Embed Size (px)
Citation preview
ORIGINAL RESEARCH
Diagnostic Performance of Vertebral Fracture Assessmentby the Lunar iDXA Scanner Compared to ConventionalRadiography
Daniele Diacinti • Romano Del Fiacco • Daniela Pisani • Federico Todde •
Maria Sofia Cattaruzza • Davide Diacinti • Serena Arima • Elisabetta Romagnoli •
Jessica Pepe • Cristiana Cipriani • Salvatore Minisola
Received: 18 May 2012 / Accepted: 31 July 2012 / Published online: 11 September 2012
� Springer Science+Business Media, LLC 2012
Abstract The purpose of this study was to evaluate the
diagnostic performance of vertebral fracture assessment
(VFA) using the Lunar iDXA scanner. Conventional spinal
radiographs and images acquired by dual-energy X-ray
absorptiometry (DXA) of 350 subjects (269 females, 81
males) were evaluated by two different readers. We visualized
4,476/4,550 (98.4 %) vertebrae from T4 to L4 on VFA images
compared to 4,535/4,550 (99.7 %) on radiographs. Among the
visualized vertebrae, 205/4,535 (4.5 %) and 190/4,476 (4.2 %)
were identified as nonfracture deformities by reading of
radiographs and VFA, respectively. Vertebral fractures (VFs)
were 231 in 126 patients and 228 in 125 patients by semi-
quantitative assessment of radiographs (SQ-Rx) and by VFA,
respectively. There was excellent agreement between the two
techniques and high diagnostic performance of VFA both on a
per-vertebra basis (k score = 0.984, 95 % CI 0.972–0.996,
sensitivity 98.68 %, specificity 99.91 %, PPV 98.25 %, NPV
99.93 %) and on a per-patient basis (k score = 0.957, 95 % CI
0.925–0.988, sensitivity 96.83 %, specificity 98.66 %, PPV
97.60 %, NPV 98.22 %). In older patients (C65 years) affected
by moderate or severe osteoarthritis, SQ-Rx and VFA iden-
tified 96 VFs and 95 versus 90 vertebral deformities, respec-
tively. This study demonstrates that most vertebrae are
evaluable using the iDXA scanner, with improved VFA
diagnostic performance even in discriminating mild VFs from
vertebral deformities. Therefore, VFA may be appropriate as
an alternative to conventional radiography in patients at high
risk of VF who are undergoing DXA bone densitometry and in
the follow-up of osteoporotic patients on treatment.
Keywords Dual-energy X-ray absorptiometry � Vertebral
fracture assessment � Vertebral fracture � Semiquantitative
assessment � Conventional radiography
Vertebral fractures (VFs) are the most common osteopo-
rosis-related fractures [1, 2], but many of these remain
unrecognized by clinicians and, therefore, undiagnosed
[3, 4] as they often are asymptomatic and occur in the
absence of specific trauma. The identification of VF has a
high predictive value, and it is important for the manage-
ment of osteoporotic patients because even with a mild
VF patients have approximately fivefold increased risk
of further VF and threefold increased risk of hip fracture
[5–7]. Multiple VFs are associated with an increased
mortality rate [8] and reduced quality of life [9].
The visual semiquantitative assessment of conventional
radiographs (SQ-Rx) described by Genant et al. [10] is one
of the most widely used methods to assess VF since it
achieves a high accuracy for diagnosing VF by an expert
The authors have stated that they have no conflict of interest.
D. Diacinti � D. Diacinti
Department of Radiology, Sapienza University of Rome,
Viale del Policlinico 155, 00161 Rome, RM, Italy
R. Del Fiacco � S. Arima � E. Romagnoli � J. Pepe �C. Cipriani � S. Minisola
Department of Clinical Sciences, Sapienza University of Rome,
Viale del Policlinico 155, 00161 Rome, RM, Italy
D. Pisani (&) � F. Todde
Department of Clinical and Molecular Medicine,
Sant’ Andrea Hospital, Sapienza University of Rome,
Via Grottarossa 1035-1039, 00189 Rome, RM, Italy
e-mail: [email protected]
M. S. Cattaruzza
Department of Public Health and Infectious Diseases,
Sapienza University of Rome, P.le Aldo Moro5,
00185 Rome, RM, Italy
123
Calcif Tissue Int (2012) 91:335–342
DOI 10.1007/s00223-012-9643-0
reader, allowing one also to distinguish between true VFs
and vertebral deformities [11]. Because of the high radia-
tion effective dose (about 600 lSv), lateral radiographs of
the thoracic and lumbar spine are used only in patients with
back pain so that most VFs, which are asymptomatic, are
often undiagnosed in clinical practice [12].
In the last decade, new developments in dual-energy
X-ray absorptiometry (DXA) scanners (fan X-ray-beam
system with pile of detectors) have provided a means to
acquire lateral images of the thoracic–lumbar spine of good
quality to detect prevalent VF [13–15].
DXA offers several advantages over conventional radi-
ography, which include a significantly lower radiation
effective dose to the patient (from 2 to about 50 lSv) [16],
lack of distortion from parallax and magnification of the
image, and quick acquisition of a single image of the
thoracic and lumbar spine in the same session as bone
mineral density measurement, lowering costs [17].
The 2007 International Society of Clinical Densitometry
(ISCD) official positions [18] stated that vertebral fracture
assessment (VFA) is the correct term to denote densitometric
spine imaging performed for the purpose of detecting VFs.
Furthermore, recommendations were provided concerning
proper indications for VFA and appropriate methods for
defining and reporting fractures on VFA. The Genant visual
semiquantitative method was indicated as the current clinical
technique of choice for diagnosing VF with VFA. In spite of
this authoritative recommendation, VFA has not yet been
widely implemented in clinical practice because up to now
available DXA devices have had low spatial resolution
(1 mm per line pair) [19].
In comparative studies with conventional radiographs
for the detection of VFs, many vertebrae (10–15 %) could
not be visualized on lateral spine DXA images, mainly at
the upper thoracic level from T4 to T7, because of the poor
image quality of the available densitometers [20].
In fact, these studies demonstrated good specificity of
VFA varying from 94 to 99 % but low sensitivity ranging
from 62 to 85 %. The variability of these results arose both
from the model of densitometers used, Hologic 4500A or
Delphi C (Hologic, Bedford, MA) [21–23] and Lunar
EXPERT-XL [24] and Lunar Prodigy [25–27] (GE Medical
Systems Lunar, Madison, WI), and from characteristics of
the studied populations.
GE Healthcare has recently developed the Lunar intel-
ligent DXA (iDXA), a fan-beam densitometer that uses
slightly higher amounts of radiation and enhanced detector
capabilities, the latter yielding improved spatial resolution
up to 0.3 mm per line pair [28].
The purpose of this study was to evaluate the reliability
and diagnostic performance of VFA in the identification of
VFs using the iDXA scanner in comparison with conven-
tional radiography.
Methods
Subjects
We enrolled 350 patients (269 females and 81 males; mean age
± SD 60.6 ± 11.6 years, range 28–85) consecutively referred to
our Mineral Metabolism Centre. They were recruited from two
sources: peri- and postmenopausal women and men referred by
general practitioner for diagnosis of osteoporosis and patients
from a study of HIV-related osteoporosis.
All patients gave written, informed consent. The study
was approved by the local ethics committee. No patients
were excluded for any health reasons (including previously
diagnosed VFs).
VFA
Lateral images of the thoracic–lumbar spine were acquired
using a Lunar-iDXA densitometer (GE Medical Systems
Lunar). This device uses a stable X-ray source with a current
of 2.5 mA and a peak X-ray energy of 100 kVp that is filtered
by a K-edge filter at 46 keV for low energy and 81 keV for
high energy. The Lunar-iDXA uses a narrow-angle (4.5�) fan
beam oriented orthogonal to the long axis of the body. The
limited-angle fan beam avoids image distortion in the
transverse direction observed with wide-fan beam devices.
The iDXA system uses a staggered array of 64 direct-digital
high-definition cadmium zinc telluride detectors—51 9
5 mm wide—to eliminate dead space between detectors
creating a high-resolution image. The enhanced digital
detectors increase image resolution, especially for bone.
Spatial resolution, evaluated by iDXA scan of a 10 line pair
phantom, was 3 LP/mm.
The patient was positioned in the left lateral decubitus,
according to the manufacturer’s guidelines. The position was
similar to standard spinal radiographs with the knees and hips
flexed in a 90� angle and the arms flexed with both hands
joined, so that the spine was parallel to the table to avoid
tilting of the vertebrae. Lateral spine VFA images, by dual-
energy modality, were used for fracture assessment, given
that the upper thoracic vertebrae are more clearly seen on
dual-energy than on single-energy images. Assuming that
the scan started in the sacrum and ended near T4, the scan
time (with Smart Scan) was estimated to be 120–240 s,
depending on patient size.
The effective radiation dose for a DXA lateral spine
scan set on standard thickness using iDXA was *12 lSv,
as declared by the manufacturer.
On spine VFA images the enCORETM Software v13.5
(Encore Software, San Jose, CA) automatically performed
vertebral morphometry, placing six points in each vertebral
body from L4 to T8 to calculate the anterior (Ha), middle (Hm),
and posterior (Hp) heights and their ratios (Ha/Hp, Hm/Hp) as
336 D. Diacinti et al.: Diagnostic Performance of VFA
123

well as the average height (HAVG) of each vertebra. The
software automatically estimated the extent of anterior or
middle vertebral height reduction with respect to posterior
height, classified the vertebrae as normal (\20 % reduction) or
fractured (wedge, biconcave, or crush), grading as mild
(20–25 % reduction), moderate (25–40 % reduction), or
severe ([40 % reduction) fractures according to the criteria of
Genant et al. [10].
Each automatic vertebral morphometry was reviewed by
a physician (R.D.F.) specialist in bone diseases with 5
years of VFA experience, who corrected manually the
marker placement in *30 % of the patients, according to
Hurxthal criteria [29]. He measured manually also the
heights of vertebrae from T7 to T4 if they were adequately
visualized.
The same physician interpreted the report of vertebral
morphometry considering both vertebral shape and the
appearance of the end plate in order to differentiate VFs
from other causes of vertebral deformities (e.g., develop-
mental variant, degenerative change, large Schmorl nodes,
Scheuermann disease) according to the ABQ method [30].
The time needed to perform VFA with vertebral mor-
phometry, including the operator review, averaged 6.5 ±
1.5 min (range 3.5–10.2).
To assess the intraoperator reproducibility of vertebral
morphometry, the spine DXA images of 50 subjects ran-
domly selected from the study population were analyzed by
the same operator twice with an interval of more than 30
days, blinded to the previous analysis.
Spine Radiographs
Conventional radiographs of the thoracic and lumbar spine
in anteroposterior and left lateral projections were acquired
by using a full digital radiographic system (Apollo DRF;
Villa Medical Systems, Milan, Italy) with the patients
positioned on the left side with the knees and hips flexed.
Tube-to-film distance was set at 105 cm, and the X-ray
beam was centered at T7 and L3 for the thoracic and
lumbar views, respectively. Conventional radiographs were
examined for VF identification by an experienced skeletal
radiologist (D.D.), who used ABQ in order to discriminate
nonfracture vertebral deformities and then classified the
true VFs according to visual SQ-Rx [10].
Statistical Analysis
Intraoperator precision was reported as the root mean
square standard deviation (RMS SD) and the coefficient of
variation (CV) of the differences between vertebral heights.
We calculated the frequency of unreadable vertebrae by
vertebral level and the prevalence of fracture, per person
and per vertebra, classifying VFs according to grade
(normal, mild, moderate, and severe).
The overall agreement, beyond that expected by chance
alone, between VFA and SQ-Rx was evaluated using a
simple kappa statistic and associated 95 % confidence
intervals (CIs). To assess the diagnostic value of VFA we
also calculated sensitivity, specificity, and positive and
negative predictive values (PPVs, NPVs) considering SQ-
Rx as the gold standard. In computing all these parameters,
vertebrae that were unreadable were classified as normal.
Finally, we repeated calculations including only subjects
with age C65 years. Analyses were performed using
statistical software (SPSS, version 18; SPSS, Inc.,
Chicago, IL).
Results
Intraoperator precision for vertebral morphometry resulted
in CV and RMS SD as follows: 1.4 % and 0.28 mm for Ha,
1.5 % and 0.27 mm for Hm, 1.7 % and 0.35 mm for Hp, 1.9
% and 0.37 mm for average height, 2.0 % and 0.019 for Ha/
Hp ratio, and 2.6 % and 0.023 for Hm/Hp ratio.
Per-vertebra Analysis
Of a total of 4,550 vertebrae from T4 to L4, the visualized
vertebrae were 4,535 (99.7 %) in the conventional radio-
graphs and 4,476 (98.37 %) in the VFA images. All unana-
lyzable vertebrae in the standard radiographs (n = 15) and in
the VFA images (n = 74) were localized in the upper thoracic
spine (T4–T6), most of them at T4 level (13 in standard
radiographs and 57 in VFA images).
Among the visualized vertebrae, 205/4,535 (4.5 %)
and 190/4,476 (4.2 %) were identified as nonfracture
vertebral deformities applying the ABQ approach to the
radiographs and VFA images, respectively. In detail,
vertebral deformities identified by conventional radiogra-
phy and by VFA were, respectively, 151 versus 144
degenerative changes, 2 versus 2 Scheuermann disease, 7
versus 7 developmental variations, and 45 versus 37
Schmorl nodes (Fig. 1).
There were 231 vertebrae classified as fractured by
SQ-Rx, whereas VFA detected 228 fractures (Fig. 2). Table
1 shows the number and grading of VFs assessed by the
two different techniques.
There was excellent agreement for VF identification,
assessed by k statistics, between SQ-Rx and VFA (agree-
ment 99.76 %, k score = 0.975, 95 % CI 0.960–0.990).
When considering also the grading of vertebral deformity,
the agreement was also very good (agreement 98.5 %,
k score = 0.871, 95 % CI 0.841–0.901).
D. Diacinti et al.: Diagnostic Performance of VFA 337
123
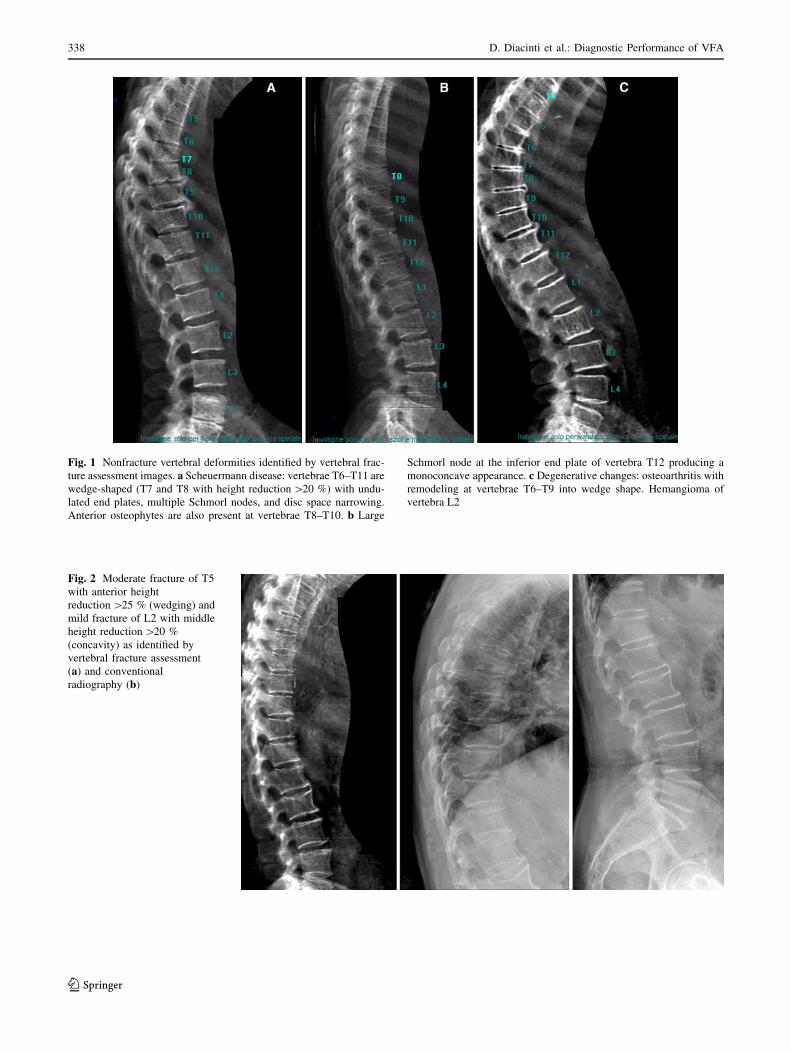
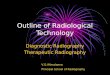
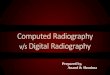
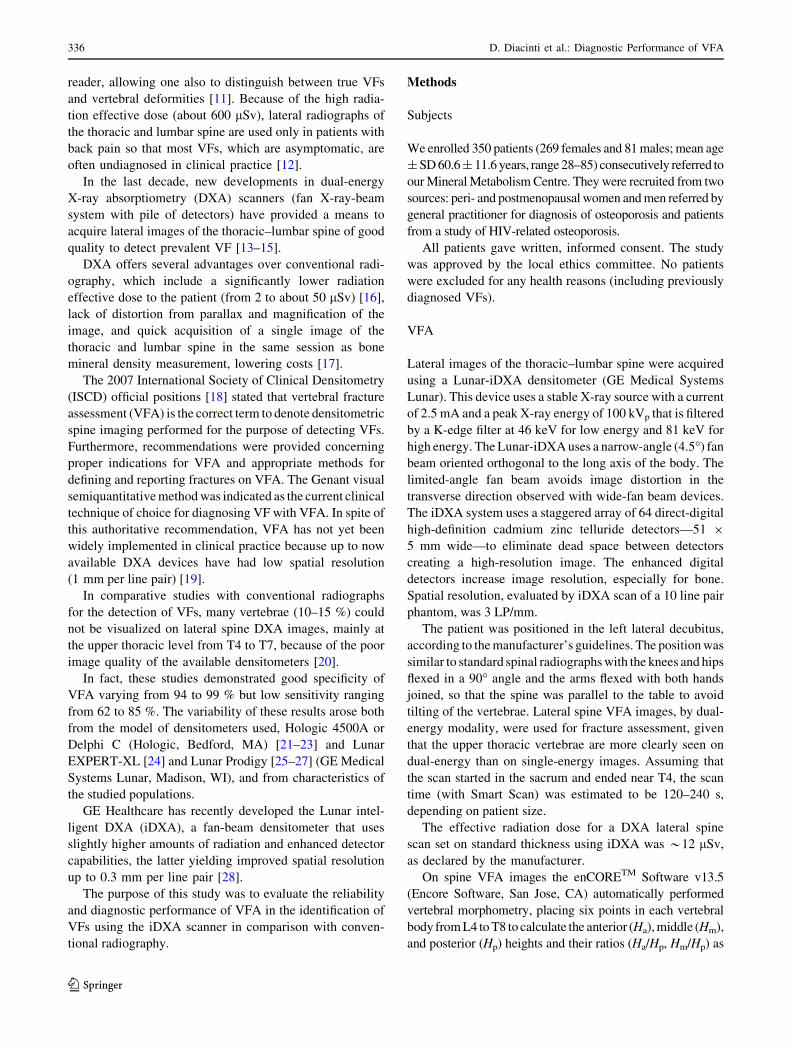
Fig. 1 Nonfracture vertebral deformities identified by vertebral frac-
ture assessment images. a Scheuermann disease: vertebrae T6–T11 are
wedge-shaped (T7 and T8 with height reduction [20 %) with undu-
lated end plates, multiple Schmorl nodes, and disc space narrowing.
Anterior osteophytes are also present at vertebrae T8–T10. b Large
Schmorl node at the inferior end plate of vertebra T12 producing a
monoconcave appearance. c Degenerative changes: osteoarthritis with
remodeling at vertebrae T6–T9 into wedge shape. Hemangioma of
vertebra L2
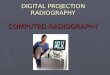
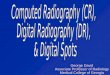
Fig. 2 Moderate fracture of T5
with anterior height
reduction [25 % (wedging) and
mild fracture of L2 with middle
height reduction [20 %
(concavity) as identified by
vertebral fracture assessment
(a) and conventional
radiography (b)
338 D. Diacinti et al.: Diagnostic Performance of VFA
123
Accepting SQ-Rx as the gold standard, all diagnostic
performance parameters of VFA were very high (sensitivity
98.68 %, specificity 99.91 %, PPV 98.25 %, NPV 99.93 %)
(see Table 2).
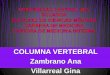
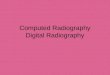
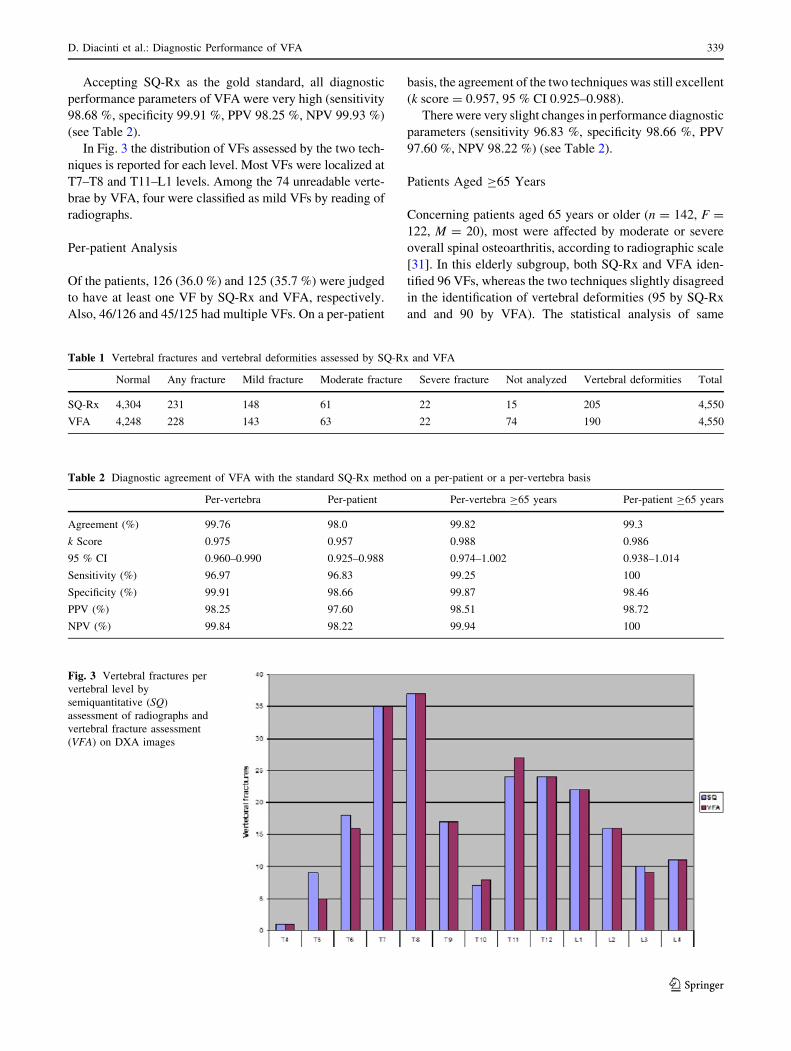
In Fig. 3 the distribution of VFs assessed by the two tech-
niques is reported for each level. Most VFs were localized at
T7–T8 and T11–L1 levels. Among the 74 unreadable verte-
brae by VFA, four were classified as mild VFs by reading of
radiographs.
Per-patient Analysis
Of the patients, 126 (36.0 %) and 125 (35.7 %) were judged
to have at least one VF by SQ-Rx and VFA, respectively.
Also, 46/126 and 45/125 had multiple VFs. On a per-patient
basis, the agreement of the two techniques was still excellent
(k score = 0.957, 95 % CI 0.925–0.988).
There were very slight changes in performance diagnostic
parameters (sensitivity 96.83 %, specificity 98.66 %, PPV
97.60 %, NPV 98.22 %) (see Table 2).
Patients Aged C65 Years
Concerning patients aged 65 years or older (n = 142, F =
122, M = 20), most were affected by moderate or severe
overall spinal osteoarthritis, according to radiographic scale
[31]. In this elderly subgroup, both SQ-Rx and VFA iden-
tified 96 VFs, whereas the two techniques slightly disagreed
in the identification of vertebral deformities (95 by SQ-Rx
and and 90 by VFA). The statistical analysis of same
Table 1 Vertebral fractures and vertebral deformities assessed by SQ-Rx and VFA
Normal Any fracture Mild fracture Moderate fracture Severe fracture Not analyzed Vertebral deformities Total
SQ-Rx 4,304 231 148 61 22 15 205 4,550
VFA 4,248 228 143 63 22 74 190 4,550
Table 2 Diagnostic agreement of VFA with the standard SQ-Rx method on a per-patient or a per-vertebra basis
Per-vertebra Per-patient Per-vertebra C65 years Per-patient C65 years
Agreement (%) 99.76 98.0 99.82 99.3
k Score 0.975 0.957 0.988 0.986
95 % CI 0.960–0.990 0.925–0.988 0.974–1.002 0.938–1.014
Sensitivity (%) 96.97 96.83 99.25 100
Specificity (%) 99.91 98.66 99.87 98.46
PPV (%) 98.25 97.60 98.51 98.72
NPV (%) 99.84 98.22 99.94 100
Fig. 3 Vertebral fractures per
vertebral level by
semiquantitative (SQ)
assessment of radiographs and
vertebral fracture assessment
(VFA) on DXA images
D. Diacinti et al.: Diagnostic Performance of VFA 339
123
parameters failed to demonstrate important changes with
respect to the whole population enrolled (see Table 2).
Discussion
This study demonstrated in a large sample of patients that
the improved quality of images by the new iDXA densi-
tometer leads to a higher accuracy of VFA in the diagnosis
of VF, identifying also most mild VFs.
In fact, most vertebrae (98.4 %) were adequately visu-
alized in VFA images. The clinical impact of the 74
unreadable vertebrae by VFA was minimal because most
of them (n = 57) were localized at the T4 level, where
fracture rarely occurs. Therefore, only four unreadable
vertebrae by VFA were classified as mild fractures by
SQ-Rx, and three of them were in patients with other VFs
who were correctly identified as ‘‘patients with fractures.’’
Furthermore, as previously reported [32], most VFs
were localized at T7–T8 and T11–L2 vertebral levels,
where all vertebrae were always well visualized. A simi-
larly high percentage of readable vertebrae was reported in
some recently published studies. Buehring et al. [33]
demonstrated that iDXA adequately visualized from T6
through L4 95 % of vertebrae compared to 87 % of ver-
tebrae by Prodigy. In two other studies, lateral spine DXA
scans were acquired using the Hologic Discovery-A
device, a densitometer with the scanner arm rotated 90�and with the patient in the supine position throughout the
procedure. Hospers et al. [34] reported in 250 patients that
98.7 % of vertebrae from L4 through T4 were analyzable
for VFA. Jager et al. [35], performing a study on a larger
population with the same densitometer, the Hologic
Discovery-A, found that the percentage of readable verte-
brae was high (93 %) in 2,247 patients from L4 through T5
but decreased to 82 % when T4 was included in the eval-
uation. The ability to adequately visualize most vertebrae
included in the scan region using the new densitometers
owing to higher resolution of images improved the diag-
nostic performance of VFA to detect vertebral fractures
[36].
In fact, the results of our study show that VFA by iDXA
had very high sensitivity and specificity and excellent
agreement with SQ-Rx, misclassifying only 11 among
4,550 vertebrae.
The accuracy of VFA performed by older models of
densitometers was lower, with sensitivity up to 84 % in
detecting vertebral fractures [21–25, 37, 38]. In all these
comparative studies, VFA was less accurate in detecting
mild VFs with respect to moderate and severe fractures. In
our study, only three mild VFs identified by SQ-Rx were
undiagnosed by VFA. It has been emphasized that the
clinical significance and true nature of mild vertebral
deformities, defined as 20–25 % height reduction, are often
questionable because vertebral deformities are not always
due to osteoporotic VFs [23, 39, 40]. Although it may be
difficult especially in mild deformities, it is necessary to
discriminate between true VF and nonfracture vertebral
deformities, in particular the so-called short vertebral
height (SVH) deformity [41]. The presence of SVH is the
greatest source of misclassification of VF, particularly by
quantitative vertebral morphometry that always judges
mild vertebral deformities as VFs.
Current guidelines for VFA [18] recommend use of the
SQ method for visual estimation of apparent reduction in
vertebral height C20 % for diagnosis of a prevalent VF.
This approach may be problematic because of the presence
of nonosteoporotic deformities that may also appear as
wedging or concavities for vertebral height reduction. The
ABQ method instead focuses on the appearance of the
central vertebral end plates to identify prevalent fractures
rather than on the appearance of ‘‘reduced’’ (short) verte-
bral height [30]. Recently, the ABQ method has been
applied in VFA, resulting in very high specificity with
absence of false-positive VFs caused by misclassification
of nonfracture deformities. Nevertheless, sensitivity was
low as the poor image quality of older DXA densitometers
led to a high percentage of false-negatives: 41 % of
radiographic VFs were either missed by VFA or not ana-
lyzed [42].
In our study we demonstrated that the high quality of
images by iDXA allowed most vertebrae to be visualized
adequately, improving the sensitivity of VFA to identify,
according to the criteria of Genant et al. [10], most VFs,
even mild, differentiating them from several other causes
of vertebral deformities. In fact, using the ABQ method,
VFA missed only 15 nonfracture vertebral deformities with
respect to conventional radiographs, demonstrating high
accuracy in the assessment of VF status.
Hence, when performing VFA, nonosteoporotic defor-
mities should be ruled out first, performing an accurate visual
assessment of all vertebrae by an expert reader using the
ABQ method, followed by determination of fracture severity
either with the SQ approach or with vertebral quantitative
morphometry. Furthermore, it could be necessary to com-
pare the measured vertebral dimensions with reference ver-
tebral height values specific for the population and probably
even for age groups to identify VFs with better accuracy for
both epidemiological studies and clinical practice [43].
Moreover, VFA images allowed us to visualize osteophytes
and vertebral remodeling due to osteoarthritis as well as
conventional radiography. In fact, our results demonstrated
that in a subgroup of older patients[65 years the presence of
moderate to severe osteoarthritis did not interfere with the
diagnostic performance of VFA, which identified in these
patients the same number of VFs as SQ-Rx.
340 D. Diacinti et al.: Diagnostic Performance of VFA
123

This study had some limitations. The studied population
included a sample (26.8 %) of relatively young patients
(mean age 50.4 ± 10.2) with suspected HIV-related oste-
oporosis. Most of these patients had absent or mild osteo-
arthritis, allowing good visibility of most vertebrae to be
analyzed by VFA. This could explain the high specificity of
VFA in our study. However, no important difference
resulted in the statistical analysis restricted to patients aged
C65 years. Furthermore, the conventional radiography that
we used as a reference standard has some well-known
limitations due to the X-ray cone beam, which causes
geometric distortion of vertebrae located at the extremities
of the scans Therefore, some vertebrae at T4–T5 level,
identified by SQ-Rx as mild fractures and judged as normal
vertebrae on VFA, could be false VFs as a result of error
from parallax of conventional radiography.
The important result obtained in this study is the
excellent agreement between the two methods, SQ-Rx and
VFA, first due to the integration of advanced iDXA tech-
nology with the experience of both readers. Second, patient
position in lateral decubitus was the same in the acquisition
of both iDXA scans and standard spinal radiographs. Third,
both examinations were performed on the same day, by a
single technician for each method, using the same X-ray
device and the same densitometer. Thus, errors due to the
use of different devices and technicians were eliminated,
improving the validity of our comparison of the two
techniques.
Appropriate indications for using VFA, in both women
and men, were suggested by the ISCD official positions, to
detect VFs among patients at high risk of fracture [18],
even though for mild fractures VFA by older DXA scan-
ners had lower sensitivity than conventional radiography. It
should be emphasized that even if mild VFs are often
asymptomatic, they significantly increase the risk of new
VFs in osteoporotic patients.
Considering the high performance of new DXA scanners
in identifying even mild VFs, we suggest the introduction of
VFA as an alternative to conventional radiography in
patients at high risk of VF who are undergoing DXA bone
densitometry and in the follow-up of osteoporotic patients on
treatment. However, it should be recommended to integrate
the advanced DXA technology with operator formal training
in, and subsequent experience with, VFA interpretation to
achieve high accuracy in VF identification.
In conclusion, VFA is a reliable and practical tool for
diagnosing VFs, taking into account its low radiation
effective dose and the opportunity of combined assessment
of bone mineral density and vertebral fracture status.
Conflict of interest The authors have stated that they have no
conflict of interest.
References
1. Cummings SR, Melton LJ (2002) Epidemiology and outcomes of
osteoporotic fractures. Lancet 359:1761–1767
2. Cauley JA, Palermo L, Vogt M, Ensrud KE, Ewing S, Hochberg
M, Nevitt MC, Black DM (2008) Prevalent vertebral fractures
in black women and white women. J Bone Miner Res 23:1458–
1467
3. Delmas PD, van de Langerijt L, Watts NB, Eastell R, Genant H,
Grauer A, Cahall DL (2005) Underdiagnosis of vertebral frac-
tures is a worldwide problem: the IMPACT study. J Bone Miner
Res 20:557–563
4. Kim N, Rowe BH, Raymond G, Jen H, Colman I, Jackson SA,
Siminoski KG, Chahal AM, Folk D, Majumdar SR (2004)
Underreporting of vertebral fractures on routine chest radiogra-
phy. Am J Roentgenol 182:297–300
5. Lindsay R, Pack S, Li Z (2005) Longitudinal progression of
fracture prevalence through a population of postmenopausal
women with osteoporosis. Osteoporos Int 16:306–312
6. Roux C, Fechtenbaum J, Kolta S, Briot K, Girard M (2007) Mild
prevalent and incident vertebral fractures are risk factors for new
fractures. Osteoporos Int 18:1617–1624
7. Cauley JA, Hochberg MC, Lui LY, Palermo L, Ensrud KE,
Hillier TA, Nevitt MC, Cummings SR (2007) Long-term risk of
incident vertebral fractures. JAMA 298:2761–2767
8. Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I,
Petterson C, De Laet C, Jonsson B (2004) Mortality after oste-
oporotic fractures. Osteoporos Int 15:38–42
9. Romagnoli E, Carnevale V, Nofroni I, D’Erasmo E, Paglia F,
De Geronimo S, Pepe J, Raejntroph N, Maranghi M, Minisola S
(2004) Quality of life in ambulatory postmenopausal women: the
impact of reduced bone mineral density and subclinical vertebral
fractures. Osteoporos Int 15:975–980
10. Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral
fracture assessment using a semiquantitative technique. J Bone
Miner Res 8:1137–1148
11. Genant HK, Jergas M, Palermo L, Nevitt M, Valentin RS, Black
D, Cummings SR (1996) Comparison of semiquantitative visual
and quantitative morphometric assessment of prevalent and
incident vertebral fractures in osteoporosis: the Study of Osteo-
porotic Fractures Research Group. J Bone Miner Res 11:984–996
12. Gehlbach SH, Bigelow C, Heimisdottir M, May S, Walker M,
Kirkwood JR (2000) Recognition of vertebral fracture in a clin-
ical setting. Osteoporos Int 11:577–582
13. Blake GM, Rea JA, Fogelman I (1997) Vertebral morphometry
studies using dual-energy X-ray absorptiometry. Semin Nucl Med
27:276–290
14. Lang T, Takada M, Gee R, Wu C, Li J, Hayashi-Clark C, Schoen
S, March V, Genant HK (1997) A preliminary evaluation of the
Lunar Expert-XL for bone densitometry and vertebral mor-
phometry. J Bone Miner Res 12:136–143
15. Crabtree N, Wright J, Walgrove A, Rea J, Hanratty L, Lunt M,
Fogelman I, Palmer R, Vickers M, Compston JE, Reev J (2000)
Vertebral morphometry: repeat scan precision using the Lunar
Expert-XL and the Hologic 4500A. A study for the ‘‘WISDOM’’
RCT of hormone replacement therapy. Osteoporos Int 11:537–
543
16. Damilakis J, Adams JE, Guglielmi G, Link TM (2010) Radiation
exposure in X-ray-based imaging techniques used in osteoporo-
sis. Eur Radiol 20:2707–2714
17. Olenginski TP, Newman ED, Hummel JL, Hummer M (2006)
Development and evaluation of a vertebral fracture assess-
ment program using IVA and its integration with mobile DXA.
J Clin Densitom 9:72–77
D. Diacinti et al.: Diagnostic Performance of VFA 341
123
18. Schousboe JT, Vokes T, Broy SB, Ferrar L, McKiernan F, Roux
C, Binkley N (2008) Vertebral fracture assessment: the 2007
ISCD official positions. J Clin Densitom 11:92–108
19. Thorpe JA, Steel SA (1999) Image resolution of the Lunar
Expert-XL. Osteoporos Int 10:95–101
20. Duboeuf F, Bauer DC, Chapurlat RD, Dinten JM, Delmas P
(2005) Assessment of vertebral fracture using densitometric
morphometry. J Clin Densitom 8:362–368
21. Rea JA, Chen MB, Li J, Blake GM, Steiger P, Genant HK,
Fogelman I (2000) Morphometric X-ray absorptiometry and
morphometric radiography of the spine: a comparison of pre-
valent vertebral deformity identification. J Bone Miner Res
15:564–574
22. Ferrar L, Jiang G, Eastell R, Peel NF (2003) Visual identification
of vertebral fractures in osteoporosis using morphometric X-ray
absorptiometry. J Bone Miner Res 18:933–938
23. Schousboe JT, Debold CR (2006) Reliability and accuracy of
vertebral fracture assessment with densitometry compared to
radiography in clinical practice. Osteoporos Int 17:281–289
24. Pavlov L, Gamble GD, Reid IR (2005) Comparison of dual-
energy X-ray absorptiometry and conventional radiography for
the detection of vertebral fractures. J Clin Densitom 8:379–385
25. Vokes TJ, Dixon LB, Favus MJ (2003) Clinical utility of dual-
energy vertebral assessment (DVA). Osteoporos Int 14:871–878
26. Binkley N, Krueger D, Gangnon R, Genant HK, Drezner MK
(2005) Lateral vertebral assessment: a valuable technique to
detect clinically significant vertebral fractures. Osteoporos Int 16:
1513–1518
27. Fuerst T, Wu C, Genant HK, von Ingersleben G, Chen Y, Johnston C,
Econs MJ, Binkley N, Vokes TJ, Crans G, Mitlak BH (2009) Eval-
uation of vertebral fracture assessment by dual X-ray absorptiometry
in a multicenter setting. Osteoporos Int 20:1199–1205
28. Krueger D, Vallarta-Ast N, Checovich M, Gemar D, Binkley N
(2012) BMD measurement and precision: a comparison of GE
Lunar Prodigy and iDXA densitometers. J Clin Densitom 15:21–25
29. Hurxthal LM (1968) Measurement of anterior vertebral com-
pressions and biconcave vertebrae. Am J Roentgenol Radium
Ther Nucl Med 103:635–644
30. Jiang G, Eastell R, Barrington NA, Ferrar L (2004) Comparison
of methods for the visual identification of prevalent vertebral
fracture in osteoporosis. Osteoporos Int 15:887–896
31. Lane NE, Nevitt MC, Genant HK, Hochberg MC (1993) Reliability
of new indices of radiographic osteoarthritis of the hand and hip and
lumbar disc degeneration. J Rheumatol 20:1911–1918
32. Ismail AA, Cooper C, Felsenberg D, Varlow J, Kanis JA, Silman
AJ, O’Neill TW (1999) Number and type of vertebral deformities:
epidemiological characteristics and relation to back pain and height
loss. European Vertebral Osteoporosis Study Group. Osteoporos
Int 9:206–213
33. Buehring B, Krueger D, Checovich M, Gemar D, Vallarta-Ast N,
Genant HK, Binkley N (2010) Vertebral fracture assessment:
impact of instrument and reader. Osteoporos Int 21:487–494
34. Hospers IC, van der Laan JG, Zeebregts CJ, Nieboer P, Wolf-
fenbuttel BH, Dierckx RA, Kreeftenberg HG, Jager PL, Slart RH
(2009) Vertebral fracture assessment in supine position: com-
parison by using conventional semiquantitative radiography and
visual radiography. Radiology 251:822–828
35. Jager PL, Jonkman S, Koolhaas W, Stiekema A, Wolffenbuttel BH,
Slart RH (2011) Combined vertebral fracture assessment and bone
mineral density measurement: a new standard in the diagnosis of
osteoporosis in academic populations. Osteoporos Int 22:1059–
1068
36. Guglielmi G, Diacinti D, van Kuijk C, Aparisi F, Krestan C,
Adams JE, Link TM (2008) Vertebral morphometry: current
methods and recent advances. Eur Radiol 18:1484–1496
37. Vosse D, Heijckmann C, Landewe R, van der Heijde D, van der
Linden S, Geusens P (2007) Comparing morphometric X-ray
absorptiometry and radiography in defining vertebral wedge
fractures in patients with ankylosing spondylitis. Rheumatology
(Oxford) 46:1667–1671
38. Chapurlat RD, Duboeuf F, Marion-Audibert HO, Kalpakcioglu B,
Mitlak BH, Delmas PD (2006) Effectiveness of instant vertebral
assessment to detect prevalent vertebral fracture. Osteoporos Int
17:1189–1195
39. Kleerekoper M, Nelson DA (1992) Vertebral fracture or vertebral
deformity. Calcif Tissue Int 50:5–6
40. Ziegler R, Scheidt-Nave C, Leidig-Bruckner G (1996) What is a
vertebral fracture? Bone 18:169S–177S
41. Ferrar L, Jiang G, Armbrecht G, Reid DM, Roux C, Gluer CC,
Felsenberg D, Eastell R (2007) Is short vertebral height always an
osteoporotic fracture? The Osteoporosis and Ultrasound Study
(OPUS). Bone 41:5–12
42. Ferrar L, Jiang G, Clowes JA, Peel NF, Eastell R (2008) Compar-
ison of densitometric and radiographic vertebral fracture assess-
ment using the algorithm-based qualitative (ABQ) method in
postmenopausal women at low and high risk of fracture. J Bone
Miner Res 23:103–111
43. Diacinti D, Pisani D, Del Fiacco R, Francucci CM, Fiore CE,
Frediani B, Barone A, Bartalena T, Cattaruzza MS, Guglielmi G,
Romagnoli E, Minisola S (2011) Vertebral morphometry by
X-ray absorptiometry: which reference data for vertebral heights?
Bone 49:526–536
342 D. Diacinti et al.: Diagnostic Performance of VFA
123