African
Americans, Mexican Americans, Catholics, Buddhists and Jews
Cultural and religious beliefs and practices are important to
nursing care at the end-of-life and immediately after death. The
following slides summarize common rituals and customs for several
cultural and religious groups. Death Rituals & Customs
Observed: American Indians
Cultural Group American Indians Ritual or Custom at Time of Death
Ritual or Custom at Time of Death Family may hug, touch, sing, stay
close to the dead person Wailing, shrieking and other outward signs
of grieving many occur, a startling contrast in demeanor compared
to pre death display of positive attitudes Ritual or Custom
Immediately After Death Family may hug, touch, sing, stay close to
the dead person Wailing, shrieking and other outward signs of
grieving many occur, a startling contrast in demeanor compared to
pre death display of positive attitudes Turning or flexing the
body, sweetgrass smoke or other purification Family stays with the
body Some want the body to rest at place of death for 36 hours to
allow the soul to depart.Women may want to prepare and dress the
body Some do not allow the mortuary to prepare the body. The family
wraps the body for burial Some avoid contact with the dead person
and his/her possessions. Others want all possessions including
collected hair and nail clippings Autopsy not desired Hair cutting
may be done as a sign of mourning (Note to instructor: Read the
list.) Death Rituals & Customs Observed: African
Americans
Cultural Group African Americans Ritual or Custom at Time of Death
Ritual or Custom Immediately After Death Family may hug, touch, and
be close to family and friends May get agitated or emotional when
anxious Person may be brought to hospital when death is imminent
Report death to oldest family member, spouse or parent Open and
public emotions expected after death May believe that death at home
brings bad luck Prefer to have body cleaned by professionals
Cremation avoided Organ and blood donations not common (Note to
instructor: Read the list.) Death Rituals & Customs Observed:
Mexican Americans
Cultural Group Mexican Americans Ritual or Custom at Time of Death
Ritual or Custom Immediately After Death Extended family members
obligated to visit dying person Spirit may get lost in hospital and
not return home Prayers at bed of dying person Wailing is
acceptable as a sign of respect Death important spiritual event
Extended family may help prepare body Family says good-bye before
dead person is taken to the morgue Organ donation not accepted
Autopsy must be decided by entire family, usually not accepted
(Note to instructor: Read the list.) Death Rituals & Customs
Observed: Religions
Spiritual or Religious Group Buddhist Catholic Jewish Ritual or
Custom at Time of Death Dying persons state of mind at moment of
death influences rebirth Many diverse rituals including last rite
chanting at bedside, family members remaining with body Cremation
often preferred Pregnant women should avoid funerals Priest, monk
or layperson may carry out traditions Permissible to refuse
treatment that carries risk or would prolong a burdensome life
Euthanasia forbidden Sacrament of the Sick [Extreme Unction]
mandatory Organ or body donation allowed All body parts must be
buried together Body may be ritually washed by members of Ritual
Burial Society Cosmetic restoration or embalming discouraged Burial
as soon as possible; cremation not appropriate Euthanasia
prohibited; autopsy permitted if legally required (Note to
instructor: Read the list.) Dyspnea Dyspnea is defined as:
Difficult or labored breathing From the perspective of the patient:
An unpleasant awareness of breathing,a sense of breathlessness or
sensationof shortness of breath Dyspnea is a subjective experience,
like pain Only the person experiencing it can know exactly what it
feels like Health professionals show a great deal of ambiguity in
the interpretation of dyspnea Dyspnea is defined as difficult or
labored breathing. Dyspnea can be observed to some extent, but it
is a subjective experience, like pain; only the person experiencing
it can know exactly what it feels like. Defined from the
perspective of the patient, dyspnea is an unpleasant awareness of
breathing, a sense of breathlessness or sensation of shortness of
breath.Like pain, this term means different things to different
people, and careful measurement of the symptom is needed. Health
professionals show a great deal of ambiguity in the interpretation
of dyspnea because it is an inadequately defined, multidimensional
symptom. Different professionals focus on some dimensions and
others focus on other aspects of the complex phenomenon. For
example, tachypnea is not dyspnea but some professionals use
tachypnea as an indicator of dyspnea.In the dying person able to
communicate, dyspnea can be defined, measured and treated as a
subjective experience.In the dying person not able to
communicative, the presence of dyspnea is likely to be observable,
but its the magnitude has not be measured with reliable results.
Dyspnea: Mechanisms & Etiology
Dyspnea is a symptom associated with a number of diseases and
conditions Example: Obesity is associated with dyspnea on exertion
Increased ventilatory demand, impaired mechanical responses, and
combinations of the two lead to dyspnea Dyspnea at rest contributes
to social isolation and decreased quality of life The neural
mechanisms of dyspnea are unknown It is known that delta opioid
receptors are present in lung tissues, which may partially explain
the effectiveness of opioids in treatment of dyspnea Dyspnea is a
symptom associated with a number of diseases and conditions (Table
9).For example obesity is associated with dyspnea on exertion.
Increased ventilatory demand, impaired mechanical responses, and
combinations of the two lead to dyspnea. Exertional dyspnea leads
patients with life-threatening illnesses to curtail progressively
their activities often to the point that they cannot even talk
because of dyspnea. Dyspnea at rest is particularly problematic and
contributes to social isolation and decreased quality of life. The
neural mechanisms of dyspnea are unknown but peripheral and central
mechanisms are implicated by the complexity of the sensation.It is
known that delta opioid receptors are present in lung tissues,
which may partially explain the effectiveness of opioids in
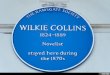
treatment of dyspnea. Prevalence of Dyspnea by Disease
Chronic ObstructivePulmonary Disease (COPD) Congestive Heart
Disease Stroke Amyotropic Lateral Sclerosis Dementia Outpatient
Cancer Terminal Cancer Lung Cancer Prevalence of Dyspnea 95% 61%
37% 47% to 50% 70% 50% 45% to 70% 90% This slide shows the
prevalence of dyspnea in several different diseases, illnesses or
populations. Dyspnea is a common symptom. (Dudgeon, 2001) Dyspnea:
Assessment Visual analogue scales and 0 to 10 number scales
successfully measure the intensity of the dyspnea sensation It is
important to seek intensity ratings with various levels of activity
(pattern of dyspnea) Walking outside, walking up stairs, eating,
talking etc. Verbal descriptors such as chest tightness may prove
useful in the future with additional research Dyspnea associated
with life threatening illness evokes affective responses including:
Panic, frustration, worry, anxiety, anger, and depression Visual
analogue scales and 0 to 10 number scales have been used
successfully to measure the intensity of the dyspnea sensation.
Given the propensity of patients to alter their activities in
response to the magnitude of their dyspnea, it is important to seek
intensity ratings with various levels of activity (pattern of
dyspnea), such as walking outside the house, walking up stairs,
walking in your home or room, eating, or talking. Verbal
descriptors of dyspnea quality such as chest tightness or deep may
prove useful in the future with additional research. Observed use
of accessory muscles has correlated with dyspnea intensity ratings.
Dyspnea associated with life threatening illness evokes affective
responses including panic, frustration, worry, anxiety, anger, and
depression. Dyspnea: Pharmacologic Management
Primary control of dyspnea in people with life threatening illness
includes: Treatment for the underlying etiology of the dyspnea
(when possible), and treatments focused on symptom relief Opioids,
corticosteroids, and anxiolytics have been effective in reducing
dyspnea sensation Morphine treatments for those without pain:
Typically 2.5 mg to 5 mg orally every four hours and a double dose
at bedtime will control dyspnea in most patients Increase based on
patient response Primary control of dyspnea in people with life
threatening illness includes treatment for the underlying etiology
of the dyspnea when possible and treatments focused on symptom
relief. For example, dyspnea related to congestive heart failure
requires medications to reduce cardiac workload and to promote
cardiac function.As well opioids, corticosteroids, and anxiolytics
have been effective in reducing the sensation of dyspnea. Dyspnea
in the person without pain is relieved by small doses of
morphine.Typically 2.5 mg to 5 mg orally every four hours and a
double dose at bedtime will control dyspnea in most patients.
Increasing the dose based on patient response (titration) may be
necessary for some patients.Rarely do patients require doses in
excess of 15 mg to 20 mg orally every four hours to relieve their
dyspnea. Close monitoring is needed when using morphine or other
opioids in people nave to opioids especially those with chronic
lung diseases. Nebulized morphine has been investigated as a
treatment for dyspnea, but research is insufficient to recommend
this treatment at this time. Dyspnea: Pharmacologic Management
II
Corticosteroids such as dexamethasone 8 mg daily also relieve
dyspnea associated with an inflammatory response Superior vena cava
syndrome and pulmonary metastatic lymphadenopathy Chlorpromazine
reduces dyspnea without affecting ventilation or causing sedation
Effective alone or combined with morphine for treatment of dyspnea
in COPD or advanced cancer Scopolamine effectively reduces
secretions and also sedates the patient. The effective dose of
scopolamine is 0.4 mg to 0.6 mg I.M. every four hours, or 2 mg to 4
mg every 24 hours by continuous subcutaneous infusion Transdermal
patches deliver 0.5 mg every 24 hours for a period of 72 hours
Corticosteroids such as dexamethasone 8 mg daily also relieve
dyspnea associated with an inflammatory response.Superior vena cava
syndrome and pulmonary metastatic lymphadenopathy are two examples
of conditions in which corticosteroids are likely to relieve
dyspnea. Chlorpromazine reduces dyspnea without affecting
ventilation or causing sedation.This drug has been effective alone
or combined with morphine for treatment of dyspnea in COPD or
advanced cancer. Dyspnea in dying patients may result from their
difficulty in managing oral secretions as a result of weakness,
immobility, or fluid overload. Scopolamine effectively reduces
secretions and also sedates the patient. The effective dose of
scopolamine is 0.4 mg to 0.6 mg I.M. every four hours, or 2 mg to 4
mg every 24 hours by continuous subcutaneous infusion.A more
manageable method is administration of scopolamine as a transdermal
patch.Each patch delivers 0.5 mg every 24 hours for a period of 72
hours. A therapeutic effect usually is obtained with 3 to 5 patches
used simultaneously. The patch should be changed every 72 hours.
(Schiro, 1992) Dyspnea: Nonpharmacologic Management
Oxygen Increasing air movement A portable fan directed towards
patients face Positions that increase the ventilatory capacity
Improve the function of the diaphragm and accessory muscles Avoid
all activity, including talking Oxygen is a nondrug, medical
treatment that can be effective in relieving dyspnea in some
conditions associated with hypoxia. Dyspnea without hypoxia is may
or may not be improved with oxygen. The goal of oxygen therapy for
dyspnea are to reduce the dyspnea sensation and maintain a PAO2 of
55 to 60 mm Hg and oxygen saturation of 88% to 90%. Use of nasal
cannula for oxygen delivery appears to be more beneficial than an
oxygen mask perhaps because of the sensation of directed airflow
and a perception of less confinement with the nasal cannula.
Similarly, increasing air movement by use of a portable fan
directed near the patients face is an efficient means relieving
dyspnea in some patients. This technique increases the sensation of
air circulation and reduces the sense of suffocation in the person
with dyspnea. Positions that increase the ventilatory capacity by
improving the function of the diaphragm and the accessory muscles
are effective in reducing mild to moderate levels of dyspnea. The
final activity-related way that patients cope with unrelieved
dyspnea is to avoid all activity, including talking. Reducing
activities, however, limits the dying persons ability to meet other
important end-of-life goals.When dyspnea is so severe that
breathing and talking cannot be done at the same time, the persons
quality of life is very compromised. Patients with dyspnea tend to
breathe inefficiently and in doing so to consume more energy than
necessary. They take short, shallow, gasping breaths and use
accessory muscles rather than the diaphragm muscle to facilitate
inhalation and exhalation. Teaching patients how to take slow, deep
breaths using the diaphragm and to exhale slowly through pursed
lips helps them to overcome inefficient breathing, which improves
their oxygenation and reduces dyspnea. Slow exhalation means that
exhaling should take twice as long as inhaling. Use of the
diaphragm and pursed-lips to breath provides several benefits, such
as reducing respiratory rate, increasing tidal volume, and
increasing functional residual capacity. Teach the patient to place
his/her fingers just below the sternum, to sniff, and to feel the
diaphragm muscle move. Alternatively, ask the patient to recline
supine with knees bent, to place a book over his/her abdomen, and
to inhale. The book moves upward allowing the patient to see the
effect of the diaphragm descending, which forces expansion of the
abdominal muscles. Inhaling sufficiently to raise the additional
weight of the book also helps to strengthen the diaphragm muscle.
The patient should practice this procedure using pursed-lip
breathing. Fatigue and Weakness (Asthenia)
Fatigue is a common symptomexperienced by people with lifelimiting
illness As illnesses progress, fatigue causespeople to curtail
first the pleasurableand leisure activities and then
otheractivities of daily living The dying person may not have
sufficient strength or energy to flush a toilet The impact of these
activity restrictions compromises the persons quality of life
Fatigue is a common symptom experienced by people with life
limiting illness. As illnesses progress, fatigue causes people to
curtail first the pleasurable and leisure activities and then other
activities of daily living. As the end of life approaches, the
dying person may not have sufficient strength or energy to flush a
toilet. The impact of these activity restrictions compromises the
persons quality of life. (Dean & Anderson, 2001) Prevalence of
Fatigue by Disease
Coronary ArteryDisease Cancer Renal Hemodialysis General Palliative
Care AIDS Children with Cancer Prevalence of Fatigue 41% to 77% 60%
to 99% 72% 51% 50% This slide shows the prevalence of fatigue in
many different conditions and populations. (Dean, 2001) Fatigue:
Mechanisms & Etiology
Fatigue is conceptualized as a multifaceted symptom with
physiological, sensory, affective, cognitive, and behavioral
components Several theories have been proposed to explain the
fatigue associated with various illnesses Unknown: Whether the
mechanisms are similar or different by disease Some evidence that
is inconclusive, includes: Accumulation of lactate or cytokines,
anemia with depletion of red blood cells or hemoglobin, or neural
mechanisms The mechanisms of fatigue have been postulated but are
not clearly understood. Fatigue is conceptualized as a multifaceted
symptom with physiological, sensory, affective, cognitive and
behavioral components. Several theories have been proposed to
explain the fatigue associated with various illnesses. Whether the
mechanisms are similar or different by disease is not
known.Accumulation of lactate or cytokines, anemia with depletion
of red blood cells or hemoglobin, or neural mechanisms are
contending postulates that are substantiated by some but not
conclusive evidence. Fatigue: Assessment Many assessment tools to
measure fatigue
Some are multidimensional, comprehensive measures of fatigue
Screening tools such as the Schwartz Cancer Fatigue Scale As with
pain, fatigue assessments that focus only on the intensity of the
fatigue provide limited perspective Assessing the following are
critical: Location (parts of body sensed as fatigued), intensity (0
to 10 scale or other intensity scale), quality (how the fatigue
feels), and pattern (onset, duration, aggravating factors,
alleviating factors) Additional data about the patients history,
physical exam, or laboratory findings Many assessment tools have
been used to measure fatigue. Some of these tools are
multidimensional, comprehensive measures of fatigue.Other tools are
screening tools such as the Schwartz Cancer Fatigue Scale. As with
pain, fatigue assessments that focus only on the intensity of the
fatigue provide limited perspective on the fatigue experience and
are insufficient to guide interventions.Assessing the location
(parts of body sensed as fatigued), intensity (0 to 10 scale or
other intensity scale), quality (how the fatigue feels), pattern
(onset, duration, aggravating factors, alleviating factors) are
critical parameters. Additional data about the patients history,
physical exam, or laboratory findings may provide additional
insight into the etiology of fatigue in the dying person.Assessing
fatigue in caregivers is also important. Schwartz Cancer Fatigue
Scale: A 6-Item Screening Tool for Fatigue
SCFS-6 1 = not at all 2 = a little 3 = moderately 4 = quite a bit 5
= extremely The words and phrases below describe different feelings
people associate with fatigue.Please read each item and circle the
number that indicates how much fatigue has made you feel in the
past 2 to 3 days. Tired Difficulty thinking Overcome Listless .
Worn out Helpless The Schwartz Cancer Fatigue Scale (SCFS): A
6-Item Screening Tool for Fatigue. (1997 A. L. Schwartz) Fatigue:
Pharmacologic Management
Virtually no information is available regarding pharmacologic
management of fatigue Exception: People with chronic renal failure
or cancer In these two populations, fatigue has been reduced by the
epoetin, which stimulated red blood cell production Pharmacologic
management of fatigue is an understudied area and virtually
nonexistent related to end-of-life care Virtually no information is
available regarding pharmacologic management of fatigue except in
people with chronic renal failure or cancer in which epoetin was
used to stimulate red blood cell production.In these two
populations, fatigue has been reduced by the epoetin. In one small
study, methylphenidate reduced fatigue in people experiencing mild
levels of opioid induced sedation. Similar findings have been noted
by other investigators. Many experts advocate use of pharmacologic
agents to relieve other symptoms that can contribute to fatigue.
Pharmacologic management of fatigue is an understudied area and
virtually nonexistent related to end-of-life care. (Littlewood,
2001) Fatigue: Nonpharmacologic Management
Many interventions are suggested to alleviate fatigue, but with
theexception of exercise, none havebeen tested Exercise, in most
cases, is a neglected area of the treatment plan for people facing
the end-of-life transition Health care providers often fail to
advise patients about exercise and the benefits that can be gained
from it Inactivity may in fact be the trigger for marked fatigue
and weakness experienced by patients Many interventions are
suggested to alleviate fatigue, but with the exception of exercise,
none have been tested. Exercise, in most cases, is a neglected area
of the treatment plan for people facing the end-of-life transition.
Health care providers often fail to advise patients about exercise
and the benefits that can be gained from it. Inactivity may in fact
be the trigger for marked fatigue and weakness experienced by
patients. Fatigue: Nonpharmacologic Management II
Aerobic exercise may prevent reduced functional capacity, nausea,
fatigue, decreased self-esteem, and other quality of life issues
that confront cancer patients Balancing energy reserves with energy
expenditures is the goal for the management of fatigue Walking and
other types of low-impact exercise Weight training early in the
illness trajectory to improve muscle tone and function,
particularly in the elderly Distraction techniques may reduce
fatigue Taking car rides, listening to music, praying, meditating,
engaging in hobbies, spending time with family and friends Benefits
of both aerobic and resistance types of exercise are
well-documented in the general population, and a growing body of
evidence suggests that aerobic exercise may prevent reduced
functional capacity, nausea, fatigue, decreased self-esteem, and
other quality of life issues that confront cancer patients. Tests
of structured aerobic exercise programs for previously sedentary
cancer patients demonstrate that exercise is safe; that patients
who are receiving chemotherapy exhibit a training effect; and that
exercise produces positive psychosocial effects. Balancing energy
reserves with energy expenditures is the goal for the management of
fatigue. In the person facing the end-of-life transition, primary
goals are to maintain what the patient can do for as long as
possible and minimize loss. Walking and other types of low-impact
exercise should be maintained as long as possible. Energy
management involves assessing the patients status, deciding which
energy-using activities can and cannot be altered and planning
energy conserving methods to aid the patient. Patients can be
taught to view their energy stores as a bank.Deposits and
withdrawals must be planned.It is important to foresee daily and
weekly activities and to then plan around them in order to ensure
that enough energy will be left for important activities.It may be
necessary to modify or replace activities that require more energy
than available to the patient. An intriguing idea is to use weight
training early in the illness trajectory to improve muscle tone and
function, particularly in the elderly. Fiatarone found that
individuals in their 80s and 90s quickly lost muscle tone with
inactivity and reported exacerbated feelings of fatigue.
Significant benefit on muscle tone, the ability to carry out more
necessary daily activities, feelings of well-being, and decreased
fatigue resulted from a brief period of daily training with very
light weights. Similar results were noted in residents of nursing
homes. Distraction techniques may reduce fatigue. Taking car rides,
listening to tapes or soft music, praying, meditating, engaging in
hobbies, spending time with family and friends are examples of
distraction activities that divert the persons attention and some
include activities that allow some level of exercise. Prevalence of
Constipation
Population Group Adults with Cancer Diabetes Children with Cancer
Older Adults Children General Population Prevalence of Constipation
78% 10% to 17% 6 to 50% 72% 11% 10 to 28% Constipation is
frequently experienced by many patient groups as indicated in this
slide. (Collins, 2000) Constipation: Mechanisms &
Etiology
Constipation is a problem for many peoplewith life-limiting illness
There are many causes of constipation: Mechanical, metabolic and
neural processesassociated with the life threatening disease
Dietary alterations Immobility Drug therapy side effects and
combinations of these factors are the typical etiologies of
constipation at end of life Its prevention is easier and more
desirable to all involved than treatment after it occurs
Constipation is a problem for many people with life-limiting
illness. There are many causes of constipation in persons facing
the end of life transition. Mechanical, metabolic and neural
processes associated with the life threatening disease, dietary
alterations, immobility, drug therapy side effects and combinations
of these factors are the typical etiologies of constipation at end
of life. Constipation is one of the most distressing symptoms
experienced by dying people and their families and its prevention
is easier and more desirable to all involved than treatment after
it occurs. Constipation: Assessment
McMillan and colleagues developed and tested a simple 8-item tool
to measure self-reported constipation Establishing the persons
normal pattern prior to the illness is also important to judge the
degree to which current bowel patterns are altered Bowel functions
are variable from person to person Establishing the baseline
pattern for the person with life-limiting illness is a critical
assessment not documented by the Constipation Assessment Scale
Documentation of other history and physical exam data is essential
McMillan and colleagues developed and tested a simple 8-item tool
to measure self-reported constipation. Establishing the persons
normal pattern prior to the illness is also important to judge the
degree to which current bowel patterns are altered.Since normal
bowel function is variable from person to person, establishing the
baseline pattern for the person with life-limiting illness is a
critical assessment not documented by the Constipation Assessment
Scale. Documentation of other history and physical exam data is
essential to high quality nursing care at the end of life.
(McMillan & Williams, 1989) Constipation Assessment Scale
Directions: Circle the appropriate number to indicate whether
during the past three days you have had NO PROBLEM, SOME PROBLEM or
a SEVERE PROBLEM with each of the items listed Item 1. Abdominal
distention or bloating 2. Change in amount of gas passed rectally
3. Less frequent bowel movements 4. Oozing liquid stool 5. Rectal
fullness or pressure 6. Rectal pain withbowel movement 7. Smaller
stool size 8. Urge but inability to pass stool noproblem
someproblem 1 severeproblem 2 The Constipation Assessment Scale is
very easy to use as indicated by the items listed on this slide. A
score of * indicates treatment is needed. Patient history and
physical exam data also helps the health professional to diagnose
and treat the constipation symptom. Patient History Data Last bowel
movement (when, how much, appearance, odor) Abdominal tenderness,
cramping, pressure, pain Unexplained nausea or early satiety
Medications (opioids, calcium channel blockers) Dietary and fluid
intake Activity status Physical Exam Findings (possible meaning)
Abdominal distension, bulges (ascites, gas, tumor or stool) Tympany
on percussion (partial obstruction) Hemorrhoids, ulcerations,
rectal fissures, impaction Bowel sounds:Absent for minimum of 5
minutes (paralytic ileus) Hyperactive (partial obstruction or
diarrhea) Hypokalemia, hypercalcemia present Signs of spinal cord
compression (McMillan & Williams, 1989) Constipation:
Pharmacologic Management
Vigilance is required to prevent constipation The cornerstone of
treatment: Anticipating that constipation will occur in people if
dietary and fluid intake is altered Prevention of constipation
requires the expectation that constipation will be a side effect of
all opioids and many of the adjuvant analgesics Patients should
expect a bowel movement no less than every three days regardless of
intake and activity level Vigilance is required to prevent
constipation. Anticipating that constipation will occur in people
who have altered their dietary and fluid intake or activity because
of advancing disease, is the cornerstone of treatment. Prevention
of constipation requires the expectation that constipation will be
a side effect of all opioids and many of the adjuvant analgesics.
With this expectation instituting prophylactic management of
constipation allows the symptom to be treated before it becomes
distressing to the patient and family. Patients should expect a
bowel movement no less than every three days regardless of intake
and activity level. Constipation: Two Rules for Management
1.Anticipate and prevent constipation 2. Reverse specific cause of
constipation with specific therapy There are two Rules for
Management of Constipation 1. .Anticipate and prevent constipation.
2. Reverse specific cause of constipation with specific therapy.
Constipation: Commonly Effective Pharmacologic Agents
Comments 1 tab reverses constipating effectof Morphine 15 mg po or
120 mgCodeine po.Activated in largeintestine by bacterial
degradation,stimulates submucosal nerveplexus and reduces sodium
andwater absorption Strong stimulation effects withcramping,
urgency, incontinence Liver and colon metabolism; effectdifficult
to predict and control. Generic Drug (Trade Drug) [Alternate Form]
Senna (Senokot) [Senokot-S with docusate (Colace)] Casanthranol
with docusate(Peri-Colace) Bisacodyl (Dulcolax) Lactulose
(Chronulac) Phenolphthalein withdocusate (Doxidan) TypicalDose 1-8
(max 10)tabs pobased onopioid doseandresponse 1-4 tabs po mg po
10-15 mg pr 15-30 ml po 1-4 tabs po Onset ofEffect 6-12 hr 6 hr
15-60 min 1-3 hr Treatment of constipation in people with
life-limiting illness usually requires use of a laxative with
stimulant action and perhaps a stool softener.A stool softener
alone is insufficient for people requiring opioid analgesics; they
require a stimulant in order to overcome the actions of the opioid
on the gastrointestinal tract.It is common for patients to be
prescribed only stool softeners and for their providers to not
understand why constipation is a problem. Large-bowel stimulant
laxatives and osmotic laxatives are often effective treatments for
constipation in people taking multiple drugs for symptom control at
end of life. This slide lists treatment plans designed to prevent
constipation as well as to restore usual bowel function.
Constipation: Treatment Plan to Restore Bowel Function
Start with senna (Senokot, fruit paste), Peri-Colace or Doxidan If
bowel movement does not occur within 24 hours, increase doses to
BID or TID administration until maximum dose is reached If no bowel
movement within 48 hours, add bisacodyl 2-3 tabs po HS to TID or
Milk of Magnesia with cascara 30 cc po HS If no bowel movement
within 72 hours and no rectal impaction, use water or oil retention
enema or a bisacodyl suppository If disimpaction is needed,
premedicate with an oil retention enema, an analgesic and a
sedative Follow with a cleansing enema and an appropriate
constipation-prevention plan This slide show one effective
treatment plan that restores bowel function in people experiencing
opioid-induced constipation. Read the slide content. (Levy, 1991)
Constipation: Nonpharmacologic Management
If the patient is able to increase fluid intake or activity levels,
there are effective nonpharmacologic treatments for constipation
Increasing fluids to 1 to 1.5 liters per day and dietary fiber
intake are recommended, but often not achievable goals as disease
progression limits the persons intake and activity If a patient is
not able to maintain adequate fluid intake, bulk laxatives may
cause severe constipation or obstruction and are contraindicated
Hospice nurses speak highly of this treatment plan: Using natural
senna a part of the dietary intake (not supported by research) If
the patient is able to increase fluid intake or activity levels,
they are effective nonpharmacologic treatments for constipation.
Increasing fluids to 1 to 1.5 liters per day and dietary fiber
intake are recommended, but often not achievable goals as disease
progression limits the persons intake and activity. If a patient is
not able to maintain adequate fluid intake, bulk laxatives may
cause severe constipation or obstruction and are contraindicated.
Constipation: Anti-constipation Recipe
Yakima Valley Anti-Constipation Fruit Paste Dionetta Hudzinski,
Hospice of Yakima 2 cups boiling water 3-4 oz senna tea leaves 1 lb
pitted prunes 1 lb raisins Prepare tea: Add tea leaves to the
boiling water and let steep for 5 minutes.Strain and remove tea
leaves. Add fruit:Place 2 cups of tea in a large put.Add all the
fruit to the tea.Boil fruit and tea for 5-10 minutes.Remove from
heat. Add sugar and lemon juice and allow to cool. Use a hand mixer
or food processor to turn fruit and tea mixture into a paste. Place
in freezer containers and store in freezer.Paste will not freeze.
Serving Ideas: spread on toast, eat straight from the spoon, mix
with hot water, use asfruit topping on cereal. 1 lb pitted figs 1
cup brown sugar 1 cup lemon juice Although not supported by
research, this slide shows a treatment plan to prevent constipation
by using natural senna a part of the dietary intake of the person
facing the end-of-life transition.Hospice nurses speak highly of
this treatment plan. Patients often have their own remedies for
constipation. If they are effective, they should be encouraged to
use them unless there are contraindications. For example, Gypsy had
always treated her constipation with sauerkraut juice.A small can,
4-6 ounces, once or twice per week was the only laxative she
required until her death from lung cancer.She favored the taste and
found it very effective in preventing constipation.Other patients
have reported similar opinions. Adapted from WSCPI News, Spring,
1993, p. 10. Used with permission of Dionetta Hudzinski, MN, RN.
Multiple Symptoms Successful treatment of symptoms requires
collaboration of the patient, family, nurses, physicians, social
workers, spiritual guide and other care providers In review of
1,000 patients, 50% experienced 11 or more symptoms with the number
of symptoms experienced ranging from 1 to 27 Pain, fatigue,
weakness, anorexia, lack of energy, dry mouth, constipation, early
satiety, dyspnea, and greater than 10% weight loss were the 10 most
prevalent symptoms Successful treatment of symptoms experienced by
the person facing the end-of-life transition requires collaboration
of the patient, family, nurses, physicians, social workers,
spiritual guide and other care providers. Symptom management is a
complex process requiring ongoing attention and diligence to
promote comfort. Patients experience not just one symptom at end of
life, but many symptoms. Walsh and colleagues found in review of
1,000 patients that 50% experienced 11 or more symptoms with the
number of symptoms experienced ranging from 1 to 27. In this study,
they found pain, easy fatigue, weakness, anorexia, lack of energy,
dry mouth, constipation, early satiety, dyspnea, and greater than
10% weight loss were the 10 most prevalent symptoms. (Walsh, 2000)
(Collins, 2000; Ng, 1998; Oliver, 1996; Wolfe, 2000)
Multiple Symptoms Other investigators note similar that not all
symptoms are relieved to the satisfaction of the adult or child
patient and the family Appropriate symptom management depends on
the patient and the family working in partnership with the health
care provider team The collaboration includes the patient and
family and requires intradisciplinary and interdisciplinary efforts
to understand the patients symptoms and to find successful
treatments Other investigators have noted similar findings and that
not all symptoms are relieved to the satisfaction of the adult or
child patient and the family. Appropriate symptom management
depends on the patient and the family working in partnership with
the health care provider members of the team.Together the patient
and family centered team participates in ongoing assessment
directed at finding effective treatments for all the patients
symptoms. The collaboration includes the patient and family and
requires intradisciplinary and interdisciplinary efforts to
understand the patients symptoms and to find treatments that will
successfully relieve the symptoms. Ongoing assessment is
facilitated by use of standardized tools to measure symptoms. The
Symptom Distress Scale is an excellent tool that allows measurement
of multiple symptoms (Table 18).This tool has been translated into
several languages.Data from this tool allows the health care
professionals to implement therapies targeted at symptom relief.
Since multiple symptoms are commonly experienced by the person with
a life-limiting illness, it is usual for multiple therapies to be
needed. Careful attention to mechanisms of action and interactions
is needed to prevent unnecessary toxicity from treatments. Often
one therapy will produce an unpleasant side effect that requires
another therapy for adequate relief. Effective symptom management
requires the health professional team to have a strong commitment
to total symptom relief, knowledge about therapy effects and side
effects, and several types of skills. (Collins, 2000; Ng, 1998;
Oliver, 1996; Wolfe, 2000) Multiple Symptoms: Necessary
Skills
Assessment of single and multiple symptoms using standardized
scales, interview history- taking, and physical exam techniques
Management of pharmacologic and nonpharmacologic therapies
Recognition and management of treatment-induced side effects
Advocacy for patient-family-centered and collaborative care at end
of life Patient and family education for them to fulfill their
partnership roles Symptom management requires skills in Assessment
of single and multiple symptoms using standardized scales,
interview history- taking, and physical exam techniques. Management
of pharmacologic and nonpharmacologic therapies. Recognition and
management of treatment-induced side effects. Advocacy for
patient-family-centered and collaborative care at end of life.
Patient and family education for them to fulfill their partnership
roles. Successful implementation of theses skills in roles that fit
comfortably for the patient and family as well as the health care
professional produces comfort at end of life that is acceptable to
the patient, supportive of the family needs and desires, and
professionally satisfying. Gypsy (Case section) is one example of
successful symptom management that allowed a respectful death.She
said, How can I be dying, I feel so good? Being part of a team that
provides this type of care is a most satisfying professional
experience for many nurses who have devoted themselves to caring
for people facing the end-of-life transition. It is a privilege to
use professional knowledge and skills to promote comfort in dying
people and their families.